
Abstract
Data on characteristics and outcomes of coronavirus (COVID)-19 patients complicated with arterial thrombosis (AT) are scarce. Therefore, we carried out a systematic review (PRISMA, PROSPERO statements; PubMed, Scopus, and Web of Science) to identify risk factors, clinical presentation, treatment, and outcomes. We included publications from December 2019 to October 2020. Groups: (a) ischemic stroke, (b) thrombotic storm, (c) peripheral vascular thrombosis, (d) myocardial infarction, and (e) left cardiac thrombus or in-transit thrombus (venous system thrombus floating or attaching to the right heart). We considered 131 studies. The most frequent cardiovascular risk factors were: hypertension, diabetes, and dyslipidemia. A high proportion presented with asymptomatic, mild, or moderate COVID-19 (n = 91, 41.4%). We identified a high percentage of isolated ischemic stroke and thrombotic storm. Groups with higher mortality rate: intracardiac thrombus (1/2, 50.0%), thrombotic storm (18/49, 36.7%), and ischemic stroke (48/131, 36.6%). A small number received thromboprophylaxis. Most patients received antithrombotic treatment. The most frequent bleeding complication was intracranial hemorrhage, primarily with isolated stroke. Overall mortality was 33.6% (74/220). Despite a wide range of COVID-19 severity, a high proportion had AT as a complication of non-severe disease. AT can affect different vascular territories; mortality is associated with stroke, intensive care unit stay, and severe COVID-19.
Keywords
Introduction
Severe acute respiratory syndrome coronavirus (SARS-CoV-2) infection caused a severe pandemic1,2 associated with a broad spectrum of clinical presentations with different degrees of systemic inflammatory response. 3 SARS-CoV-2 infection leads to an over-activated inflammatory response expression (cytokine storm), inducing endothelial dysfunction, hypercoagulable state, and arterial and venous thrombosis in large and small vessels.4–7 Mortality and poor outcome are closely related to immune, coagulation, and immunothrombosis systems dysregulation. Early reports demonstrated a high incidence of venous thromboembolism 8 and a low incidence of arterial thrombosis (AT) (1.8% to 3.7%)9–14 with a wide-ranging clinical presentation.15,16
Although currently, we have data on the clinical presentation and incidence of venous thromboembolism, 17 the evidence on AT is scarce and restricted to case reports 3 and limited systematic reviews. 18 Therefore, we conducted, to our knowledge, the first systematic review following the Preferred Reporting Items for Systematic reviews and Meta-Analysis (PRISMA) and International Register of Systematics Review (PROSPERO) statements to identify risk factors, clinical presentation, therapeutic strategies, and outcomes of coronavirus (COVID)-19 patients complicated with AT.19–23
Methods
According to the PRISMA statement, we performed the protocol and registered it in the prospective international register of systematic reviews (PROSPERO) (ID: CRD42020213639). In addition, we included cohorts, case series, case reports, letters to the editor, consensus reviews, and systematic reviews published on COVID-19–induced AT in patients from December 1, 2019, to October 1, 2020.
We included all patients with a confirmed diagnosis of COVID-19 and evidence of AT. In addition, we defined 5 groups based on arterial thrombus location: (a) ischemic stroke, (b) thrombotic storm, (c) peripheral vascular thrombosis (limbs, great vessels, and visceral vessels), (d) myocardial infarction, and (e) left cardiac thrombus or in-transit thrombus (venous system thrombus floating or attaching to the right heart). We defined a thrombotic storm as two or more arterial or venous thrombi simultaneously or with a difference of ≤30 days between both events. 24 We also determined major (including intracranial hemorrhage), minor, and clinically relevant bleeding complications following the International Society on Thrombosis and Haemostasis definitions. 25 Other definitions, including COVID-19 severity classification and arterial thrombotic events, are available in the Supplementary Appendix. Finally, we investigated the incidence of AT in patients without previous cardiovascular disease and the presence of deep venous thrombosis, pulmonary embolism, and thrombotic storm.
Search Strategy
We performed a systematic review through PubMed, Scopus, and Web of Science using the following terms: (thrombosis OR venous thrombosis OR arterial thrombosis OR stroke OR acute ischemia OR thrombotic storm OR left ventricular thrombus) AND (disseminated intravascular coagulation OR thrombolysis OR anticoagulants OR enoxaparin OR fibrin fibrinogen degradation products OR fibrinolytic agents OR heparin OR platelet aggregation inhibitors OR tissue plasminogen activator OR thrombectomy OR NOAC OR DOAC OR vitamin K antagonist OR acenocoumarin OR acenocoumarol OR warfarin OR coumadin OR phenprocoumon) AND (coronavirus OR COVID OR COVID-19 OR severe acute respiratory syndrome coronavirus 2 OR SARS-COV2). No filters or limits were applied besides the date and language of publication. We included articles published in English and Spanish only. We organized references with Zotero reference manager software (https://www.zotero.org/).
Selection and Data Collection Process
Two reviewers independently identified potentially eligible studies by examining titles and abstracts. They obtained full articles to assess eligibility criteria and extracted cases that met them. They double-checked papers deemed suitable, and the pair revised the article and decided as a team in case of lack of consensus. All investigators performed and analyzed the data extraction of every case report to improve the quality of data extraction. The authors are cardiologists, cardiology fellows, and medical students who received adequate training. We had a weekly group discussion to analyze and resolve disagreements by consensus. We collected the data extracted through an online collaborative database with controlled access. We included variables of interest in the following categories: epidemiology, risk factors, arterial thrombosis, clinical manifestations, concomitant vascular complications, diagnosis, treatment, prevention, mortality, prognosis, and follow-up. Two researchers reviewed 30% of the database to establish strict quality control of the extracted data. In addition, we reviewed several databases to diminish the risk of bias, including gray literature. Additionally, we performed manual analyses with snowballing method 26 to ensure appropriate information coverage.
Statistical Analysis
We used summary statistics for continuous and categorical variables according to their types and distributions. In addition, we report the frequency and percentage for categorical variables and the median and interquartile range for continuous variables. We used the IBM SPSS® software platform (Chicago, IL, USA) for descriptive statistical analysis.
Results
We conducted the systematic search during October 2020 and included articles published until October 1st, 2020. The search period provides for unvaccinated patient inclusion. Figure 1 shows the flowchart, including the 4 phases of PRISMA and the number of obtained, duplicated, and excluded papers. We collected 2059 papers from PubMed, Scopus, and Web of Science in the identification phase. Next, we carefully reviewed the full text for eligibility criteria and selected 171 papers for the quality assessment. Finally, we extracted the data for this review from 131 studies, including individual data of 220 patients. PRISMA 2009 Flow Diagram. Note. From: Moher D, Liberati A, Tetzlaff J, Altman DG, The PRISMA Group (2009). Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med 6(7): e1000097. doi:10.1371/journal.pmed1000097.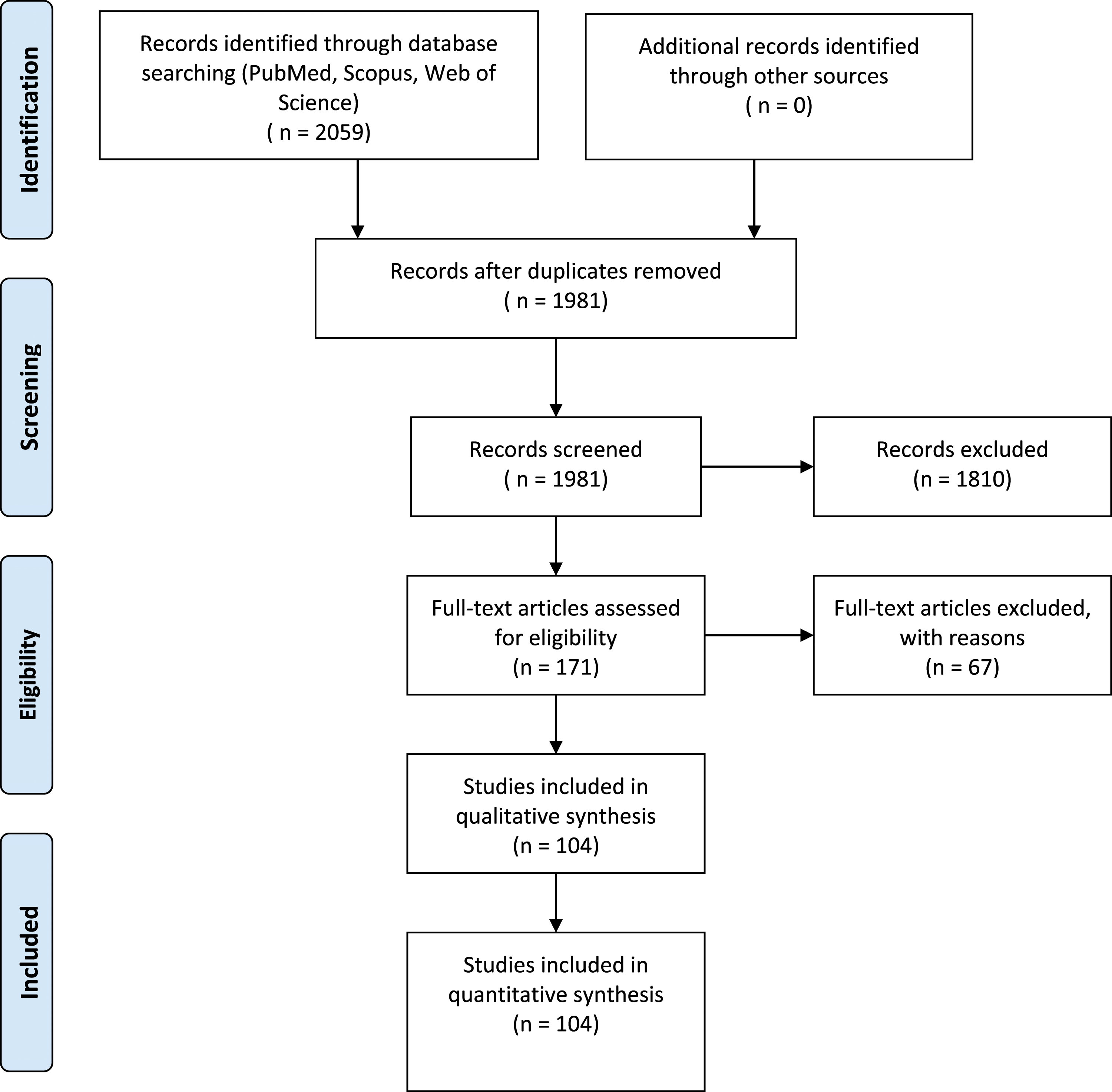
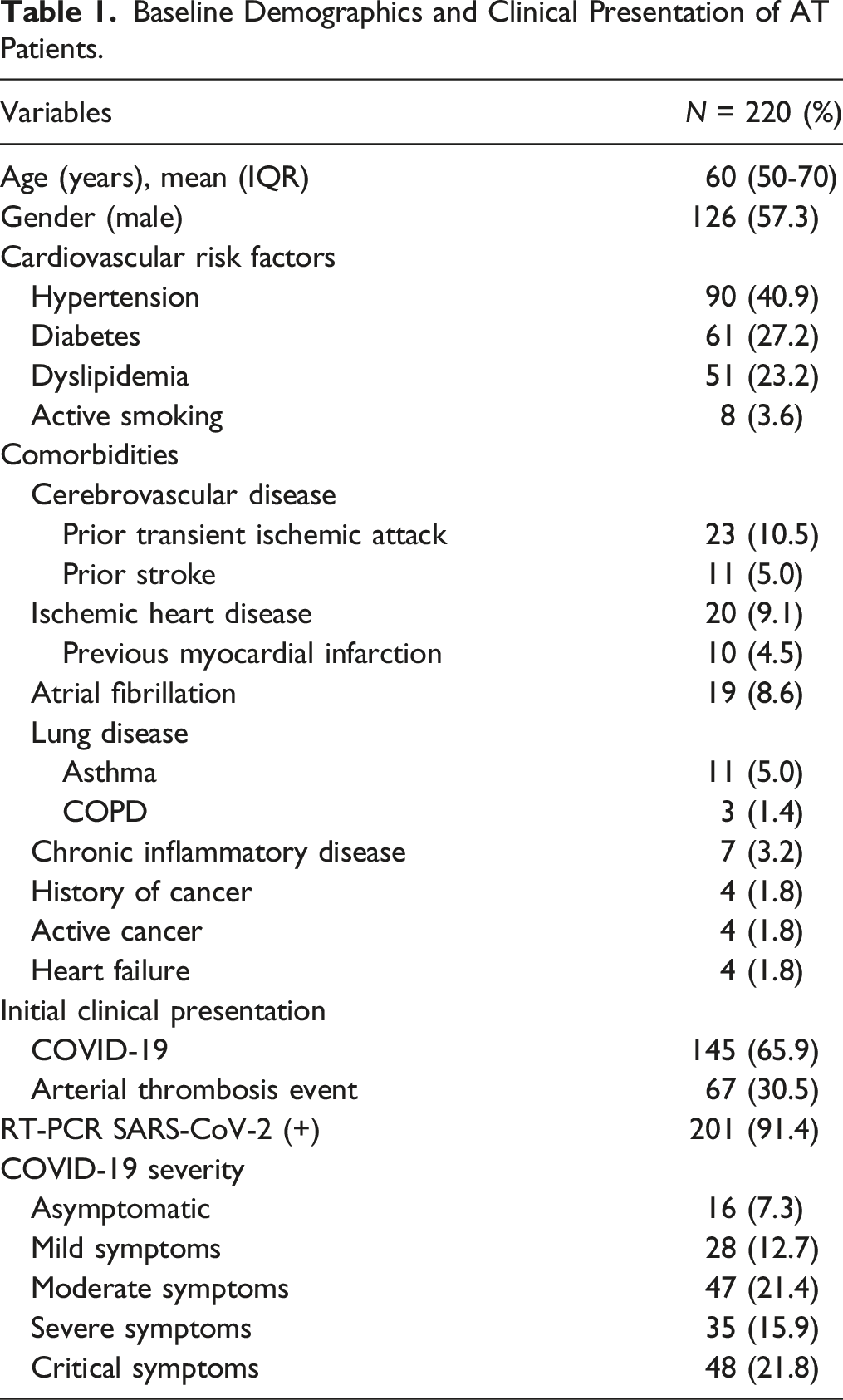
Baseline Demographics and Clinical Presentation of AT Patients.
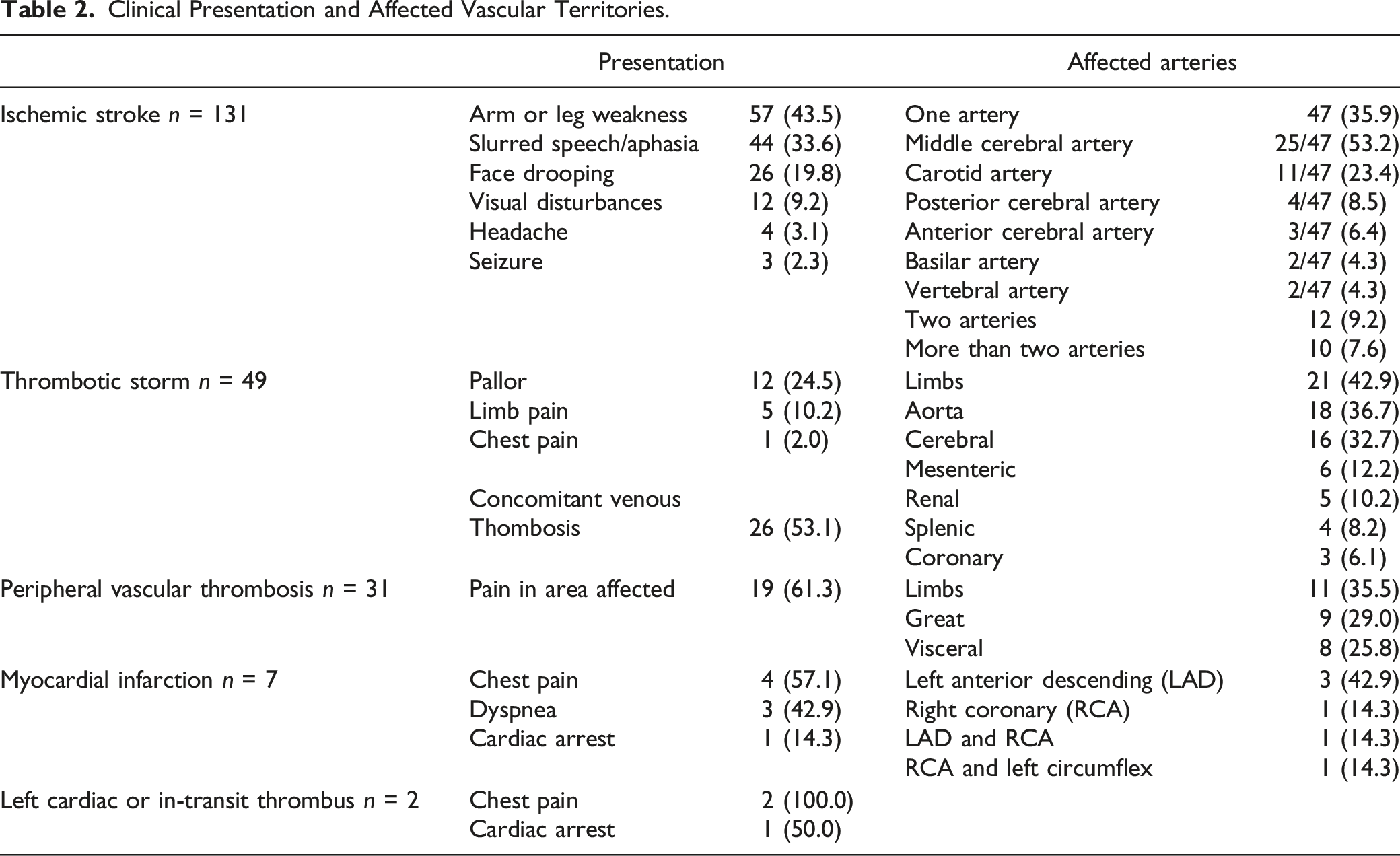
Clinical Presentation and Affected Vascular Territories.
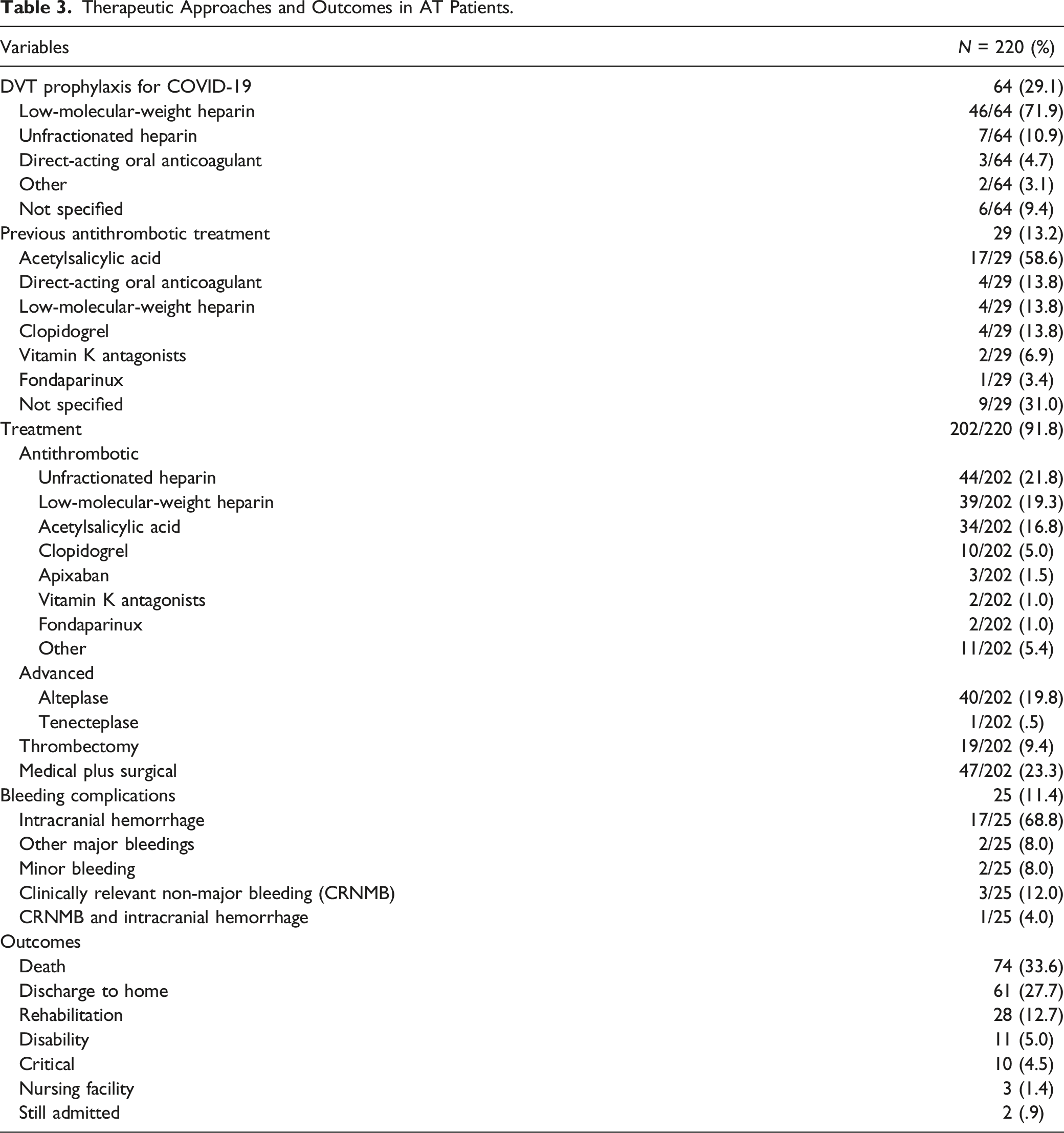
Therapeutic Approaches and Outcomes in AT Patients.
COVID-19 Characteristics.
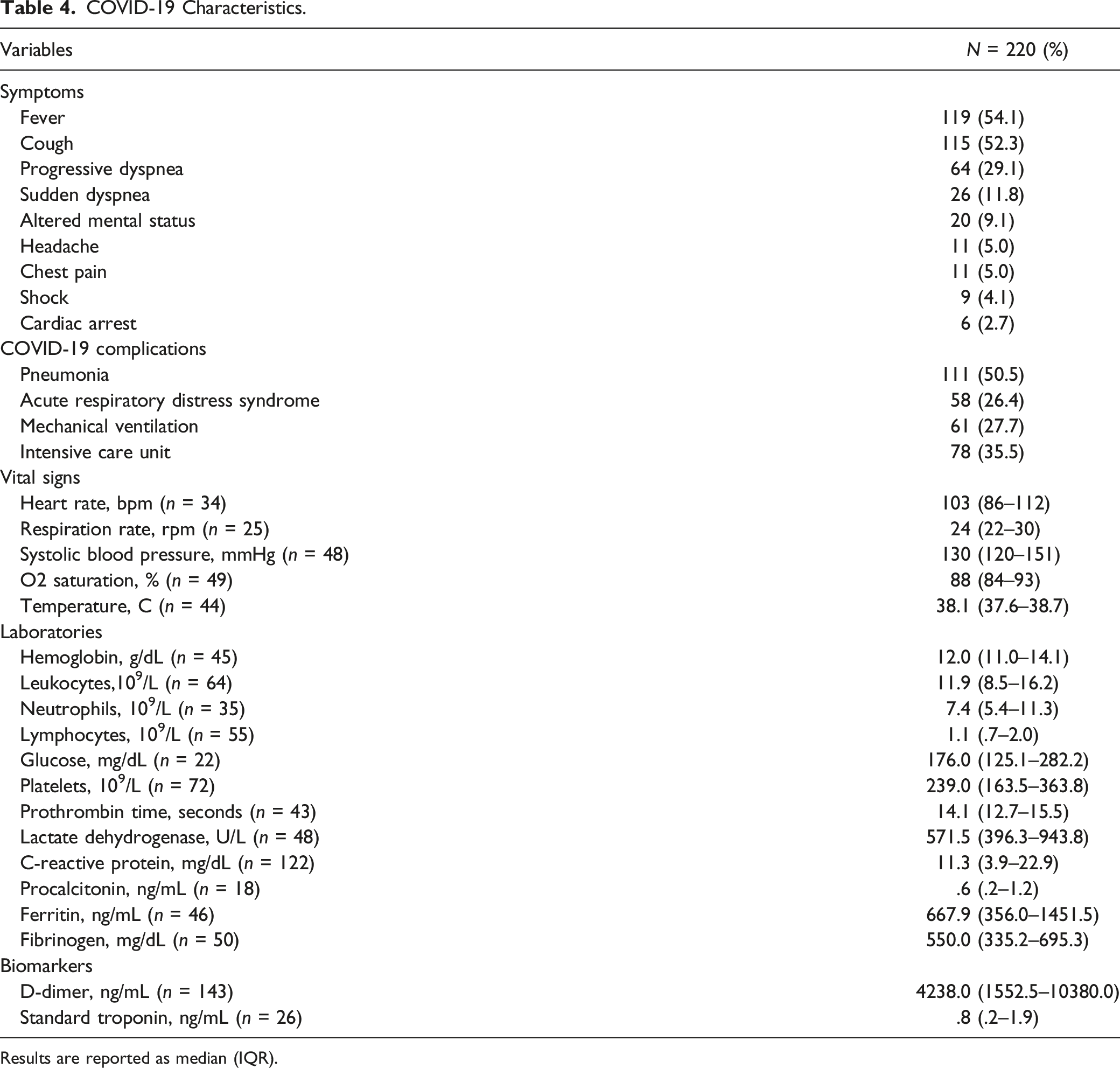
Results are reported as median (IQR).
Discussion
This systematic review highlights the clinical presentation, therapeutic trends, and outcomes of unvaccinated COVID-19 patients with AT during the early pandemic phase. The key findings of this systematic review were: First, a high proportion of patients with asymptomatic, mild, and moderate COVID-19 developed AT. Second, stroke and thrombotic storms were the most frequent AT events, driving vascular mortality. Finally, overall mortality was associated with stroke, ICU stay, and severe COVID-19.
Emerging evidence suggests that COVID-19 is characterized by endothelitis secondary to direct viral infection facilitated by the overexpression of angiotensin-converting enzyme receptor 2, the receptor for cell entry of SARS-CoV-2 in endothelial cells, highly expressed in the lungs, heart, veins, and arteries.18,27,28 SARS-CoV-2 in most patients causes a high prothrombotic state inducing thrombosis through inflammation pathways, endothelial activation, immunothrombosis, 29 cytokine storm, 30 and coagulation system activation. Dysregulation of the renin-angiotensin system and the innate and adaptive immune system also plays an essential role.30,31 All these mechanisms associated with in-hospital and ICU risk factors 30 explain the high incidence of venous thromboembolism.8–10,17,31 SARS-COV-2 inflammation can destabilize a vulnerable plaque 32 in the elderly with ischemic heart disease and subclinical atherosclerosis.3,7,18 Consequently, these mechanisms may also explain the high incidence of AT in non-critically and critically ill unvaccinated patients with COVID-19 (Table 1).
The COVID-19 phenotype in this systematic review included mainly elderly males with cardiovascular risk factors and comorbidities (Table 1). This phenotype is similar to that observed in ST-elevation myocardial infarction, 33 suggesting that SARS-COV-2 identifies as a target of an activated endothelium. The endothelium dysfunction is driven by inflammasome activation and reduced endogenous anti-inflammatory mechanisms in the elderly population.34,35 In addition, inflame-aging activates leukocytes and endothelial and vascular smooth muscle cells,34,35 and aging induces factors V, VII, VIII, and X, increasing the von Willebrand factor. 36 The higher incidence of AT in males reproducing previous evidence 18 suggests differences in hormonal and genetic profiles of both sexes, with female sex hormones producing a favorable immune modulation. 18 Additionally, the prevalence and severity of COVID-19 have since been established to be higher in males than in females. 18
In this systematic review, we observed a high rate of AT in non-severe unvaccinated COVID-19 patients. As in other published studies, the clinical profile consisted of a hyper-inflammatory and hypercoagulable state 28 (Table 4). Some have proposed the definition of a COVID-19-associated hyperinflammation phenotype as a CRP concentration >15 mg/dL or a ferritin level >1500 ng/mL. 37 In our cohort, 50 (22.7%) and 11 (5.0%) patients met these criteria for CRP and ferritin, respectively. Although existing guidelines 38 recommend primary prevention against venous thromboembolism in-hospital patients with critical illness, the incidence remains high (6–11%). 39 Notably, before vaccines were available for primary prevention in hospitalized COVID-19 patients, recommendations did not differ from non–COVID-19 in-hospital patients. 40
Furthermore, the National Institute of Health guidelines do not recommend anticoagulation prophylaxis to prevent AT outside the usual standard of care for non–COVID-19 patients. 40 D-dimer demonstrated a consistently elevated pattern in COVID-19 patients with thrombosis, while platelet count, fibrinogen levels, and prothrombin time (PT) vary from standard to high levels. 28 Our cohort displayed a similar pattern, with 118 (53.6%) patients with D-dimer >1000 ng/mL, and only 16 (7.3%), 26 (11.8%), 35 (16.0%) with platelet count >400 109/L, prothrombin time >13.5 s, and fibrinogen levels >400 mg/dL, respectively. Despite some evidence pointing towards the benefit of higher D-dimer measurements, there are no recommendations for using coagulopathy markers to guide treatment. 40 Consequently, we do not have guidance for AT primary prevention or measures for early detection in the broad clinical spectrum of unvaccinated COVID-19 patients. Antithrombotic and anti-inflammatory drugs remain the cornerstone for COVID-19 disease and COVID-19-induced thrombosis. 28 Thrombectomy and surgery have a more minor but significant role, with a prevalence of 30% (66/220 patients) in this systematic view.
Ischemic strokes were the most frequent AT group (Table 2) associated with poor outcomes. These findings could explain the lack of benefit of oral anticoagulants or anti-inflammatory agents prescribed before and during the first week after discharge. Also, we cannot exclude the possibility of paroxysmal atrial fibrillation or subclinical atherosclerosis as an embolic source in patients with ischemic stroke. We found a similar rate of atrial fibrillation (19, 8.6%) to that reported in a previously published systematic review. 41 We identified a few cases of aortic thrombosis as incidental findings during imaging studies for other reasons. Consequently, aortic thrombosis may be underestimated. Pain drove high clinical suspicion among peripheral vascular thrombosis patients. In those with lower limb AT, we cannot exclude subclinical atherosclerosis. In addition, half of the myocardial infarction group has isolated ST-elevation myocardial infarction with thrombosis in the left coronary artery (Table 2). The abnormal ejection fraction possibly had several mechanisms as myocardial infarction, myocarditis, and cytokine storm. 32 In the last group, the low incidence of left ventricular and in-thrombus transit could be attributed to the low use of echocardiography screening in COVID-19 patients. The echocardiogram is limited to those with a suspected acute cardiac event or pulmonary embolism, so the true incidence of this complication may be unknown.
Around 33.6% had mortality related to ischemic stroke, ICU stay, and severe COVID-19. Studies have reported a mortality rate of 20–35% in the same population (ischemic stroke, ICU, severe COVID-19).18,41 On the other hand, intracranial hemorrhage had a lower-than-expected incidence among other hemorrhagic complications. 18 Furthermore, evidence suggests a poor survival prognosis in AT COVID-19 unvaccinated patients. 42 Unfortunately, systematic reviews, meta-analyses, and registries are scarce, so it is difficult to determine the true incidence of AT in unvaccinated and vaccinated COVID-19 patients.
Further research is mandatory to identify high-risk patients and whether primary prevention for venous thromboembolism is effective and safe to avoid or reduce AT in non-severe COVID-19 patients. Recent evidence showed that AT and venous thromboembolism incidence remains high up to 49 weeks after COVID-19 diagnosis. Therefore, preventing severe COVID-19 through vaccination remains a priority. 43
The study’s limitations include a potential loss of case reports from search engines. In addition, we know that a substantial proportion of patients did not have a PCR to establish the diagnosis. The trend is not to report patients with poor in-hospital outcomes or serious adverse events. However, considering gender, risk factors, and comorbidities, we cannot rule out paroxysmal atrial fibrillation secondary to emotional stress, hypoxia, mechanical ventilation, etc., and subclinical atherosclerosis in the carotid, vertebral, and peripheral vascular systems. In addition, obtaining information on the timing of the D-dimer measurements and other biomarkers and bleeding complications outcomes during follow-up was impossible. In some cases, it was also challenging to determine if intracerebral hemorrhage presented before or after treatment. We only retrieved data from the published articles and did not contact any author. Therefore, our results should be analyzed with caution. Another limitation is that clinical variables are constantly absent in these studies. Also, we could not identify the time between diagnosis, hospital admission, or symptom onset. However, our review allows us to overview clinical presentation, therapeutic trends, and outcomes in unvaccinated COVID-19 patients complicated with AT during the early phase of the pandemic. Another limitation is the included unvaccinated population. After 2020, vaccine programs and the new strains with lower virulence changed the clinical spectrum, as reported in this systematic review. Although worldwide vaccination reduced the incidence and severity of SARS-COV-2 infection, we cannot exclude the emergence of new strains, regional or global rebound, and people rejecting vaccines. Therefore, clinical observations from unvaccinated patients could help improve patient care currently and in the future. As for any systematic review, our results should be considered hypothesis-generating, and prospective studies are mandatory to confirm our findings. Few cases (or just one case) report considerable heterogeneity in numerous factors/characteristics.
Considering the heterogeneity of the data obtained, we propose developing a standard framework for reporting cases during and after the COVID-19 pandemic. Authors should provide detailed information, including patient demographics, risk factors, clinical presentation, in-hospital outcomes, and therapeutic approaches, helping to compare cases pre- and post-vaccination, possibly improving patient care. In addition, drug names, dosages, numbers of days given, and follow-up data to understand the impact of treatment after discharge. We believe this editorial strategy could substantially improve the quality of future systematic reviews and facilitate research on COVID-19 and its severe complications.
Despite a wide range of COVID-19 severity on admission, many unvaccinated patients had AT as a complication of non-severe COVID-19 disease. Furthermore, AT can affect different vascular territories, and mortality is associated with stroke, ICU stays, and severe COVID-19. Therefore, creating guidelines for preventing thrombotic complications, increasing early detection, and promoting COVID-19 vaccines remains imperative. Retrospective and prospective research is mandatory to compare early pandemic and post-vaccination AT complications.
Supplemental Material
Supplemental Material - Risk Factors, Clinical Presentation, Therapeutic Trends, and Outcomes in Arterial Thrombosis Complicating Unvaccinated COVID-19 Patients: A Systematic Review
Supplemental Material for Risk Factors, Clinical Presentation, Therapeutic Trends, and Outcomes in Arterial Thrombosis Complicating Unvaccinated COVID-19 Patients: A Systematic Review by Alejandra Castro-Varela, Daniela M Martinez-Magallanes, Maria Fernanda Reyes-Chavez, Jose Manuel Gonzalez-Rayas, Jose Gildardo Paredes-Vazquez, Eduardo Vazquez-Garza, Mauricio Castillo-Perez, Yoezer Z Flores-Sayavedra, Arturo Martinez, Ray Erick Ramos Cazares, Jaime Guajardo, Hector Lopez-de la Garza, Jose Alfredo Salinas-Casanova, Hector Betancourt, Abigail Montserrat Molina-Rodriguez, Jathniel Panneflek, Mario Alejandro Fabiani, and Carlos Jerjes-Sanchez in Angiology
Footnotes
Author Contributions
All authors contributed to: (1) substantial contribution to conception and design, or acquisition of data, or analysis and interpretation of data, (2) drafting the article or revising it critically for important intellectual content, and (3) final approval of the version to be published.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.