
Abstract
The use of beta-blockers (BB) in reduced left ventricular ejection fraction (LVEF) post-myocardial infarction (MI) is associated with reduced 1-year mortality, while their role in patients with mid-range and preserved LVEF post-MI remains controversial. We studied 31,620 patients who presented with acute coronary syndrome (ACS) enrolled in seven Arabian Gulf registries between 2005 and 2017. Patients with LVEF ≤40% were excluded. The remaining cohort was divided into two groups: BB group (n = 15,541) and non-BB group (n = 2,798), based on discharge medications. Patients in the non-BB group were relatively younger (55.3 vs. 57.4, P = .004) but higher risk at presentation; with higher Global Registry of Acute Coronary Events (GRACE) score (119.2 vs 109.2, P < .001), higher percentage of cardiogenic shock (3.5 vs 1.4%, P < .001), despite lower prevalence of comorbidities, such as hypertension and hyperlipidemia. BB use was associated with lower 1-year mortality in a multivariate logistic regression analysis, adjusting for major confounders [adjusted odds ratio (OR): 0.71 (95% CI 0.51–0.99)]. This remained the case in a sensitivity analysis using propensity score matching [adjusted OR: 0.34 (95% CI 0.16–0.73)]. In this study, using Arabian Gulf countries registries, the use of BB after ACS with LVEF >40% was independently associated with lower 1-year mortality.
Introduction
Patients presenting with myocardial infarction (MI) often leave the hospital with multiple drugs, including dual antiplatelet agents, statins, and beta-blockers (BB). All have been shown to reduce mortality in all MI patients except the BB, where its role has been questioned in patients with normal and mildly reduced LVEF.1-3 The data supporting a mortality benefit of BB in patients with MI goes back to 1981 before the revascularization era. Aside from mortality in the pre-revascularization era, there was 1.5% relative reduction in ventricular arrythmias. 4 However, even at the time of fibrinolysis, there was a controversy about its protective role. A large randomized controlled trial showed that there was no difference in the composite outcome of mortality, reinfarction, or cardiac arrest post-fibrinolysis. 5 There was a 0.5% reduction in both reinfarction and ventricular arrhythmia in the group treated with BB but came with the expense of 1.1% increase in cardiogenic shock, and therefore, the recommendation based on this trial was to use it 1 day after fibrinolysis in hemodynamically stable patients. 5
The American College of Cardiology (ACC) and the American Heart Association (AHA) non-ST elevation acute coronary syndrome (NSTE-ACS) 2014 guidelines indicated that it is reasonable to use BB in patients with normal left ventricular (LV) function and NSTE-ACS (Class IIa, Level of Evidence (LOE) C). This recommendation was based on data from meta-analyses that included many studies carried out before coronary stenting was adopted and also included heart failure patients.6-8 The latest ACC/AHA/Society for Cardiovascular Angiography and Interventions (SCAI) coronary artery revascularization guidelines give a class III recommendation, with no benefit in patients with normal left ventricular function who presented with stable coronary artery disease and underwent revascularization. However, the societies also endorsed an unclear benefit in patients post-MI with preserved ejection function and therefore their use should be on an individualized basis. 9 The use of BB in patients after MI with preserved ejection fraction remains debatable in the post-revascularization era.
While some data suggest no protective benefit of BB in patients post-MI without heart failure in the reperfusion era,10-12 others suggest that BB use has a protective role and discontinuation after MI without heart failure may lead to more ACS or mortality.13-16 Recently published data from SWEDEHEART showed no benefit of using BB beyond 1 year and up to 4.5 years 17 However, the benefit from other trials might vary from short-term <30 days, 2 years, or ≥3 years 14,15,18,19 Overall, only a few large registry data included a pre-defined LVEF >40%.15,16,18,19
The present study pooled data from seven Arabian Gulf countries registries, which included patients who presented with ACS. The aim was to establish if patients discharged on BB after ACS admission with ejection fraction >40% have a better survival compared with those who are not on BB at the time of discharge.
Methods
Study Population and Outcomes
This is a retrospective cohort study using data from seven prospective registries: Saudi Project for Assessment of Coronary Events (SPACE), Gulf Registry of Acute Coronary Events (Gulf RACE), Gulf RACE-2, Gulf RACE-3, Gulf Locals with Acute Coronary Syndrome Events Registry (Gulf COAST), Kuwait Reperfusion in ST-Segment–Elevation Myocardial Infarction (Kuwait REPERFUSE), and Saudi Acute Myocardial Infarction Registry (STARS).20-29 The registries represent data from seven countries: Saudi Arabia, Kuwait, Bahrain, Qatar, United Arab Emirates, Oman, and Yemen. They enrolled patients with ACS between 2005 and 2017. All seven registries have in-hospital outcomes. Four of the registries have 1-month and 1-year mortality outcomes (Gulf RACE-2, Gulf COAST, Kuwait REPERFUSE, and STARS). All registries are summarized in Supplementary Table 1. 30 We excluded patients with heart failure with reduced ejection fraction (HFrEF) (LVEF ≤40%) based on index admission echocardiography. We then divided up the patients to beta-blocker use (BB) or non-beta-blocker use (non-BB) based on their discharge medications, which was at the discretion of the primary physician. Primary outcome was 1-year all-cause mortality. Secondary outcome was 1-month mortality.
Study Variables
Study variable included baseline characteristics (i.e., demographics, smoking history, and comorbidities), presentation (i.e., hemodynamics, GRACE score and Killip class, ACS type, LVEF, cardiogenic shock, and cardiac arrest), in-hospital outcomes (i.e., revascularization, recurrent ischemia, heart failure, stroke, bleeding, discharge status, and medications on discharge), and mortality (1-month and 1-year all-cause mortality).
Statistical Analysis
Continuous data were reported as mean (± standard deviation) and categorical data as numbers (percentages). Student’s t test, Chi Square test, and Fisher’s exact test were used as appropriate to analyze data. Given that statistical significance is an insensitive measure of the effect size that can be misinterpreted when the sample size is large, we quantified the effect size using the standardized mean difference for continuous variables and phi coefficient for categorical variables. 10% or less (≤10%) is considered small effect size for both statistics.31,32
To assess the independent effect of BB at discharge on 1-year mortality, we used multivariate logistic regression modeling to adjust for important confounders. We included all the variables that were significantly associated with 1-year mortality in univariate analysis. In addition, we included variables that were significantly associated with BB use in univariate analysis. The final model included the following variables: baseline characteristics (age, sex, ethnicity, current smoking, obesity, diabetes mellitus, hypertension, dyslipidemia, history of coronary artery disease, history of chronic kidney disease, history of heart failure, and history of stroke), presentation characteristics (heart rate, systolic blood pressure, acute coronary syndrome type, cardiogenic shock, cardiac arrest, and Killip class), in-hospital outcomes (revascularization, primary percutaneous coronary intervention (PCI) for ST-elevation myocardial infarction (STEMI), atrial fibrillation, recurrent ischemia, heart failure, stroke, and major bleeding), and medications on discharge (antiplatelet therapy, angiotensin-converting-enzyme (ACE) inhibitors, and statin).
We also performed a sensitivity analysis using propensity score matching. Matching was performed at a ratio of 1:1 using the nearest neighbor method with a caliper width of 0.2 times the standard deviation. Analyses were performed using SAS (version 9.4, The SAS institute, Cary, North Carolina USA). Two-tailed tests were used, and P < .05 was considered statistically significant.
Results
Overall Cohort
A total of 31,620 patients were enrolled in seven Arabian Gulf registries. After excluding patients with LVEF <40%, 18,339 patients were included (15,541 in the BB group and 2,798 in the non-BB group), (Figure 1). Baseline characteristics, presentation, medications on discharge, and hospital course data are summarized in Table 1. Flow chart of the study cohort. ACS, acute coronary syndrome LVEF, left ventricular ejection fraction BB, and beta-blocker. Baseline Characteristics, Presentation, and In-Hospital Outcomes of Patients Discharged on a Beta-Blocker Vs Those Not Discharged on a Beta-Blocker Post-Acute Coronary Syndrome Admission. *Data shown as n (%) values except as noted. **Data as mean ± SD. BB, beta-blocker; BMI, body mass index; GRACE, Global Registry of Acute Coronary Events; ACS, acute coronary syndrome; STEMI, ST-elevation myocardial infarction; NSTEMI, non-ST elevation myocardial infarction; ACEI, angiotensin-converting enzyme inhibitor; ARB, angiotensin II receptor blocker; PCI, percutaneous coronary intervention.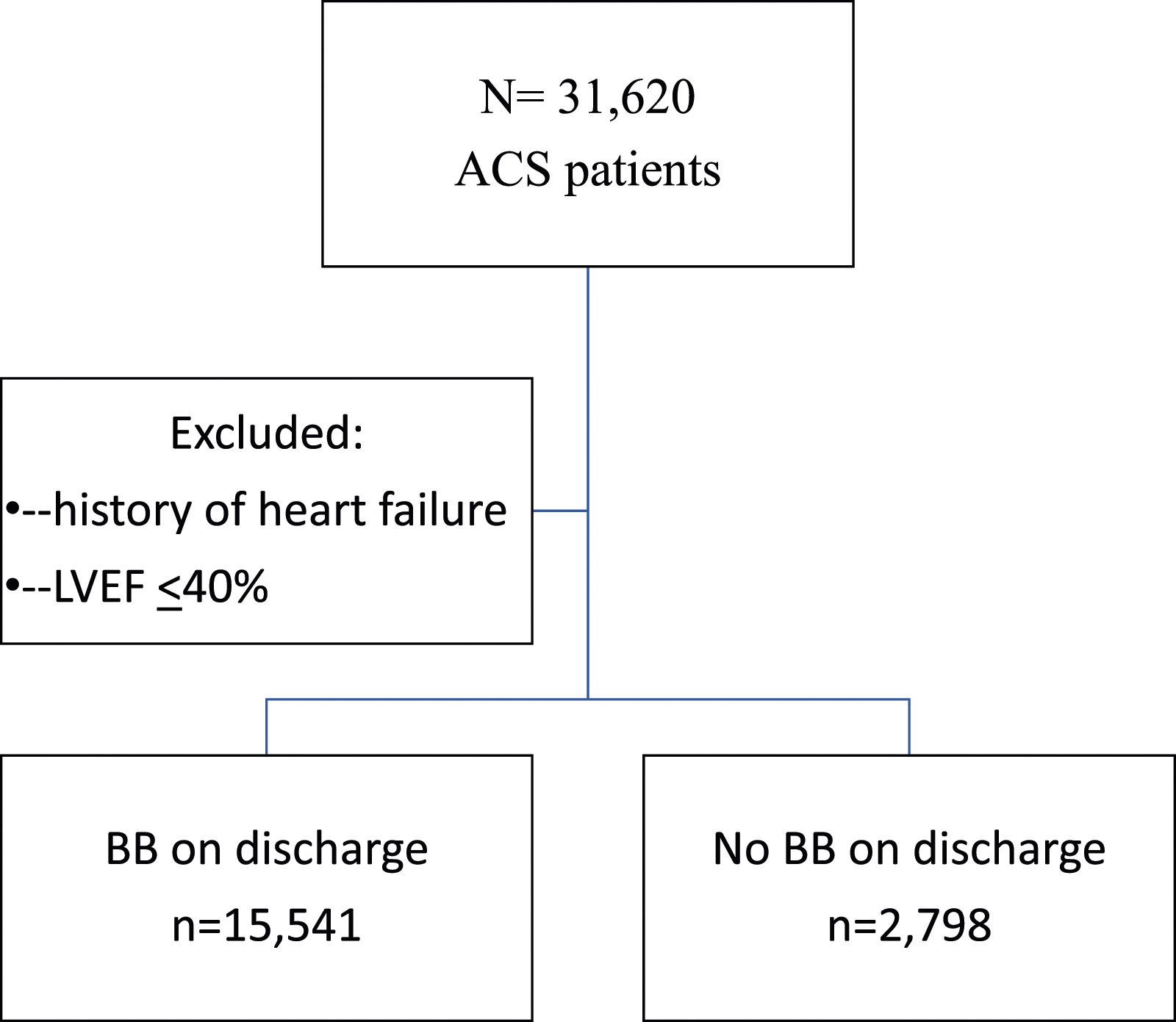
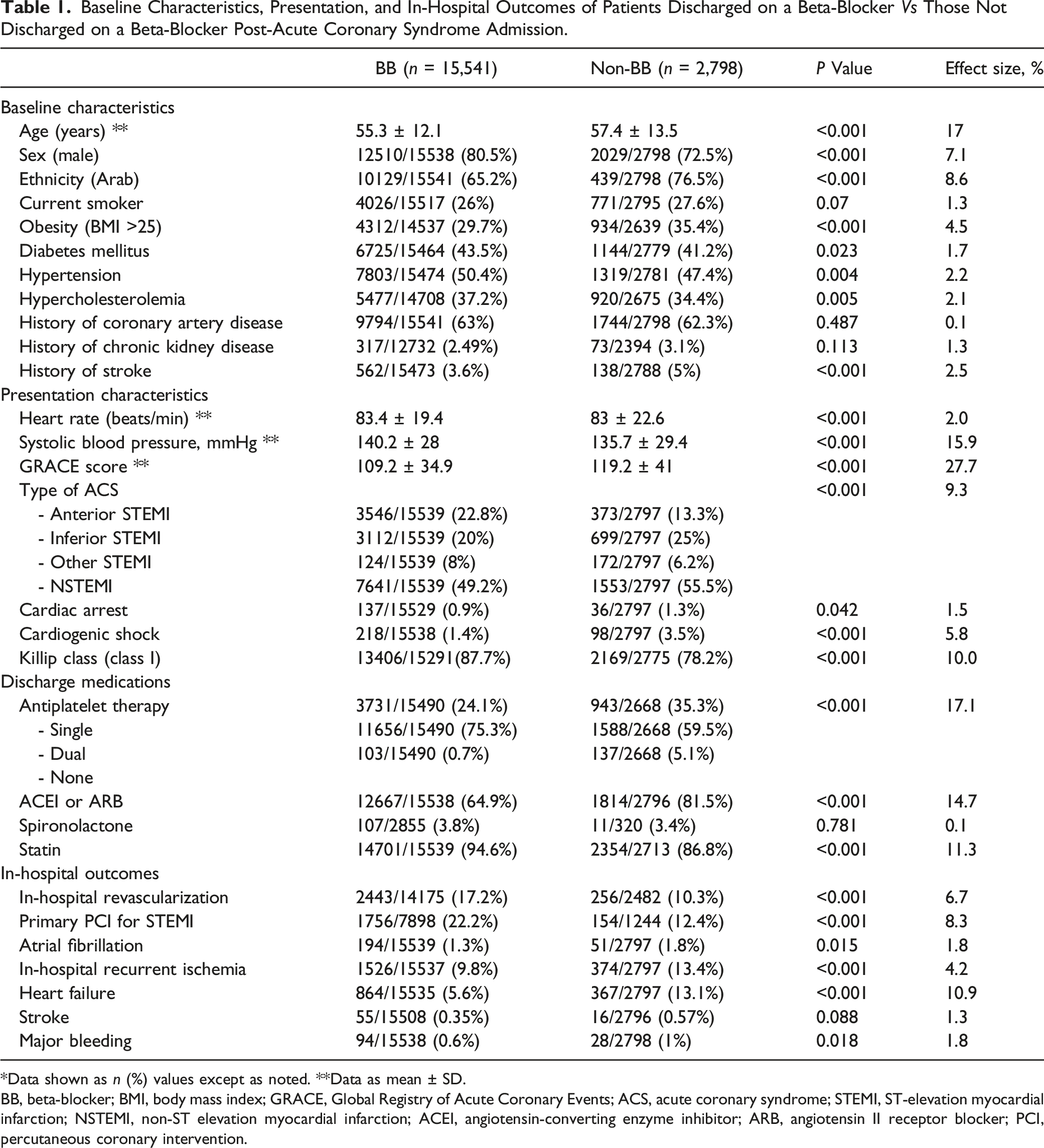
Mean age was 57.4 years in the non-BB group vs 55.3 years in the BB group (P < .001). The BB group had a higher prevalence of diabetes mellitus (43.5 vs 41.2%, P = .023), hypertension (50.4 vs 47.4%, P = .004), and hyperlipidemia (37.2 vs 34.4%, P = .005). The non-BB group had higher prevalence of obesity (35.4 vs 29.7%, P < .001), history of stroke (5 vs 3.6%, P < .001), and more presentation of cardiac arrest (1.3 vs 0.9%, P = .042) and cardiogenic shock (3.5 vs 1.4%, P < .001).
Primary PCI for STEMI was higher in the BB group (22.2 vs 12.4%, P < .001) so as in-hospital revascularization (other than primary PCI) 17.2 vs 10.3% in the BB group vs non-BB group (P < .001). Recurrent ischemia was higher in the non-BB group (13.4 vs 9.8%, P < .001) along with in-hospital heart failure incidence (13.1 vs 5.6%, P < .001). The BB group were more likely to be discharged on DAPT (75.3 vs 59.5%, P < .001), statin (94.6 vs 86.8%, P < .001) and less likely to be discharged on angiotensin-converting enzyme inhibitor (ACEI) or angiotensin II receptor blocker (ARB) (64.9 vs 81.5%, P < .001).
Mortality Difference
Primary and Secondary Outcomes in Beta-Blocker vs Non-Beta-Blocker Groups.
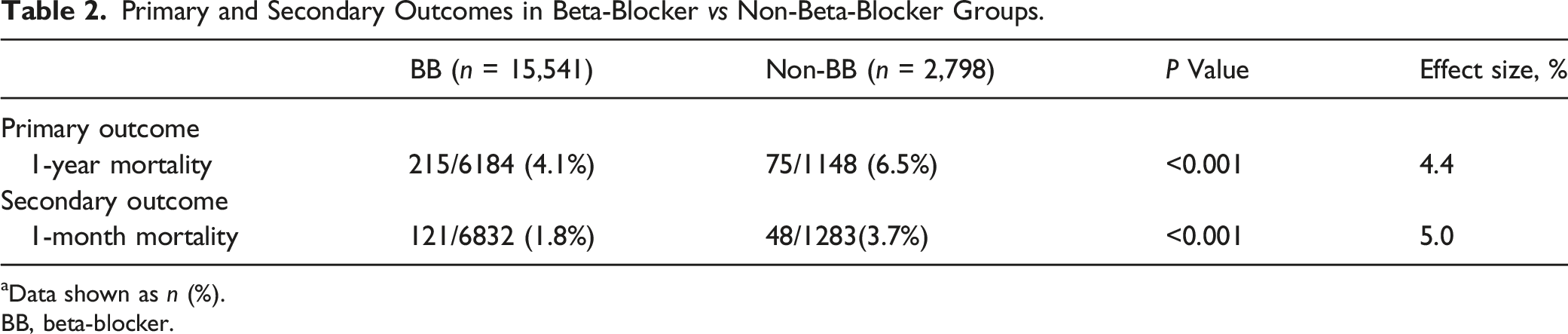
aData shown as n (%).
BB, beta-blocker.
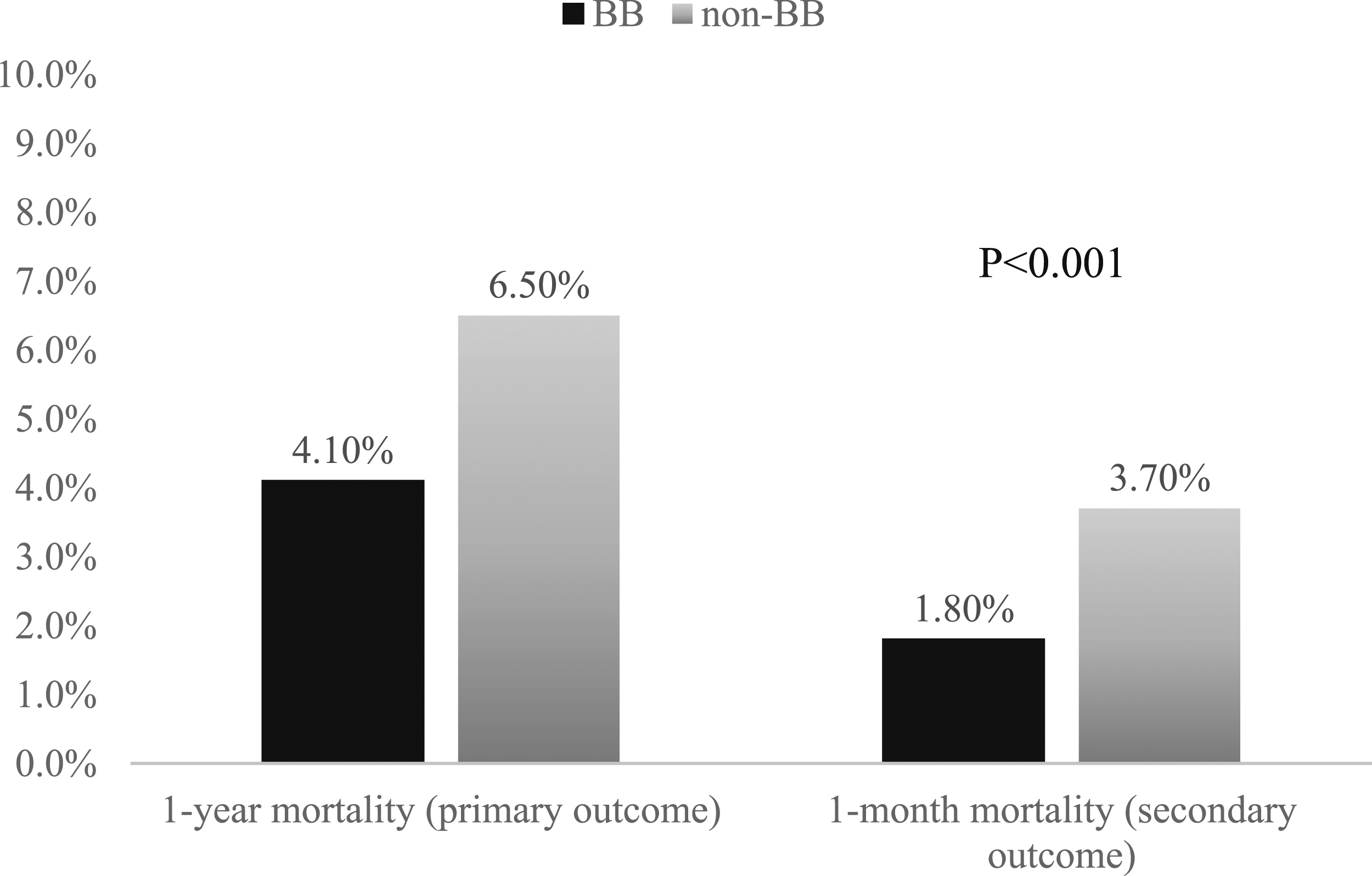
Primary and secondary outcomes in BB vs non-BB.
Sensitivity Analysis
An additional sensitivity analysis was performed using propensity score matching (Figure 3). As shown in Supplementary Table 2, characteristics were well-balanced after matching, including primary PCI and revascularization with small effect size. Even after adjusting for BP, antiplatelet therapy, BB use was associated with a significant reduction in 1-year mortality [adjusted OR: 0.34 (95% CI 0.16–0.73)]. Primary and secondary outcomes after propensity score matching in BB vs non-BB.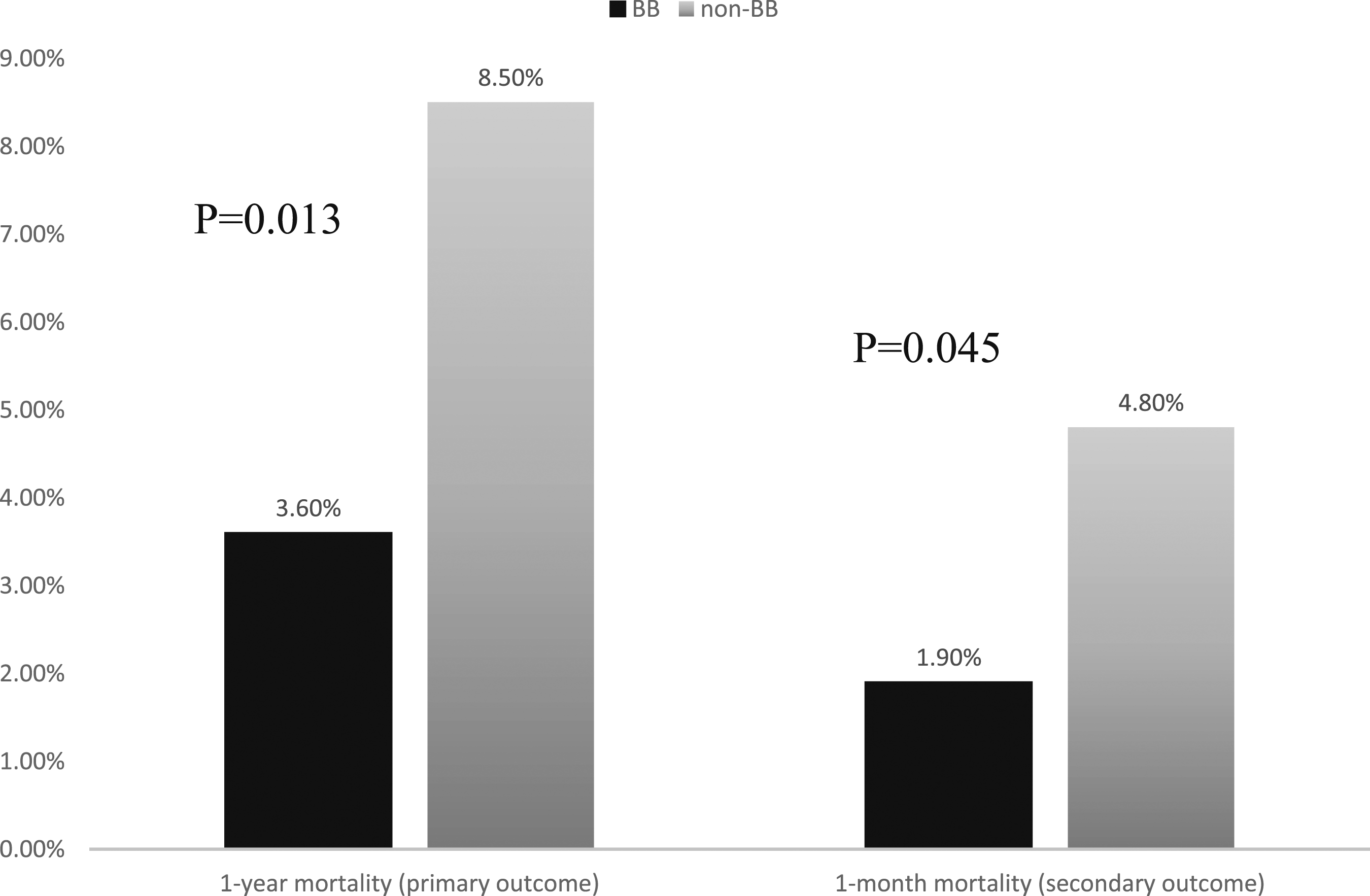
Subgroup Analysis
Subgroup analysis (Figure 4) showed no significant interaction based on age (<50, 51–75, and >75), sex, ethnicity, obesity, DM, presentation (STEMI and NSTEMI), and LVEF (41–50% and >50%). Although the OR of 1-year mortality was pointing towards a protective BB effect for all the subgroups except for the revascularized subgroup, the CI did not support that finding. The OR of 1-year mortality with BB in the revascularized group was 2.3, pointing towards a non-protective BB effect, but had a wide 95% confidence interval (0.3–17.7) and non-significant P value (P = .242). The subgroup analysis results could be because of smaller samples to see the difference. Moreover, there was a mortality benefit with BB use in the propensity score matching regardless of revascularization. Subgroup analysis of BB use and mortality effects.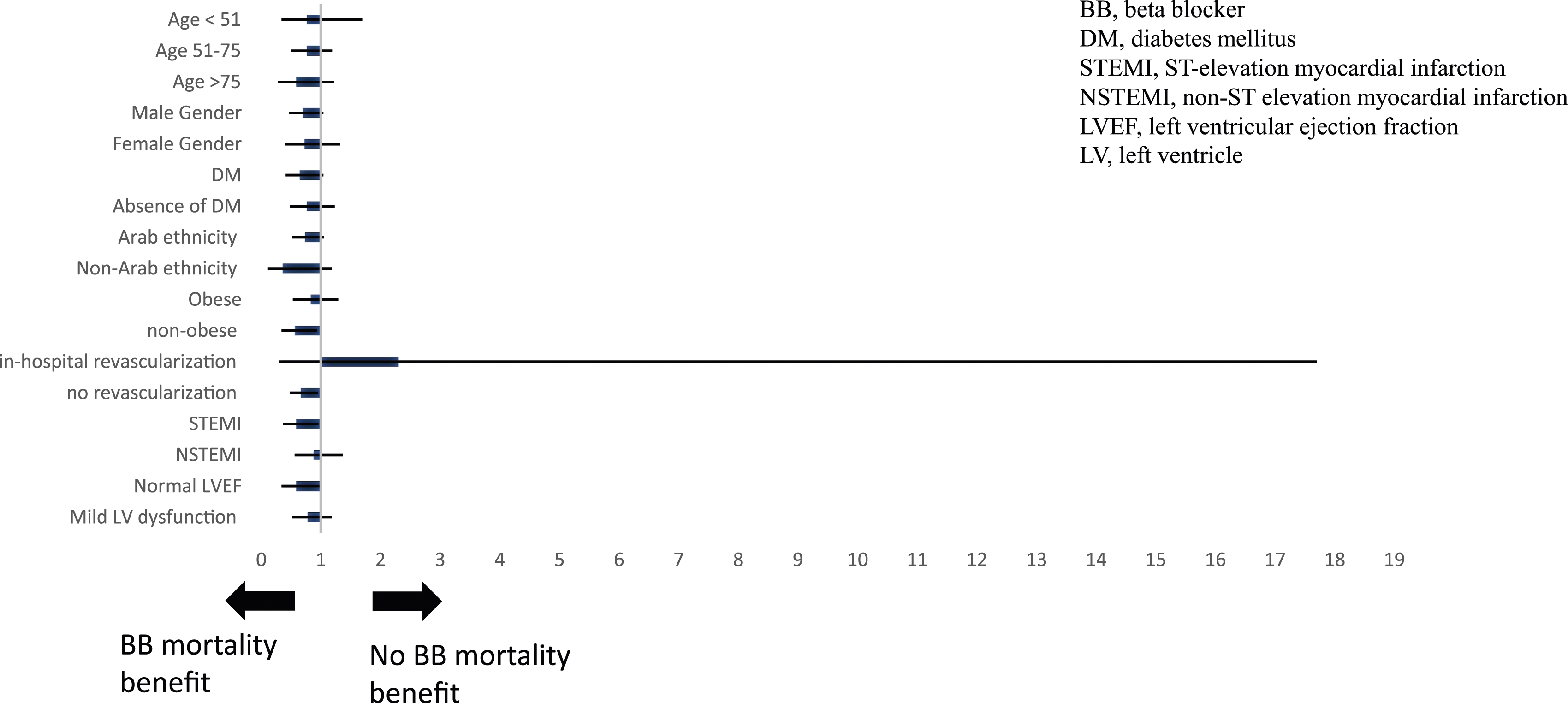
Discussion
Our data from large multi-center prospective registries showed that BB use was associated with a significant 1-year mortality reduction in patients who presented with ACS with mid-range and preserved LVEF, even after extensive adjustment for confounders and propensity score matching. This is one of the largest studies that used a pre-defined LVEF to address the effect of BB post-ACS with mid-range and preserved LVEF.
Previously Published Articles on BB Use in ACS Without Heart Failure.
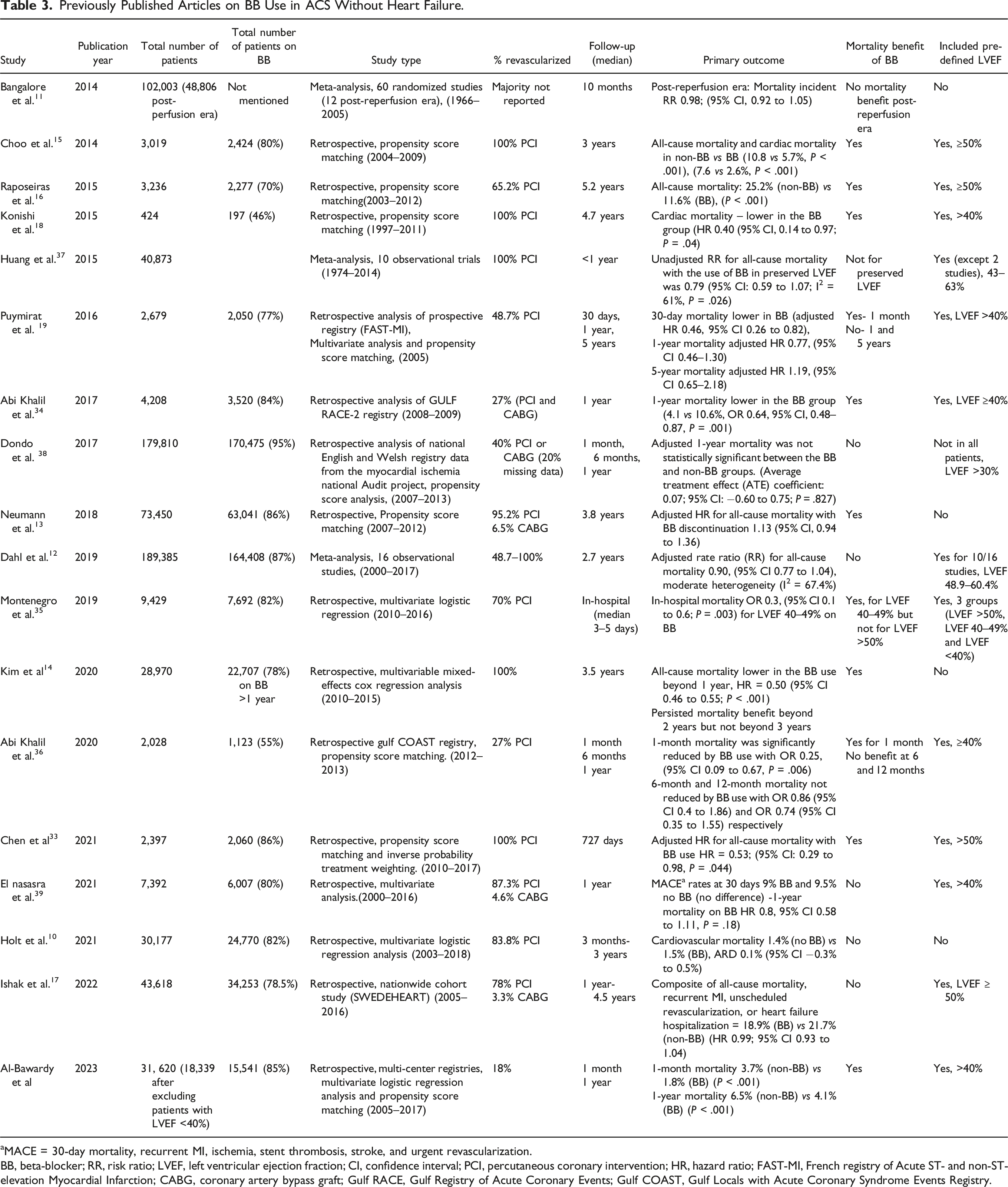
aMACE = 30-day mortality, recurrent MI, ischemia, stent thrombosis, stroke, and urgent revascularization.
BB, beta-blocker; RR, risk ratio; LVEF, left ventricular ejection fraction; CI, confidence interval; PCI, percutaneous coronary intervention; HR, hazard ratio; FAST-MI, French registry of Acute ST- and non-ST-elevation Myocardial Infarction; CABG, coronary artery bypass graft; Gulf RACE, Gulf Registry of Acute Coronary Events; Gulf COAST, Gulf Locals with Acute Coronary Syndrome Events Registry.
Data with Evidence That BB Have a Protective Role
There is data to support the findings of our study. Several small observational studies showed mortality benefit of BB when used post-MI with pre-defined LVEF.15,16,18,33 Larger registries from Korea and France showed potential protective role with the use of BB in patients who present with AMI and undergo revascularization with no HF.
A Korean registry of 3,109 patients with AMI who underwent PCI and had pre-defined LVEF ≥50% found a reduction in all-cause mortality and cardiac mortality beyond 3 years in patients treated with BB compared with those who are not (5.7 vs 10.8%, P < .001, 2.6 vs 7.6%, P < 001). 15 Another observational study of 3,236 patients with pre-defined LVEF ≥50% showed that the use of BB in patients post-MI with normal LVEF is associated with lower long-term mortality with a median follow-up of 5 years (11.6 vs 25.2%; P < .001). 16 A smaller additional study of 424 patients with pre-defined LVEF >40% post-MI found that the use of BB significantly reduced cardiac mortality with a median follow-up of 4.7 years. 18
A French registry found that out of all patients (n = 73,450) who presented with AMI without HF and underwent revascularization, the discontinuation of BB after a year with follow-up up to 3.8 years had higher rates of all-cause mortality or ACS (adjusted HR for mortality of ACS 1.17 (95% CI, 1.01–1.35). However, the difference did not reach statistical significant for all-cause mortality (adjusted HR 1.13 (95% CI, 0.94–1.36). 13 Nonetheless, one of the main limitations of the study was the lack of pre-defined LVEF. Another Korean registry followed 28,970 patients for a year after presenting with AMI resulting in coronary revascularization. Receiving BB beyond a year was also associated with a lower HR (0.81, 95% CI 0.72–0.91) for all-cause mortality, which was persistent beyond 2 years as well but not beyond 3 years. 14 This study also lacked pre-defined LVEF.
Similar to our findings, Abi Khalil and colleagues saw a difference in mortality favoring BB with pre-defined LVEF ≥40% after ACS. 34 However, their sample size is smaller with 4,208 patients.
Is the Benefit Short-Term Only?
Our study showed both 1-month and 1-year mortality benefit with BB use in patients with AMI and LVEF ≥40%. The short-term mortality benefit was also supported by other studies. A Portuguese national registry data enrolling 9,429 ACS patients showed an in-hospital mortality benefit with the use of BB post-ACS with LVEF 40–49% but not for >50%. 35 Nonetheless, the study did not have long-term outcome to see if it is a sustainable benefit. A French registry enrolled 2,679 patients post-MI with pre-defined LVEF >40% and found that BB use reduced 30-day mortality. 19 However, its discontinuation after 1 year did not increase mortality at 1-year and 5 years. 19 This was an older study from 2005 and had fewer patients compared with our study. Our study did not go beyond 1-year follow-up to look for a difference beyond a year.
Another registry from the Gulf region (GULF COAST registry) showed 30-day mortality benefit in patients treated with BB after their ACS presentation with LVEF >40% compared with those who were not. 36 However, that mortality benefit faded away at 1 year and was no longer significant. 36 It is important to mention the study was smaller than ours with 2,028 patients.
In summary, the studies that showed short-term benefit only had fewer patients than ours.
Data With No Protective Role of BB
There is also data supporting a lack of protective role of BB in patients post-MI without heart failure. Several meta-analyses carried out had multiple limitations such as including observational studies and pre-reperfusion old studies with missing pre-defined LVEF.
An old meta-analysis published in 2014 showed no mortality or net benefit of BB in MI patients without heart failure in the reperfusion era compared to pre-reperfusion era. 11 Although there was a decrease in MI and angina in the reperfusion era, it came with the expense of more heat failure and cardiogenic shock as well as higher drug discontinuation. 11 Although the exclusion criteria of this meta-analysis included post-MI heart failure trials, not all included trials studied preserved LVEF patients only. Most importantly, they were mainly old trials, of which only two trials were published after 2005.
A subsequent meta-analysis published the following year in 2015 showed that all-cause and cardiac mortality was lower in the group treated with BB compared with no BB, but the finding was restricted to those with reduced LVEF. 37 Nevertheless, they included observational studies, some prior to the reperfusion era.
Another more recent meta-analysis published in 2019 with all 16 studies published in the 2000s found that there was 26% reduction in all-cause mortality with BB after MI with no heart failure. However, that effect disappeared when controlling for bias. 12 Most studies included did not have pre-defined LVEF and only four had pre-defined LVEF >40% (2 of them with LVEF ≥50%). 12
There are several registries published that also support the lack of BB protective effect. However, some limitations include the lack of pre-defined LVEF. One example is a large registry data from the UK with >170,000 patients admitted with AMI between 2007 and 2013 that showed an overall higher mortality at 1 year, 5.2%, which is similar to our cohort. 38 Although the unadjusted 1-year mortality was lower in the BB group compared with those not on a BB (4.9 vs 11.2%; P < .001), the adjusted mortality was similar in the two groups. 38 One of their limitations is that the definition of heart failure for their study was based on the hospital records, which did not always include a pre-defined LVEF and included clinical heart failure definition. 38 Another example of the lack of pre-defined LVEF is a Danish registry published in 2021 that showed that the use of BB medications beyond 3 months post-MI in patients without HF did not affect cardiovascular mortality, recurrent MI, or composite of the two outcomes after 3 years compared with patients who are not on BB after 3 months of their MI and up to 3 years. 10 However, their outcomes which included cardiovascular mortality at 3 years were very low in both groups <2% compared with our mortality rates. 10
Two registries found no protective role of BB with pre-defined LVEF. The first is a smaller registry (n = 7,392) from Israel that showed also no 30-day or 1-year mortality benefit with BB use in patients with AMI and LVEF 40–49% or >50%. However, the study cohort included patients as early as 2000 and one main difference with our study is the very low rates of 30-day mortality (0.6%) and 1-year mortality (2.7%) to possibly detect a difference. 39
The second and largest registry (n = 43,618) that showed no protective role of BB with pre-defined LVEF comes from SWEDEHEART. They found no benefit in the use of BB in patients post-MI with normal LVEF starting 1 year and up to median of 4.5 years on composite outcomes that included all-cause mortality, recurrent MI, unscheduled revascularization, and heart failure hospitalization. 17 However, their study addressed the effect of BB use beyond 1 year of MI and excluded mid-range LVEF but had higher rates of revascularization compared with our study.
In summary, most of the studies that showed no benefit of BB on mortality in patients without heart failure were either beyond a year with normal LVEF, limited by small numbers of events or lacked a pre-defined LVEF. In comparison, we have included large number of patients with pre-defined LVEF in the mid-range or preserved. Our mortality rates were higher than some of previous studies which could potentially explain the difference in outcomes.10,39 However, we had low numbers of revascularization compared with previously mentioned trials (40–92 vs 18%), which may have contributed to our finding of protective BB role with possible residual CAD.10,17,38,39 Nonetheless, as described above, even with 100% revascularization rates, some studies have shown the benefit of BB on mortality.15,18,33 It remains unclear if revascularization lessens the effects of BB on mortality in those with mid-range and preserved LVEF.
Although this study is a large study that includes multiple registries, it carries the expected limitations of registries. The 30-day and 1-year mortality were not available for all the registries. We do not have data on adherence to medications that could affect the interpretation of the reported outcomes. Another limitation of our study is the missing data on residual CAD after PCI and whether BB play a protective role in that patient population. Although with matched cohort and similar comorbidities, the extent of CAD is likely similar in the two groups. We also have low percentage of revascularization that could have affected the generalizability of our results due to recruitment of non-PCI hospitals in the registries. The revascularization rates could be higher than reported, as they will not be captured if patients were transferred to PCI centers. However, even with propensity score matching regardless of revascularization, there was a mortality benefit of BB in mid-range and normal LVEF post-MI up to a year post-MI. We do not have data beyond 1 year and it is unclear if the benefit fades away after a year.
In conclusion, our study shows 1-month and 1-year mortality benefit of BB use in the Gulf population patients after ACS with mid-range and preserved LVEF. The mortality benefit remained statistically significant even after propensity score matching with adjustment for residual confounders. Randomized controlled trials will be needed to address this question and produce definitive answers.
Supplemental Material
Supplemental Material - The Effect of Beta-Blocker Post-Myocardial Infarction With Ejection Fraction >40% Pooled Analysis From Seven Arabian Gulf Acute Coronary Syndrome Registries
Supplemental Material for The Effect of Beta-Blocker Post-Myocardial Infarction With Ejection Fraction >40% Pooled Analysis From Seven Arabian Gulf Acute Coronary Syndrome Registries by Rasha Al-Bawardy, MD, MSc, Wael Alqarawi, MD, MSc, Jassim Al Suwaidi, MBChB, Wael Almahmeed, MD, Mohammad Zubaid, MBChB, Haitham Amin, MD, Kadhim Sulaiman, MD, Ahmad Al-Motarreb, MD, and Khalid Alhabib, MBBS in Angiology.
Footnotes
Acknowledgments
The authors acknowledge the Gulf Heart Association, the Saudi Heart Association, the College of Medicine Research Center at King Khalid University Hospital, and the King Saud University, Riyadh, Saudi Arabia for their support with the initial registries.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.