
Abstract
The present study aimed to investigate the balance between angiotensin II (Ang-II) and kallikrein (KLK1) in the pathogenesis of ST-segment elevation acute myocardial infarction (STEMI). The study included a total of 261 participants: 151 STEMI patients and 110 individuals with normal coronary arteries. The plasma levels of Ang-II and KLK1 were measured using enzyme-linked immunosorbent assays (ELISA). Multivariate logistic regression analysis indicated that the plasma levels of Ang-II, KLK1 and the ratio of Ang-II and KLK1 (Ang-II/KLK1) independently correlated with the presence of STEMI. Furthermore, we found independent associations between STEMI and smoking, cholesterol (CHO), high-density lipoprotein cholesterol (HDL-c), as well as age. The ratio of Ang-II/KLK1 correlated with the plasma level of the inflammatory cytokine, interleukin-6 (IL-6). Both Ang-II and KLK1 levels are significantly elevated in patients with STEMI. An increased Ang-II/KLK1 ratio may result in the over-activation of Ang-II and exacerbate the progression of STEMI(P = .046). In conclusion, we have demonstrated, for the first time, an Ang-II and KLK1 imbalance in patients with STEMI.
Keywords
Introduction
Inflammation is a component of the atherosclerotic (AS) process. Recent studies have demonstrated that the inflammatory scores are predictors of short- and long-term mortality in patients with cardiogenic shock or ST-segment elevation acute myocardial infarction (STEMI).1–3 Evidence suggests that the renin angiotensin system (RAS) plays a crucial role in the pathophysiology of coronary artery disease (CAD).1,2 Data suggests that angiotensin-converting enzyme 2 (ACE2) and kallikrein 1 (KLK1) have recently emerged as protective components of the RAS and the kallikrein-kinin system (KKS), respectively, against AS. 3 Furthermore, ACE2 and KLK1 enzymes play a crucial role in mitigating the development of AS plaques by reducing vascular inflammation, promoting vasodilation, and exhibiting anti-inflammatory properties. 4 A study reported increased plasma KLK1 levels in a Chinese population with CAD. 5 However, KLK1 is known to be a cardio-protective agent, which exhibits a major cardio-protective role by reducing infarct size, improving cardiac function and attenuating myocardial remodeling.6,7
Moreover, some studies showed that the serum C-reactive protein (CRP)/albumin ratio (CAR) value in predicting mortality among heart failure with reduced ejection fraction (HFrEF) patients or coronavirus disease 2019 (COVID-19) pneumonia patients.8,9 Lutfu Askin et al 10 reported that as an ischemia-dependent risk index, CAR is an independent marker of in-hospital and long-term all-cause mortality in STEMI. The results indicate that CAR is a more effective prognostic marker than either CRP or albumin. The previous studies illustrate that Ang-II stimulates CRP and Matrix metalloproteinase-9 (MMP-9) expression in vascular smooth muscle cell (VSMC). 11 However, KLK1 has been reported to have inhibitory effects on oxidative stress, inflammation, and apoptosis. 12 The relationship between the two and albumin has been rarely reported. Although CAR is a good indicator of CAD, it is mainly an inflammatory marker that is considered to have prognostic value in many diseases, whose predictive value has been utilized in relation to various cancers, sepsis, 2 diabetes and acute pancreatitis, and chronic obstructive pulmonary disease (COPD).13–16 The predictive value of CAR is limited due to it being influenced by several diseases. Therefore, it would be more useful to identify a more effective prognostic marker than CAR for predicting STEMI occurrence.
We hypothesized that interactions among the inflammation, Ang-II/KLK1 ratio may contribute to the development of STEMI. KLK1 plays a crucial role in the process of post-ischemic revascularization. 17 A previous study has indicated that both kallikreins mRNA and activity were significantly elevated in areas of human carotid atheroma. 18 In contrast, another study showed that CAD patients had low levels of urinary KLK1 activity. 19 The relationship of KLK1 and cardiovascular disease (CVD) is not clear and remains controversial. In addition, there have been no clinical studies to confirm a link between plasma Ang-II or Ang-II/KLK1 and STEMI in humans.
The present study aimed to determine whether Ang-II and the balance of Ang-II and KLK1 are associated with the presence of STEMI defined by coronary angiography (CAG).
Materials and Methods
Participants
The study was approved by the Ethics Committee of the Central Hospital of Zibo (approval no. ZBH05485). Each patient gave written informed consent. The study enrolled a total of 261 participants who were admitted to an education and research hospital with suspected STEMI. A total of 10 patients were excluded from our study because percutaneous coronary intervention (PCI) was not carried out.
Each enrolled patient (n = 151) underwent a successful primary PCI procedure. All patients who were included in the study met the specific criteria. These criteria consisted of an electrocardiography (ECG) test that revealed STEMI. Additionally, these patients had to show a rise in troponin I levels, with at least one value exceeding the upper reference limit set at the 99th percentile. Furthermore, it was required that patients experienced continuous chest pain lasting >30 min. Moreover, they needed to exhibit ST-segment elevation >2 mm in two contiguous ECG leads within 24 h from the onset of symptoms.
The control group comprised of 110 individuals who were suspected to have CAD and were scheduled for diagnostic coronary angiography (CAG). Patients in this group exhibited unremarkable coronary arteries without any evidence of atherosclerotic lesions. Patients with suspected CAD received conventional antiplatelet and statin therapy to stabilize the plaque prior to CAG.
The patients who had multiple blood pressure readings exceeding 140/90 mmHg or those taking antihypertensive medication were classified as hypertensive. Patients with fasting plasma glucose levels >126 mg/dL on several measurements or taking antidiabetic medications were considered to have diabetes. The definition of smoking was a daily habit that persists for more than 1 year. Drinking was defined as the daily consumption of at least 50 g of liquor for >1 year. The exclusion criteria for the STEMI patients and control group included individuals with severe hepatic disease, severe renal failure (serum creatinine >180 µmol/l), peripheral angiopathy, serious infections, cancer, and a family history of cardiovascular disease (CVD). The family history of patients with CVD was considered positive if at least one immediate family member experienced premature death before the age of 65 years for women or 55 years for men, or if there was a confirmed history of CAD. Patients treated with angiotensin converting enzyme inhibitors (ACEIs) or angiotensin receptor blockers (ARBs) were also excluded because ACEIs may affect the levels of Ang-II. 20 Finally, a total of 261 patients were enrolled in the study.
Data Collection
Quality control was implemented throughout the entire process of collecting data, ensuring its accuracy and reliability. The comprehensive clinical and demographic data were meticulously extracted from the medical charts, encompassing a wide range of crucial parameters such as age, gender, height, body weight, heart rate, and blood pressure.
Biochemical Tests
Fasting blood samples were collected from the peripheral veins after a minimum 12-h overnight fast, and routine tests for blood, lipid profiles, and coagulation were routinely analyzed in hospital laboratories. Blood samples were carefully collected from participants using plain tubes, which accurately measure the levels of both Ang-II and KLK1 in their plasma. Following centrifugation for 10 min, the plasma was isolated from the blood and subsequently stored at −80°C until analysis. We utilized high-quality commercial ELISA kits Lengton Bioscience Co. Ltd. (Shanghai, China) to accurately quantify the levels of Ang-II and KLK1 in plasma. Plasma and tissue kallikreins are both potent kininogenases and serine proteases. A single gene encodes for plasma kallikreins, and there is a large family of glandular kallikreins genes; however, KLK1 is the only kallikrein known to generate kinins. 21 As the close relationship between kinin and CVD, KLK1 was measured and analyzed in this study. Furthermore, we used the state-of-the-art facilities of a hospital laboratory to accurately assess and quantify the concentration of plasma C-reactive protein (CRP) and IL-6.
Coronary Angiography (CAG)
The participants underwent CAG via either their right femoral or radial arteries. Subsequently, the skilled examiner proceeded to assess the stenosis of the coronary arteries. They carefully scrutinized each artery, including the left main trunk, left anterior descending artery, left circumflex artery, and right coronary artery. Two experienced specialists independently came to a unanimous conclusion regarding the outcome of the coronary angiography. The CAG results showed that the patients suffered from acute occlusion of at least one major coronary vessel or its major branches.
Statistical Analysis
The researchers conducted statistical analysis with the help of SPSS version 19.0 (SPSS Co., Chicago, IL, USA) on a Windows platform. A two-tailed P-value of less than 0.05 was considered statistically significant. In the analysis of variance (ANOVA), we obtained an F statistic with a value of 17.191 and a corresponding P-value less than 0.001, which indicates a highly significant difference in Ang-II/KLK1 level ratios among groups compared to within-group differences. This finding enhances the regression variation and reduces the residual variation, thereby successfully establishing the model. The goodness of fit test passed the Durbin–Watson test with a value of 1.245. Continuous variables with a normal distribution were expressed as the mean value ±standard deviation (SD), while categorical variables were presented as percentages. Student'st test was used to compare continuous variables that followed a normal distribution, while the chi-squared test was used to compare categorical data. The binary and multinomial logistic regression were conducted to adjust the variables that exhibited significant differences in the univariate analysis (P < .05). Odds Ratios (ORs) with 95% confidence intervals (CI) were used to estimate the strength of the association between various risk factors and the occurrence of STEMI. Correlation between plasma Ang-II/KLK1 and IL-6 levels. Ang-II: angiotensin II; KLK1: kallikrein; IL-6: interleukin-6.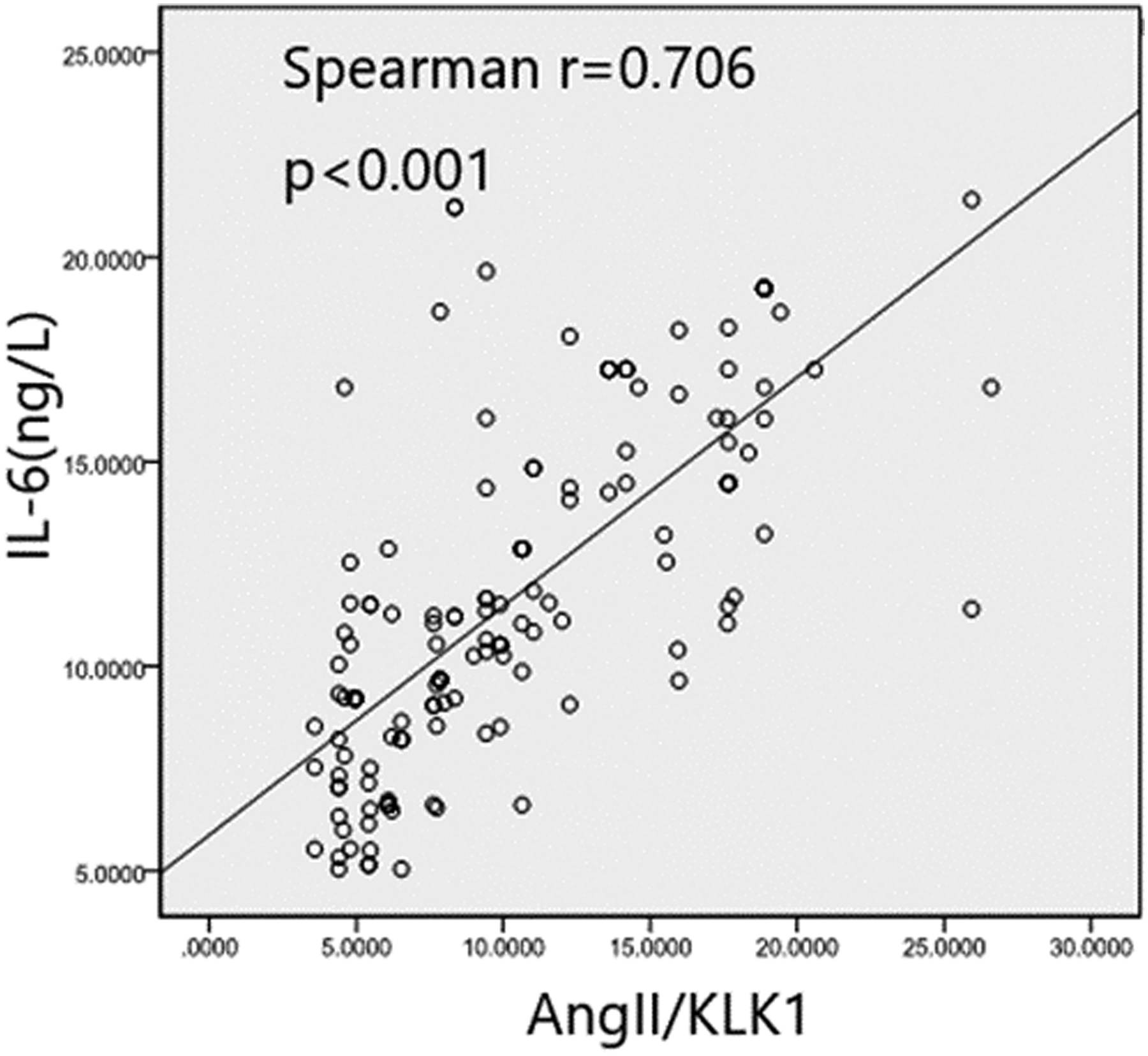
Results
General Clinical and Biochemical Characteristics
Clinical Characteristics of Patients With STEMI.
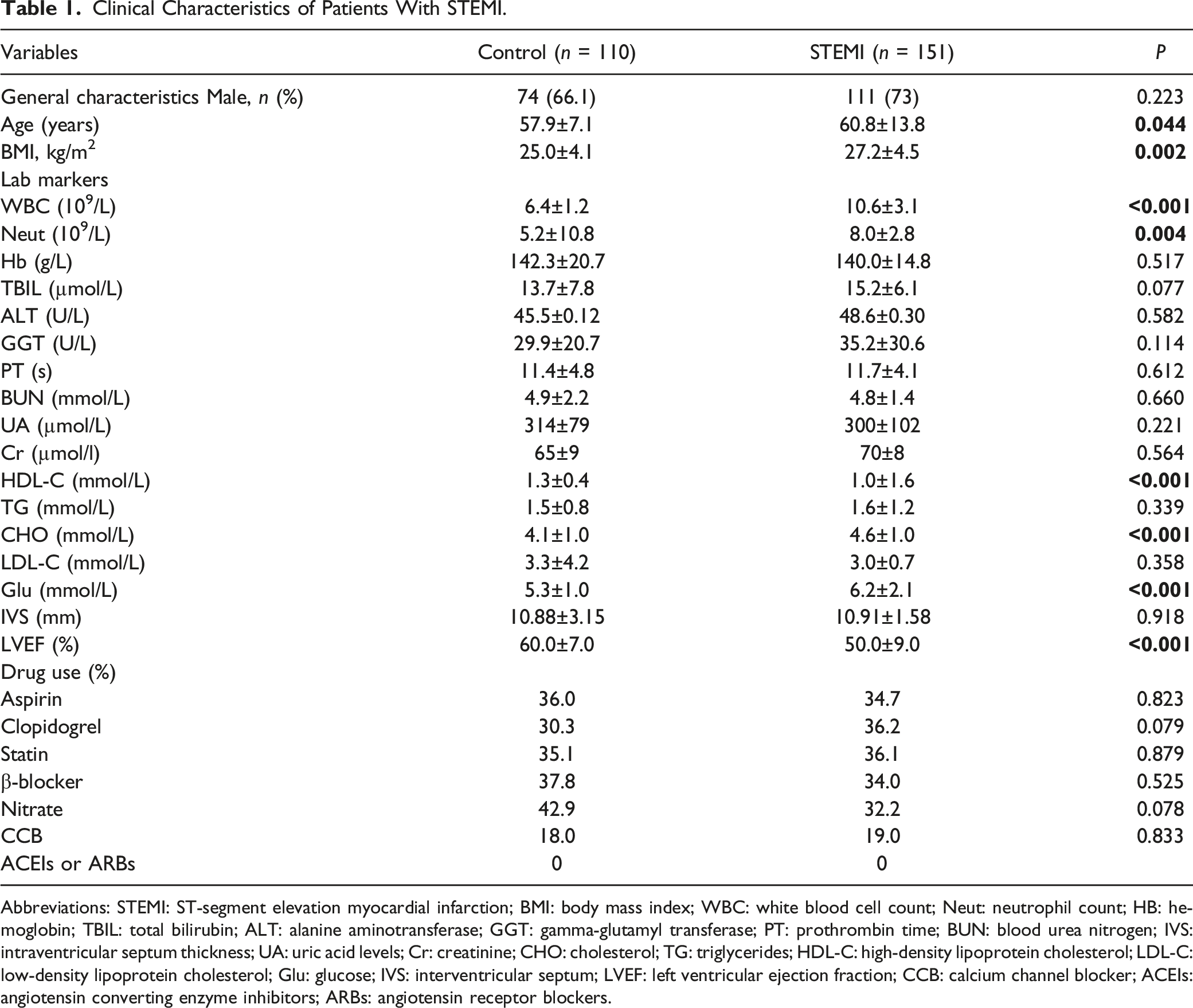
Abbreviations: STEMI: ST-segment elevation myocardial infarction; BMI: body mass index; WBC: white blood cell count; Neut: neutrophil count; HB: hemoglobin; TBIL: total bilirubin; ALT: alanine aminotransferase; GGT: gamma-glutamyl transferase; PT: prothrombin time; BUN: blood urea nitrogen; IVS:intraventricular septum thickness; UA: uric acid levels; Cr: creatinine; CHO: cholesterol; TG: triglycerides; HDL-C: high-density lipoprotein cholesterol; LDL-C: low-density lipoprotein cholesterol; Glu: glucose; IVS: interventricular septum; LVEF: left ventricular ejection fraction; CCB: calcium channel blocker; ACEIs: angiotensin converting enzyme inhibitors; ARBs: angiotensin receptor blockers.
Previous History, Plasma Ang-II, KLK1, Ratio of Ang-II/KLK1 and IL-6 Levels of the Study Population.
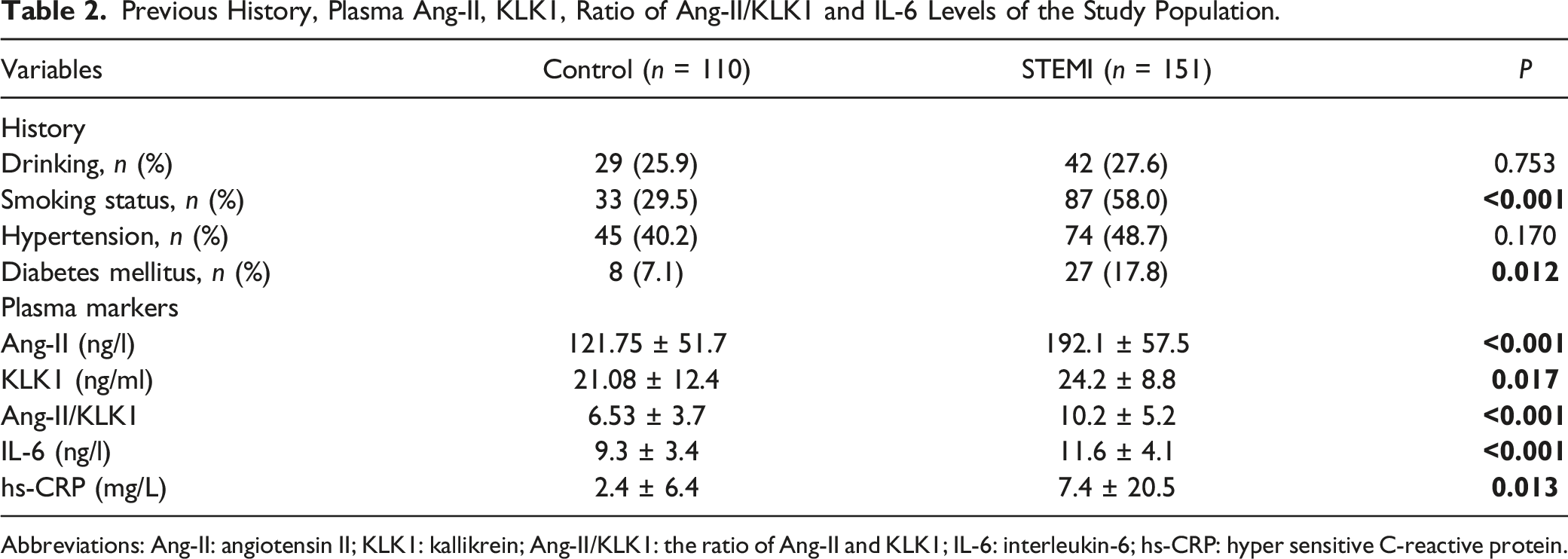
Abbreviations: Ang-II: angiotensin II; KLK1: kallikrein; Ang-II/KLK1: the ratio of Ang-II and KLK1; IL-6: interleukin-6; hs-CRP: hyper sensitive C-reactive protein.
The findings of our study had revealed some significant differences between the STEMI group and the control group. First, we observed that age, BMI, total white blood cell (WBC), Neut, cholesterol (CHO), glucose (Glu), left ventricular ejection fraction (LVEF), smoking status, the levels of highly sensitive C-reactive protein (hs-CRP) and interleukin-6 (IL-6), and levels of both Ang-II and KLK1 were all significantly higher in the STEMI group compared with the control group. Furthermore, we also found that there was a significant increase in the ratio of Ang-II/KLK1 in patients with STEMI compared with those without (Tables 1 and 2). The prevalence of diabetes was significantly higher in the STEMI group compared with the normal group, as shown in Table 2. The control group had a significantly higher HDL-C than those of the STEMI (Tables 1 and 2). A higher level of HDL-C is likely to decrease the risk of cardiovascular events. 22
Multivariate Logistic Regression Analysis Showing the Independent Predictors for the Presence of STEMI.
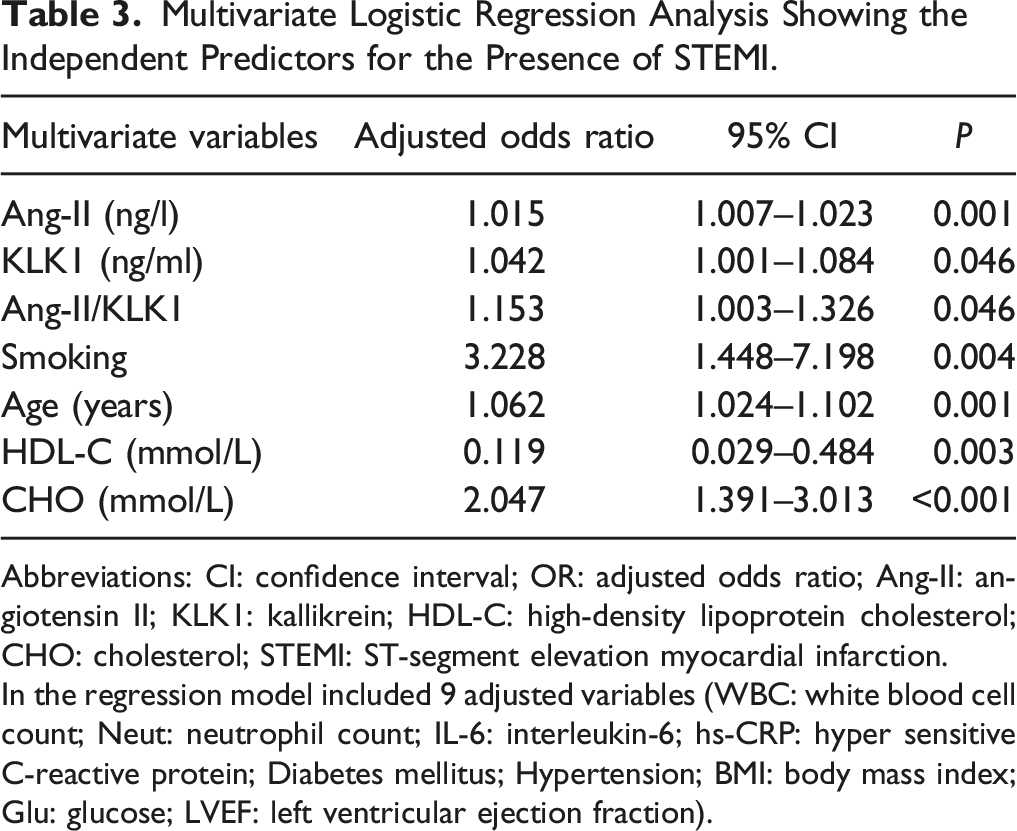
Abbreviations: CI: confidence interval; OR: adjusted odds ratio; Ang-II: angiotensin II; KLK1: kallikrein; HDL-C: high-density lipoprotein cholesterol; CHO: cholesterol; STEMI: ST-segment elevation myocardial infarction.
In the regression model included 9 adjusted variables (WBC: white blood cell count; Neut: neutrophil count; IL-6: interleukin-6; hs-CRP: hyper sensitive C-reactive protein; Diabetes mellitus; Hypertension; BMI: body mass index; Glu: glucose; LVEF: left ventricular ejection fraction).
Correlation Between Ang-II/KLK1 andIL-6
The levels of plasma IL-6 were significantly higher in the STEMI group compared with the normal group (Table 2). Correlation analysis showed a positive association between Ang-II/KLK1 and IL-6 level (r = 0.706, P < .001) (Figure 1).
Discussion
The RAS, especially Ang-II overexpression, plays an important role in AS progression. 23 KKS is considered the dominant mechanism for counteracting the detrimental effects of the hyperactive RAS. 24 KLK1 has been proved as a protective factor against AS because of its vasodilatory, antiproliferation, and anti-inflammatory effects. 25 Urinary KLK1 levels have been inversely linked to blood pressure in patients with essential hypertension, according to epidemiological studies. 26 A multicenter case-control study in China also revealed a negative correlation between plasma KLK1 levels and both first-ever stroke incidence and stroke recurrence. 27 A study indicated that unstable coronary plaques demonstrated markedly increased KLK1 levels, macrophage infiltration and high microvessel density. 28 Nevertheless, another study showed that CAD patients had low levels of urinary KLK1 activity, suggesting that renal KKS activity may be reduced in patients with this disease. 19 The literature on the relationship between KLK1 levels and CAD is limited and controversial, especially STEMI patients. The study demonstrated, that in patients with STEMI, while both Ang-II and KLK1 were elevated, the elevation of Ang-II was more pronounced, resulting in the significant surge of the ratio of Ang-II/KLK1 compared with those in patients with normal groups. Therefore, it is speculated that both Ang-II and KLK1 are activated in patients with STEMI, the over-activation of Ang-II and disruption of the balance between Ang-II and KLK1, lead to increased vascular proliferation and inflammation, ultimately accelerating rapture of coronary plaque. In the present study, we have demonstrated for the first time that the role of balance between Ang-II and KLK1 in human STEMI.
Tissue KLK1 is an essential enzyme belonging to the serine proteinase family. KLK1 is the sole enzyme capable of generating kinin, which performs its primary function by processing low-molecular weight kininogen substrates to release vasoactive peptides known as bradykinin (BK) and Lys-BK (kallidin), playing crucial roles in various physiological processes within the human body. 24 Our study revealed that STEMI patients exhibited higher levels of plasma KLK1 compared to the control group. Logistic regression analysis showed that this association was independent of other factors associated with risk for arterial disease. However, KLK1 is recognized as a cardio-protective agent, exhibiting a broad range of beneficial effects such as reducing the size of infarction, enhancing cardiac function, improving micro circulation, and mitigating myocardial remodeling. 29 It is paradoxical that in our study, plasma KLK1 levels were found to be independently and positively associated with the presence of human STEMI, despite clinical and experimental studies indicating KLK1 and its products kinins were involved in cardio-protection in ischemia.30,31 All the above results demonstrated exogenous KLK1 had protective effects on the heart and kidney disease in animal models. 24
The possible explanation for the association between elevated plasma KLK1 levels and increased incidence of STEMI is as follows. Based on the literature and previous research, it is hypothesized that up regulation of KLK1 as a compensatory mechanism for dysfunctional state in STEMI patients may account for this phenomenon. Patients with heart failure often experience elevated levels of atrial natriuretic peptide (ANP) in their plasma. ANP is a hormone that is helping to regulate blood pressure and fluid balance in the body. In addition to its role in regulating fluid balance, ANP may also play a role in slowing the progression of heart failure. 32 It is similar with another study that KLK1 levels were higher in subjects with type 2 diabetes. 33 Pancreatic KLK1 can protect against diabetic retinopathy by activating β1 and β2 receptors and inhibiting oxidative stress, inflammation, and apoptosis. Thus, pancreatic KLK1 may represent a new therapeutic agent for diabetic retinopathy. 12 We hypothesize that the increase in plasma KLK1 levels serves as a protective response against STEMI, and therefore, elevated plasma KLK1 may serve as a biomarker for dysfunctional states rather than being a risk factor for STEMI. However, further research is needed to fully elucidate the underlying mechanism.
The discovery of KKS in 1909 revealed that urine, rich in kinins, not only reduces blood pressure but also has modulatory effects on angiogenesis and can ameliorate heart and kidney dysfunction.24,31 Moreover, KLK1 has the ability to promote angiogenesis, a crucial process for tissue repair and regeneration. 34 However, recent studies have revealed that patients with restenosis exhibit an increase in the concentrations of kininogens, as well as plasma and tissue KLK1, indicating activation of this inflammatory pathway. 35 KLK1 and kinins have been reported to have pleiotropic effects on inflammation, fibrosis, and apoptosis in different experimental animal models and to have a protective effect against diabetic nephropathy (DN). 12 Tissue KLK1 increases nitric oxide levels and Akt activation, and attenuates Ang-II-induced inflammation by reducing transforming growth factor-β, TGF-β(TGF-β1) expression, and reactive oxygen species formation. 36 A recent study found that KLK1 activity was inhibited while the RAS upregulated in the kidney of kallistatin transgenic kallistatin transgenic (KS-tg)/a transgenic model of type 1 diabetes (OVE) mice compared to wild-type (WT)/OVE mice, suggesting a disturbed balance between the RAS and KKS. 37 Thus, it has been found that as a KLK1-binding protein, kallistatin inhibits KLK1 activity and reduces kinin generation, which could explain its deleterious effect on DN. These results demonstrated high levels of kallistatin exacerbate DN at least partly by inducing RAS over activation and hypoxia. 37 Studies have shown that KLK1 can reduce inflammation, oxidative stress, and fibrosis in various organs affected by Ang-II, such as the heart, kidneys, and lungs.31,38 The aforementioned findings can be partially elucidated by our inference that the excessive activation of Ang-II and disruption of the equilibrium between Ang-II and KLK1 contribute to augmented vascular proliferation and inflammation, ultimately expediting coronary plaque rupture. Further nonclinical studies are necessary to determine the mechanism.
In this study, correlation analysis showed a positive association between the ratio of Ang-II/KLK1 level and IL-6. Inflammation is believed to play a crucial role in the pathogenesis of AS. IL-6 concentrations have been previously demonstrated to be strong and independent predictors of cardiovascular mortality. 39 Pancreatic KLK1 has been reported to have inhibitory effects on oxidative stress, inflammation, and apoptosis. 12 The findings of this study support the recent observation that Ang II stimulation significantly increases the expression levels of angiotensinIItype1receptor (AT1R), IL-6, cyclooxygenase-2 (COX-2), and Glial fibrillary acidic protein (GFAP) in astrocytes. 40 It is noteworthy that the levels of KLK1 exhibited an inverse association with elevated IL-6 in STEMI patients, which contradicts the findings of a previous studies, which is recombinant KLK1 stimulated the production of inflammatory cytokines in proximal tubular epithelial cells via the activation of p42/44 and p38 Mitogen-activated protein kinases signaling pathways. 41 We hypothesized that the varying balance between Ang-II and KLK1 in early versus late stages of atherosclerotic lesions may account for the differential impact of endogenous KLK1 on STEMI. In early stages, up-regulation of KLK1 likely serves as an adaptive mechanism to counteract hypoxia and promote angiogenesis/vascular protection. In turn, revascularization suppressed KLK1 levels in the ACS subgroup. 28 When increased KLK1 levels are insufficient to counteract hypoxia, the inflammatory response triggered by Ang-II tends to prevail, resulting in STEMI induction. The findings of the current study are also in accord with previous observations that Ang-II increases the expression of IL-6, while KLK1 counteracts the effect of Ang-II on IL-6, leading to decreased inflammatory levels that can in turn reverse the promoting effects of Ang-II on inflammation and athermanous plaque formation and progression.1,12,24 In conclusion, these findings establish the linkage between Ang-II/KLK1 and IL-6 expression, and the inflammation in human STEMI.
The following study limitations should be taken into account. First, the study is a cross-sectional one, which limits our ability to draw causal conclusions. Another limitation is the absence of patients with obstructive CAD who did not experience STEMI. In summary, the present study is the first to identify an imbalance between Ang-II and KLK1 in patients with STEMI. And the ratio of Ang-II/KLK1 correlated with the plasma level of the inflammatory cytokine, interleukin-6 (IL-6). Developing clinical strategies to increase plasma KLK1 levels and maintain the balance between Ang-II and KLK1 could provide a novel therapeutic approach for preventing and treating STEMI. Further prospective studies are needed.
Footnotes
Author Contributions
Each author has made significant contributions to the conception and design, the process of obtaining, analyzing, and interpreting data; drafting or critically revising the article for important intellectual content; and granting final approval for the version to be published.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Natural Science Foundation of Shandong Province (ZR2021QH032 and ZR2020QH281).