
Abstract
The present study investigated the association between the presence of periodontitis and aortic calcification (AC) risk among Chinese adults. A total of 6059 individuals who underwent regular health check-ups and received a diagnosis of periodontitis between 2009 and 2016 were included. The outcome was AC, assessed by a chest low-dose spiral CT scan. Cox proportional hazards regression analysis was used to assess the association between periodontitis and AC risk after adjusting for several confounders. After a median follow-up period of 2.3 years (interquartile range: 1.03–4.97 years), 843 cases of AC were identified, with 532 (12.13%) and 311 (18.59%) patients in the non-periodontitis group and periodontitis group, respectively. Multivariate analyses demonstrated that, compared with those without periodontitis, the hazard ratio and 95% confidence interval for AC risk in participants with periodontitis was 1.18 (1.02–1.36) (P = .025) in the fully adjusted model. Stratified analyses showed that the positive relationship between periodontitis and AC was more evident in males and participants <65 years of age (pinteraction = .005 and .004, respectively). Our results show that the presence of periodontitis was positively associated with AC among Chinese adults, especially among males and younger participants.
Introduction
As the leading cause of mortality globally, cardiovascular diseases (CVDs) account for the deaths of 17.9 million people every year. 1 Half of the world’s cardiovascular burden is estimated to occur in Asia, 2 and CVD causes 40% of deaths in the Chinese population. 3 Cardiovascular calcification, such as aortic calcification (AC), is an independent and reliable predictor of CVD events and mortality.4-6 Previous studies have demonstrated that the presence of thoracic AC was associated with an increased risk of coronary artery calcium and predicted the presence and severity of coronary artery disease.7-9 Besides, thoracic AC could be a potential marker for development of subclinical atherosclerotic disease in the cardiac, cerebral and peripheral arterial circulation.4,10,11 Increased knowledge of risk factors of AC may contribute to the prevention of CVD.
Periodontitis is a highly prevalent chronic infectious disease caused by pathogenic microflora, mainly Gram negative and anaerobic species, resulting in alveolar bone resorption and periodontal tissue damage.12,13 Periodontitis may play an important role in the formation and development of aortic atherosclerosis mainly through inducing increased pro-inflammatory cytokines, lipid accumulation and peroxidation.14-19 In addition, periodontal infection may have an effect on atherosclerotic lesions by regulating angiopoietin expression in aortic smooth muscle cells. 14 During the course of atherosclerosis progression, AC may occur by cellular osteogenic differentiation within atherosclerotic plaques, resulting in aortic stiffness.15,16
Some epidemiologic studies have investigated the relationship between periodontitis and AC risk,17,18,20,21 but the results were inconsistent. In a prospective longitudinal cohort study including 106 patients, severe periodontal disease was demonstrated to be associated with increased aortic arch atheroma plaque thickness and calcification. 17 However, the study population was limited to patients with stroke or transient ischemic attack at baseline. A retrospective cross-sectional study with 531 participants also indicated that marginal periodontitis was significantly associated with AC. 18 Furthermore, Nakib et al. 20 found that periodontitis was not strongly associated with coronary artery calcification (CAC) in the Atherosclerosis Risk in Communities (ARIC) cohort with 6931 participants and the First National Health and Nutrition Examination Survey (NHANES I) Epidemiologic Follow-up Study that included 8032 participants did not find convincing evidence of a causal association between periodontal disease and coronary heart disease (CHD) risk. 21
Considering the inconsistent findings and limited sample sizes of previous studies and a lack of prospective studies among general populations, we conducted a prospective cohort study to investigate the relationship between periodontitis and the subsequent occurrence of AC, with a relatively larger number of participants (Chinese adults).
Methods
Study Population
The current cohort study used data from a follow-up study conducted in Xiaotangshan hospital, Beijing, China. The design of the study has been described in detail.22-24 Briefly, subjects enrolled in the cohort study were adults who underwent regular health check-ups annually or biennially at the clinics of this hospital. The study population consisted of nearly 90% civil service officers with free annual or biennial health check-up benefits and 10% individuals who purchased their own check-up examinations.
A total of 52402 individuals who underwent health check-up examinations performed between January 1, 2009 and December 31, 2016 were included in this cohort study. However, a sub-cohort included 16518 individuals who participated in the ultrasound examination. For our analysis, we firstly excluded subjects who received examinations less than twice (n = 6568) and those who aged <18 years old (n = 21). Subjects with a history of stroke, cancer, CHD, myocardial infarction or AC disease at baseline (n = 384) were also excluded. In addition, we excluded those with missing data or pre-existing diagnosis of AC before the study (n = 1067) and those who did not complete an oral examination in health check-ups at baseline (n = 2067). Furthermore, subjects with outliers for continuous index (eg, total cholesterol and triglycerides) which under .1% or/and over 99.9% at baseline were excluded (n = 352). The remaining 6059 participants were enrolled in the final study population. The flowchart of participant selection is shown in Figure 1. Flowchart of participant selection.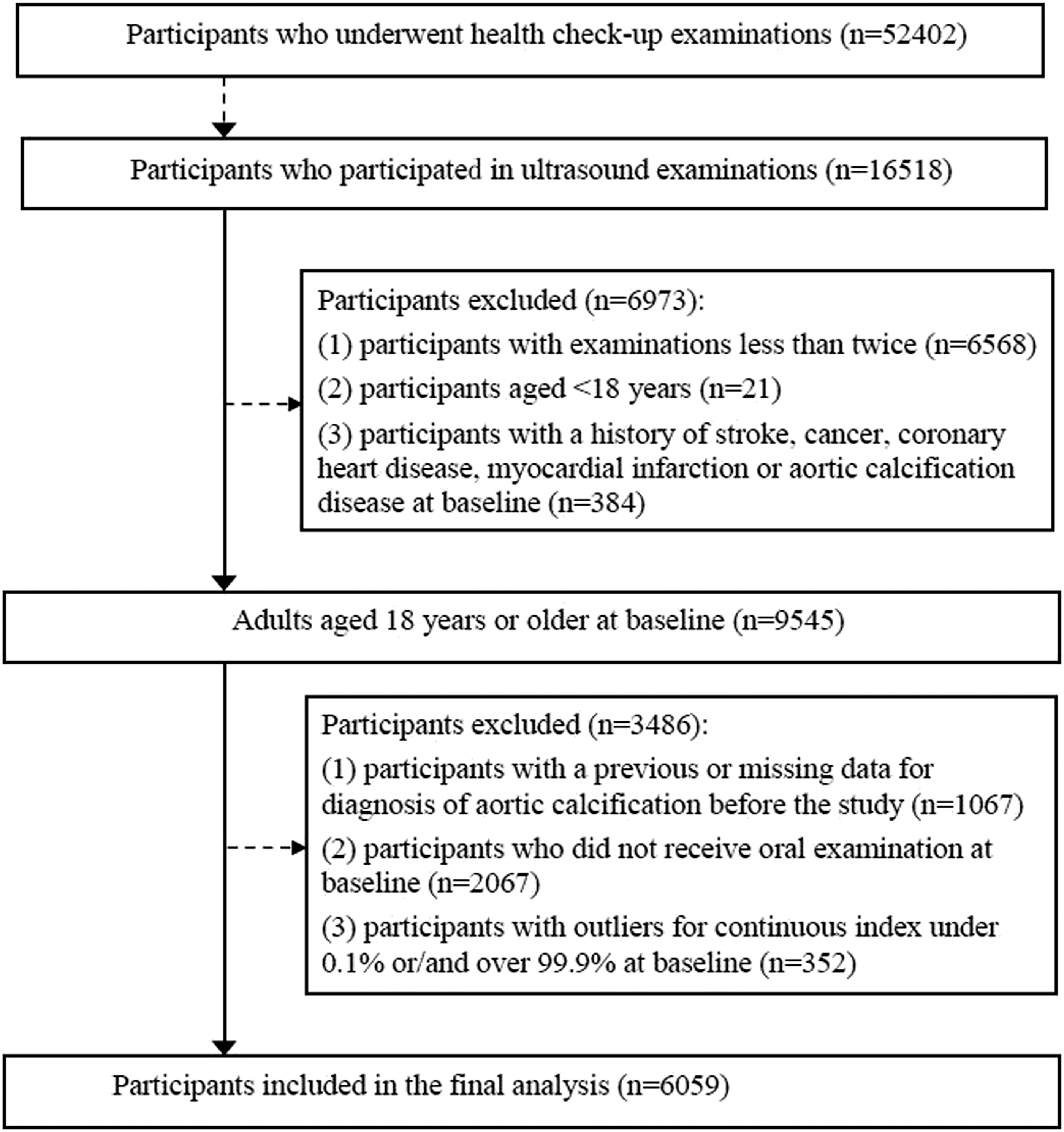
Data Collection
Subjects received health check-up examinations at the clinics of the Xiaotangshan hospital in Beijing, China. Before the examinations, participants completed a self-administered questionnaire to collect information including sociodemographic characteristics (eg, age, gender, and marital status), lifestyle (eg, smoking and alcohol drinking status), history of chronic diseases, and medical and family history via face-to-face interviews carried out by trained nurses. After the interviews, anthropometric data of standing height, body weight and blood pressure were measured. Body mass index (BMI) was calculated as weight in kg divided by height in m squared and classified into 3 groups: overweight for a BMI of 24–27.9 kg/m2 and obesity for BMI ≥28 kg/m2. 19 Hypertension was defined as systolic blood pressure/diastolic blood pressure (SBP/DBP)≥130/85 mmHg or on antihypertensive drug treatment in patients with a history of hypertension. 25
The periodontal examination was conducted by trained dentists during clinical examinations. Clinical periodontal measurements included probing depth (PD) and gingival recession were performed on 6 sites per tooth (mesiobuccal, midbuccal, distobuccal, mesiolingual, midlingual, and distolingual) in the full mouth (excluding third molars and tooth furcation lesion measurements) using a manual periodontal probe with millimeter markers (Hu-Friedy, Chicago, IL, USA). Measurements were mathematically rounded to whole millimeters. Clinical attachment loss was evaluated by the difference between PD and gingival recession. Periodontitis was diagnosed according to the Centers for Disease Control and Prevention and the American Academy of Periodontology (CDC/AAP) definition. 26 Periodontitis was defined as ≥2 interproximal sites with loss of attachment ≥3 mm and ≥2 interproximal sites with periodontal probing depth ≥4 mm (not on the same tooth) or 1 site with ≥5 mm.
For biochemical laboratory tests, blood samples were collected from an anterior cubital vein after at least overnight fasting. Serum lipids (total cholesterol (TC), low-density lipoprotein cholesterol (LDL-C), triglycerides (TG), and high-density lipoprotein cholesterol (HDL-C)) were measured with an enzymatic colorimetric assay (Type 7600; Hitachi Ltd., Tokyo, Japan). Hemoglobin A1c (HbA1c) was measured by high-performance liquid chromatography (HPLC) with the Bio-Rad Variant II (Bio-Rad, Munich, Germany). Biochemical indicators (fasting plasma glucose (FPG), 2 h postprandial plasma glucose) were measured by an automatic biochemical analyzer (Olympus AU400, Tokyo, Japan).
The study protocol was approved by the Institutional Review Board of Xiaotangshan Hospital (No. 202006), which waived the requirement for informed consent because we only used the routine health anonymized screening data.
Outcome
Study participants underwent a low-dose spiral CT scan for chest examination using a 16-row spiral CT scanner (Bright speed, General Electric Company, Fairfield, CT, USA). Participants were instructed to hold their breath during the chest CT scan and images were acquired from lung apex to diaphragm. All scan data were saved on an optical disc and images were displayed on a workstation. AC was defined as an area of ≥1 mm2 with a density of >130 Hounsfield units. AC was evaluated by trained radiology technicians who were blinded to each participant’s characteristics.
Statistical Analysis
For analysis, participants of the study were divided into two categories by the occurrence of AC, as well as with or without periodontitis. Descriptive statistics of the baseline population characteristics were described with means ± standard deviations for continuous variables, and numbers and proportions for categorical variables. Significant differences of baseline characteristics were assessed using the independent samples t-test (continuous variables) or the chi-square test (categorical variables).
Kaplan–Meier analysis was applied to estimate the cumulative incidence of AC by age (<65 vs ≥65 years), gender (male vs female), BMI (<24, 24–27.9, or ≥28 kg/m2), periodontitis (yes vs no), hypertension (yes vs no), diabetes (yes vs no), smoking status (never, past, or current smoker) and drinking status (never, past, or current drinker) and a log-rank test was used to examine the difference between groups.
Cox proportional hazards regression analysis was used to estimate the hazard ratio (HR) and 95% confidence interval (95% CI) for the association between periodontitis and incident AC.
Four models were applied to adjust potential confounding factors: model 1 only adjusted for age (continuous, years) and gender (male vs female); model 2 additionally adjusted for marital status (married vs unmarried), smoking status (never, past, or current), drinking status (never, past, or current) and BMI (continuous, kg/m2); model 3 further adjusted for hypertension (yes vs no) and diabetes (yes vs no); and model 4 adjusted for confounders in model 3 + TC (continuous, mmol/L), TG (continuous, mmol/L) and HDL-C (continuous, mmol/L).
We also performed subgroup analyses according to age (<65 vs ≥65 years), gender (male vs female), BMI (<24, 24–27.9, or ≥28 kg/m2), diabetes (yes vs no), smoking status (never, past, or current smoker) and drinking status (never, past, or current drinker). Subgroup analyses were conducted using model 4 and the P value for interaction was also calculated between periodontal status and the above variables.
All statistical analyses were performed with R-3.6.1 (R Development Core Team, Vienna, Austria). A 2-tailed P < .05 was considered statistically significant.
Results
Baseline Characteristics of the Study Population by Aortic Calcification Status.
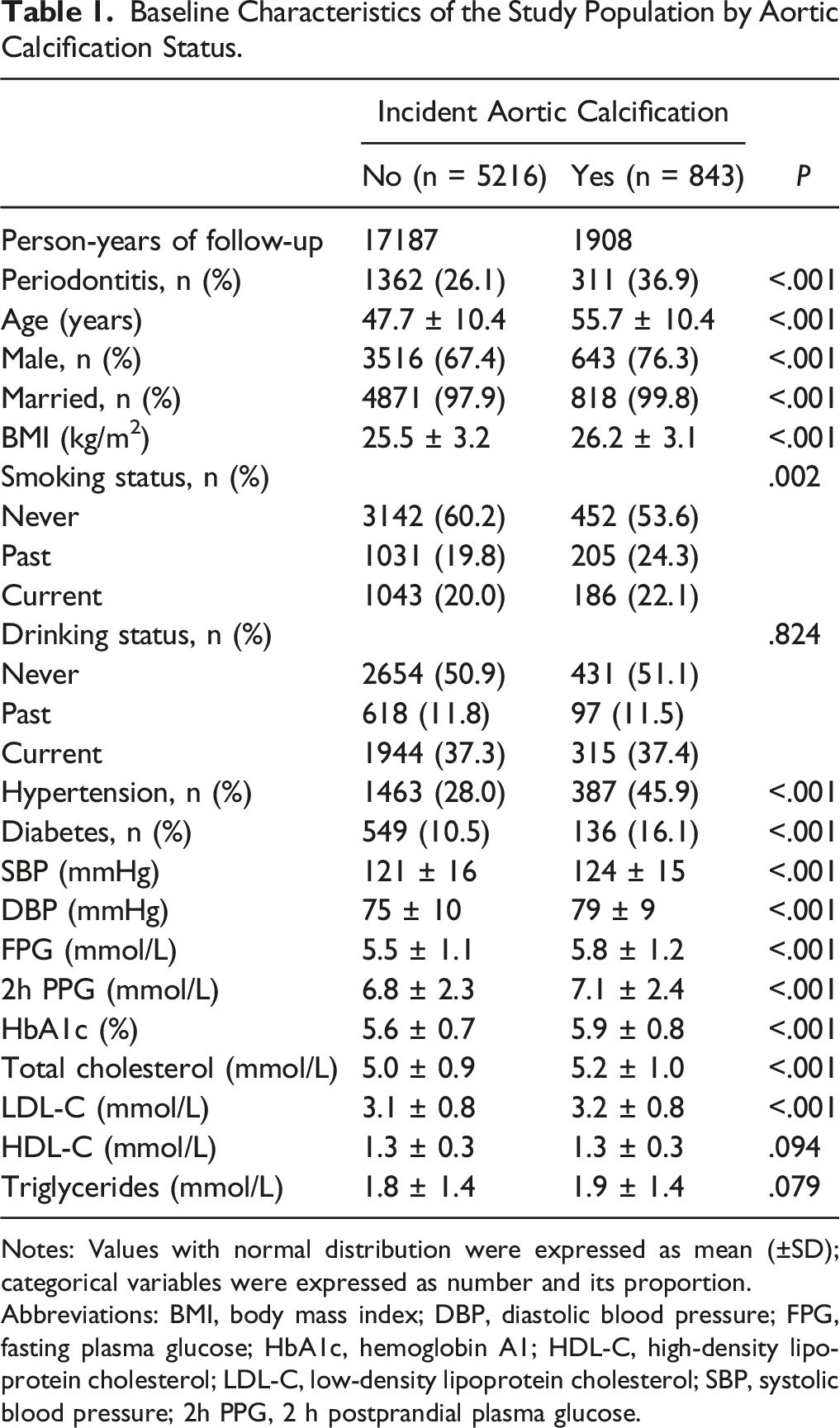
Notes: Values with normal distribution were expressed as mean (±SD); categorical variables were expressed as number and its proportion.
Abbreviations: BMI, body mass index; DBP, diastolic blood pressure; FPG, fasting plasma glucose; HbA1c, hemoglobin A1; HDL-C, high-density lipoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol; SBP, systolic blood pressure; 2h PPG, 2 h postprandial plasma glucose.
Kaplan–Meier analyses indicated that the cumulative incidence of AC was higher in participants aged >65 years (log-rank test, P < .0001), males (log-rank test, P < .0001), with a higher BMI (log-rank test, P < .0001), with periodontitis(log-rank test, P < .0001), with hypertension (log-rank test, P < .0001), with diabetes (log-rank test, P < .0001) or smokers (log-rank test, P = .0022) (Figure 2). Kaplan–Meier curves of the incidence of aortic calcification (AC) by age, gender, body mass index (BMI), periodontitis, hypertension, diabetes, smoking and drinking status.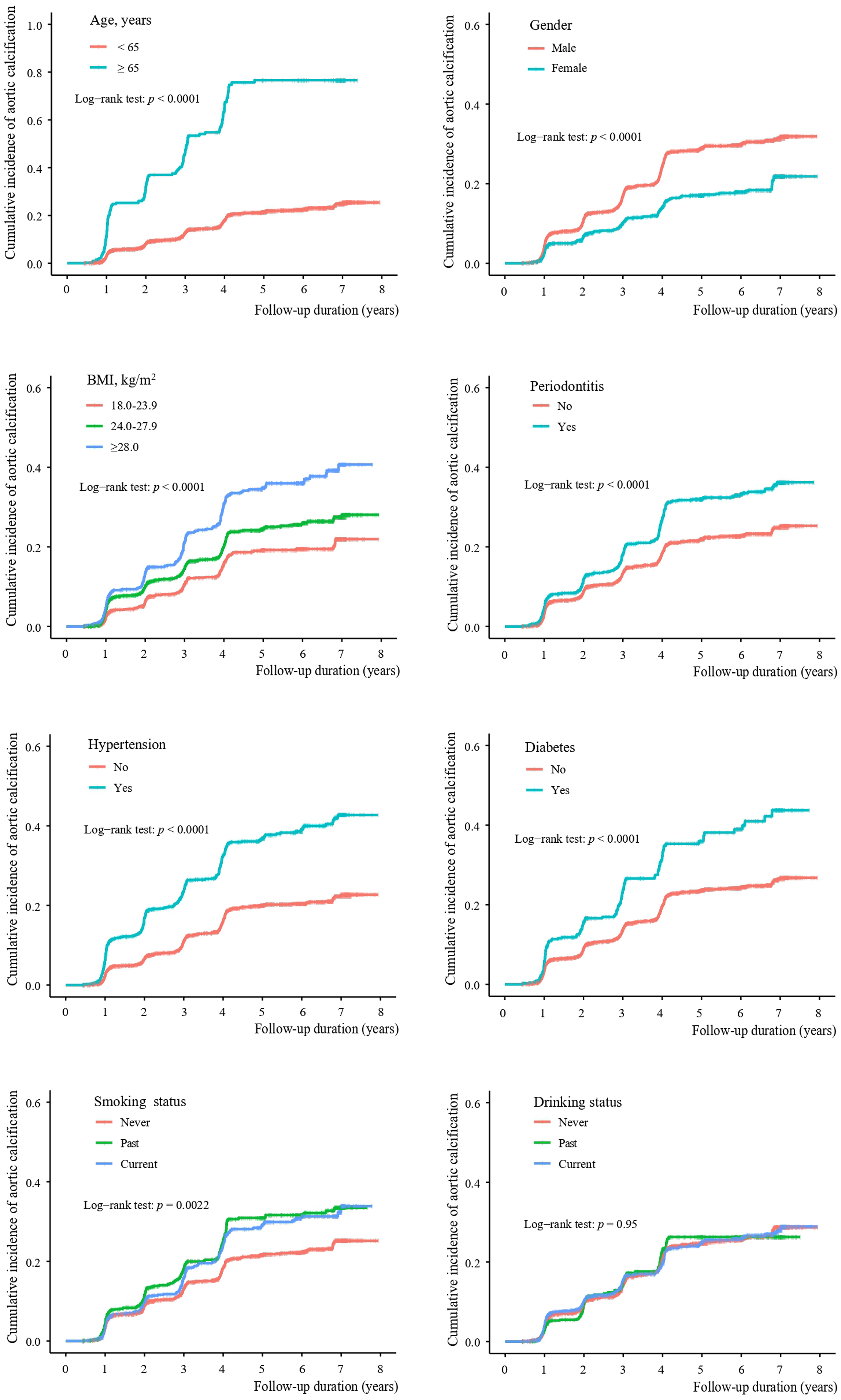
HR (95% CIs) of Periodontitis and Other Factors on the Incidence of Aortic Calcification.
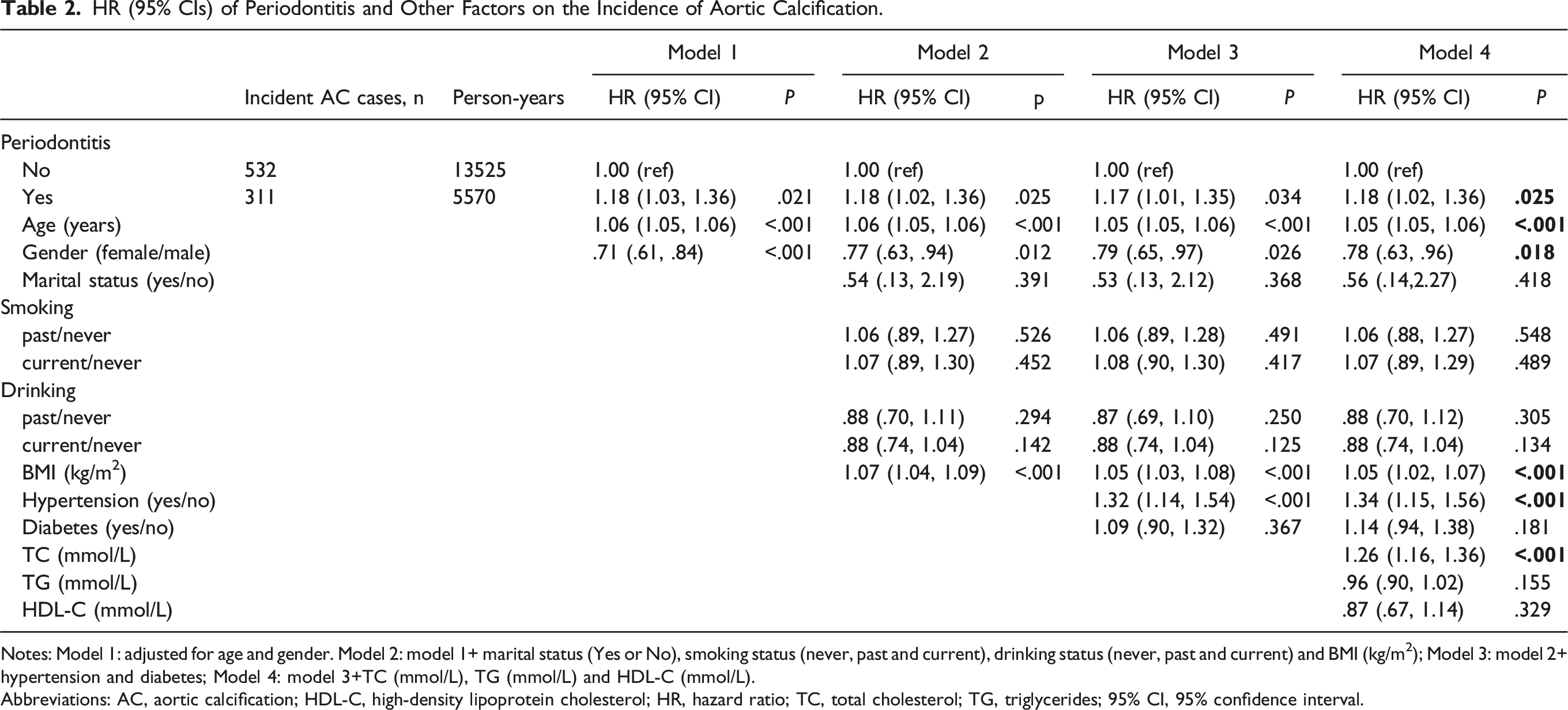
Notes: Model 1: adjusted for age and gender. Model 2: model 1+ marital status (Yes or No), smoking status (never, past and current), drinking status (never, past and current) and BMI (kg/m2); Model 3: model 2+ hypertension and diabetes; Model 4: model 3+TC (mmol/L), TG (mmol/L) and HDL-C (mmol/L).
Abbreviations: AC, aortic calcification; HDL-C, high-density lipoprotein cholesterol; HR, hazard ratio; TC, total cholesterol; TG, triglycerides; 95% CI, 95% confidence interval.
Subgroup Analyses of Variables in Relation to Periodontitis with the Incidence of Aortic Calcification.
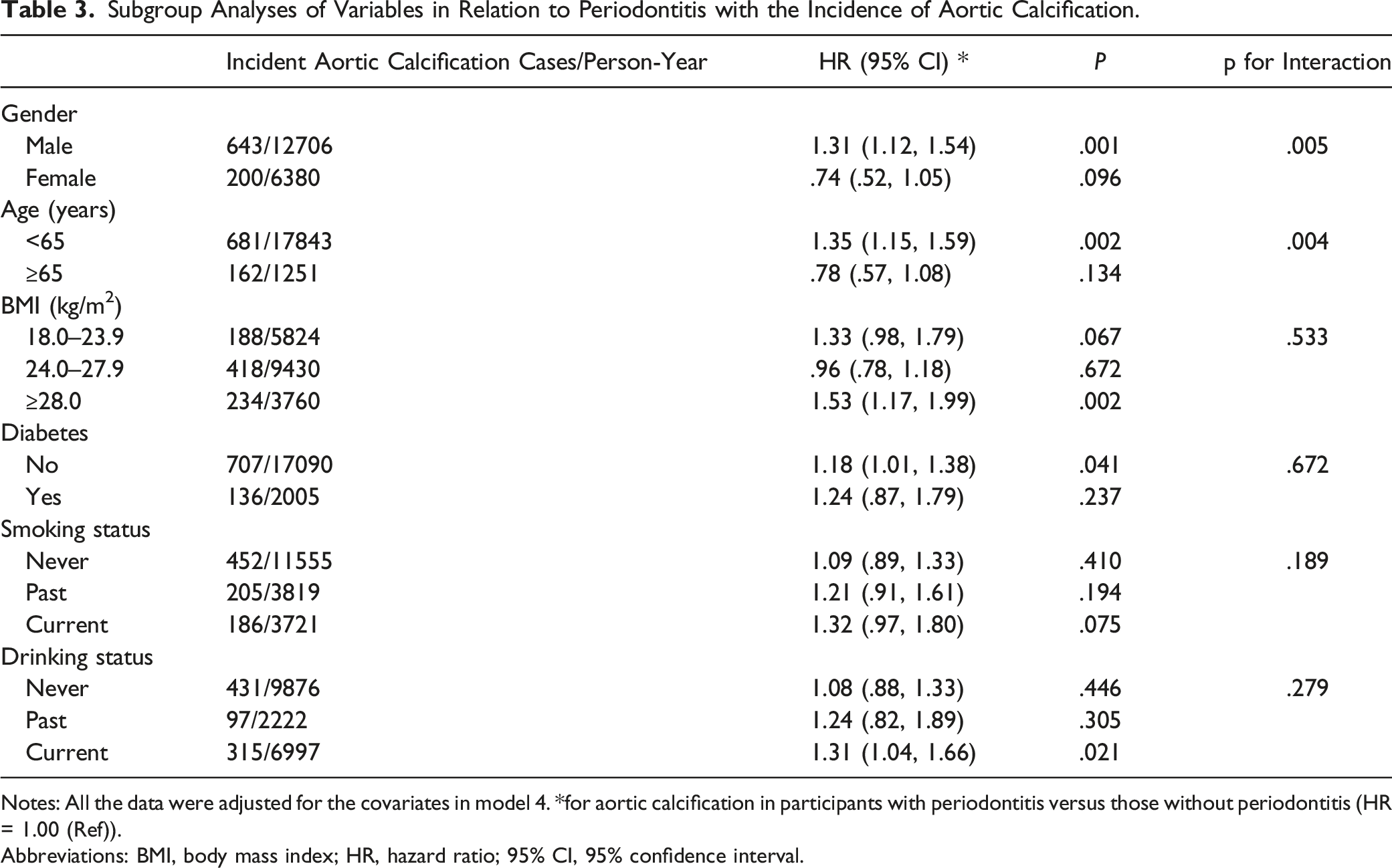
Notes: All the data were adjusted for the covariates in model 4. *for aortic calcification in participants with periodontitis versus those without periodontitis (HR = 1.00 (Ref)).
Abbreviations: BMI, body mass index; HR, hazard ratio; 95% CI, 95% confidence interval.
Discussion
This cohort study investigated the association of periodontitis and the occurrence of AC among Chinese adults. Our results showed that individuals with periodontitis had a higher risk of developing AC compared with those without periodontitis, especially among those who were males and aged <65 years.
Comparisons with Other Studies
There is a limited number of studies investigating the relationship between presence of periodontitis and AC. It has been established that periodontal disease is an independent predictor of intracardiac calcification. 27 In the latest consensus report on periodontitis and CVD, 28 it was noted that strong epidemiological evidence has shown that periodontitis increased the risk of future CVD. In the American Heart Association statement, 29 it was noted that observational studies supported the association between periodontitis and the development of CVD. In the first systematic review and meta-analysis there was a positive association between periodontitis and carotid artery calcification. 30 Similar findings have been obtained in clinical and animal studies.31,32 In our prospective cohort study conducted in a non-selected population of 6059 individuals, periodontitis was associated with the occurrence of AC (HR and 95% CI: 1.18 (1.02–1.36), P = .025).
Potential Mechanisms
Although the potential mechanisms involved in the association between periodontitis and the AC remain unclear, based on the current findings, we hypothesize that inflammation may be the key underlying mechanism. 27 Nucleotide-binding oligomerization domain (NOD), leucine-rich repeat (LRR), and pyrin domain-containing protein 3 (NLRP3) and C reactive protein (CRP) may be biomarkers of periodontitis and vascular calcification.29,33 Firstly, periodontitis pathogens such as Porphyromonas gingivalis (P. gingivalis) can cause inflammation and periodontal destruction, 34 and NLRP3 is activated as an important inflammatory agent of the immune response when the organism is attacked by pathogens. This induces the maturation and release of pro-inflammatory cytokines such interleukin-1 (IL-1) and IL-8 and their accumulation locally in the gingiva,29,35 which are responsible for recruitment of cells involved in the innate and acquired immune response and inflammatory process. 36 Studies have shown that the gingival sulcus is the main source of oral bacteria and blood entry point, 37 and when cytokines enter the circulation from the gingival sulcus, they may invade aortic vascular wall smooth muscle cells and aortic endothelial cells. IL-1β induces the secretion of RANKL (receptor activator of NF-κB ligand) and activates osteoclasts, 38 causing a series of inflammatory responses and producing the inflammatory marker CRP, 29 allowing the recoding of vascular smooth muscle cells (VSMCs) towards an osteoblast-like phenotype, and VSMCs secrete bone-associated matrix proteins,39,40 which cause vascular wall calcification and vascular lesions.30,41 However, the inflammatory markers mentioned above were not measured and these mechanisms could not be verified in this study. More studies are needed to confirm these hypotheses.
Second, membrane vesicle derived from P. gingivalis, increased the expression of the bone markers alkaline phosphatase (ALP), collagen type I alpha 1(ColIA1), and osteocalcin (OC) of aortic smooth muscle cells from mice by activating the osteogenic and runt-related transcription factor 2, and subsequently induced calcification. 42 As systemic spread of P. gingivalis and its invasion of the aorta were demonstrated in an infected mice model, 43 where the periodontal bacteria may directly stimulate aortic smooth muscle cells and promote AC. Activation of NLRP3 inflammatory vesicles accelerates vascular calcification in vivo and in vitro, and it plays a key role in VSMCs calcification. 33 Patients with periodontitis have high serum CRP levels, 44 and evidence from randomized clinical trials suggests that periodontal treatment reduces the number of pathogenic microorganisms in plaque and decreases systemic levels of interleukins, CRP, and E selectin. 45 Although these studies suggest a possible mechanism of association between periodontitis and AC, definitive experimental studies are lacking and therefore more epidemiological studies and experimental studies are needed.
Age and Gender Differences
Stratified analyses indicated that the positive association between periodontitis and AC varied in different age groups. In terms of age, we observed that individuals with periodontitis in the younger group were more likely to develop AC compared with those age >65 years and the interaction between periodontitis and age was statistically significant (pinteraction = .005). Age has been confirmed to be an important risk factor for AC, possibly resulting from the progression of atherosclerotic and lesions becoming calcified as age increased.16,46 Our findings may be consistent with previous findings, probably due to older age of the excluded participants with or lack of data with a diagnosis of AC at baseline than the participants included in the present study (51.2 ± 15.4 vs 48.8 ± 10.8 years).
Moreover, our data suggested that men with periodontitis had a higher risk for the occurrence of AC than women and the significant interaction between periodontitis and gender was also demonstrated (pinteraction = .004). Previous studies have revealed that men have a higher overall prevalence of atherosclerotic disease compared with women and the average age for the appearance of vascular calcification in man was much younger than in women.46,47 The possible mechanism could be different levels of estrogen among males and females, as estrogen plays a role in regulating lipid metabolism, 48 which may further affect the process of atherosclerosis. However, further studies are needed to explore the potential mechanisms involved.
Strengths and Limitations
The present study included a relatively large population containing a considerable proportion of periodontitis patients to investigate its relationship with AC. However, some limitations need to be mentioned. First, the strength of causal association still needs further confirmation due to the relatively short follow-up duration. Second, the study population consisted of individuals who received health check-ups at Xiaotangshan hospital in Beijing, China, and most of them were civil service officers, which may limit the extrapolation of our findings to the general population. Third, as oral examination for periodontitis diagnosis was only performed at baseline, the development of periodontitis during the follow-up period was not considered and this may influence the strength of the association between periodontitis and AC. Moreover, AC was only identified by chest CT scan. The detection of AC may be limited by the sensitivity of CT examination and the possibility of invisible imaging manifestations in the early stage of AC. In addition, it has been suggested that the number of tooth loss may influence the association between periodontal disease and CVD; unfortunately, this variable was not included in our current study because it was not collected in the database. Finally, although a variety of confounding factors in the relationship between periodontitis and AC have been controlled in our analyses, there is a possibility of residual confounders.
Conclusion
This cohort study suggested that periodontitis was positively associated with AC risk in Chinese adults, especially in men and those aged <65 years. More studies with longer follow-up duration and larger sample size are needed to confirm this relationship.
Supplemental Material
Supplemental Material - Association between Periodontitis and Aortic Calcification: A Cohort Study
Supplemental Material for Association between Periodontitis and Aortic Calcification: A Cohort Study by Ying-lin Yu, Jun-rong Ma, Shu-na Li, Min-qi Liao, Shan Xu, Hong-en Chen, Shu-hong Dai, Xiao-lin Peng, Dan Zhao, Yan-mei Lou, Xiao-xuan Yu, Xu-ping Gao, Yan-hua Liu, Jun Liu, Xing-yao Ke, Zhao Ping, Li Wang, Chang-yi Wang, and Fang-fang Zeng in Angiology
Footnotes
Acknowledgments
We thank all participants from the Beijing Xiao Tang Shan Hospital and the Shenzhen Nanshan Centre for Chronic Disease Control for their valuable contributions.
Author Contributions
Fang-fang Zeng and Chang-yi Wang contributed to the study concept, design, data acquisition, analysis, interpretation and critically revised manuscript. Ying-lin Yu, Jun-rong Ma and Shu-na Li wrote the first draft of the manuscript, and contributed to conception, the data acquisition, analysis, interpretation and critically revised manuscript. Min-qi Liao, Shan Xu and Hong-en Chen contributed the study conception and design, and data acquisition, analysis, and interpretation. Shu-hong Dai, Xiao-lin Peng, Dan Zhao, Yan-mei Lou, Xiao-xuan Yu, Xu-ping Gao, Yan-hua Liu, Jun Liu, Xing-yao Ke, Zhao Ping, and Li Wang contributed to the study conception and design, and/or data acquisition, analysis, and interpretation of manuscript. All authors participated in critically revising the manuscript, agreed to be accountable for all aspects of work and approved the final version of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the National Natural Science Foundation of China (grant number: 81602853).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.