
Abstract
Mesenteric artery dissection (D) and wall-thickening (WT) are rare vasculopathies that can lead to serious complications. This is a single center analysis of all patients evaluated for mesenteric arterial (celiac, superior (SMA) and/or inferior mesenteric (IMA)) D and/or WT from January 1, 2000, to January 31, 2020 at our hospital. Among the 101 included patients, the average age was 55.6 ± 13.6 years, mostly affecting men (62%). There were 20 celiac artery D, 8 WT, 15 D with WT, 15 SMA D, 7 WT, 8 D with WT, one IMA D, two WT, and 25 with multiple arterial involvement. Primary etiologies included segmental arterial mediolysis (SAM) (n = 17), isolated D (n = 17), localized vasculitis of the gastrointestinal tract (LVGT) (n = 16), fibromuscular dysplasia (FMD) (n = 13), extension of thoracoabdominal aortic D (n = 12), and trauma (n = 12). Most (71%) patients presented with abdominal pain. Hypertension (55%), hyperlipidemia (33%) and tobacco use (31%) were prevalent. Management included conservative (22%), medical (47%), endovascular (19%), and/or open repair (12%) with high in-hospital survival (98%) and symptom relief (73%). Our paper complements the scarce literature addressing the diagnosis and management of rare mesenteric vasculopathies. Most patients improved with conservative management, reserving endovascular or surgical interventions for symptomatic patients with more complicated presentations.
Introduction
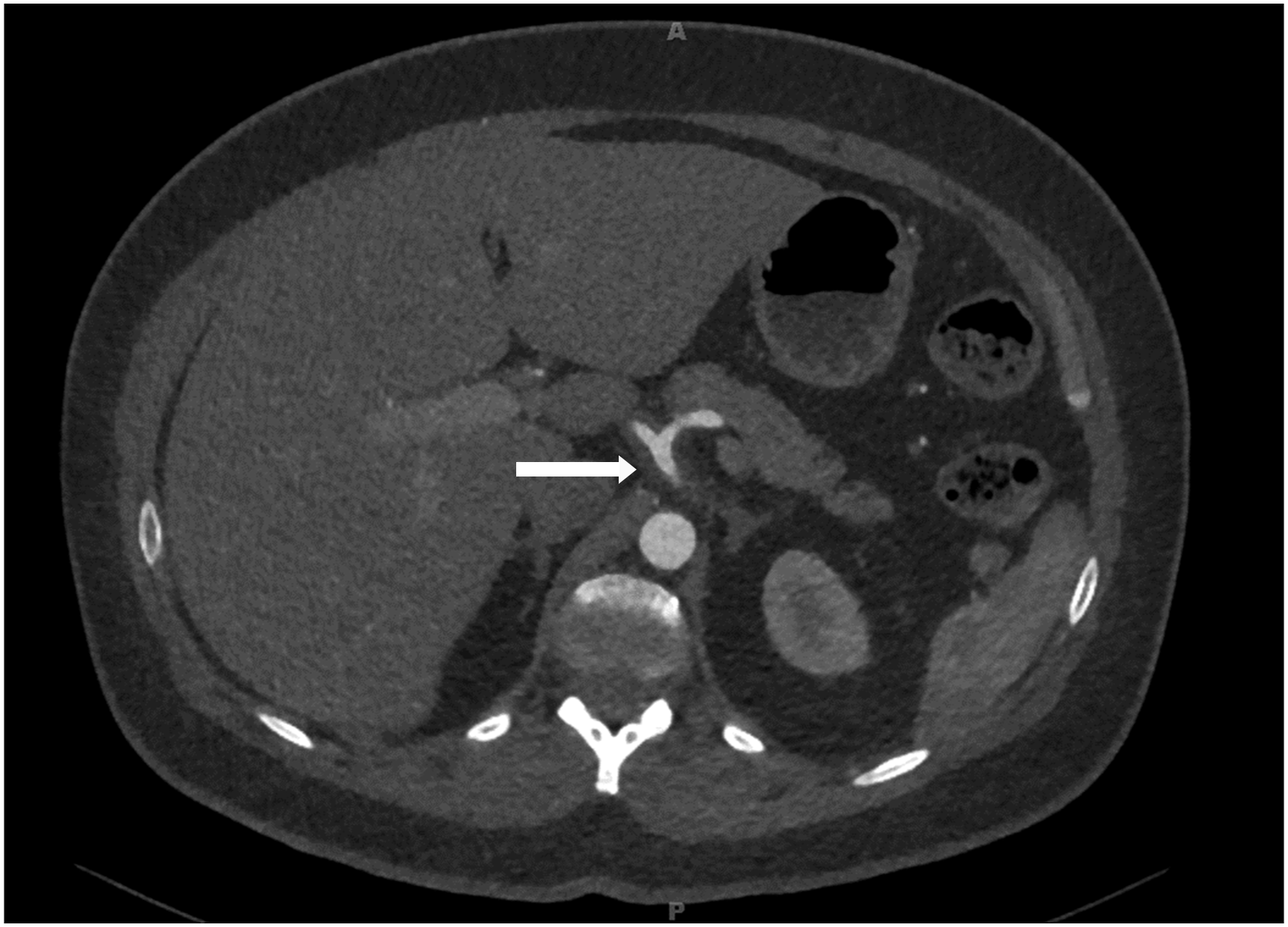
Mesenteric artery dissection (D) (Figure 1) and wall thickening (WT) (Figure 2) are uncommon vasculopathies caused by different etiologies. Although atherosclerosis is the most common underlying etiology, such arterial pathologies can also be nonatherosclerotic in nature.
1
Nonatherosclerotic mesenteric arteriopathies have distinct pathophysiology, and require different diagnostic and management approach. This heterogenous group of conditions include systemic or localized vasculitis, including systemic or localized vasculitis, noninflammatory disorders such as fibromuscular dysplasia (FMD) and segmental arterial mediolysis (SAM), and genetic connective tissue disorders such as vascular Ehlers–Danlos syndrome (vEDS) or Loeys–Dietz syndrome (LDS). Though uncommon, arteriopathies associated with these conditions can have considerable clinical significance. For example, localized vasculitis of the gastrointestinal tract (LVGT) may have a mortality rate of nearly 40%.
2
Although half of patients with SAM may present with intraabdominal bleeding, a mortality of 50% has been reported.3,4 Furthermore, 80% of patients with vEDS will experience a major vascular complication by the age of 40 years.
5
CT angiographic sagittal image showing celiac artery dissection in a patient with biopsy-confirmed segmental arterial mediolysis. CT angiographic transverse image showing celiac artery wall thickening in a patient with clinically-confirmed localized vasculitis of the gastrointestinal tract.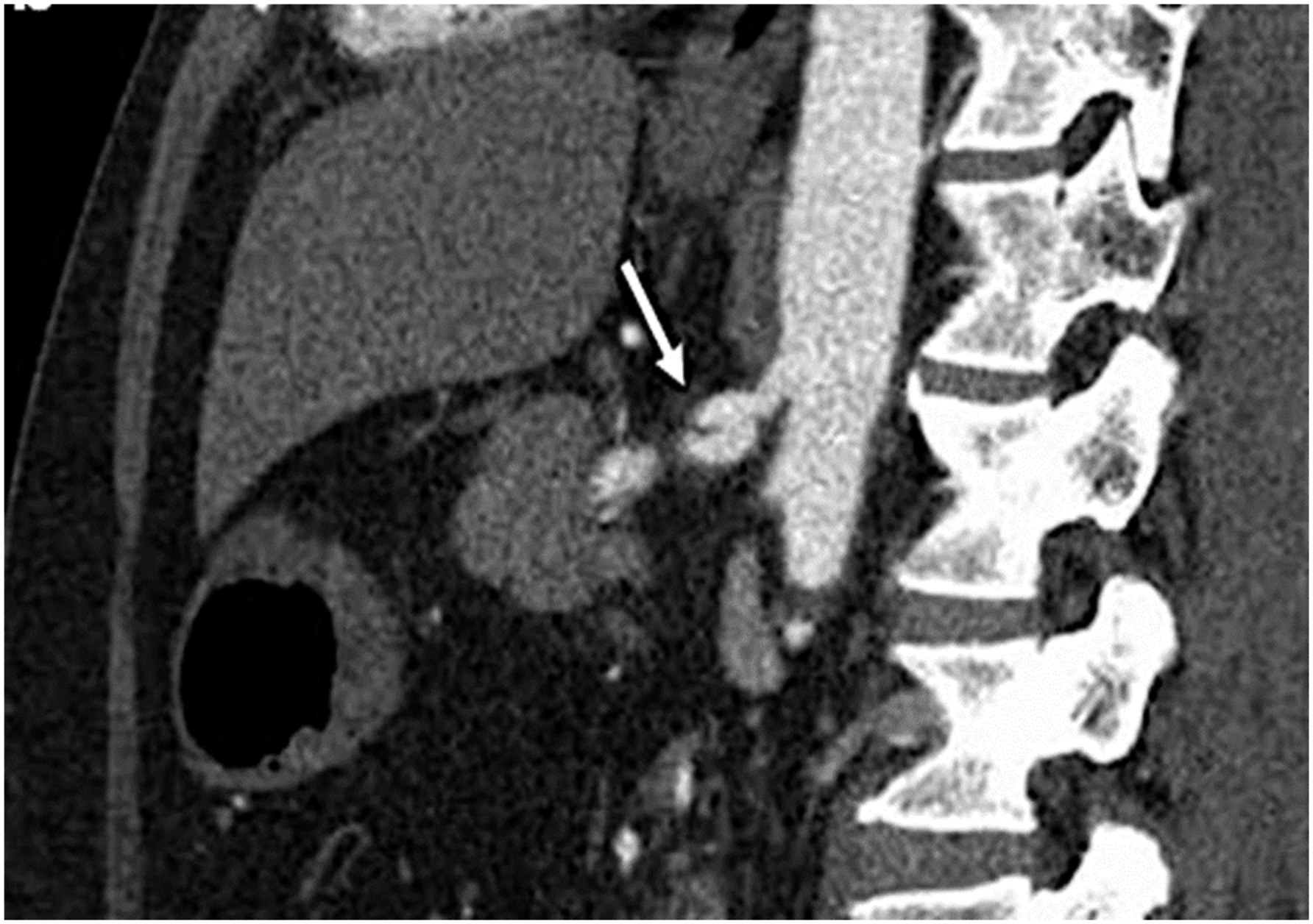
There is no consensus as to the appropriate diagnosis and management of these patients. Furthermore, current literature is scant, and to our knowledge, there are no published articles addressing mesenteric artery D and/or WT collectively. Therefore, we present our center’s experience with 101 cases of mesenteric artery D and/or WT, and discuss the various etiologies, clinical presentation, management strategies, and outcomes.
Patients and Methods
Patient Identification
Charts of 1924 patients who presented at Abbott Northwestern Hospital between January 1, 2000 and January 31, 2020 were identified based on search criteria including patients with current procedural terminology (CPT) codes for mesenteric, celiac, SMA, or IMA dissection, wall thickening, inflammation, vasculitis, arteriopathy, or vasculopathy. Patients were included if they were 18 years or older, and had radiographic imaging identifying D and/or WT (≥3 mm) involving the celiac, superior mesenteric, and /or inferior mesenteric arteries.
Data Collection
Baseline data collected included age at diagnosis, gender, comorbid conditions (including diabetes mellitus [DM], hypertension [HTN], hyperlipidemia, current or history of tobacco use, peripheral artery disease [PAD], and coronary artery disease [CAD]), presenting symptoms, vital signs, laboratory values, and imaging findings. Laboratory values and imaging results from follow-up visits were also collected if available. Data for other vascular involvement (e.g., cerebrovascular) were not collected since it is out of scope for this project. Furthermore, most patients had no neurological symptoms to warrant cerebrovascular images.
The Allina Institutional Review Board approved this study. Informed consent for research review of the medical record was in accordance with Minnesota state law.
Study Definitions
An erythrocyte sedimentation rate (ESR) >15 mm/h (for males <50 years of age), >20 mm/h (for males >50 and females <50 years of age), >30 mm/h (for females >50 years of age), and a C-reactive protein (CRP) level greater than .50 mg/dL were considered abnormal. For ESR and CRP laboratory data at follow-up, stable was defined if values were unchanged from those at presentation (variation in ESR <5 mm/h or in CRP <1 mg/dL), normalized as a decrease of a previously elevated value placing it within the normal range, improved as a decrease of an elevated value but still elevated, and worsened as an increase of an elevated value. Follow-up for ESR and CRP data were defined as the most recent hospital encounter or clinic visit during which ESR and CRP were measured.
Arterial WT measurements were performed on axial images of computed tomography angiography (CTA) by the first author (NS). Abnormal arterial WT was diagnosed if thickness was equal to or more than 3 mm.6,7 At follow-up, imaging outcome was classified as improved, worsened, or unchanged. Improvement was defined as a ≥1 mm decrease in WT, worsened as a ≥1 mm increase in WT, and unchanged as a <1 mm change in WT.
Follow-up was defined as the most recent hospital encounter or clinic visit during which imaging of the artery was performed. At follow-up, symptoms were classified as improved if they were eased or alleviated, as worsened if they recured or new related symptoms developed, or as unchanged.
Statistical Methods
Descriptive statistics are displayed as median and 25th and 75th percentiles for continuous variables; number and percentage with characteristics are given for categorical variables. Formal analyses were not performed, given the small sample sizes within groups.
Diagnosis
All cases were reviewed by a vascular medicine specialist to confirm final diagnoses according to the diagnostic criteria listed below. The diagnostic criteria are based on consensus committees or expert opinion.1,3
Segmental arterial mediolysis was considered if an imaging study revealed evidence of D and/or aneurysm with or without organ infarction in multiple mesenteric and/or renal arteries with exclusion of other vasculopathies, such as FMD, LVGT, or connective tissue disorders, and no significant concurrent arterial WT (<3 mm) or elevation of inflammatory markers (ESR <20 mm/h and CRP <5 mg/dL).3,8-10
Isolated D was defined as a D involving a single mesenteric artery in patients who did not meet the criteria for other vasculopathies.
Localized vasculitis of the gastrointestinal tract is a single-organ vasculitis in which one or more gastrointestinal (GI) arteries shows imaging findings of smooth segmental narrowing, dilation, occlusion, or aneurysm. 2 Localized vasculitis of the gastrointestinal tract was considered in patients with recently acquired GI manifestations (including abdominal pain, nausea or vomiting, diarrhea, weight loss, and melena), either histopathological evidence of vasculitis in a GI specimen or high-probability angiographic findings, and significant WT (≥3 mm). Diagnosis requires the absence of any vessel changes consistent with atherosclerosis, FMD, or SAM 2 and the exclusion of systemic vascular inflammation at the time of diagnosis and throughout a follow-up period of 6 months. 11 Inflammatory markers can be normal or elevated.
Prior to the publication of the new criteria proposed by the “First International Consensus of the diagnosis and management of fibromuscular dysplasia,” the diagnosis of FMD was considered if imaging findings revealed stenosis, occlusion, D, or aneurysm in the renal and/or extracranial cerebrovascular arteries with concurrent string of beading appearance (multifocal FMD) or circumferential stenosis (focal FMD) in setting of no aortic involvement and normal inflammatory markers. 12 The new criteria defines FMD as an idiopathic, segmental, nonatherosclerotic, and noninflammatory disease of the musculature of arterial walls, leading to stenosis of small and medium-sized arteries. 13
Extension of thoracoabdominal aortic D was defined as a D of the aorta which extended into one or more of the mesenteric arteries.
Trauma was considered as the underlying etiology in patients who had a history of a trauma to the area of the diagnosed D or WT.
Both polyarteritis nodosa and granulomatosis with polyangiitis are necrotizing vasculitides that can involve mesenteric vasculature. Diagnosis was made by a certified rheumatologist based on the American College of Rheumatology criteria.6,14
Median arcuate ligament syndrome was considered based on a combination of symptoms (e.g., postprandial abdominal pain and weight loss), CTA findings of celiac artery compression by the median arcuate ligament with post-stenotic dilation or aneurysm, and increased velocity during exhalation compared with inhalation in an ultrasound (US).15,16
The American College of Rheumatology criteria was used to diagnose Takayasu’s arteritis (TA). Patients had to meet at least three of the following criteria: age of onset ≤40 years; claudication of extremities; decreased pulsation of one or both brachial arteries; difference of at least 10 mmHg in systolic blood pressure between the arms; bruit over one or both subclavian arteries or abdominal aorta; and arteriographic narrowing or occlusion of the aorta, primary branches or larger arteries in the proximal upper or lower extremities not secondary to arteriosclerosis, FMD, or any other cause.17,18
vEDS (type IV) was diagnosed in patients who met Villefranche criteria and were confirmed by genetic testing.19,20
Loeys–Dietz Syndrome (LDS) was considered in patients with hypertelorism, a bifid uvula and/or cleft palate, and tortuous arteries with widespread aneurysm. Diagnosis was confirmed by genetic testing. LDS type 3 is characterized more specifically by aortic and arterial aneurysms and dissections, as well as early-onset osteoarthritis.21,22
Marfan syndrome was diagnosed if the patient met revised Ghent nosology criteria. Considerations included a positive family history, aortic root dilation or D, ectopia lentis, a causal fibrilin (FBN)1 mutation, and presence of various systemic features. 23
Systemic Lupus Erythematosis (SLE) is a complex, multisystemic autoimmune disease that has frequent vascular involvement. Diagnosis of Lupus Vasculitis was made by a certified rheumatologist based on the most recent European League Against Rheumatism/American College of Rheumatology criteria. 24
Giant Cell Arteritis was considered in patients with age ≥50 years who presented with new headaches, abrupt onset of visual disturbances, jaw claudication, unexplained fever, anemia, or high ESR, and/or CRP. Diagnosis was made by a certified rheumatologist based on the American College of Rheumatology criteria. 25
Results
Study Population
Out of the total 1924 patients, twenty-two were excluded before chart review due to pregnancy (9), no consent for research (9), or being treated outside of the study period (4). The remaining 1902 charts were reviewed: 1639 were excluded for lack of D or WT in the arteries of interest, 157 for diagnosed atherosclerosis, 4 for missing information, and 1 for a complex, unclear etiology. The remaining 101 patients were grouped based on diagnoses into SAM, isolated D, LVGT, FMD, extension of thoracoabdominal aortic D, trauma, polyarteritis nodosa (PAN), median arcuate ligament syndrome (MALS), TA, vEDS, LDS, Marfan syndrome, lupus vasculitis, systemic vasculitis (e.g., granulomatosis with polyangiitis (GP)), and giant cell arteritis (Figure 3). Mesenteric artery chart review methods. Abbreviations: D: dissection, FMD: fibromuscular dysplasia, LVGT: localized vasculitis of the gastrointestinal tract, MALS: median arcuate ligament syndrome, PAN: polyarteritis nodosa, SAM: Segmental arterial mediolysis, WT: wall thickening.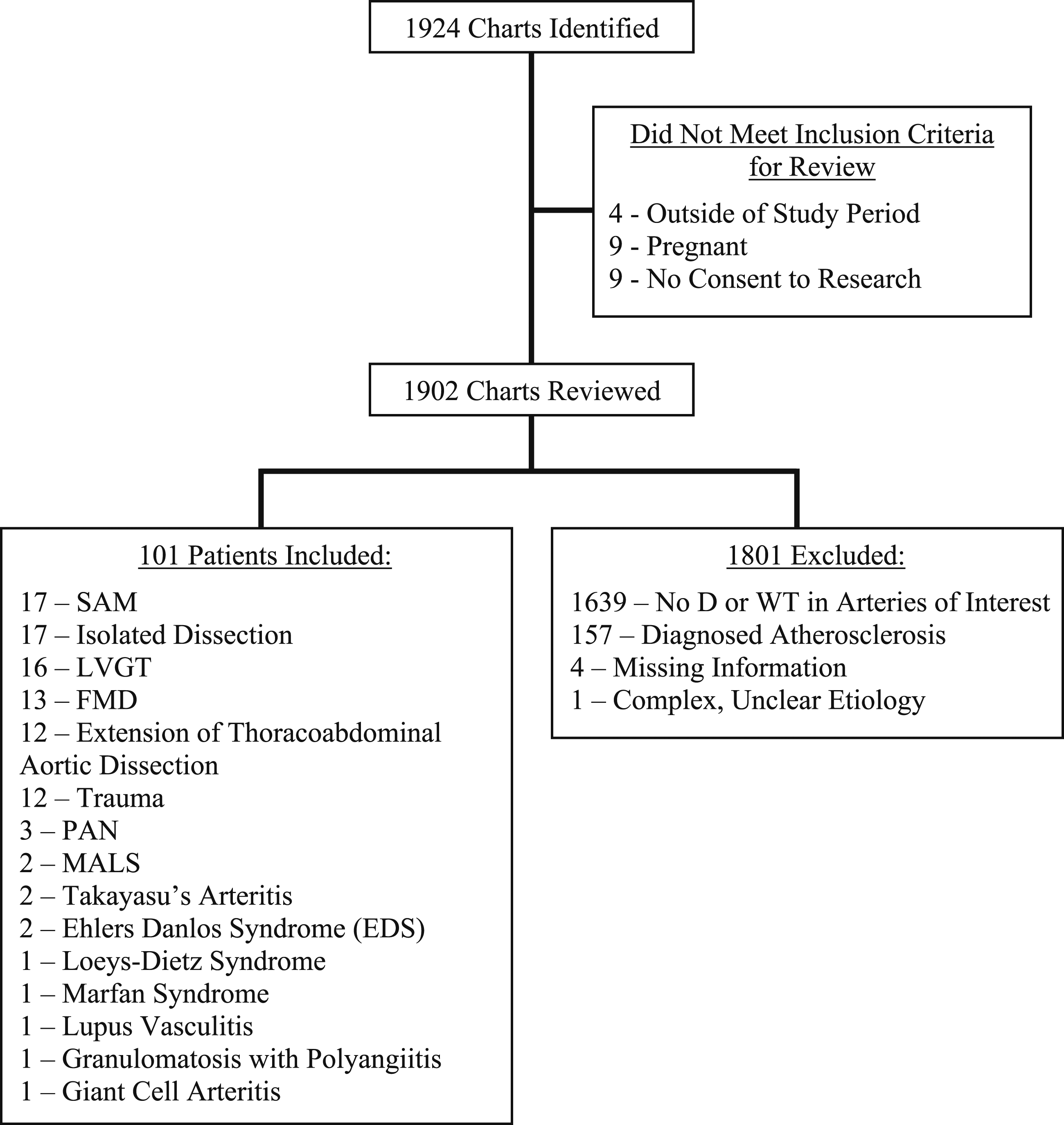
Patient demographics.
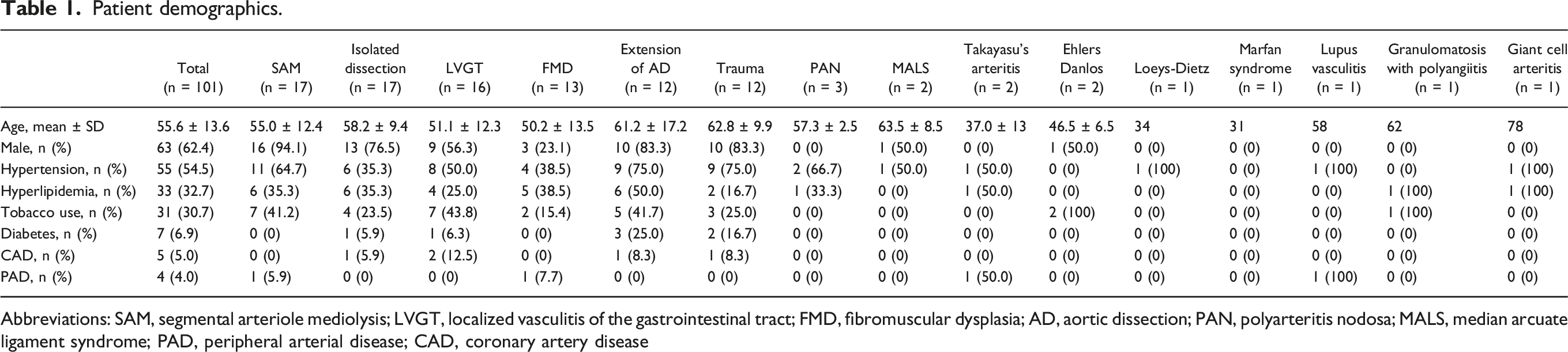
Abbreviations: SAM, segmental arteriole mediolysis; LVGT, localized vasculitis of the gastrointestinal tract; FMD, fibromuscular dysplasia; AD, aortic dissection; PAN, polyarteritis nodosa; MALS, median arcuate ligament syndrome; PAD, peripheral arterial disease; CAD, coronary artery disease
Presenting Findings and Symptoms
Presenting symptoms.
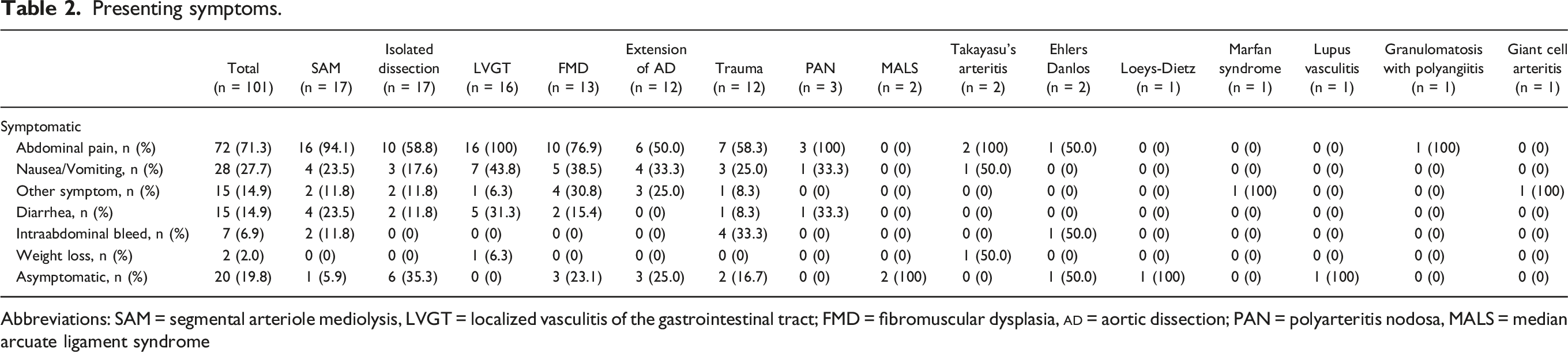
Abbreviations: SAM = segmental arteriole mediolysis, LVGT = localized vasculitis of the gastrointestinal tract; FMD = fibromuscular dysplasia,
Vital Signs, Laboratory Findings, and Imaging
Vital signs, laboratory findings, and imaging modality.
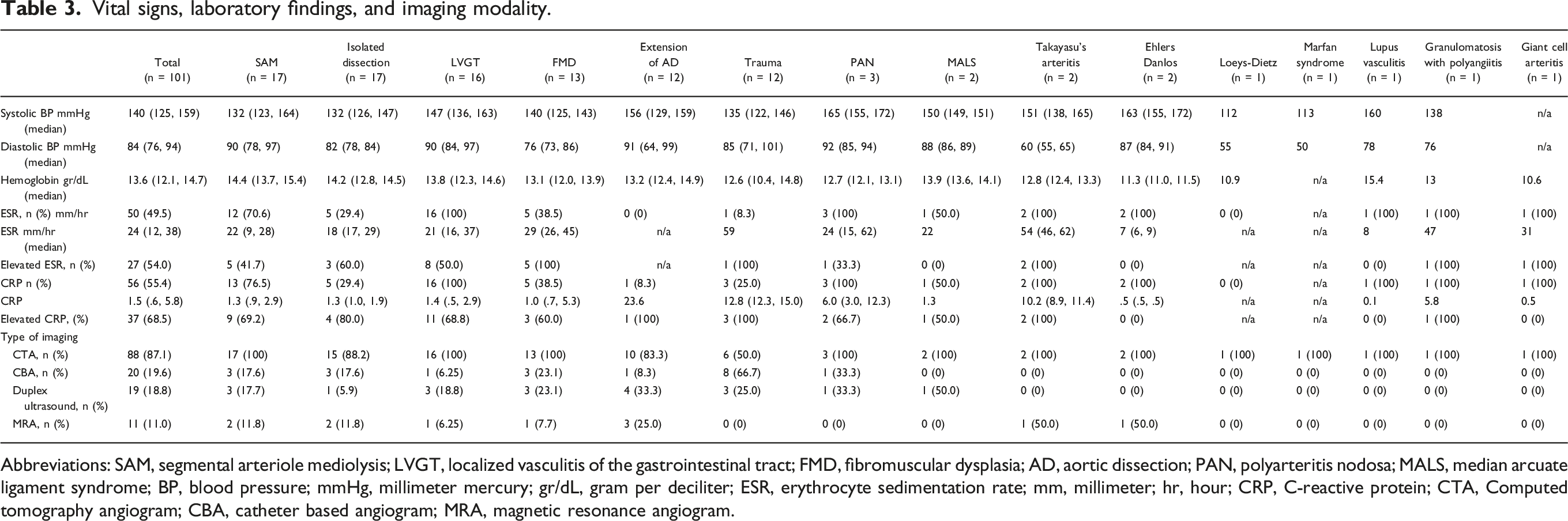
Abbreviations: SAM, segmental arteriole mediolysis; LVGT, localized vasculitis of the gastrointestinal tract; FMD, fibromuscular dysplasia; AD, aortic dissection; PAN, polyarteritis nodosa; MALS, median arcuate ligament syndrome; BP, blood pressure; mmHg, millimeter mercury; gr/dL, gram per deciliter; ESR, erythrocyte sedimentation rate; mm, millimeter; hr, hour; CRP, C-reactive protein; CTA, Computed tomography angiogram; CBA, catheter based angiogram; MRA, magnetic resonance angiogram.
Computed tomography angiography was the most frequently used method for diagnostic imaging (87.1%), followed by catheter-based angiography (CBA) (19.6%), duplex ultrasound (18.8%), and magnetic resonance angiography (MRA) (11.0%).
Anatomic Involvement
Anatomy distribution.
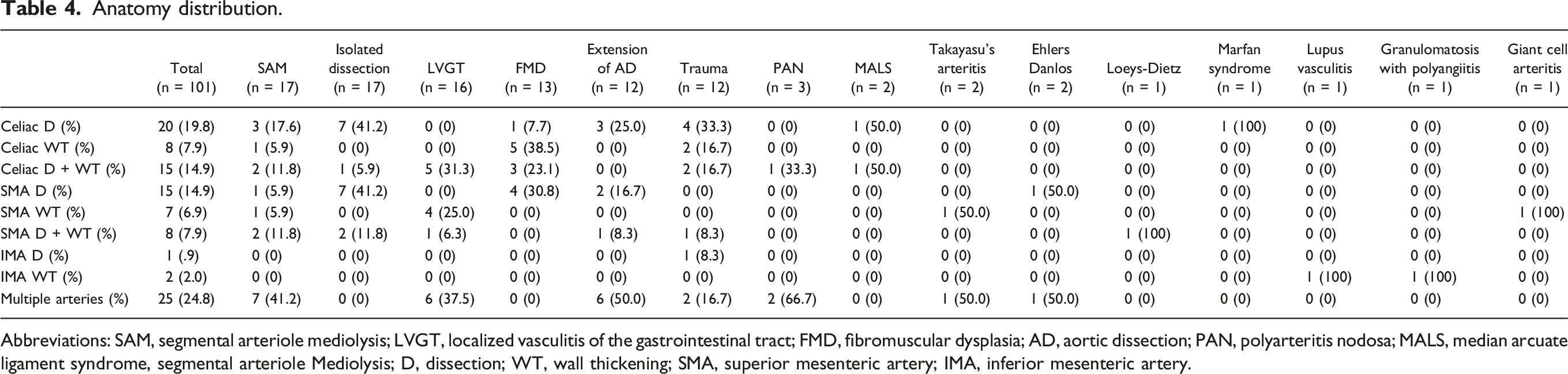
Abbreviations: SAM, segmental arteriole mediolysis; LVGT, localized vasculitis of the gastrointestinal tract; FMD, fibromuscular dysplasia; AD, aortic dissection; PAN, polyarteritis nodosa; MALS, median arcuate ligament syndrome, segmental arteriole Mediolysis; D, dissection; WT, wall thickening; SMA, superior mesenteric artery; IMA, inferior mesenteric artery.
Treatments and Outcomes
Treatment.
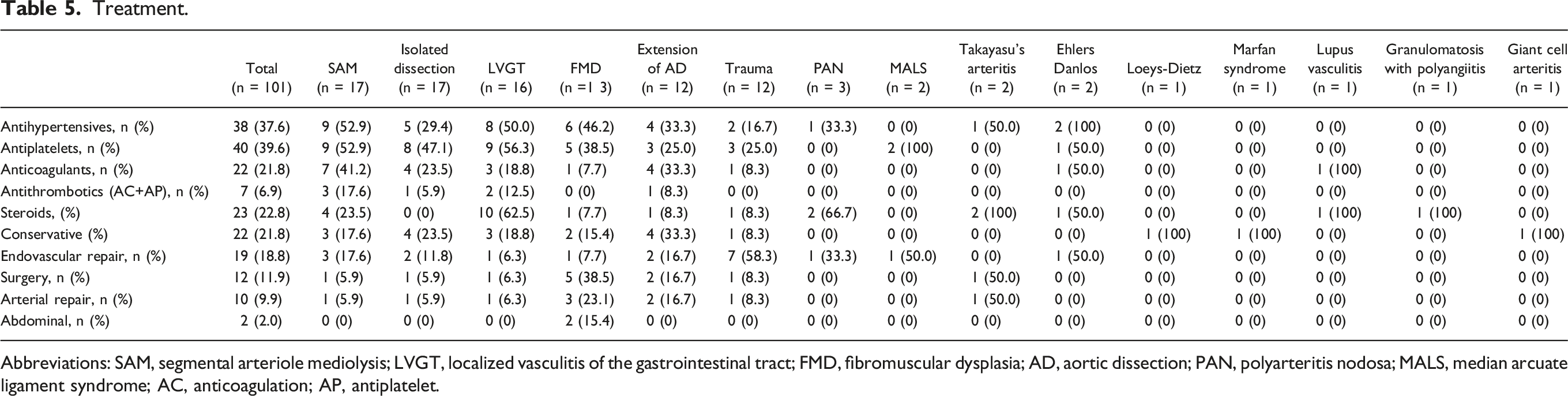
Abbreviations: SAM, segmental arteriole mediolysis; LVGT, localized vasculitis of the gastrointestinal tract; FMD, fibromuscular dysplasia; AD, aortic dissection; PAN, polyarteritis nodosa; MALS, median arcuate ligament syndrome; AC, anticoagulation; AP, antiplatelet.
Endovascular and Surgical Interventions.
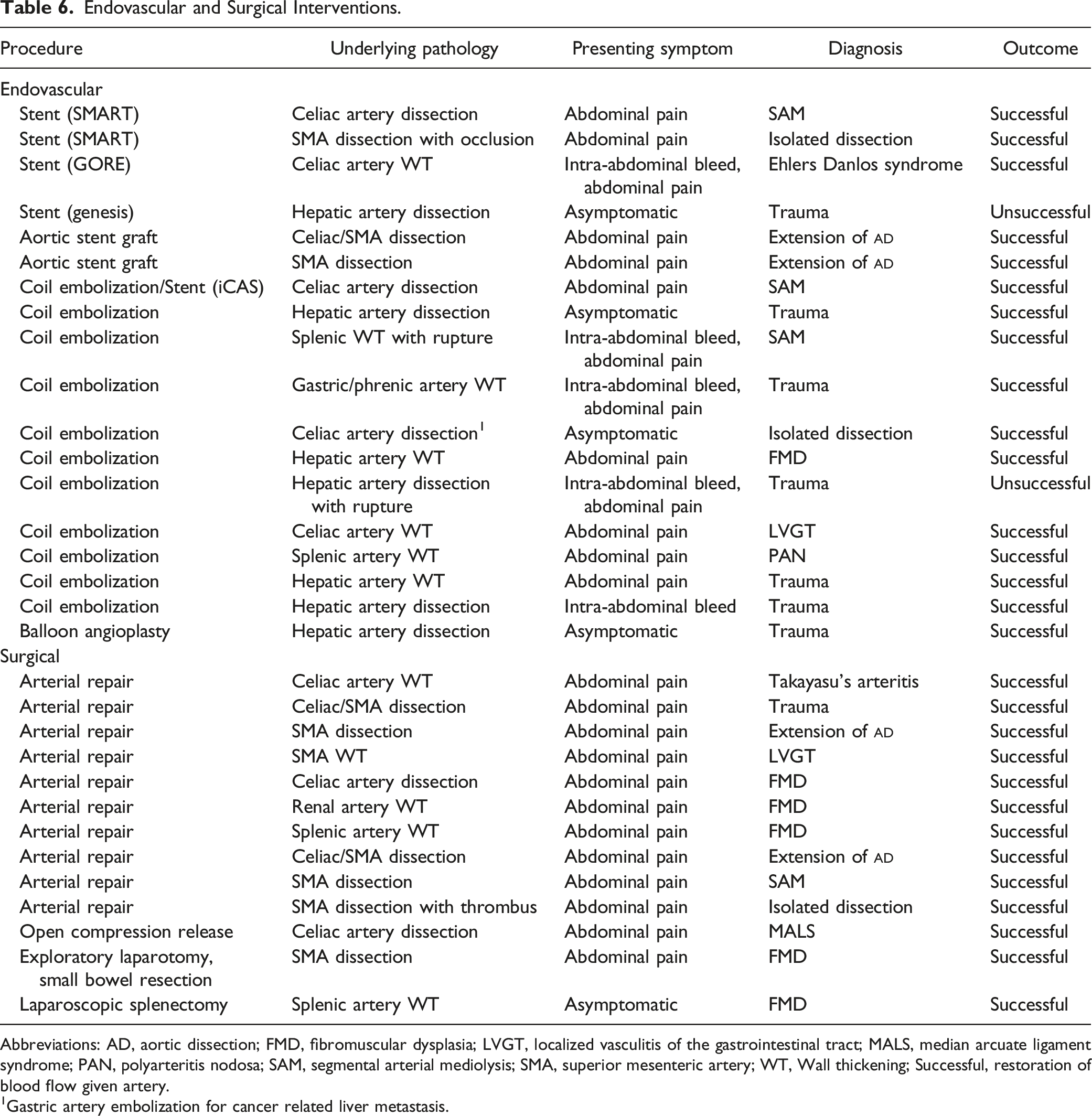
Abbreviations: AD, aortic dissection; FMD, fibromuscular dysplasia; LVGT, localized vasculitis of the gastrointestinal tract; MALS, median arcuate ligament syndrome; PAN, polyarteritis nodosa; SAM, segmental arterial mediolysis; SMA, superior mesenteric artery; WT, Wall thickening; Successful, restoration of blood flow given artery.
1Gastric artery embolization for cancer related liver metastasis.
More than a third of FMD patients (38.5%) required surgical treatment, of which 3 were arterial repairs and 2 were abdominal surgeries (exploratory laparotomy with small bowel resection, and laparoscopic splenectomy). Additionally, one patient (7.7%) underwent endovascular repair, and conservative treatment was used in 15.4%. The majority of LVGT patients were treated with prednisone (62.5%), followed by antiplatelets and antihypertensives (56.3% and 50.0%, respectively), anticoagulants (18.8%), and conservative treatment (18.8%). Among patients with SAM, antihypertensives were used in 52.9%, antiplatelets in 52.9%, anticoagulants in 41.2%, steroids in 23.5%, endovascular repair in 17.6%, and conservative treatment in 17.6%. Antiplatelet agents were the most used medications in patients with isolated D (47.1%), followed by antihypertensives (29.4%), anticoagulants (23.5%), and conservative treatment (23.5%). All patients with TA Lupus Vasculitis, and GP were treated with prednisone.
During a median follow-up period of 115 days (41, 461), the majority (73.3%) of patients had relief of their symptoms. All patients with PAN, TA, GP, and giant cell arteritis had symptom relief during their follow-up period. The majority of patients with SAM (88.2%), isolated D (64.7%), LVGT (93.8%), and FMD (92.3%) also experienced symptom relief. There was no death throughout the study duration.
Outcomes. 1
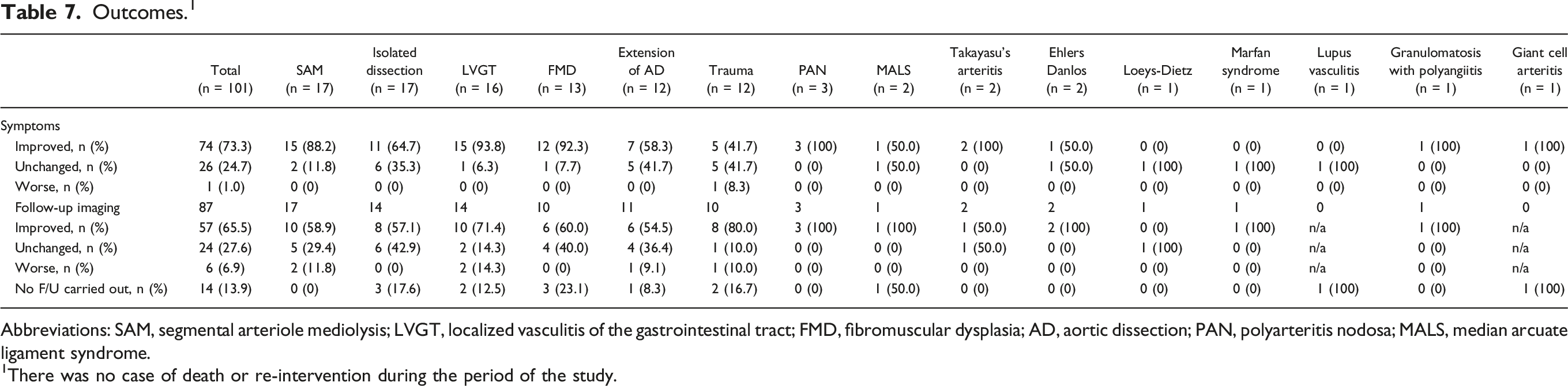
Abbreviations: SAM, segmental arteriole mediolysis; LVGT, localized vasculitis of the gastrointestinal tract; FMD, fibromuscular dysplasia; AD, aortic dissection; PAN, polyarteritis nodosa; MALS, median arcuate ligament syndrome.
1There was no case of death or re-intervention during the period of the study.
Discussion
This paper discusses our center’s experience with the diagnosis and management of this rare group of mesenteric vasculopathies. Our approach for the diagnosis of mesenteric arteriopathies is summarized in Figure 4. Our strategy for diagnosing nonatherosclerotic mesenteric artery vasculopathies. Abbreviations: CBC = complete blood count, LFT = liver function test, ESR = erythrocyte sedimentation rate, CRP = C-reactive protein, ANCA = antineutrophil cytoplasmic antibody, IgG4 = immunoglobulin G4, CT = computed topography, MRA = magnetic resonance angiography SAM = segmental arteriole mediolysis, LVGT = localized vasculitis of the gastrointestinal tract, FMD = fibromuscular dysplasia, PAN = polyarteritis nodosa, MALS = median arcuate ligament syndrome.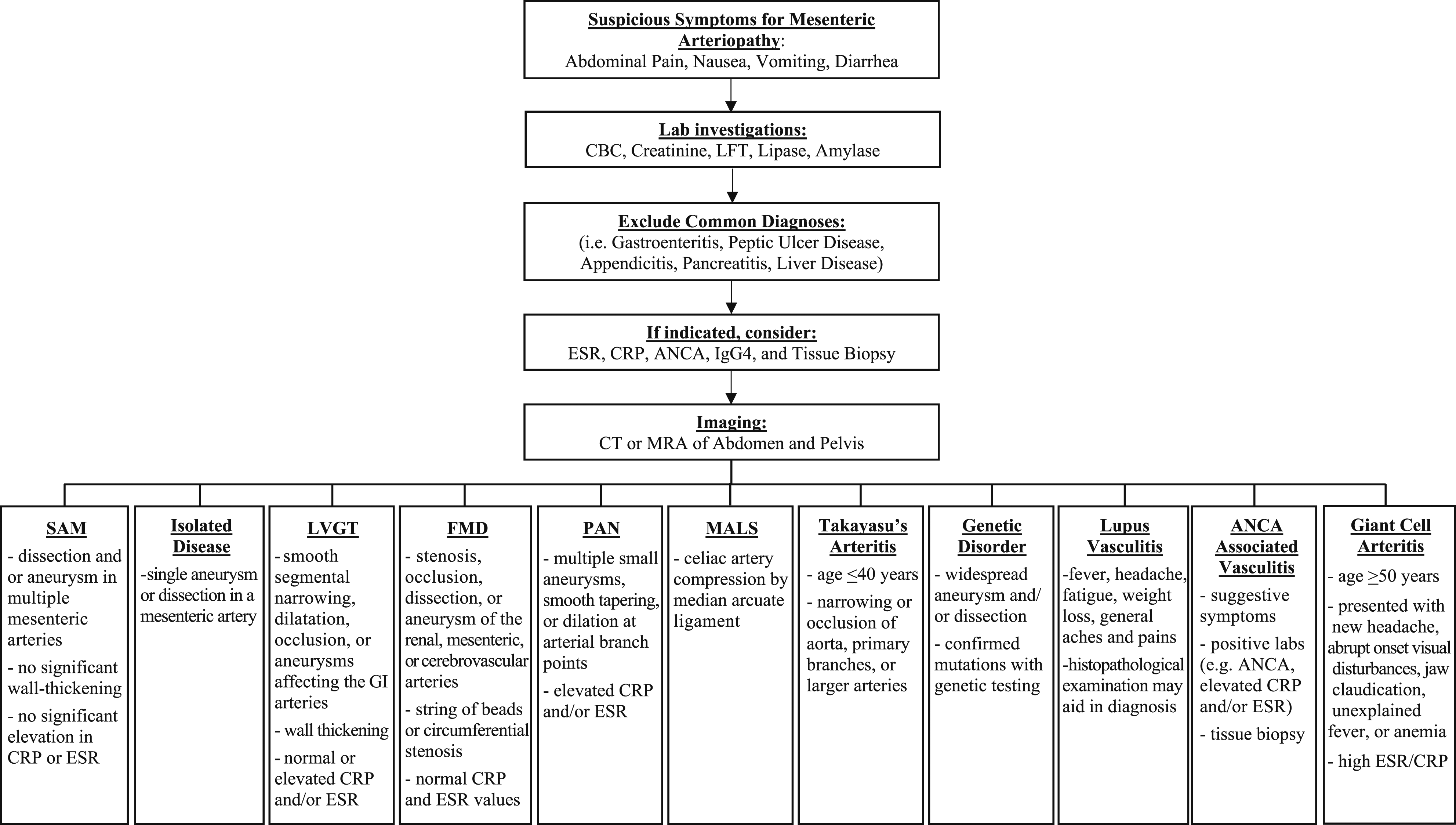
Consistent with previous studies, non-atherosclerotic mesenteric vasculopathies affect middle-aged adults.1,3 Furthermore, the incidence is higher in males (62.5%) which is consistent with our previous review that included patients with SAM. 3 However, inclusion of patients with both mesenteric and renal vasculopathies resulted in a higher (63.9%) female predominance that can be explained by higher numbers of FMD cases-a disease that predominantly affects females. 1 As expected, SAM, isolated D, and LGVT are among the most reported diagnoses based on included anatomical distribution and pathological findings. As we previously reported, nausea, vomiting and diarrhea are the most common presenting symptoms. Consistent with our previous report, HTN, hyperlipidemia, and tobacco abuse are prevalent co-morbidities. 1 Furthermore, CTA continues to be the imaging study of choice based on its availability and imaging quality for medium and small arteries.1,3 Although we did not encounter any contrast induced nephropathy in this study subjects, we still prefer MRA in patients with contrast allergies or those who need long-term surveillance.
Interestingly, 54% and 69% of patients who had ESR and CRP testing had elevated levels, respectively, regardless of the presence of underlying vasculitis, which raises concern regarding their sensitivity and specificity. Elevated ESR and CRP were also reported to be elevated in patients with SAM (33.3% and 68.6%, respectively) and in patients with other mesenteric and renal non-atherosclerotic vasculopathies (53.9% and 93.3%, respectively). Given the small sample size, it is not possible to link any connection between the outcome and steroid use.
It is unclear as to why some cases with mesenteric arterial D have concurrent WT, while others do not. We assume that concurrent WT is caused by intra-mural hematoma which may be determined by the site and severity of the D, and branches or layers involved. On the other hand, it is very hard to rule out a small D that could have been missed on the imaging study in cases with WT and no confirmed diagnosis of LVGT. Furthermore, D can also be a result of inflammation seen in patients with LGVT. Differential diagnoses can be extremely difficult and requires data collection from detailed history, physical exam, appropriate laboratory and imaging findings interpreted by a vascular specialist with an expertise in this field. Although figure 4 summarizes our differential diagnoses process, we call for more research to standardize diagnostic criteria for these arteriopathies that have similar symptomatic and imaging presentations.
Based on our and other centers experience, we continue to favor conservative and medical treatment including smoking cessation, bowel rest, hydration, and blood pressure and pain control, especially in asymptomatic patients and those with high risk of procedural complications.26,27 Consistent with limited available literature, in acute presentations with concurrent intra-abdominal bleed or end organ ischemia, we favor endovascular intervention over open repair, as these vessels are often friable making open repair difficult.1,28-30 Using this strategy, most of our patients showed improved symptoms and imaging findings.
Segmental Arterial Mediolysis
Epidemiology
94.1% of our SAM patients were male with a mean age of 55 years. Similarly, 67.8% of our previously reported 143 patients with SAM were male with a median age of 55 years. 3 Another systemic review of 85 patients reported a slight male predominance of 1.5:1 and average age in the mid-50s. 4 Other studies suggested that patients at all ages can be affected, but incidence is greatest in the fifth and sixth decades. 31
In this paper, most common anatomic involvement were multiple mesenteric arteries with different pathologies (41.1%), celiac artery D (17.6%) followed by celiac artery D with WT (11.8%), and SMA D with WT (11.8%). Arteries reported to be most affected in 143 patients with SAM were SMA (53.1%), hepatic (44.8%), celiac (35.7%), renal (25.9%), and splenic (24.5%). 3 Another systemic review of 85 patients showed that the celiac axis and branches are the most involved arteries, followed by the SMA axis and branches. 4
Clinical Presentation
94.1% our patients in this report presented with abdominal pain, compared with (74%) reported by Naidu et al. 32 Overall, the most common symptom at presentation in our previous SAM review was abdominal pain (79.7%), followed by intraabdominal bleeding (49.7%). 3
Treatment
There are currently no formal guidelines addressing the management of SAM.3,33 However, it is important to rule out other rheumatologic disorders as anti-inflammatory and immunosuppressive medications are not effective in SAM. 31 Based on findings from our previous report, we favor supportive and medical management for patients with SAM. Coil embolization was the most reported interventional technique.3,4
Most of our symptomatic patients with SAM in this paper and previous review experienced symptom relief after treatment (88.2% and 90.6%, respectively). 3 Although our previous review reported a mortality rate of 7%, Shenouda et al. reported a slightly higher rate of 26%, though 13 of the 21 deaths occurred prior to intervention. 4 This can be explained by improved sensitivity and specificity of the diagnostic criteria used to distinguish SAM from more fatal diseases such as connective tissue or vasculitis disorders.
Localized Vasculitis of the Gastrointestinal Tract
Epidemiology
There is limited data regarding the diagnosis and management of LVGT. 34 To our knowledge, the present report represents the second largest case series of LVGT, with 16 patients diagnosed. Nine of these patients (76.5%) were male with an average age of 51 years. The celiac artery was the most commonly affected (68.8%), followed by the SMA (62.5%) and IMA (6.3%). These findings differ slightly from the largest case series of 18 LVGT patients by Salvarani et al. in which females were more predominant (66.7%) with a median age of 53.5 years and the SMA being the most affected (73.3%) followed by the celiac artery (60%). 2
Clinical Presentation
All our 16 patients presented with abdominal pain, and 43.8% additionally experienced nausea and vomiting. Similarly, Salvarani et al reported 94.4% and 66.7%, respectively. Also, elevated CRP and ESR were found in 68.8% and 50.0% of our patients, respectively, in line with the findings of Salvarani et al, who reported 50% with elevated ESR. 2
Although medium vessel CBA findings have been well characterized for systemic vasculitis, CBA does not allow visualization of vessel wall. Therefore CTA/MRA provides better visualization of WT, which can help differentiate LVGT from other similar conditions. 2 According to our criteria (WT ≥3 mm), all 16 of our patients showed arterial WT on CT/CTA. Nine patients (56.3%) also had concurrent D, which is not commonly described in LVGT, and was not observed in the case series by Salvarani et al. Although most of our diagnoses were based on CTA imaging, Salvarani et al mostly relied upon CBA (77.8%) and vascular biopsy (22.2%). None of our patients underwent vascular biopsy for histological confirmation due to the risks of the procedure. 35
Treatment
Localized vasculitis of the gastrointestinal tract is typically treated with steroids, such as prednisone; 62.5% of our patients were managed with prednisone, 18.8% received conservative treatment, 18.8% were given anticoagulation, 6.3% underwent endovascular repair, and 6.3% underwent surgical arterial repair. The typical dose consists of 20–40 mg of prednisone for one month, followed by a taper in 3 months, depending on symptoms, laboratory values, and imaging results. Salvarani et al reported 16.7% were managed with conservative treatment, 27.8% with prednisone only, 27.8% with prednisone plus other immunosuppressive therapy, 22.2% with surgery, and 44.4% with surgery and medical therapy. Most of our patients had symptom relief (93.8%), whereas Salvarani et al. reported that less than half of patients responded to treatment. 2 This discrepancy in outcomes between the two studies could be explained by the slight differences in diagnostic criteria used. We used similar diagnostic criteria to Salvarani et al, but additionally focused on WT (≥3 mm) as the primary qualifier. For this reason, we may have been better equipped to differentiate between SAM, isolated D, and LVGT and thus had greater treatment success. Due to its rarity, there is no established treatment for LVGT. However, early diagnosis is important to reduce morbidity and mortality. 2
Fibromuscular Dysplasia
Epidemiology
Fibromuscular Dysplasia has a strong female predominance (80–90%) with an average age of 52 years.36-39 Based on the criteria used in our study, we only included FMD patients with mesenteric artery involvement, and thus some of our results differ from other FMD analyses. Consistent with previous reports, 76.9% of our patients were female with an average age of 50.2 years.
Clinical Presentation
Although patients with FMD can be asymptomatic, others can present with symptomatic arterial D and end organ ischemia or bleeding. 40 As expected, abdominal pain was significantly more common in our study compared with previous reports (76.9 vs 17.2%), as we only focused on mesenteric arterial involvement. 39 Although 23% of our patients were asymptomatic, others reported a rate of only 5.6%. 37 Hypertension was a common comorbidity we observed in 38.5% of our patients, which is slightly lower than previous reports of 60–80%.37,39,41
We observed much higher rates of arterial D (61.5%) than what was reported by the United States FMD registry (17.0%). 37 All our FMD patients were diagnosed using CT or CTA, in addition to 23.1% with ultrasound, 7.7% with MRA, and 23.1% with CBA imaging, similar to previous reports in which 93.6% were diagnosed with CTA and 6.4% with MRA. 41
Treatment
Conservative management was used in 15.4%, antiplatelet in 38.5%, anticoagulation in 7.7%, endovascular repair in 7.7%, and surgical repair in 38.5% of our patients, of which 3 patients underwent arterial repair and 2 underwent abdominal surgeries. Although 92.3% of patients had symptoms relief, all patients who had follow-up imaging showed improved or stable disease.
Genetic Disorders (Ehlers Danlos, Loeys–Dietz, Marfan Syndrome)
Epidemiology
Each has a typical onset in early to mid-adulthood. 5 Loeys–Dietz syndrome is generally more severe, with 37 years reported as median age of survival and 29.8 years as median age of the first major vascular event, compared to vEDS with 48–24.6 years, respectively. 22 However, Marfan syndrome has a better average survival of nearly 70 years. 42 Arterial D or rupture is the most common cause of death, with 66% of arterial ruptures with vEDS occurring in the abdominal vasculature. 43 There is equal gender prevalence in each of these disorders.
Clinical Presentation
Of the two patients with vEDS, one presented with abdominal pain and had finding of celiac artery D with WT of both the celiac and SMA on CTA. The other patient had a SMA D but was asymptomatic. The single LDS patient had asymptomatic SMA D with concurrent WT. The patient with Marfan syndrome presented with chest pain, and a CTA finding of celiac artery D.
Treatment
There are currently no approved therapies to delay the onset of major vascular events in vEDS, but early diagnosis can help with timely management. 20 Options include celiprolol, a beta-blocker currently not available in the US, restrictions on strenuous exercise, frequent cardiovascular imaging, and prophylactic surgical repair of worsening arterial findings. 44 Loeys–Dietz syndrome has been reported to have a fatal complication rate of 45% after surgery, compared with 1.7% in vEDS. 22 Due to this high risk, our LDS patient was managed conservatively, but showed no improvement in symptoms or imaging findings at follow-up. Our vEDS patients were each managed differently; the patient with celiac artery D and WT of the celiac and SMA underwent endovascular repair and received anticoagulants, antiplatelets, antihypertensives, and steroids; the second patient who had asymptomatic SMA D was managed with anticoagulants and antihypertensive medications. At follow-up, both showed improved imaging findings. The patient with Marfan Syndrome was managed conservatively, and although she did not experience any symptom relief, she showed improved imaging findings at follow-up.
Polyarteritis Nodosa
Epidemiology
The peak incidence of PAN occurs in the fifth and sixth decades of life with male predominance.45-47 In contrast, all 3 of our patients were female with an average age of 57.3 years. Gastrointestinal tract involvement has been reported in 40-70% of PAN cases, and it usually reflects worse outcomes.46,48-51
Clinical Presentation
A review of 348 PAN patients reported GI manifestations in 132 patients, of which presenting symptoms of abdominal pain (94%), bleeding (9%), perforation (11%), cholecystitis (10%), appendicitis (3%), and pancreatitis (10%) were reported. In addition, 36% of these patients required surgery. 47 Consistent with PAN presentation trends, all 3 of our patients presented with abdominal pain, in addition to one with nausea and vomiting and another with diarrhea. One patient had celiac artery D and WT, another had celiac and SMA WT, and the last had only WT involving the celiac, SMA, and IMA.
Treatment
Corticosteroids are usually recommended as first-line treatment, but other immunosuppressants may be used as steroid-sparing agents. 46 Although required in some circumstances, need for surgical intervention for GI complications is a significant predictor of reduced survival in patients with PAN. 52 Two of our patients with PAN were treated with anticoagulation and steroids, and the other with endovascular repair; all 3 had improved symptoms and imaging findings at follow-up. Untreated patients with PAN compared with those who received medical or interventional therapies have 13% and 80% five-year survival rates, respectively, which further emphasizes the need for early diagnosis and management. 52
Median Arcuate Ligament Syndrome
Epidemiology
One of our two patients with MALS was a female with an average age of 63.5 years. Literature reported that MALS has a greater female predominance (4:1 ratio) and presents most commonly between 40 and 60 years of age in patients with a thin body habitus.53,54
Clinical Presentation
Both of our patients with MALS were asymptomatic. In contrast, Columbo et al has reported that all their 21 patients presented with abdominal pain, in addition to 81% of cases with nausea and 47% with diarrhea. Both our patients were observed to have celiac artery D, and one additionally had WT of the celiac artery.
Treatment
Both patients were treated with antiplatelet therapy, and one had endovascular repair. Although the patient treated with antiplatelet therapy reported no change in symptoms but had improvement in imaging findings, the patient treated with intervention had improvement in symptoms, but had no follow up imaging. Published reports describe a variable response to revascularization and nerve plexus resection suggest a need for translational research to better characterize this poorly understood clinical entity. 16
Takayasu’s Arteritis
Epidemiology
Based on the current literature, TA predominantly affects females with an average age of 30 years. 55 Similarly, our study found both patients with TA were females, with an average age of 37 years.
Clinical Presentation
Takayasu’s arteritis most commonly affects the thoracic aorta and its major branches (e.g., left subclavian, right subclavian, and left carotid) and usually presents with arterial stenosis.55,56 Abdominal arterial involvement has also been reported. In a study involving 104 patients with TA, Vanoli et al reported involvement of the renal arteries (34.4%), SMA (31.6%), celiac artery trunk (21.4%), and IMA (9.4%). One of our two patients had WT of both celiac and SMA, and the other had only WT involving the SMA. Both patients presented with elevated ESR and CRP.
Treatment
Vanoli et al. treated 86% of their patients with glucocorticoids, 56% with cytotoxic agents, 54% with angioplasty, and 42% with surgical bypass revascularization. 55 Both of our patients received prednisone, in addition, one underwent surgical aorto-celiac and SMA bypass. Both patients reported improved symptoms, and one had improved imaging findings while the other’s remained unchanged.
Study Limitations
This is a retrospective analysis of a single center evaluating a group of patients with heterogeneous diseases affecting the mesenteric arteries. The sample size was small to make statistically significant comparisons between different disease groups. Some of these disorders, like SAM or LVGT, are not well-studied, and as such, there is no established clear diagnostic criteria. Given the lack of standardized diagnostic criteria for some of these disorders, we used most supported evidence in addition to our own experience to finalize the diagnoses. Furthermore, the new criteria used at the 2019 first international consensus on FMD diagnosis has expanded the required arterial involvement for the diagnosis of FMD to include any single or multiple medium artery, making it very hard to distinguish SAM from FMD in situations when there are multiple arterial pathologies involving multiple medium size arteries. Therefore, a few of the cases with proposed SAM diagnosis in our series, could have been considered to have FMD. Most of our patients did not have arterial biopsy since it is not always safe, feasible or required to confirm most of these diagnoses. Furthermore, genetic testing was only considered based on physician discretion in selected patients with findings consistent with genetic connective tissue disorders.
Conclusion
Mesenteric artery D and WT are rare arteriopathies that can have serious complications including death. As most patients with different etiologies may present in a similar manner, more research is required to standardize diagnostic criteria and improve management plans. Our study showed better outcomes for most of these arteriopathies than previously reported, which can be explained by multidisciplinary and conservative approach in addition to better defined diagnostic criteria. Although we favor conservative and medical management for most patients, we recommend intervention (preferably endovascular) for cases with urgent presentations such as arterial rupture, expanding pseudoaneurysm, and or end organ severe ischemia.
Footnotes
Author contribution
All authors contributed to: (1) substantial contributions to conception and design, or acquisition of data, or analysis and interpretation of data, (2) drafting the article or revising it critically for important intellectual content, and, (3) final approval of the version to be published.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.