
Abstract
Dyslipidemia is an important risk factor for cardiovascular morbidity and mortality. Although low-density lipoprotein (LDL) is primarily responsible, the importance of triglyceride (TG) and high-density lipoprotein (HDL) has also been recognized. The present study investigated the effect of the atherogenic index of plasma (AIP), in which atherogenic and protective lipoproteins were evaluated together, on the initial flow in patients with ST elevation myocardial infarction. AIP was calculated as log(TG/HDL-cholesterol). Patients included in the study (n = 1535) were divided into Thrombolysis in Myocardial Infarction (TIMI) flow grade 0 and >0. AIP was found to be significantly different between 2 groups (.55 ± .23 vs .67 ± .21; P < .001). AIP was an independent predictor for pre-intervention TIMI flow (Odds Ratio: 2.778). A moderate correlation was found between TIMI frame count measurements, calculated in patients with TIMI 2–3, and AIP (Pearson correlation coefficient: .63, P < .001). In the receiver operating characteristic analysis, AIP showed the highest area under curve (AUC) compared with other lipid parameters for predicting vascular patency. The AUC of AIP was .634, the cut-off value was .59, and the sensitivity and specificity were 67.6% and 68.4%, respectively (P < .001). In conclusion, AIP was found to be an important marker affecting pre-percutaneous coronary intervention TIMI flow.
Keywords
Introduction
Dyslipidemia is a well-established risk factor for cardiovascular disease (CVD). 1 The increase in low-density lipoprotein cholesterol (LDL-C) and circulating triglyceride (TG) and the decrease in high-density lipoprotein cholesterol (HDL-C) levels affect clinical outcomes. 2 This condition has been termed atherogenic dyslipidemia. 3 Although LDL-C concentrations play a fundamental role in the relationship of lipids to CVD, the atherogenic potential of a high TG has also attracted attention.4,5
The atherogenic index of plasma (AIP) is a powerful and sensitive index reflecting the interaction between atherogenic and protective lipoproteins. This index is calculated as log(TG/HDL-C). AIP <.1 was associated with low risk, .1–.24 with medium risk, and >.24 with high risk. 6 AIP has been associated with several risk factors for CVD, such as abdominal obesity, insulin resistance, and metabolic syndrome.7,8 AIP stands out as a strong predictor of atherosclerosis and coronary heart disease. A significant correlation was found between protective and atherogenic lipoproteins and smaller LDL-C particles. 9
Although the results of high AIP on long-term survival after revascularization in cases presenting with the acute coronary syndrome are known, there are limited and low sample data on thrombus burden and vascular patency during ST elevation myocardial infarction (STEMI). Thrombolysis in myocardial infarction (TIMI) flow grade (TFG) and TIMI frame count (TFC), which evaluate angiographic coronary blood flow as a result of primary percutaneous intervention (pPCI), are important scoring systems associated with the development of heart failure, impaired left ventricular ejection fraction, and mortality after STEMI. 10
The present study was designed to investigate whether API, which is considered a marker of long-term cardiovascular prognosis, affects pre-pPCI TIMI flow.
Methods
Study Population
The present study had a retrospective design. The study population consisted of 1535 patients. Patients who attended the emergency department of our high-volume tertiary-level hospital between June 2016 and December 2019 and were admitted to the catheter laboratory for pPCI after being diagnosed with acute STEMI were included in the study. The symptoms of the patients were within the first 12 h. Clopidogrel (600 mg) or ticagrelor (180 mg) with aspirin (300 mg) and weight-adjusted heparin were administered to each patient at the time of diagnosis in the emergency department before the transfer to the laboratory. The diagnosis of STEMI was made based on the latest guidelines of the European Society of Cardiology. 11 Demographic and clinical characteristics, previous medical history, physical examination, laboratory examination, and intervention-related data were obtained from the patient file and hospital database. Patients with advanced kidney and liver disease, malignancy, history of coagulopathy, lactation, pregnancy, and previous use of anti-platelet and anti-lipid agents were not included in the study. The definition of diabetes mellitus was determined according to the American Association of Clinical Endocrinology Clinical Practice guideline. 12 Patients were grouped into current smokers and non-smokers for smoking status. Ethics committee approval was obtained from Dışkapı Yıldırım Beyazıt Training and Research Hospital.
Blood Samples
It was determined from the hospital records that blood samples were obtained at 6 am the following day. Samples were studied with Atellica CH 930 chemistry analyzer, Siemens Healthcare, Erlangen, Germany. AIP was calculated as log(TG/HDL-C mmol/l). 6
Angiographic Results
Coronary angiography was performed on all study patients using the Judkins technique using 6F or 7F guide catheters via the femoral or radial route. Two expert interventional cardiologists, blinded to all clinical data, analyzed the digital angiograms.
TFG was grouped according to the degree of coronary blood flow. In the first angiographic recording images, completely occluded vessels were determined as no-reflow and the state in which the flow was present, albeit partially, was determined as reflow. The TIMI flow grade was assessed as previously defined at the TIMI Angiographic Core Laboratory. 13 According to this scoring system; TIMI 0 was defined as the absence of antegrade flow, TIMI 1 flow not reaching the distal vascular bed even though it went beyond the occlusion, TIMI 2 as delayed antegrade flow, and TIMI 3 as normal flow. TIMI frame count was also calculated from the records of patients with TIMI 2 and 3 flows. Frame counts were determined using the method described by Gibson et al. 13 Accordingly, the initial frame was determined as the first frame where the dye completely entered the coronary, and the last frame was the frame in which the dye reached the last points specified for the arteries. These distal landmarks are as follows: The distal bifurcation point (Whale’s tail) for the left anterior descending artery (LAD), the distal branch of the lateral branch furthest from the coronary ostium for the circumflex artery (CX), and the first branch to branch of the posterolateral artery for right coronary artery (RCA). These frame counts are corrected for the longer length of the LAD by dividing by 1.7 to arrive at the corrected TIMI frame count (cTFC). Lesion characteristics were determined by the American College of Cardiology (ACC) and the American Heart Association (AHA) coronary lesion classification. 14
Statistical Analysis
SPSS statistical software program was used for statistical analysis (IBM SPSS Inc., Chicago, IL, USA). The distribution characteristics of the variables were evaluated using the Shapiro–Wilk test. Student’s t-test was used to analyze normally distributed variables and was expressed as mean ± standard deviation. The Mann–Whitney U test was used for non-normally distributed variables, expressed as the median (interquartile range). Pearson’s rank correlation analysis was used to determine correlations between variables. Univariate and multivariate analyses of predictors for TIMI flow were performed using bivariate regression analysis. The ability of lipid parameters to discriminate pre-PCI flow was calculated by receiver operating characteristic (ROC) analysis. ROC curve plots the true-positive rate (sensitivity) against the false-positive rate (1-specificity) for all possible cut-off values. P < .05 was considered statistically significant.
Results
Baseline demographic and laboratory characteristics of the patients according to TIMI flow grade.
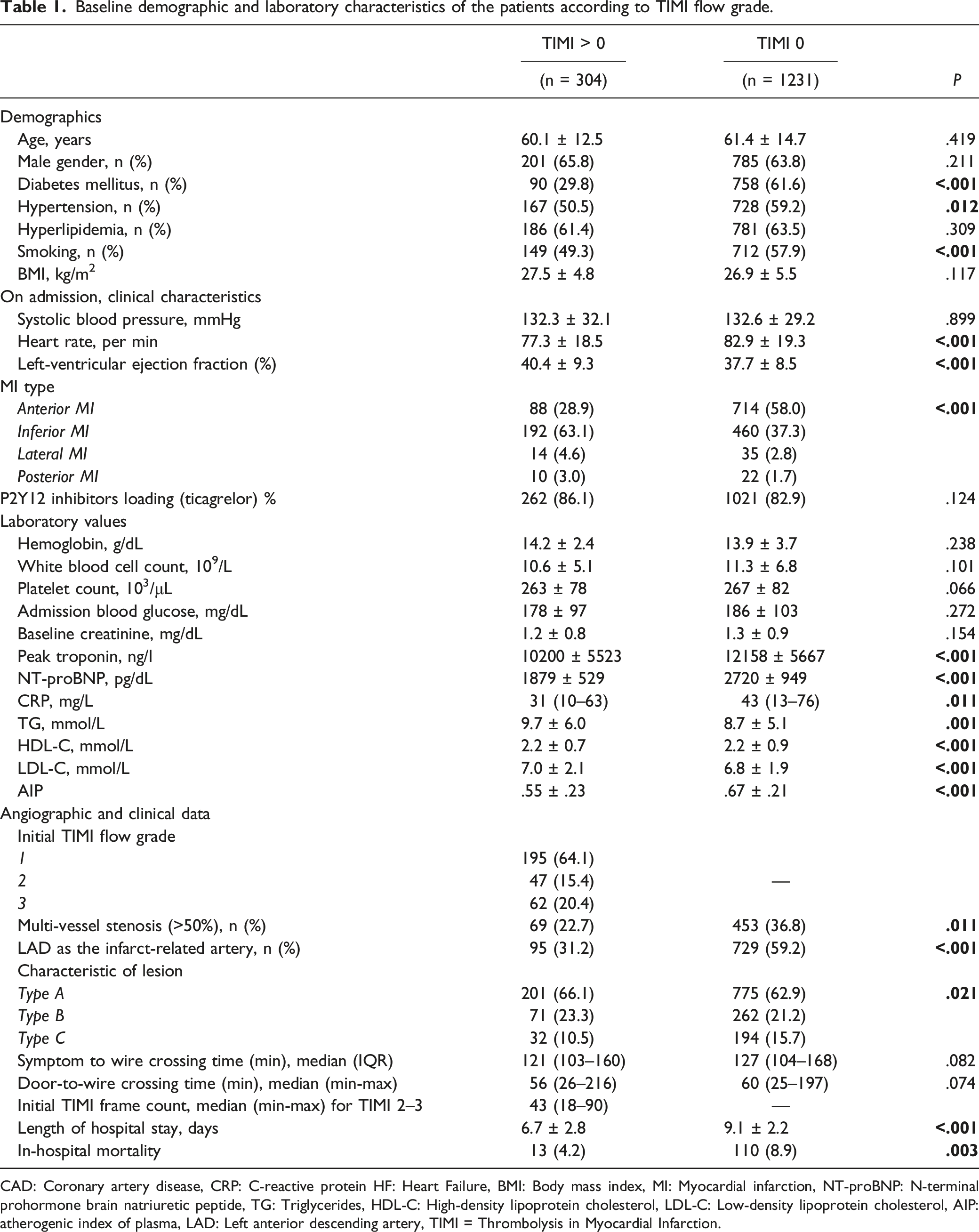
CAD: Coronary artery disease, CRP: C-reactive protein HF: Heart Failure, BMI: Body mass index, MI: Myocardial infarction, NT-proBNP: N-terminal prohormone brain natriuretic peptide, TG: Triglycerides, HDL-C: High-density lipoprotein cholesterol, LDL-C: Low-density lipoprotein cholesterol, AIP: atherogenic index of plasma, LAD: Left anterior descending artery, TIMI = Thrombolysis in Myocardial Infarction.
Predictors of pre-pPCI flow.
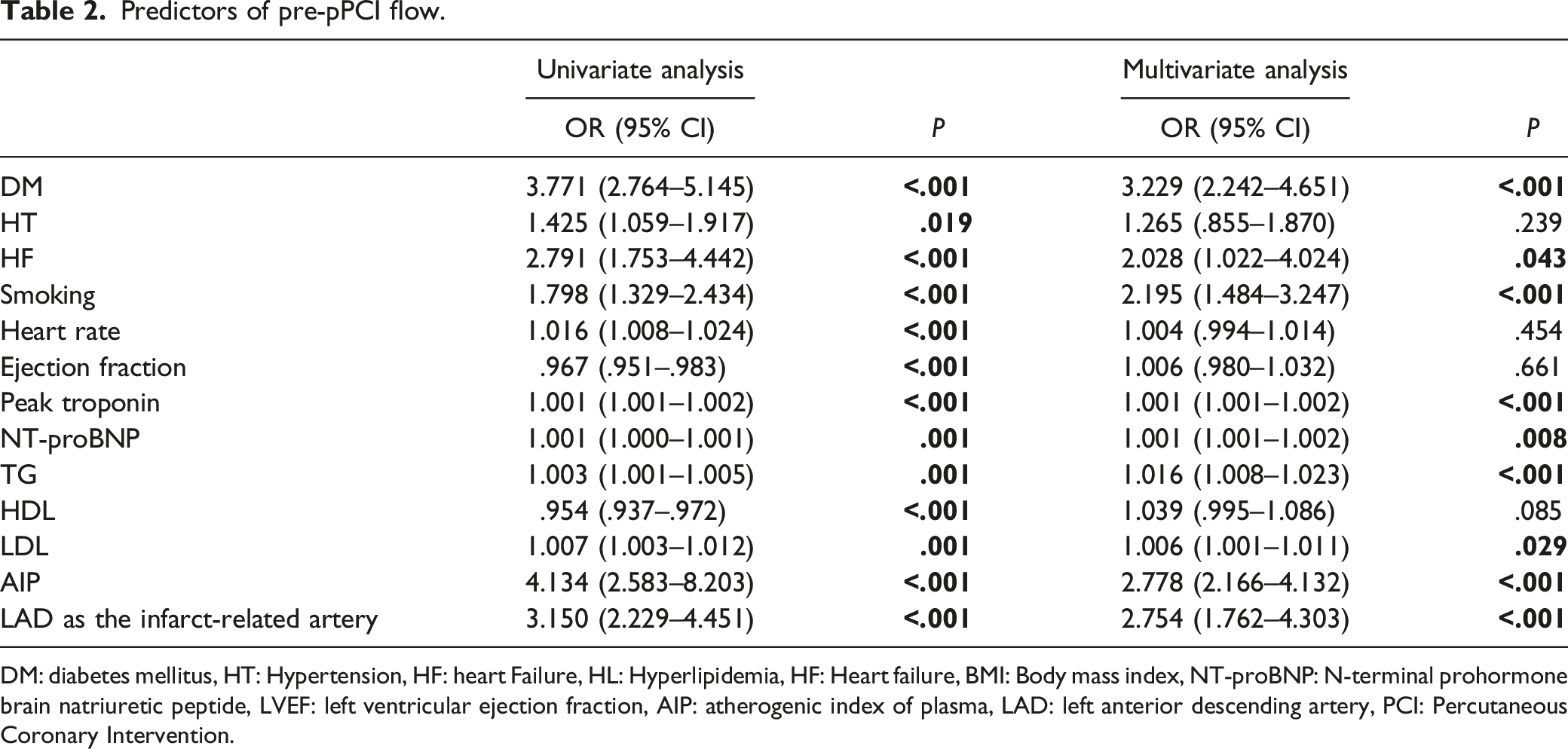
DM: diabetes mellitus, HT: Hypertension, HF: heart Failure, HL: Hyperlipidemia, HF: Heart failure, BMI: Body mass index, NT-proBNP: N-terminal prohormone brain natriuretic peptide, LVEF: left ventricular ejection fraction, AIP: atherogenic index of plasma, LAD: left anterior descending artery, PCI: Percutaneous Coronary Intervention.
TFC of patients with adequate flow from the culprit lesion to the distal landmark region, described above, were calculated as a result of angiographic images. TIMI 2–3 flow was detected in 109 patients. As AIP increased in this patient group, an increase in TFC was also observed, and a moderate correlation was found between AIP and TFC (Pearson correlation co-efficient: .63 R2:0.40, P < .001) (Figure 1). Relationship between thrombolysis in myocardial infarction (TIMI) frame count and atherogenic index of plasma in TIMI flow grade 2–3 patients.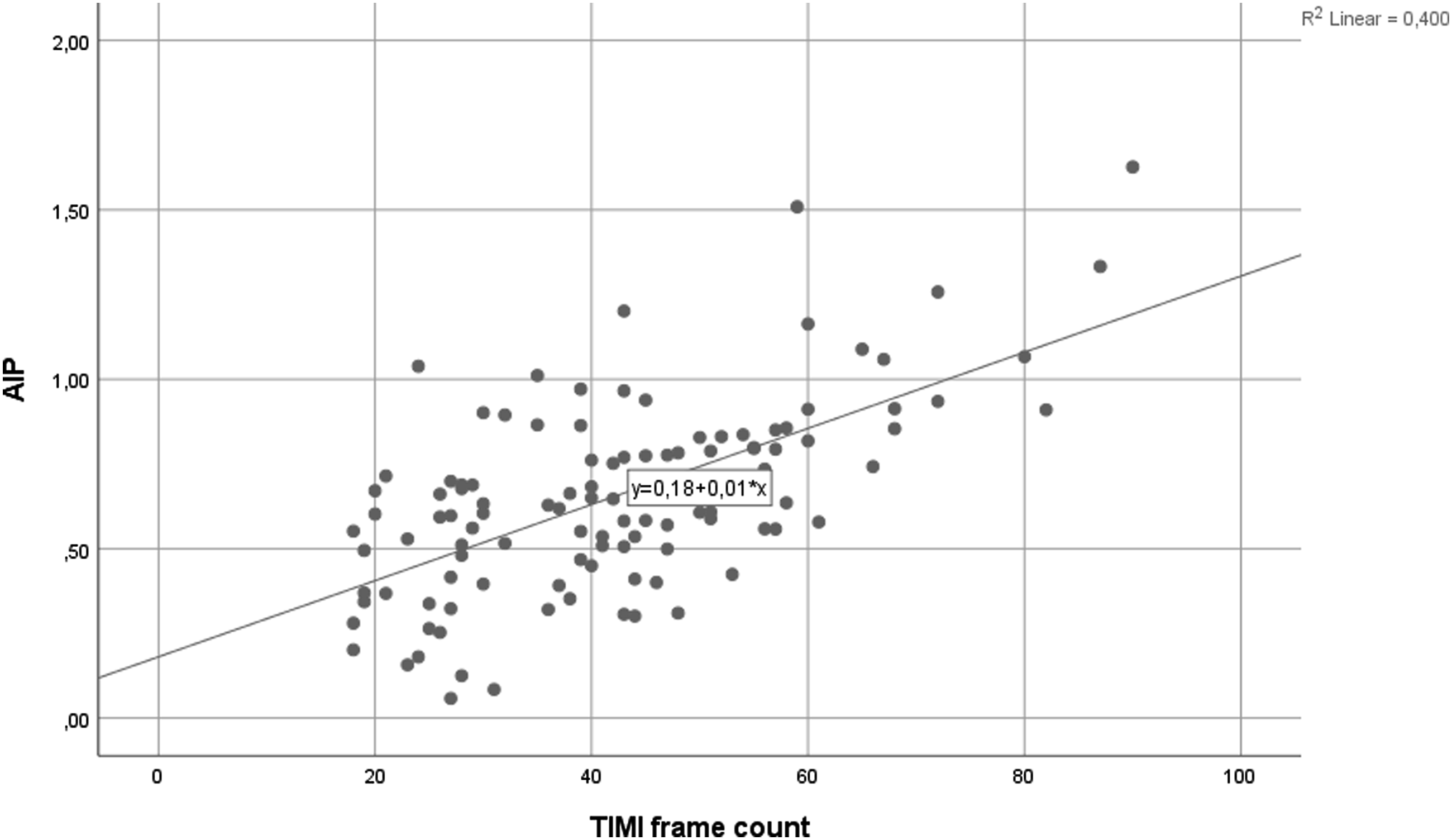
ROC analysis for discriminate pre-PCI flow.
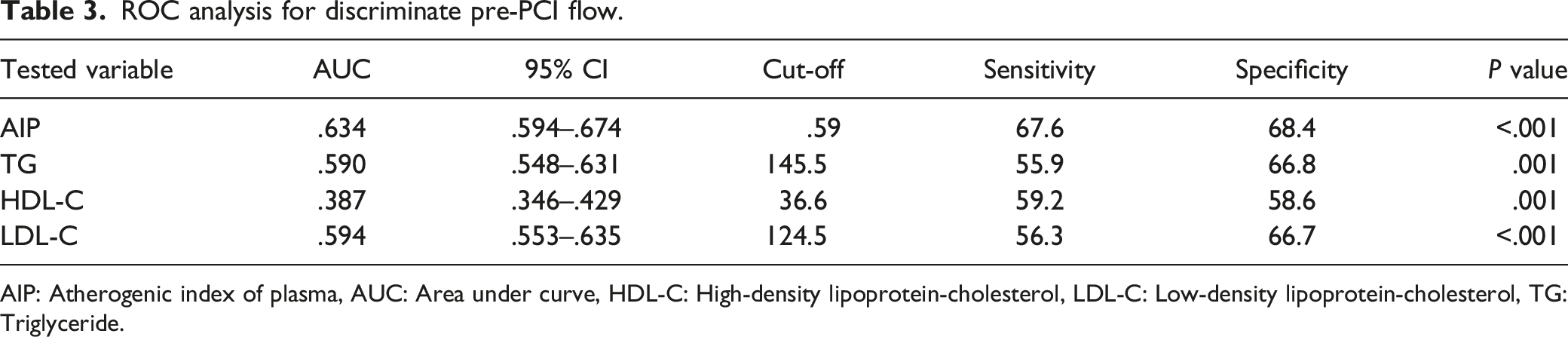
AIP: Atherogenic index of plasma, AUC: Area under curve, HDL-C: High-density lipoprotein-cholesterol, LDL-C: Low-density lipoprotein-cholesterol, TG: Triglyceride.
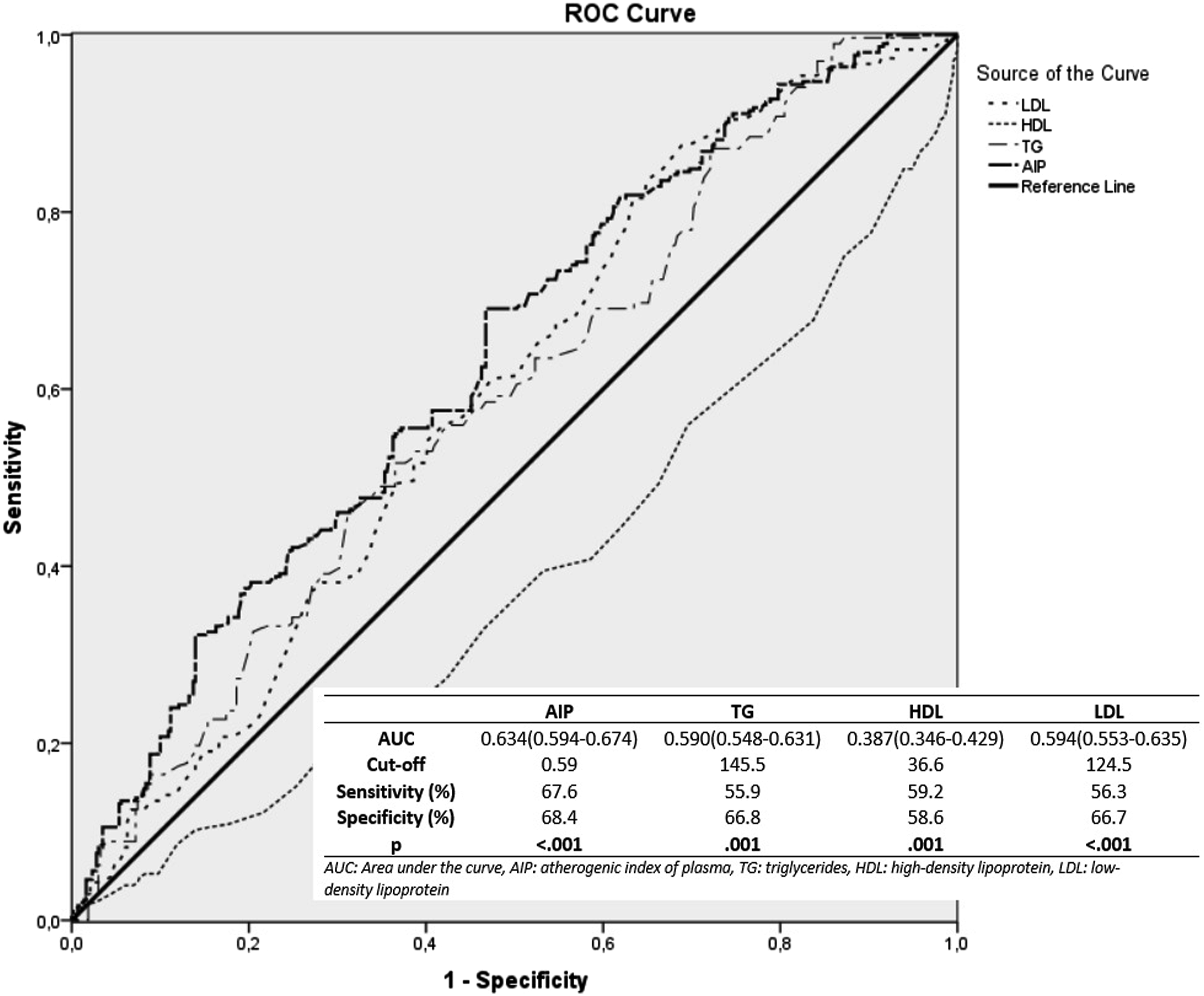
Comparison of low-density lipoprotein-cholesterol (LDL-C), triglyceride (TG), high-density lipoprotein-cholesterol (HDL-C), and atherogenic index of plasma in the receiver operating characteristic (ROC) curve analysis.
Discussion
The present study determined that AIP affects pre-pPCI TIMI flow in STEMI patients and is an independent predictor. It is the first study on this subject in the literature. AIP was associated with better sensitivity and specificity at determined cut-offs in predicting TIMI flow grade before pPCI compared to other lipid subgroups.
Atherosclerosis is a systemic and inflammatory disease that is the primary target for reducing cardiovascular events worldwide. Inflammation at the site of the atheroma plaque has a critical pathophysiological role in acute rupture. 15 Dyslipidemia is among the most important components of this chain of events and has an essential role in the progression of coronary atherosclerosis. 16 LDL-C remains the most critical target in the struggle against atherosclerosis, as recommended by current guidelines. 2 However, studies have shown that small-dense LDL (sdLDL) particles are more valuable than large-dense LDL-C in demonstrating early atherosclerosis. 17 sdLDL is easier to oxidize and foam cell formation occurs faster with interaction with macrophage cells. 18 Oxidized LDL particles were also found to be associated with a decrease in coronary flow reserve (CFR). 19 However, routine measurements of these special particles in the laboratory are not easy due to measurement techniques and cost difficulties. AIP was reported as inversely proportional to the diameter of the LDL-C particles and reflects sdLDL particle size. 9
A meta-analysis evaluating 9 clinical studies determined that non-HDL-C concentrations and obtained TG concentrations were closely associated with coronary atheroma progression and regression, independent of obtained LDL-C, C-reactive protein concentration, and DM status. 20 Also, TG concentrations are directly related to residual lipoproteins that are highly atherogenic and have a high risk of penetrating the arterial wall. 21 When the TG level reaches 180 mg/dL, atherogenic particles become evident. 22 Puri et al. showed that atheroma plaque progression began when the TG level was >200 mg/dL. 20
HDL-C, due to the property to remove excess LDL-C accumulated in the intima of the vessel, is considered cardio/atheroprotective. 23 The source of this antiatherogenic ability is known as reverse cholesterol transport. 24 However, the actions of HDL-C are not limited to this. It also causes vasodilation by increasing nitric oxide synthesis from endothelial cells and improves endothelial function. 25 HDL-C also contributes to the regulation of thrombogenicity by the induction of enzymes such as cyclooxygenase-2 (COX-2) and prostacyclin I2 (PGI2) in endothelial cells. 26 Due to these properties, the decrease in platelet adhesion and antiaggregant effects causes positive results in terms of cardiac events. Peroxidation of lipoproteins is critical in transforming fatty streak formation to atheroma plaque. 27 Oxidation causes inflammation, endothelial dysfunction, and apoptosis. 28 HDL-C, on the other hand, is directly related to enzymes such as paraoxonase-1 (PAO-1), which is involved in transforming oxidized LDLs and has atheroprotective properties. 29
Burke et al. found a significant relationship between thrombosis caused by plaque rupture and high TG, low HDL-C, and high TG/HDL-C ratio. This finding demonstrated the importance of AIP in acute coronary syndrome. 30 The effect of high API values during acute coronary syndrome is thought to be a lipid-related inflammatory process. 31 AIP is strongly associated with high levels of C-reactive protein (CRP). 32 Inflammatory biomarkers, such as high sensitivity C-reactive protein (hsCRP), fibrinogen, and albumin levels, correlate positively with platelet aggregation in STEMI patients undergoing pPCI. 33 Also, studies have shown that both the thrombus load before the procedure and the risk of developing no-reflow during the procedure are closely associated with AIP. In particular, it has been assumed that the risk of no-reflow development is due to arterial wall inflammation caused by TG-rich lipoproteins.28,34 Inflammation is known to be a precursor to fibrin and accelerates platelet aggregation. 33 In addition to AIP, as in our study population, a significant difference may have occurred in pre-procedural TIMI flow grades due to increased platelet aggregation and increased adhesion activity in DM patients, increase in inflammation and LDL oxidation in smoking, and patients presenting with anterior MI which have a higher risk group and higher SYNTAX score compared with inferior MI.35,36
Although the relationship between dyslipidemia and atherosclerosis is well known, thrombus burden during STEMI is also important regarding prognosis. Because dyslipidemia affects platelet function, it can change the clinical status before and after the procedure. Although oxidized LDL-C is the primary molecule for potential platelet response, HDL-C can also show anti-thrombotic properties. In in vitro studies, it can regulate platelet aggregation with its effect on ADP and collagen. 37 In a recent study, AIP was closely associated with pre-intervention thrombus burden. The data of our study was also in agreement with this study. 38
As a result of the mechanisms mentioned earlier, the TG/HDL-C ratio may be related to the TIMI flow during STEMI due to both the diffusiveness of atherosclerosis and the effects on thrombus load. The effect of TG levels on recurrent ischemic events has been proven, even when treated with statins. 39 Treatment with TG-lowering therapy should be a target in these patients. In addition, although AIP studies have been found to predict cardiovascular outcomes after coronary revascularization, the pre-procedural coronary flow should be evaluated as a part of success in procedural complications, cardiac function, and long-term follow-up.
Limitations
The study was designed as single center and retrospective. This study did not evaluate long-term outcomes since we focused on pre-pPCI angiographic data, even though mortality data were available. The effects of anti-platelet and anti-lipid agents could have provided valuable information, but these patients were excluded from the study.
Conclusion
Lipid parameters and subgroup TG and HDL-C ratio, which are a part of routine laboratory evaluation, may contribute to the improvement of long-term results by causing less thrombus burden and less total occluded lesion in STEMI patients.
Footnotes
Author Contributions
All authors contributed to (1) substantial contributions to conception and design, or acquisition of data, or analysis and interpretation of data, (2) drafting the article or revising it critically for important intellectual content, and (3) final approval of the version to be published.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.