
Abstract
The Naples score (NS), which is a composite of cardiovascular adverse event predictors including neutrophil-to-lymphocyte ratio, lymphocyte-to-monocyte ratio, albumin, and total cholesterol, has emerged as a prognostic risk score in cancer patients. We aimed to investigate the predictive value of NS for long-term mortality in ST-segment elevation myocardial infarction patients (STEMI). A total of 1889 STEMI patients were enrolled in this study. The median duration of the study was 43 months (IQR: 32–78). Patients were divided into 2 groups according to NS as group 1 and group 2. We created 3 models as a baseline model, model 1 (baseline + NS in continuous), and model 2 (baseline + NS as categorical). Group 2 patients had higher long-term mortality rates than group 1 patients. The NS was independently associated with long-term mortality and adding NS to a baseline model improved the model performance for prediction and discrimination of long-term mortality. Decision curve analysis demonstrated that model 1 had a better net benefit probability for detecting mortality compared with the baseline model. NS had the highest contributive significant effect in the prediction model. An easily accessible and calculable NS might be used for risk stratification of long-term mortality in STEMI patients undergoing primary percutaneous coronary intervention.
Introduction
ST-segment elevation myocardial infarction (STEMI) is the significant cause of mortality among acute coronary syndrome spectrum. Although several treatment options, such as reperfusion therapies, recent antithrombotic drugs, advanced primary percutaneous techniques, and secondary prevention modalities have been widely used, the long-term mortality rates of STEMI patients change between 4 and 12% worldwide. 1 Various factors can determine the risk of death in STEMI patients including, treatment delay, age, Killip status, number of diseased coronary vessels, left ventricular ejection fraction (LVEF), diabetes mellitus (DM), and history of coronary artery disease. 1 The most widely used scoring system in predicting mortality in STEMI is the Global Registry of Acute Coronary Events (GRACE) risk stratification score. 2 However, this risk scoring system does not include the components of the inflammation and nutritional status, which play a critical role in the prognosis of STEMI.3,4 Thus, new scoring systems including the above-mentioned factors have been widely investigated in recent studies.
The Naples score (NS) has emerged as a valuable prognostic tool in cancer patients. NS is a composite of serum albumin levels, total cholesterol levels, neutrophil/lymphocyte ratio (NLR), and lymphocyte/monocyte ratio (LMR). 5 This score can be used to assess both the inflammatory and nutritional status of patients. All components of NS have been solely reported as associated with long-term mortality in STEMI patients in previous research.6-9 However, the combination of these parameters might have more predictive ability for long-term mortality than each alone. Thus, we aimed to investigate the association of NS with the long-term mortality in STEMI patients in this study.
Material and Methods
This study had observational and retrospective study design and a total of 1889 patients with STEMI who underwent primary percutaneous coronary intervention (pPCI) between June 2013 and September 2022 were enrolled. All patients underwent pPCI within 12 h of the onset of symptoms. Patients with active infection or inflammatory disease, microalbuminuria, malnutrition, chronic liver disease, active malignancy, chronic kidney disease, and undergoing hemodialysis or peritoneal dialysis were excluded from the study. This study was approved by the local ethics committee of our institute and because of the retrospective and observational design of this study, written informed consent from the patients was not required.
Laboratory Analysis
Before pPCI, blood samples were obtained from an antecubital vein upon admission to the emergency room. The Beckman Coulter LH 780 hematology analyzer (Beckman Coulter, Miami, FL, USA) was used to assess the hematologic parameters, and a Beckman Coulter LH 780 was used to analyze the biochemical data (Beckman Coulter Ireland Inc., Mervue, Galway, Ireland).
Angiographic Procedure
Depending on the operator’s preference, either the transradial or transfemoral approach was used according to the Seldinger procedure for routine coronary angiography. Before the coronary angiographic procedure, all patients received a standard dosage of unfractionated heparin (70–100 U/kg), a loading dose of 300 mg of acetylsalicylic acid, and P2Y12 inhibitors, unless contraindicated. The use of glycoprotein IIb/IIIa receptor blockers was left up to the operator. The angiographic images of all patients were assessed carefully by 2 experienced cardiologists, who were blinded to all clinical data.
Definitions and Study Outcomes
The following criteria were used to determine the diagnosis of STEMI in accordance with the recent guidelines for the universal definition of myocardial infarction: 1- ST-segment elevation >2.5 mm in men aged <40 years, >2 mm in men aged >40 years, or >1.5 mm in women at 2 or more contiguous leads in v2-v3 and/or >1 mm in other leads; 2- Based on the recent guideline for the universal definition of myocardial infarction, the diagnosis of STEMI was made using the following criteria: 1- [for the cases that do not have left ventricle hypertrophy or left bundle branch block] ST-segment elevation ≥2.5 mm in men younger than 40 years, ≥2 mm in men older than 40 years, or ≥1.5 mm in women at least 2 contiguous leads in V2-V3 and/or ≥1 mm in the other leads; 2- typical chest pain that lasted >30 min at rest; 3- elevation of serum biomarkers that are specific to myocardial damage. 10 The presence of hypertension (HT) was accepted with systolic blood pressure >140 mmHg and/or diastolic blood pressure >90 mmHg on at least 2 different times and/or the using antihypertensive drugs. A fasting plasma glucose level >126 mg/dL, a postprandial glucose level >200 mg/dL, and/or the use of anti-diabetic medications were used to diagnose diabetes mellitus. Hyperlipidemia was identified with a high total cholesterol >200 mg/dL and/or using anti-hyperlipidemic drugs. Smoking was defined as patients who had smoked for at least 6 consecutive months in the past year. Body mass index (BMI) was measured using the formula, BMI = weight (kg)/height (m). 2 Thrombolysis in myocardial infarction (TIMI) flow and TIMI myocardial perfusion grade (TMPG) were evaluated as previously described.11,12 The presence of TIMI ≤2 in the final angiogram was accepted as no-reflow.
The NS was calculated using the following parameters, serum albumin, serum total cholesterol, neutrophil-to-lymphocyte ratio (NLR), and lymphocyte-to-monocyte (LMR) ratio as described in Supplementary file 1. Using this scale, group 1 consisted of patients with NS of 0–1, and 2, and group 2 consisted of patients with NS of 3 and 4.
The long-term mortality encompassed deaths that occurred after being discharged from the hospital. The long-term survival rates were determined using data from the National Death Registry System.
Statistical Analysis
The data analyses were conducted using R software v. 4.2.2 (R statistical software, Institute for Statistics and Mathematics, Vienna, Austria). The normal distribution assumption was assessed with the Kolmogorov–Smirnov test. Normally distributed variables were expressed as mean (SD) and non-normally distributed variables were expressed as median (interquartile range (IQR)).
Categorical data were presented using numbers and percentages. The χ2 test or Fisher’s exact test was used to compare categorical variables. For comparing continuous variables between the groups, the independent Student’s t-test or Mann–Whitney U tests were used. Univariable logistic regression analysis was used to detect the association of variables with mortality. A baseline multivariable logistic regression model was built with variables, including age, hemoglobin (Hb), red cell distribution width (RDW), LVEF, lesion length, thrombus burden grade, female gender, HT, DM, cigarette smoking, hyperlipidemia, and no-reflow, which were detected as significantly correlated with a P < .05 in univariable regression or clinically relevant with the presence of mortality. Model 1 and model 2 were created by adding the NS as continuous and as categorical to the baseline model, respectively. Multicollinearity was evaluated with VIF (variance inflation factor >3) and tolerance (<.1) values. The independent contributions of each variable to the variance of the results were calculated by the ratio of partial X2 to the total X2 of the model. The discriminative ability of model 1 and the baseline model was compared using receiver operating characteristics (ROC) curve analysis. For the model performance comparisons, the Akaike index criterion (AIC), 13 Bayesian index criterion (BIC), 14 Brier-scaled score, 15 Nagelkarke R2, and c-statistic were calculated. Better model performance was indicated with lower levels of AIC, and Brier-scaled score and higher levels of Nagelkarke R2 and c-statistic. 16 Decision curve analysis was performed to calculate the net benefit of model 1 over the baseline model to obtain the additive effect of the NS. The results were analyzed based on a significance threshold of a 2-sided P < .05 and a 95% confidence interval (CI). Kaplan–Meier survival curves were used to compare mortality rates between study groups.
Results
Comparison of Demographic, Clinical, and Laboratory Features of Study Groups.
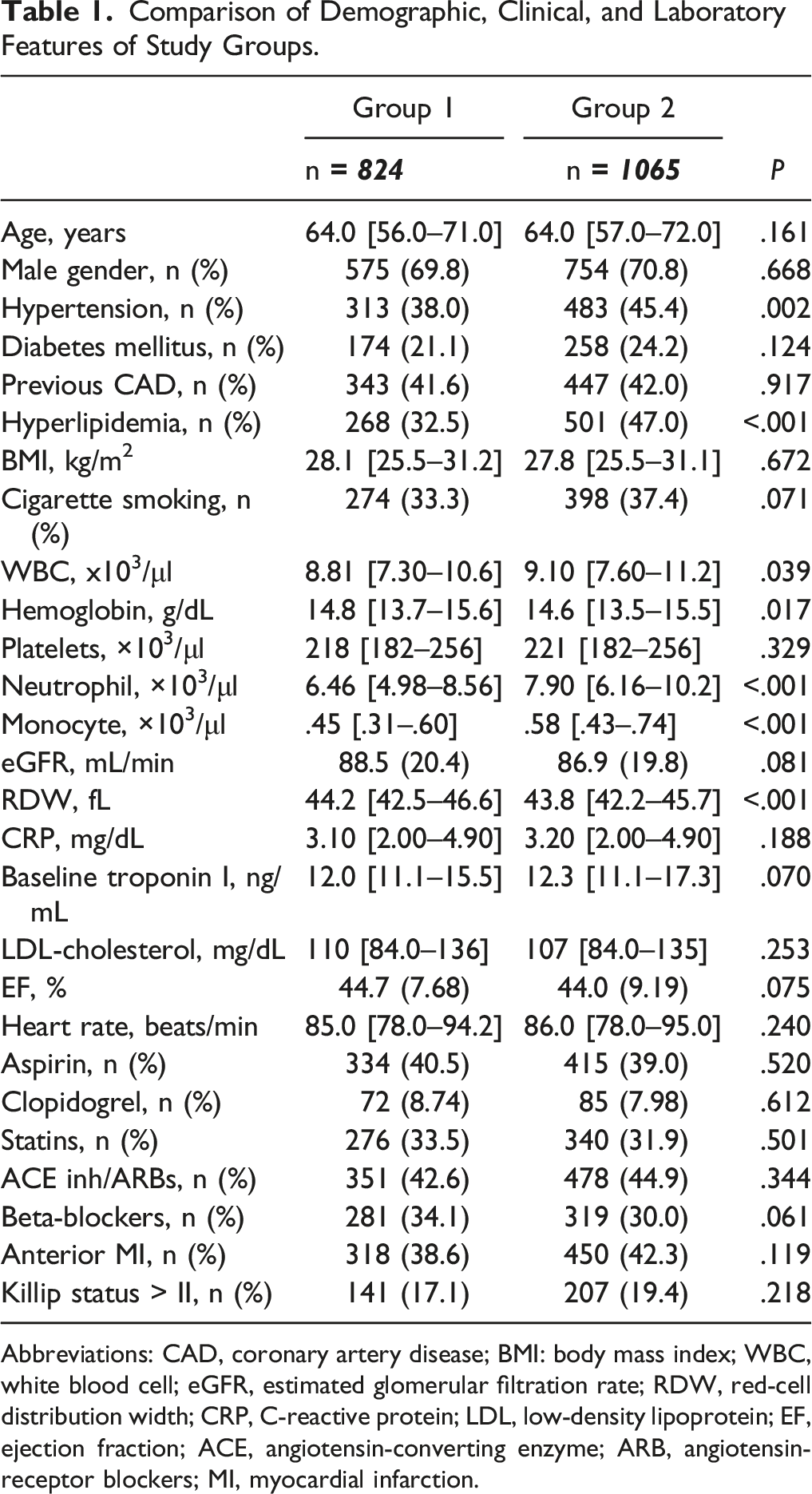
Abbreviations: CAD, coronary artery disease; BMI: body mass index; WBC, white blood cell; eGFR, estimated glomerular filtration rate; RDW, red-cell distribution width; CRP, C-reactive protein; LDL, low-density lipoprotein; EF, ejection fraction; ACE, angiotensin-converting enzyme; ARB, angiotensin-receptor blockers; MI, myocardial infarction.
Comparison of Naples Score Parameters Between Study Groups.
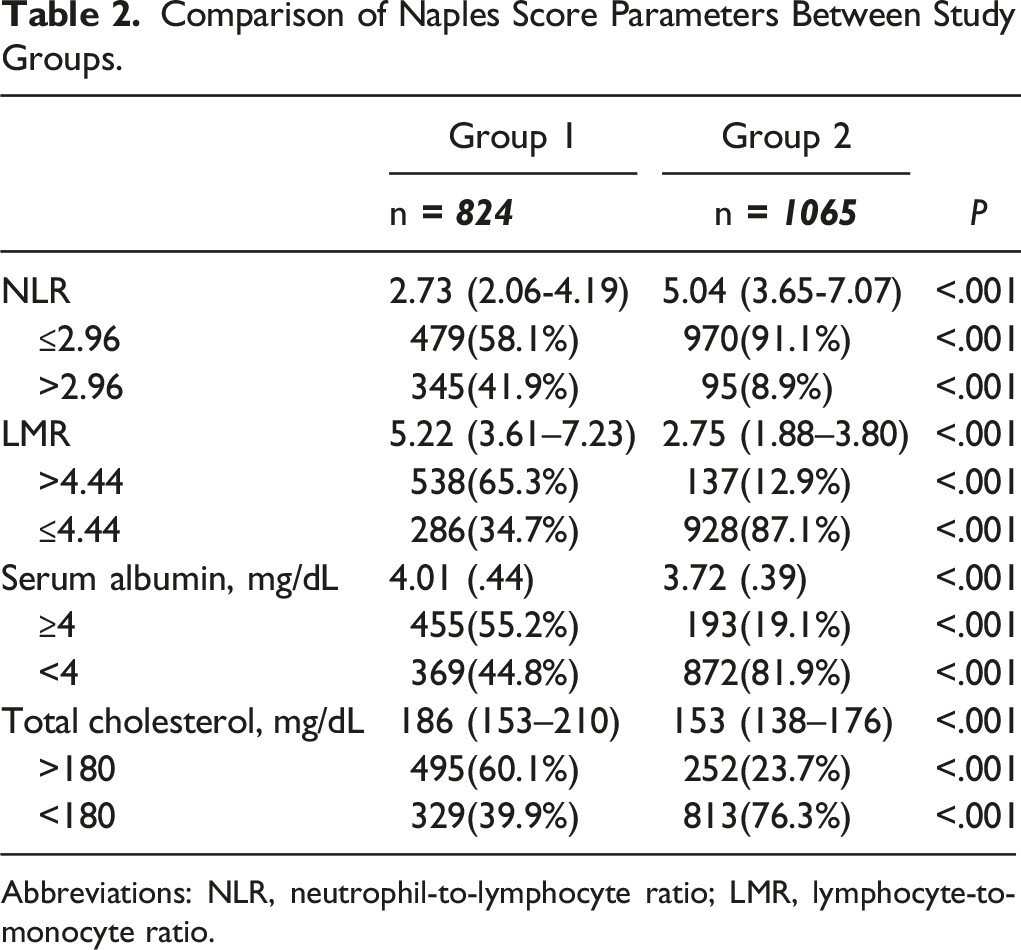
Abbreviations: NLR, neutrophil-to-lymphocyte ratio; LMR, lymphocyte-to-monocyte ratio.
Baseline Angiographic, Periprocedural Characteristics and Mortality Rates According to Naples Score Groups in Patients with STEMI.
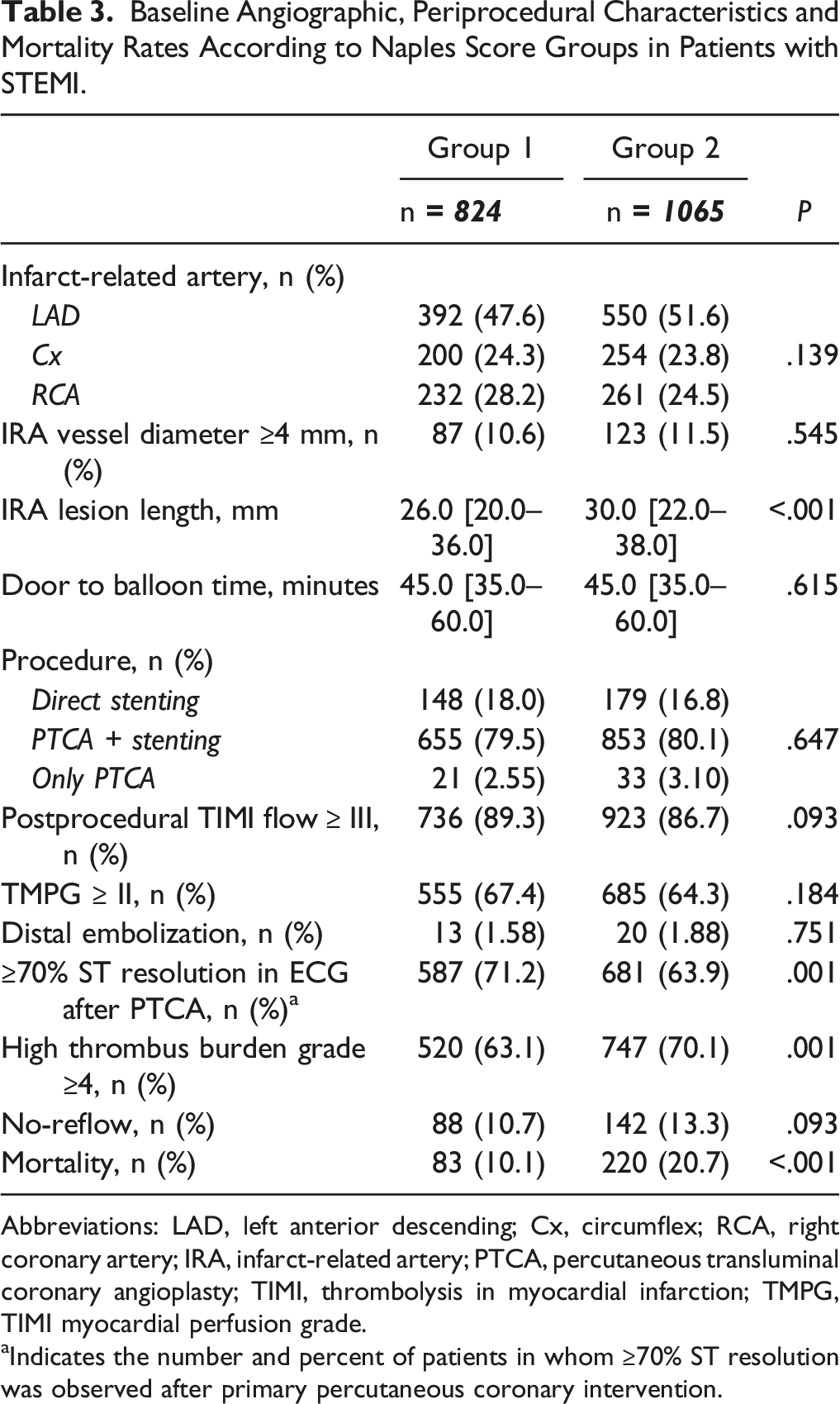
Abbreviations: LAD, left anterior descending; Cx, circumflex; RCA, right coronary artery; IRA, infarct-related artery; PTCA, percutaneous transluminal coronary angioplasty; TIMI, thrombolysis in myocardial infarction; TMPG, TIMI myocardial perfusion grade.
aIndicates the number and percent of patients in whom ≥70% ST resolution was observed after primary percutaneous coronary intervention.
Multivariable Models for Detecting Long-Term Mortality in STEMI Patients.
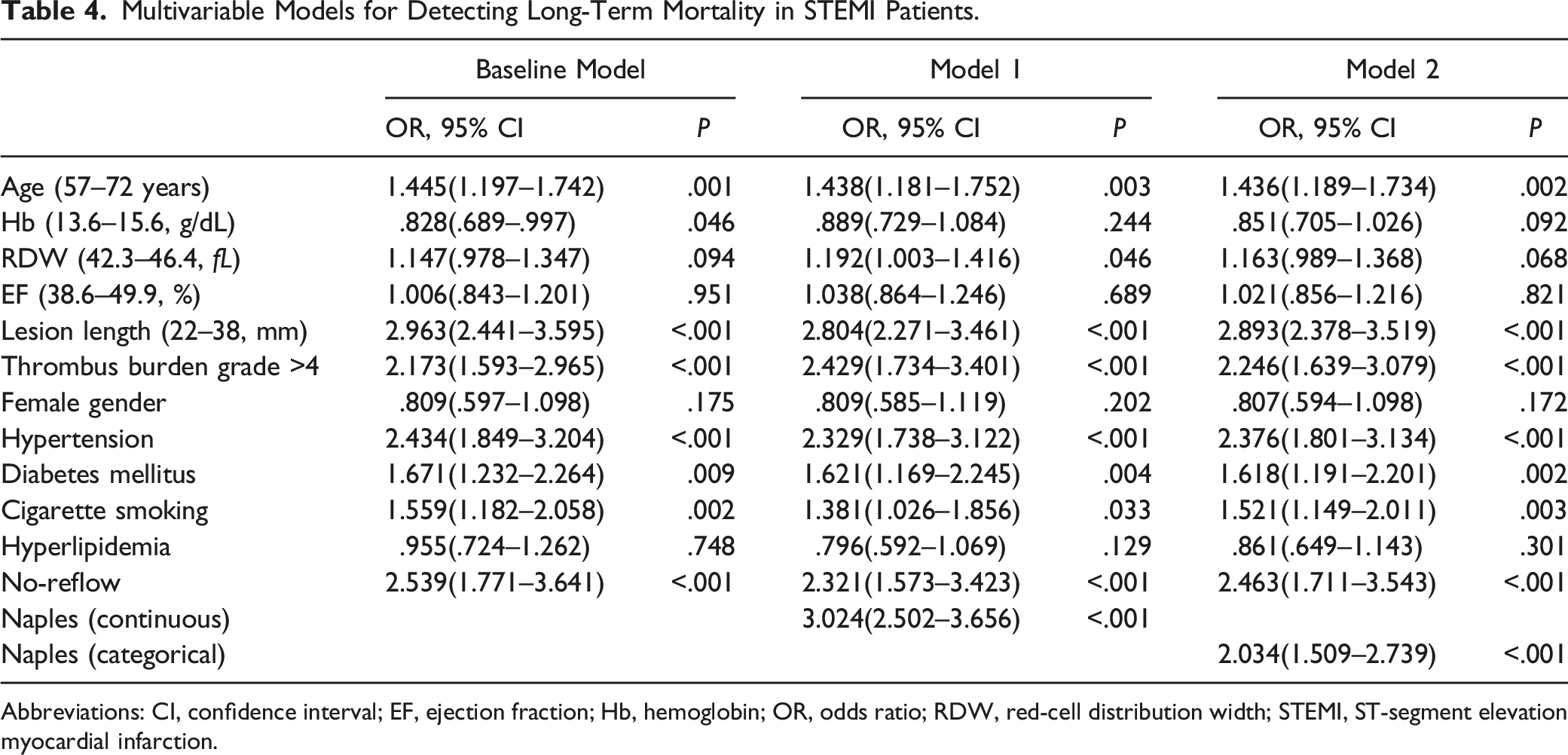
Abbreviations: CI, confidence interval; EF, ejection fraction; Hb, hemoglobin; OR, odds ratio; RDW, red-cell distribution width; STEMI, ST-segment elevation myocardial infarction.
Performances of Models.
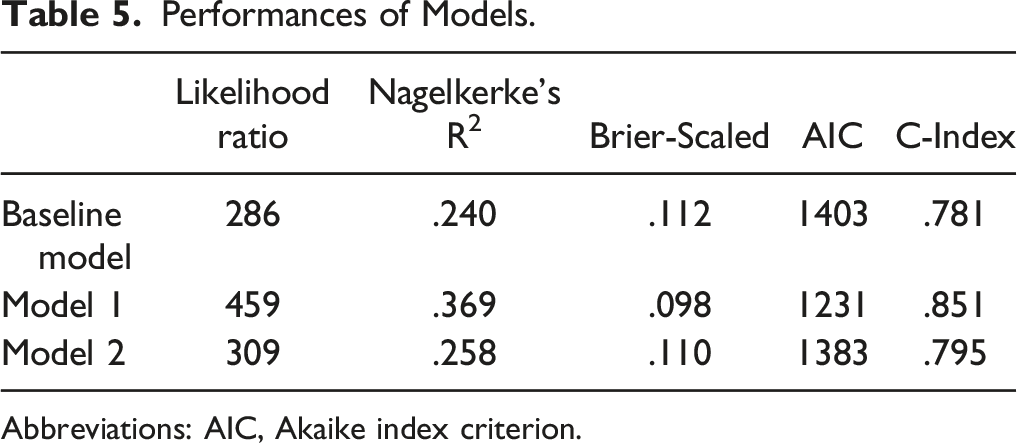
Abbreviations: AIC, Akaike index criterion.
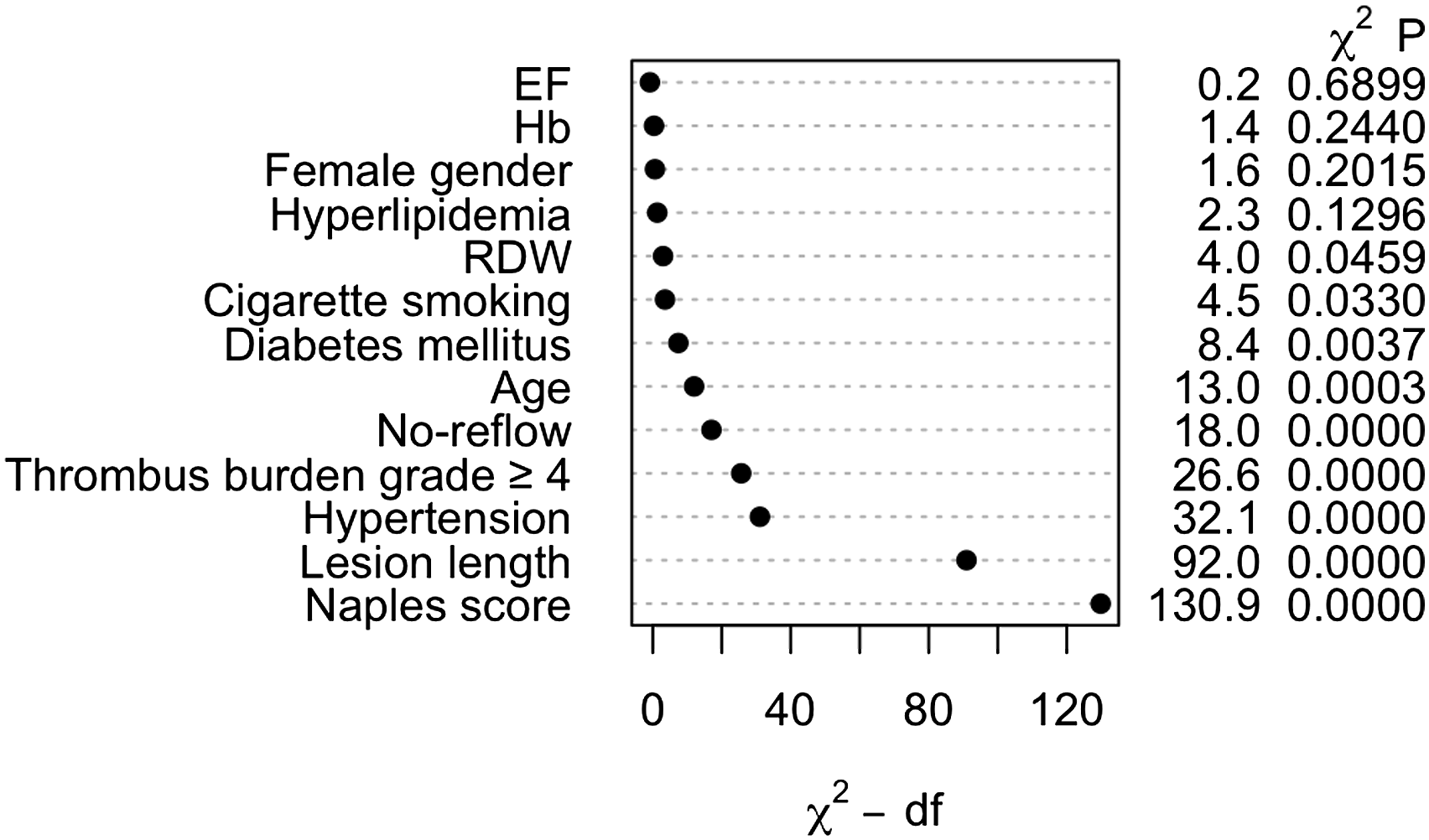
Ranking of importance of predictors of mortality in the multivariable model.
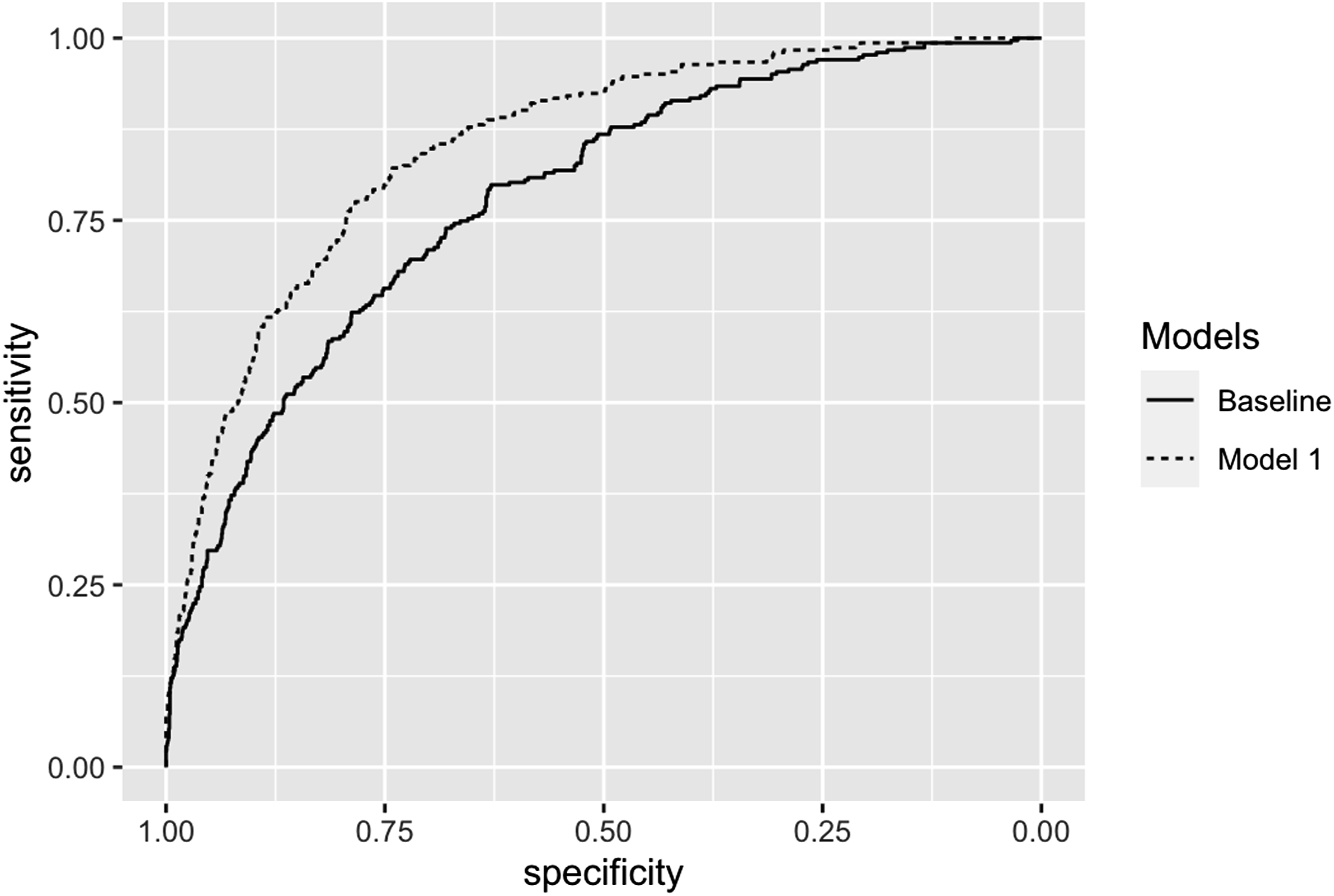
The receiver operating characteristics comparison of the baseline model and model 1.
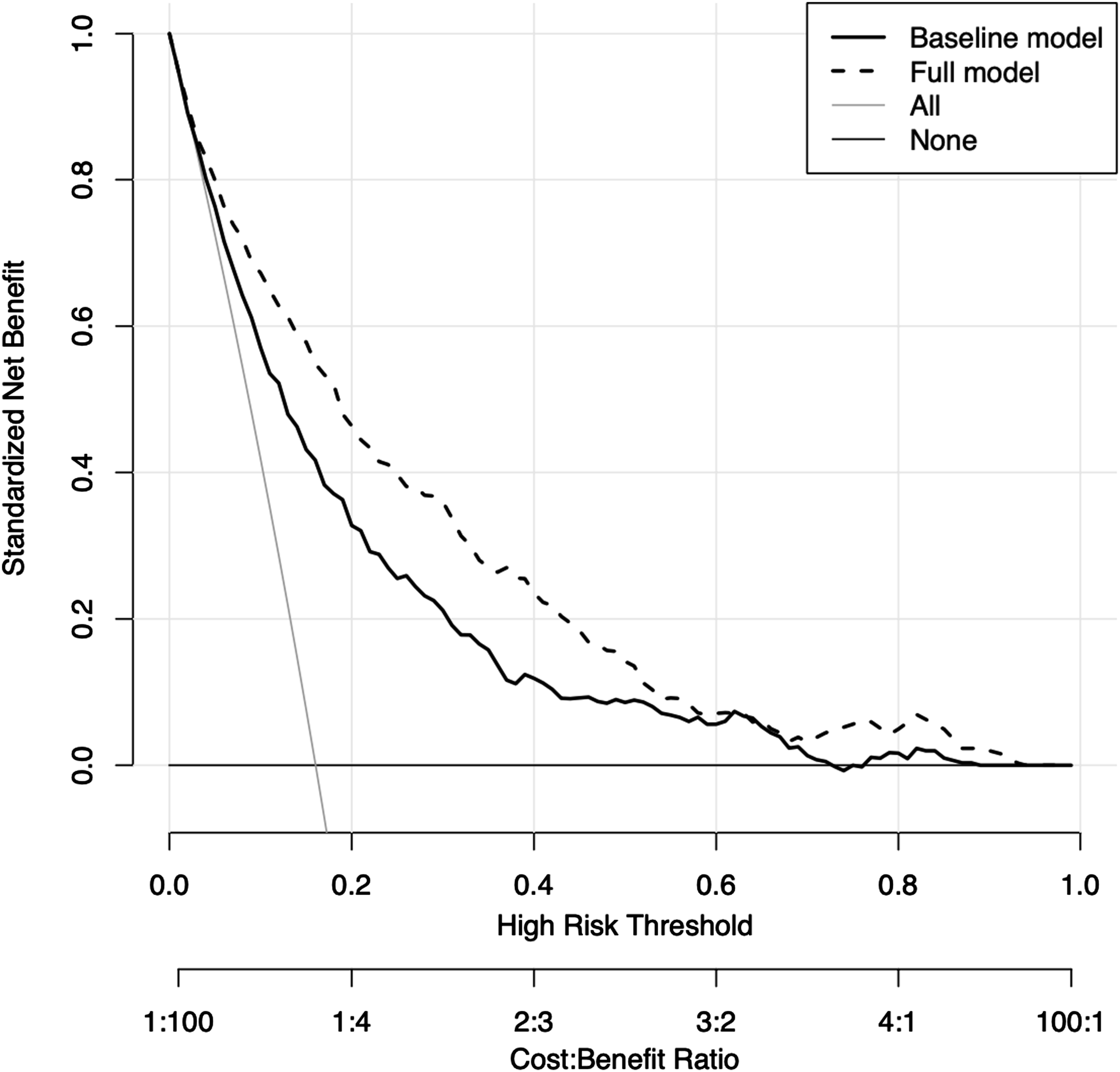
Decision curve analysis of baseline model and model 1.
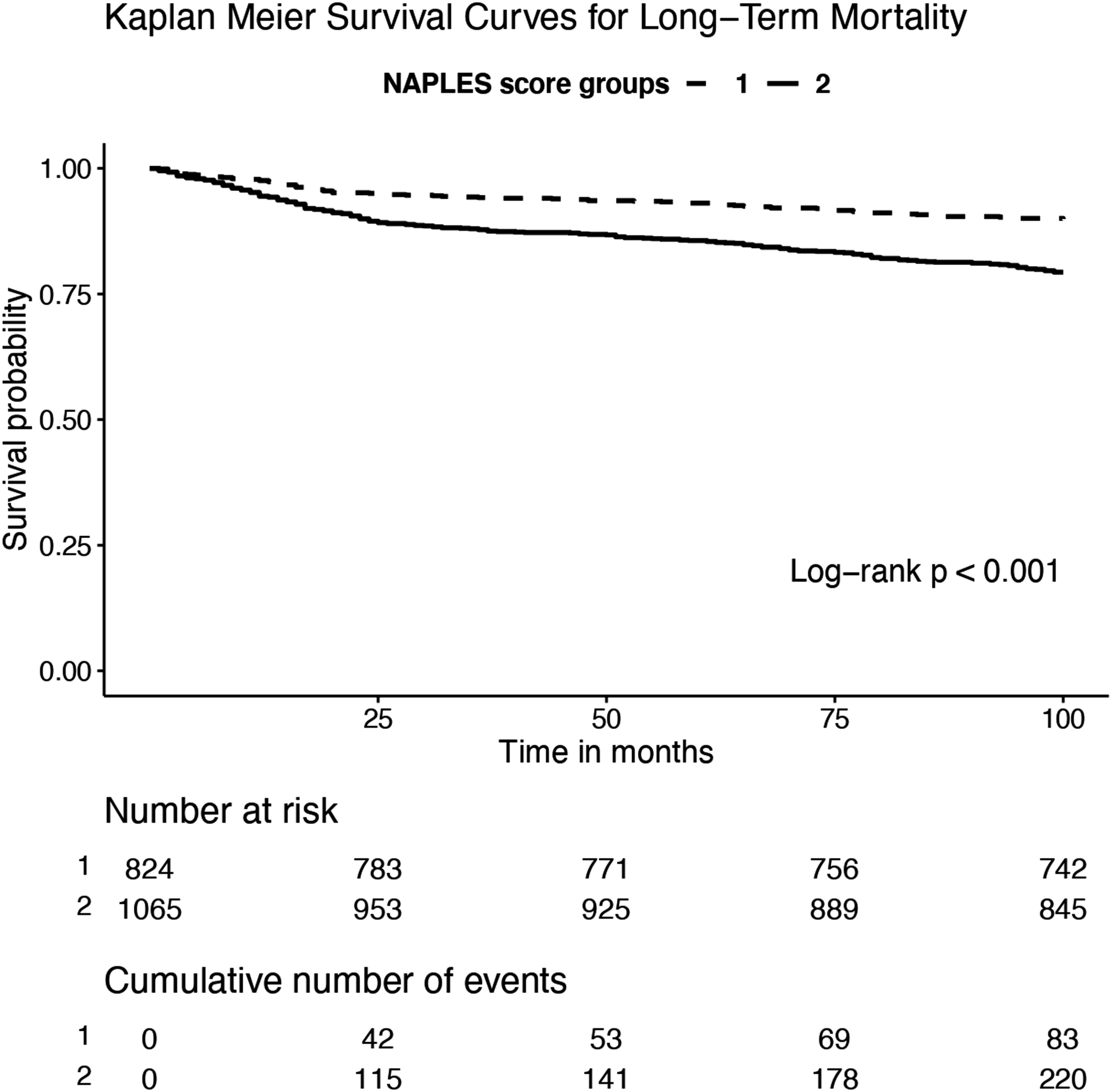
Kaplan–Meier survival curves of study groups.
Discussion
This study identified that patients with high NS had higher long-term mortality rates than patients with low NS. Additionally, the NS was an independent predictor of long-term mortality, and adding the NS to the baseline prediction model improved model performance statistics and had a higher net-benefit effect on the detection of long-term mortality.
Although several improvements have been achieved in the treatment of STEMI over the years, long-term mortality rates are still high worldwide. Several factors can influence the high risk of long-term mortality in those patients. Older age, presence of HT and DM, and cigarette smoking have been reported as worse prognostic factors for long-term mortality in STEMI patients.17-20 Rossington et al. 21 reported that no-reflow and high thrombus burden were independent predictors of mortality in STEMI patients. Similarly with the above findings, this study showed these variables as independently associated with long-term mortality in patients with STEMI. The baseline model including those variables in our study had a good discriminative ability for long-term mortality with an AUC of .781.
Inflammation plays a critical role both in the pathogenesis and prognosis of STEMI. Inflammation leads to the instability of atherosclerotic plaques and provides the adherence of thrombus to the affected plaque surface.3,4 Ruptured atherosclerotic plaques in STEMI might cause microcirculation dysfunction, which exacerbates systemic inflammatory response. 3 A high inflammatory state is associated with worse outcomes and high neutrophil count was an independent predictor of mortality in STEMI. 22 However, lymphocytes have a regulated inflammatory process, which leads to a lower immune response and suppressed myocardial damage. 23 Thus, lower lymphocyte counts have been found to be associated with a higher risk of cardiovascular mortality. 24 Sawant et al. 6 showed that STEMI patients with high NLR had a higher mortality rate and NLR was independently associated with long-term mortality in such patients. Monocytes are important in the development of atherosclerosis and high monocyte levels have been related to adverse events in STEMI. 25 So, a low LMR is expected to be associated with a greater risk of adverse events in STEMI patients. Kiris et al. 8 reported that low LMR was associated with 30-day and long-term mortality in STEMI patients. Albumin is essential for maintaining plasma oncotic pressure at a target level and is a negative acute phase reactant, which has protective properties against inflammation. 26 Hypoalbuminemia can lead to elevated inflammation and oxidative damage. 27 Albumin acts as an antioxidant, inhibits the binding of fibrinogen to endothelial cells, and reduces thrombotic activity which are result in lower atherosclerosis. 28 Hypoalbuminemia is a potent predictor of cardiovascular and all-cause mortality regardless of comorbidities and normalization of albumin reduces mortality risk. 29 Bicciré et al. 7 showed that low level of albumin was associated with mortality in STEMI patients. Although it is well known that high total cholesterol is a risk factor for atherosclerosis, 30 it has been demonstrated as a paradox that low total cholesterol levels were associated with higher mortality. Bae et al. 31 showed that total cholesterol level <160 mg/dL was associated with mortality from cardiovascular diseases. Similarly, Gnanenthiran et al. 32 demonstrated the association between low total cholesterol and major adverse cardiovascular events. Rauchaus et al. showed that heart failure patients with low cholesterol levels had higher mortality rates compared to control patients. 33 Tracy et al. reported that hypercholesterolemia was associated with lower mortality in acute coronary syndrome (ACS) patients. 9 Similar results in ACS patients were demonstrated in a study conducted by Ahmad et al. 34 But the underlying mechanism of this paradigm could not have been explained clearly yet. Especially low cholesterol levels were associated with non-cardiac mortality. According to the general consensus, when total cholesterol drops to less than 160 mg/dL, the risk of non-cardiac death rises due to stroke, heart disease, and cancer.35,36 For example, lung cancer is the most linked disease of non-cardiac mortality that is related to low cholesterol levels. 35 Although the target is to lower the cholesterol level below a certain level in coronary artery disease patients, low cholesterol was not only found to be associated with mortality, but also linked to liver disease, bowel disease, chronic bronchitis, suicide, and cancer. 37
The NS has emerged as a useful prognostic scoring model in cancer patients. 38 The NS has been recently reported to be associated with in-hospital and short-term mortality in STEMI patients. 39 However, the predictive capability of NS for long-term mortality of STEMI patients was lacking in the literature. The logical explanation of this prognostic relationship could be explained in several possible ways. Higher NLR and lower LMR, albumin, and total cholesterol levels lead a higher NS in combination, which has been reported as associated with higher ischemic events, myocardial infarction, and aggravations of heart failure providing higher rates of mortality in cardiac patients. Higher NLR and lower LMR values were associated with ischemic stroke.40,41 Similarly, lower LMR and albumin levels were associated with higher rates of myocardial infarction.41,42 Heart failure patients with higher NLR, or lower LMR, albumin, and total cholesterol levels had higher rates of in-hospital death.43-46 In a consequence, patients with a higher NS should be followed more closely and treated more aggressively for reducing ischemic events, worsening and hospitalization from heart failure, and myocardial infarction.
Because the higher values of NLR and lower values of LMR, albumin, and total cholesterol were associated with mortality in STEMI, a composite of those variables, the NS, might better predict mortality than the individual components. Adding the NS to a baseline model led to the highest contribution to the model, improved the model performances, and had a net clinical benefit of detecting mortality in STEMI patients.
Limitations
Retrospective and single-center study design were the major limitations of this study. Due to the cross-sectional study, a causal relationship between NS and long-term mortality could not be established. The single-geographical location was another limitation that reduces the generalizability of the study findings. Because this study consisted solely of STEMI patients, the results are not applicable to other ACS populations. There might be uncontrolled covariates that might affect the multivariable regression results. The lack of follow-up values of variables, which are the components of the NS was another limitation and it might have been better to interpret the follow-up values of NS of patients in this study.
Conclusion
As easily accessible and calculable risk score, the NS might be used for risk stratification for long-term mortality in patients with STEMI undergoing pPCI.
Supplemental Material
Supplemental Material - Evaluation of Naples Score for Long-Term Mortality in Patients With ST-Segment Elevation Myocardial Infarction Undergoing Primary Percutaneous Coronary Intervention
Supplemental Material for Evaluation of Naples Score for Long-Term Mortality in Patients With ST-Segment Elevation Myocardial Infarction Undergoing Primary Percutaneous Coronary Intervention by Faysal Şaylık, Tufan Çınar, Murat Selçuk, Tayyar Akbulut, Mert İlker Hayıroğlu, and İbrahim Halil Tanboğa in Angiology
Footnotes
Author Contribution
All authors contributed to: (1) substantial contributions to conception and design, or acquisition of data, or analysis and interpretation of data, (2) drafting the article or revising it critically for important intellectual content, and (3) final approval of the version to be published.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.