
Abstract
Deep vein thrombosis (DVT) is an important complication of stroke. As coronavirus disease 2019 (COVID-19) enters the stage of persistent and long-term management, the clinical management of DVT in stroke patients may require adjustment. The present study evaluated whether there was an increased risk of DVT in stroke patients during the COVID-19 period. Furthermore, we analyzed the possible risk factors and developed an easy-to-use nomogram to predict DVT in stroke patients during the long-term management of COVID-19. A total of 7087 stroke patients during the COVID-19 period and 14,174 patients with age, sex, and National Institutes of Health Stroke Scale (NIHSS) scores matched before the period from four centers were included. The incidence of DVT in stroke patients during the COVID-19 period (20.5%) was significantly higher than that before this period (15.9%, P < .001). Age, body mass index, smoking, D-dimer, physical activity level, NIHSS score, and intermittent pneumatic compression were significant predictors of DVT during the COVID-19 period (P < .05). A nomogram was constructed; internal and external validations showed high accuracy, and decision curve analysis showed excellent clinical applicability. This nomogram could evaluate the risk of DVT after stroke and assist in its early prevention during the long-term management of COVID-19.
Introduction
Deep vein thrombosis (DVT) is an important complication of ischemic stroke, and the incidence of DVT post-stroke varies from 10 to 75%. 1 The most serious complication of DVT is pulmonary embolism, which is the third most common cause of death from cardiovascular disease after heart attack and stroke. 2 DVT and pulmonary embolism are leading causes of death after stroke and during the period of active rehabilitation, with newly developed DVT increasing the rate of mortality at 3 months after stroke. 3 The current guidelines suggest that early preventive measures should be taken in stroke patients at high risk of DVT. 4 Hence, early and accurate identification of these high-risk patients is of great importance.
Although the coronavirus disease 2019 (COVID-19) global health emergency is over, it does not mean that the threat of COVID-19 to global human health has come to an end. According to World Health Organization (WHO) reports, COVID-19 has claimed 6.9 million lives and affected the health of over 770 million people. 5,6 The number of deaths due to COVID-19 last year is still as high as nearly 20,000/month, and the actual number may be higher. 6 WHO advised that it is time to transition to long-term management of the COVID-19 pandemic, which may take decades. Multiple studies have demonstrated an increased risk of DVT in COVID-19 patients, and COVID-19 was probably an additional risk factor for DVT in hospitalized patients. 7–12 In addition, some other studies found that the transition of people’s lifestyle during the COVID-19 period caused a decrease in physical activity and an increase in immobilization, especially for elderly people, which is known as one of the most important risk factors for DVT. 13–16 Due to the serious consequences of DVT in stroke patients, it is essential to explore whether the incidence and risk factors of DVT in stroke patients changed during the COVID-19 period. If they have changed, it is crucial to develop and validate a new clinical prediction model to identify the stroke patients at high risk of DVT during the period. However, there are few studies of these currently to the best of our knowledge.
Therefore, this study aimed to (a) compare the incidence of DVT in patients with acute ischemic stroke (AIS) during and before the COVID-19 period, (b) analyze the possible risk factors, and (c) develop and validate an easy-to-use and effective nomogram for evaluating the risk of DVT in AIS patients during the long-term management of COVID-19, for early prevention in the future.
Materials and Methods
Patients and Study Design
This multicenter study was performed at four large general hospitals in northeast China. AIS patients within 7 days from stroke onset who were admitted to the stroke centers of the four hospitals between June 2021 and May 2023 were consecutively enrolled. Patients were excluded if they (1) were aged <18 years, (2) did not have diffusion-weighted imaging to confirm ischemic stroke, or (3) were diagnosed with DVT before admission. Figure 1 shows the flowchart of the study. First, the incidence of DVT in AIS patients during the COVID-19 period was quantified. Second, each enrolled participant was randomly matched with two patients with AIS for age, sex, and National Institutes of Health Stroke Scale (NIHSS) scores between January 2018 and October 2019 using the electronic database of the stroke centers of the four hospitals. The incidence of DVT in AIS patients before and after the COVID-19 period was compared. Finally, the possible risk factors were analyzed, and a nomogram was developed and validated to predict the risk of DVT in AIS patients during the COVID-19 period. Study flowchart. DVT, deep vein thrombosis; COVID-19, coronavirus disease 2019.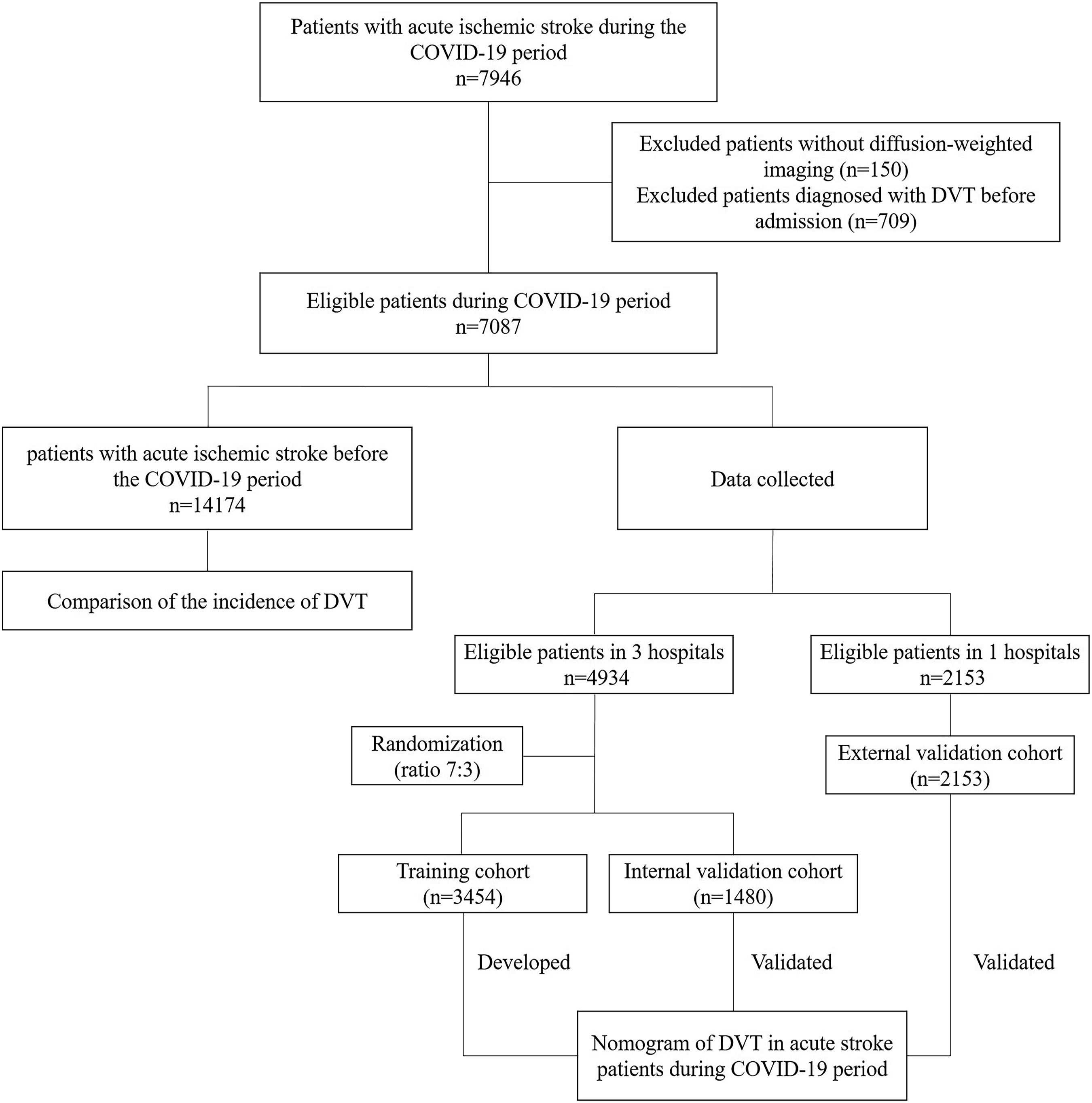
The study protocol was approved by the Ethics Committee of the First Hospital of Jilin University on February 16, 2021 (approval number: 2021-484). We prospectively collected the data of the patients with stroke between June 2021 and May 2023, and all these patients were fully informed of the procedure and provided written informed consent. We retrospectively reviewed the data of the patients with stroke between January 2018 and October 2019 using the electronic database, and the ethics committee waived the need for informed consent owing to the retrospective nature of the review. The study was completed in compliance with current privacy regulations.
Data Collection
Demographic data collected included age, sex, body mass index (BMI), medical comorbidities, pharmacological history, smoking, excessive drinking, history of DVT, and physical activity. Smoking was defined as having smoked at least one cigarette per day for 6 months or more. Excessive drinking was defined as consuming one or more alcoholic drinks per day during the past year. Physical activity levels were measured using the International Physical Activity Questionnaire (IPAQ)-Long Form according to the status in the last 7 days before admission and were classified as high-level, moderate-level, and low-level. 17 Laboratory data, including hemoglobin level, white blood cell count, platelet count, albumin level, fasting blood glucose level, homocysteine level, international normalized ratio, prothrombin time, activated partial thromboplastin time, fibrinogen level, D-dimer level, and C-reactive protein level, were measured within 24 h of admission. Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection within 3 months before admission, COVID-19 vaccination, and COVID-19 time duration at admission were also recorded. COVID-19 time duration at admission was defined as the time interval between patient enrollment and March 11, 2020, since COVID-19 being declared a global pandemic by the WHO on March 11, 2020. We defined the patients admitted before March 14, 2022, as those within the Delta variant period and the patients admitted after March 14, 2022, as those within the Omicron variant period since China’s National Health Commission announced that Omicron had replaced Delta as the main epidemic variant of COVID-19 in China on March 14, 2022. The neurological severity was collected and evaluated by the NIHSS scores examined by experienced vascular neurologists, initially at the time of admission. The component of arm and leg weakness of the NIHSS score was also presented, separately. The mechanism of the stroke was classified according to the TOAST (Trials of Org 10,172 in Acute Stroke) classification at discharge. 18 Furthermore, the administration of anticoagulant, antiplatelet, lipid-lowering agents, decompressive craniectomy, dehydration therapy, endovascular and thrombolysis therapies, and stay in intensive care unit (ICU) for acute stroke and intermittent pneumatic compression (IPC) for DVT prophylaxis during hospitalization were recorded. Dehydration therapy was defined as the use of osmotic agents after acute ischemic stroke, such as mannitol or hypertonic saline. 19
Lower Extremity Ultrasonography
The patients underwent lower extremity ultrasonography (LEUS) on the 7th day of admission, with the procedure being conducted by experienced physicians blinded to the clinical data. Data were obtained from the bilateral femoral, popliteal, peroneal, posterior tibial, and calf muscle veins using B-mode and color Doppler in the transverse and longitudinal views. Lack of compressibility or direct identification of an endoluminal thrombus was the criteria used for the diagnosis of DVT, as established in the literature. 11
Statistical Analyses
Normality of distribution was assessed using the Kolmogorov–Smirnov test. Continuous variables are expressed as mean ± standard deviation (SD) or median (interquartile range), and categorical variables are expressed as frequencies and percentages. Continuous variables were analyzed using the independent samples t-test or Mann–Whitney U-test, and categorical variables were analyzed using the chi-squared test or Fisher’s exact test. The patients enrolled between January 2018 and October 2019 were randomly matched with those enrolled between June 2021 and May 2023 for age ±2, sex, and NIHSS score equality using the electronic database. The eligible data from three hospitals during the COVID-19 period were randomly divided into training and internal validation cohorts at a ratio of 7:3 using the function “createDataPartition” in R (version 4.2.2, R Foundation for Statistical Computing, Vienna, Austria) to ensure that outcome events were randomly distributed between the two cohorts. Eligible data from one hospital during the COVID-19 period were used for the external validation cohort. Univariate variables with P ≤ .1 were retained in a multivariate logistic regression analysis, and backwards stepwise selection was performed, with improvement in the goodness-of-fit assessed by a reduction in the Akaike Information Criterion. We used Pearson’s or Spearman’s correlation coefficient or the chi-squared test and phi (φ) coefficient, whenever appropriate, to calculate the correlation among the statistically significant variables in the multivariate analysis. The variables with mild correlation were used to construct a nomogram to predict the risk of DVT. Nomogram performance was evaluated with respect to discrimination and calibration. For discrimination ability, the nomogram was evaluated using the area under the receiver operating characteristic (ROC) curve (AUC). For calibration ability, the nomogram was assessed using calibration curves. Internal and external validations were performed to validate the nomogram, and 1000 bootstrapping resamples were performed in each group for internal and external validations. Decision curve analysis (DCA) was used to evaluate the clinical benefits and utility of the nomogram. The 95% CIs and 2-tailed P-values were calculated. A P < .05 was considered statistically significant. Statistical analysis was performed using SPSS (version 26.0, IBM Corporation, Chicago, USA) and R version 4.2.0 (The R Foundation for Statistical Computing, Vienna, Austria).
Results
Incidence
During the COVID-19 period, 7946 AIS patients were admitted to the four stroke centers. After excluding 150 patients without diffusion-weighted imaging and 709 patients diagnosed with DVT before admission, 7087 patients were finally enrolled. Of these, 1456 patients (20.5%, 95% confidence interval [CI]:19.6%–21.5%) were positive for DVT. DVT was found in the femoral veins in 360 patients (24.7%), popliteal veins in 342 patients (23.5%), posterior tibial veins in 325 patients (22.3%), peroneal veins in 220 patients (15.1%), and calf muscle veins in 868 patients (59.6%). DVT was found on the left side in 833 patients (57.2%), the right side in 623 patients (42.8%), and bilaterally in 430 patients (29.5%). DVT was found in a single lower extremity vein in 1009 patients (69.3%) and >2 veins in the remaining patients. A total of 125 (8.6%) patients had pulmonary embolization.
A total of 14,174 patients with age, sex, and NIHSS scores matched before the COVID-19 period were randomly assigned, and 2256 patients (15.9%, 95% CI: 15.3%–16.5%) were positive for DVT. The incidence of DVT during the COVID-19 period was significantly higher than that before the period (P < .001). The characteristics of patients before and during the period are shown in Supplemental Table 1.
Characteristics of Patients During the COVID-19 Period
Of the 7087 patients during the COVID-19 period, 3454 were assigned to the training cohort, 1480 to the internal validation cohort, and 2153 to the external validation cohort. The patient characteristics are shown in Supplemental Table 2. Age, BMI, smoking, physical activity, D-dimer, stroke mechanism (large artery atherosclerosis and small vessel disease), NIHSS score (initial NIHSS score, NIHSS score of upper extremity, and NIHSS score of lower extremity), time from onset to admission, SARS-CoV-2 infection within 3 months, initial treatment in hospital (decompressive craniectomy and IPC), and ICU admission differed significantly between the non-DVT and DVT groups in the training set (all P < .05). There was no significant difference between the incidence of DVT in patients with moderate-level physical activity and high-level physical activity (15.7 vs 13.9%, P = .378), but they were both significantly lower than the incidence of DVT in patients with low-level physical activity (27.0%, P < .001).
Risk Factors
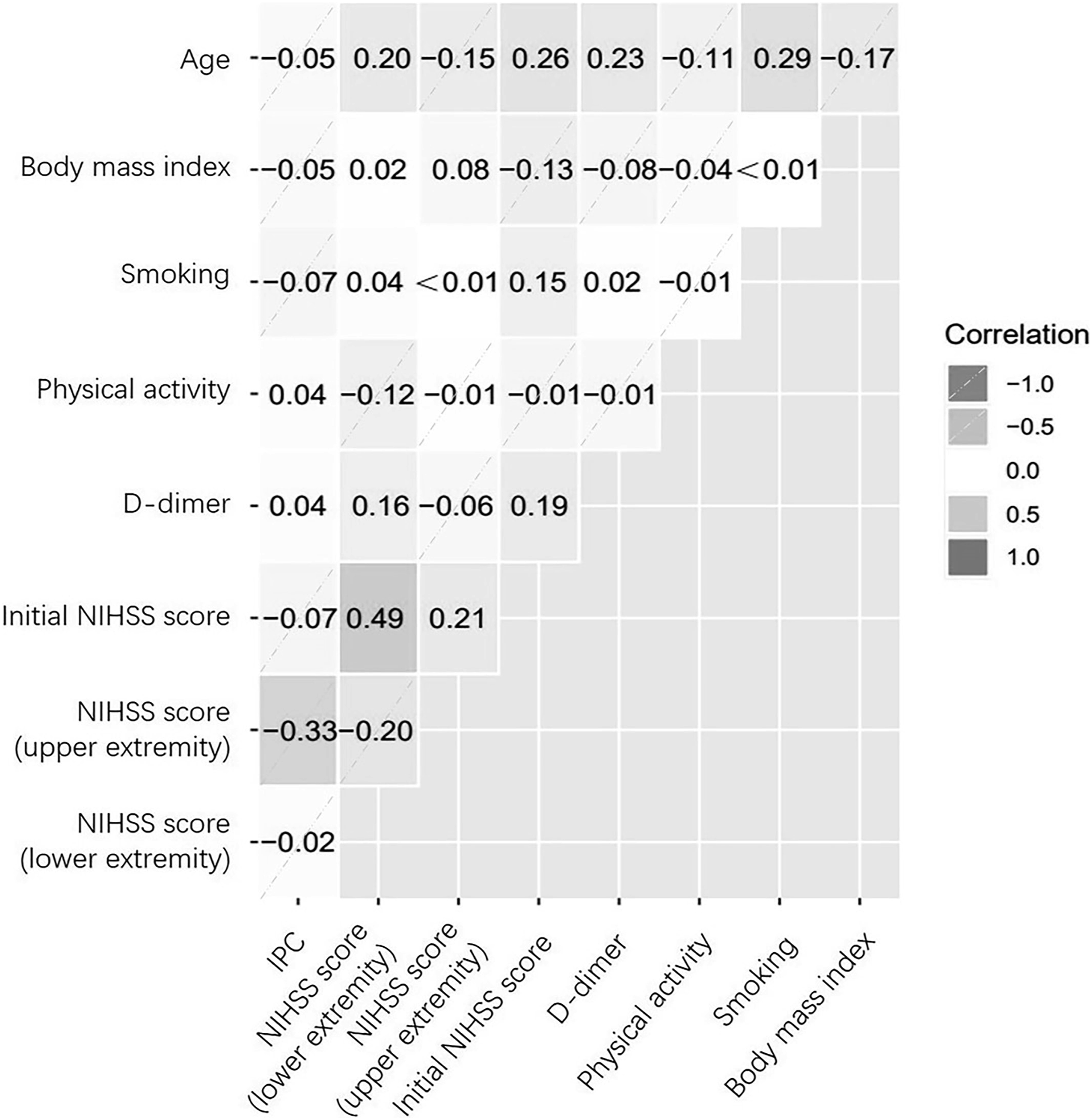
A total of 19 factors including age, sex, BMI, diabetes mellitus, dyslipidemia, smoking, physical activity, D-dimer, stroke mechanism (large artery atherosclerosis, small vessel disease, and cardioembolism), NIHSS score (initial NIHSS score, NIHSS score of upper extremity, and NIHSS score of lower extremity), time from onset to admission, SARS-CoV-2 infection within 3 months, initial treatment in hospital (decompressive craniectomy and IPC), and ICU admission were included in the multivariate logistic regression analysis, based on the univariate analyses (Supplemental Table 2). In the multivariate logistic regression model, we found that older age, higher BMI, smoking, low-level physical activity, higher D-dimer, and higher NIHSS score (initial NIHSS score, NIHSS score of upper extremity, and NIHSS score of lower extremity) were independently associated with increased odds, and IPC was independently associated with decreased odds of DVT in AIS patients (Figure 2). All the significant factors had mild correlations in the multivariate logistic regression model (all r or φ < 0.50, P < .001, Figure 3). Risk factors associated with stroke patients with deep vein thrombosis during the COVID-19 period. OR, odds ratio; CI, confidence interval; BMI, body mass index; NIHSS, National Institutes of Health Stroke Scale; SARS-CoV-2, severe acute respiratory syndrome coronavirus 2. Correlations among risk factors associated with patients with stroke and deep vein thrombosis during the COVID-19 period. NIHSS, National Institutes of Health Stroke Scale; IPC, intermittent pneumatic compression.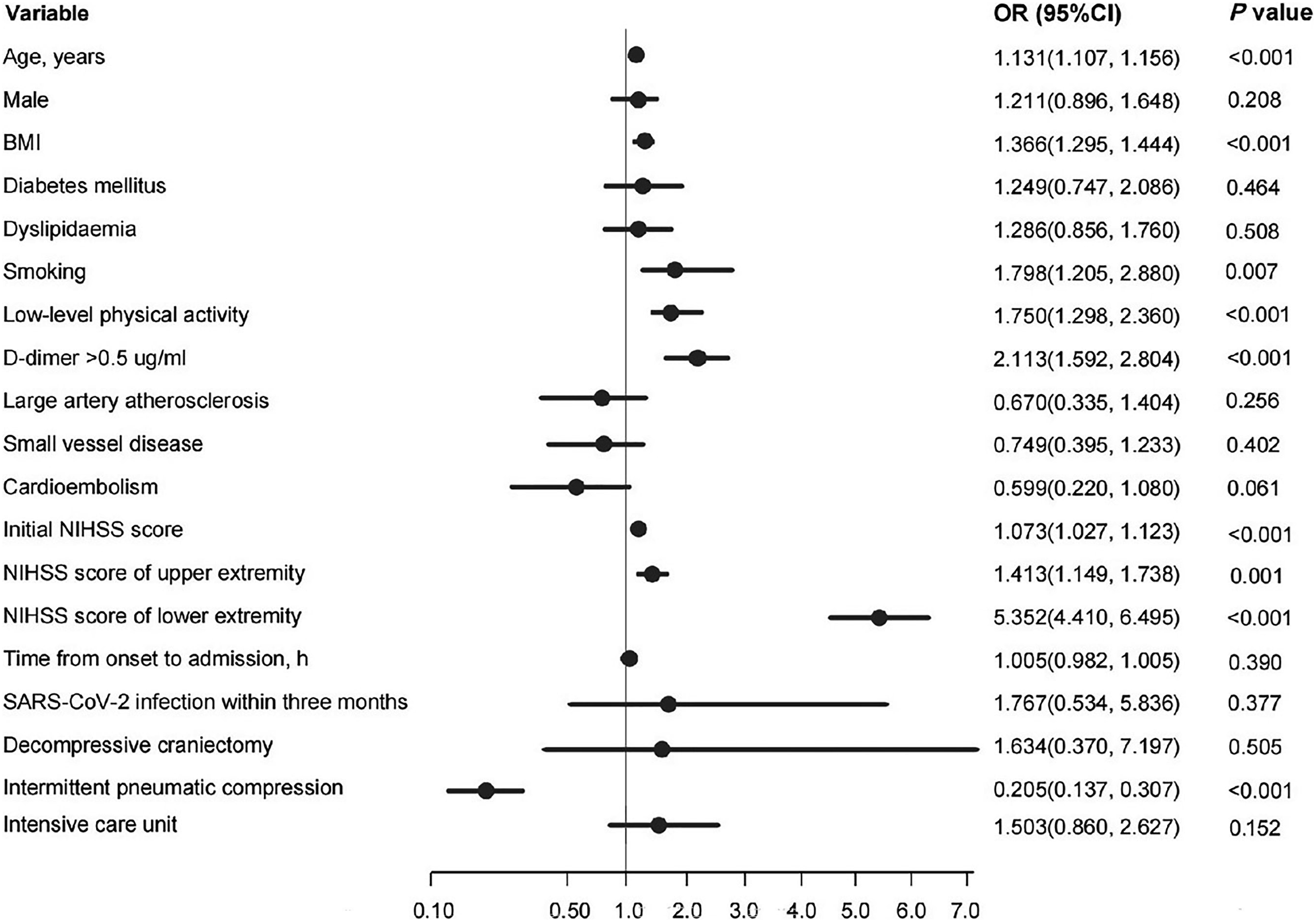
Nomogram Construction
The final logistic model incorporated nine independent predictors (age, BMI, smoking, physical activity, D-dimer, initial NIHSS score, NIHSS score of upper extremity, NIHSS score of lower extremity, and intermittent pneumatic compression) was developed as a simple-to-use nomogram, as shown in Figure 4. In the tool, the total points score was obtained by summing the calculated points of each variable; thus, the probability of DVT was estimated. For example, an acute stroke patient of 80 years old, a BMI of 30, smoking, normal D-dimer, low-level physical activity, initial NIHSS score of 12, NIHSS score of lower extremity of 2, NIHSS score of lower extremity of 3, and without IPC for DVT prophylaxis had an approximately 50% predicted probability of DVT using this nomogram. Nomogram of DVT in stroke patients during the COVID-19 period. DVT, deep venous thrombosis; BMI, body mass index; NIHSS, National Institutes of Health Stroke Scale.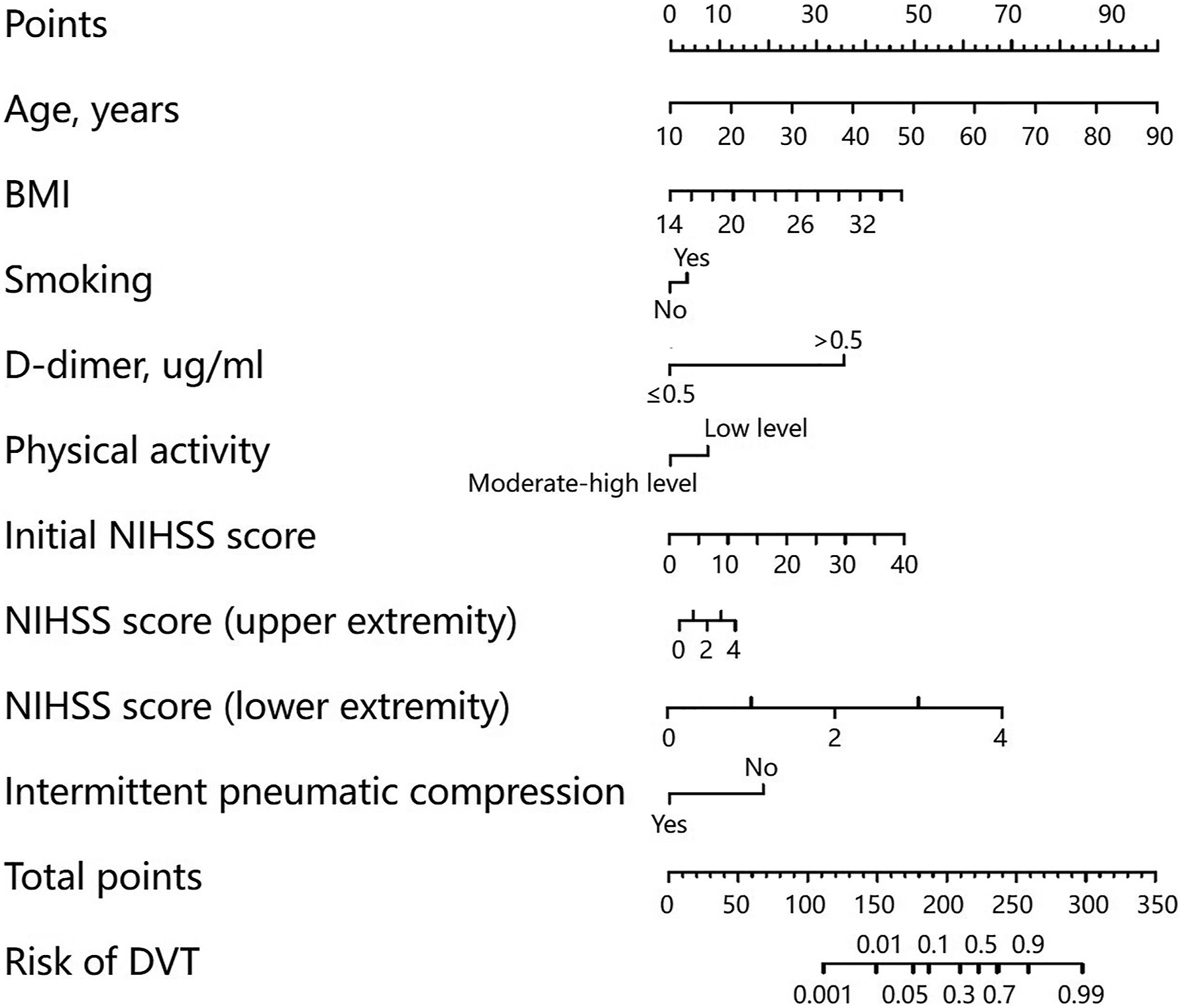
Performance and Validation of the Nomogram
The calibration of the model was assessed using calibration curves. The nomogram calibration curve demonstrated a good agreement between the prediction and observation in all cohorts (Supplemental Figure 1). ROC analysis was used to evaluate the predictive efficiencies of the nomogram model and showed excellent discrimination in all cohorts (Supplemental Figure 1). The AUC values of the nomogram in the training, internal validation, and external validation cohorts were 0.908 (95% CI, 0.895–0.921), 0.874 (95% CI, 0.853–0.895), and 0.892 (95% CI, 0.874–0.910), respectively.
Clinical Use
To evaluate the clinical applicability of the nomogram, DCA (Supplemental Figure 2), an advanced method for analyzing the net clinical benefits of predictive models, indicated that the most favorable threshold probability for predicting DVT in the training cohort with the nomogram was 0.1–0.8. As demonstrated by the favorable threshold probability, it indicated that the nomogram could assist clinicians to assess the risk of DVT in AIS patients during the COVID-19 period accurately.
Discussion
This study compared the incidence of DVT in AIS patients before and during the COVID-19 period, analyzed the possible risk factors, and developed and validated a nomogram to evaluate the risk of DVT in AIS patients during the COVID-19 period. Three main results were obtained in our study. First, the incidence of DVT in AIS patients during the COVID-19 period was significantly higher than that before the period. Second, we found that age, BMI, smoking, physical activity, D-dimer, NIHSS score (initial NIHSS score, NIHSS score of upper extremity, and NIHSS score of lower extremity), and IPC were independently associated with DVT in AIS patients during the COVID-19 period. Third, a reliable nomogram was constructed based on the significant risk factors. Internal and external validations of the nomogram showed a high accuracy in predicting DVT in AIS patients during the COVID-19 period.
Multiple studies have demonstrated an increased risk of DVT in COVID-19 patients and suggested that individual thromboprophylaxis therapy be considered for them. 7–12 Indeed, patients hospitalized for COVID-19 are the prototypical examples of acutely ill medical patients at an increased risk of DVT, as they suffer from an acute infection, may have acute respiratory failure, are often bedridden, or have reduced mobility, because they need oxygen supplementation and/or are isolated in their room due to hospital restrictions. 11 In addition, recent studies found that the people’s lifestyle changed during the COVID-19 period, especially for elderly people, which manifested in a decrease in physical activity and an increase in immobilization. It is known as one of the most important risk factors for DVT. 13–16 DVT is an important complication of ischemic stroke. DVT and pulmonary embolism are leading causes of death in stroke patients. 3 Hence, it is important to identify whether the conditions of DVT in stroke patients change during the COVID-19 period. Our study compared the hemostasis variables in AIS patients before and during the COVID-19 period and found no significant differences between the variables before and during the period (Supplemental Table 1). Besides, our study compared the incidence of DVT in AIS patients before and during the COVID-19 period. In order to reduce the bias caused by the difference in the severity of neurological deficits of hospitalized stroke patients before and after the COVID-19 period, we adopted the age, sex, and NIHSS score matched method to enroll AIS patients before and during the period. We found that the incidence of DVT in AIS patients during the period was significantly higher than that before the period.
Since the incidence was increasing, it is very important to identify the risk factors of DVT in this specific period. In our study, older age, higher BMI, smoking, low-level physical activity, higher D-dimer, and higher initial NIHSS score (initial NIHSS score, NIHSS score of upper extremity, and NIHSS score of lower extremity) were independently associated with increased odds, and IPC was independently associated with decreased odds of DVT in AIS patients during the period. As described in our study, increased age, obesity, and smoking as risk factors for DVT have been confirmed in multiple subgroups of patients in many studies. 7,10,20–22 These studies have shown that the estimated annual incidence of DVT is 0.1%, and it occurs more commonly as people age, with the rate in persons aged ≥60 years rising to nearly 1%. 21,23 A BMI >30 roughly doubles the risk of DVT through a mechanism of venous stasis related to decreased lower-extremity muscle contraction and venous pump. 21 Smoking is significantly associated with an increased risk of DVT, regardless of currently smoking or quitting smoking. 22 Severe neurological deficits were also associated with DVT in acute ischemic stroke patients. There was a significant difference in the NIHSS score between those with and without DVT. Especially the NIHSS score of the lower leg weakness, which directly influences the ambulation in their acute period, showed a significant difference. D-dimer is a significant predictor of DVT. But it has a high sensitivity but low specificity for the diagnosis of DVT. Elevated D-dimer levels are nonspecific and can also be seen in pregnancy, heart disease, and recent surgery as well as inflammatory conditions. 24
Previous studies found that IPC was an effective and inexpensive method of reducing the risk of DVT and improving survival in immobile stroke patients. 25 Our study confirmed the protective effect of IPC on DVT. Furthermore, most of the evidence has identified a significant decrease in physical activity level during the COVID-19 period. 14 Although most scholars believe that lack of physical activity is a risk factor for venous thromboembolism, the relationship between physical activity and venous thromboembolism is complex, and there is a controversy over whether there is a dose-dependent relationship between physical activity and venous thromboembolism, due to the lack of an operational definition and standardized assessment method for physical activity. 26 In our study, we applied the IPAQ-Long Form to evaluate physical activity in AIS patients and divided it into three levels. IPAQ is a comparable and standardized self-report measure of habitual physical activity of populations from different countries and socio-cultural contexts. Its validity and reliability have been verified by multiple countries and populations. 17 To the best of our knowledge, our study is the first to apply this questionnaire to evaluate the physical activity of patients with DVT. The results showed that low-level physical activity was independently associated with increased odds of DVT in AIS patients. Moreover, compared with other risk factors for DVT in AIS patients during the COVID-19 period in our study, physical activity and IPC were controllable factors. Therefore, moderate-high level physical activity evaluated by IPAQ-Long Form and IPC are recommended during the COVID-19 period, especially for older patients and those with obesity.
The current guidelines suggest that early preventive measures should be taken in stroke patients at high risk of DVT. 4 So an early and accurate DVT risk assessment in AIS patients during the COVID-19 period is of great importance. For this purpose, we constructed a personalized nomogram to predict the risk of DVT in AIS patients during the period and proved the accuracy of its prediction results through internal and external validations. The nomogram demonstrated good discrimination and performance in the training and validation cohorts. Our study should provide reference for the management of DVT in AIS patients during the COVID-19 period.
Our study had some limitations. First, although we enrolled almost all AIS patients in four centers in northeast China during the COVID-19 period, the sample size was relatively small. In future, we plan to conduct a similar study with a larger sample size in other regions or countries to verify our results. Second, many confounding factors could have affected the results in the comparison of the incidence of DVT in patients with acute ischemic stroke before and during the COVID-19 period. Therefore, we matched the patients for age, sex, and National Institutes of Health Stroke Scale score to reduce the bias caused by the difference in the severity of neurological deficits in patients hospitalized for stroke before and during the COVID-19 period. However, potential unmeasured confounders may have persisted. We aim to conduct a study in the future to balance additional potential confounding factors and verify our results.
Conclusion
The incidence of DVT in AIS patients during the COVID-19 period was significantly higher than that before the period. Age, BMI, smoking, D-dimer, physical activity, NIHSS score (initial NIHSS score, NIHSS score of upper extremity, and NIHSS score of lower extremity), and IPC were significant predictors of DVT in AIS patients during the COVID-19 period. The nomogram provides a simple-to-use tool to evaluate the risk of DVT in AIS patients during the period, with the aim of early prevention.
Supplemental Material
Supplemental Material - A Nomogram for Predicting the Risk of Deep Vein Thrombosis in Patients With Acute Ischemic Stroke During the COVID-19
Supplemental Material for A Nomogram for Predicting the Risk of Deep Vein Thrombosis in Patients With Acute Ischemic Stroke During the COVID-19 by Jie Zhang, Shurui Zhang, Ge Song, Shimeng Zhuang, Hua Li, Lisi An, Yan Meng, Jiayu Fan, and Lijuan Wang in Angiology.
Footnotes
Acknowledgments
The authors acknowledge all the patients for their participation in this study.
Author’s note
This author takes responsibility for all aspects of the reliability and freedom from bias of the data presented and their interpretation.
Author contributions
All authors substantially contributed to (1) conception and design, or acquisition of data, or analysis and interpretation of data, (2) drafting the article or revising it critically for important intellectual content, and (3) final approval of the version to be published.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Natural Science Foundation of Jilin Province (YDZJ202201ZYTS139) and Department of Science and Technology of Jilin Province (20230508100RC).
Data Availability Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.