
Abstract
Lipoprotein (a) [Lp(a)] could contribute to coronary artery disease (CAD) through proinflammatory effects. The neutrophil to lymphocyte ratio (NLR) is an inflammatory biomarker. We consecutively enrolled 7,922 CAD patients to investigate the synergistic association of Lp(a) and NLR with prognosis in patients undergoing percutaneous coronary intervention (PCI). NLR was calculated as the neutrophil count divided by the lymphocyte count. Cutoff for NLR was a median of 2.07. The threshold value was set at 30 mg/dL for Lp(a). The primary endpoint was major adverse cardiac events (MACEs), including all-cause mortality and myocardial infarction. During 2 years follow-up, 111 (1.40%) MACEs occurred. Lp(a) > 30 mg/dL was associated with an increased MACE risk in participants with NLR ≥2.07 [adjusted hazard ratio (HR), 1.84; 95% CI, 1.12–3.03], but not in participants with NLR <2.07 (adjusted HR, 0.74; 95% CI, 0.38–1.45) (Pinteraction = 0.021). Subgroup analysis demonstrated that the synergistic association of Lp(a) and NLR with prognosis was more pronounced in female patients (Pinteraction = 0.028). This study suggested that combining Lp(a) and NLR may be useful for risk stratification in CAD population.
Keywords
Introduction
Substantial residual atherosclerotic cardiovascular disease (ASCVD) risks persist despite established therapies have led to the effort to identify novel biomarkers and treatment targets. Lipoprotein (a) [Lp(a)] is a low-density lipoprotein (LDL)-like particle comprising an apolipoprotein B-100 (apoB) covalently bound to a single apolipoprotein(a) [apo(a)] particle via a disulfide linkage. 1 Lp(a) has been shown to promote ASCVD through atherogenic, proinflammatory, and prothrombotic effects. Data from cohort and genetic studies have suggested a causal association of elevated Lp(a) with the risk of ASCVD, calcific aortic valve stenosis, and ischemic stroke. 2
Inflammation is another emerging therapeutic target to potentially reduce residual ASCVD risks.3,4 Recent studies have demonstrated that inflammation could modify Lp(a)-related ASCVD risk in the context of both primary and secondary preventions.2,5
The neutrophil to lymphocyte ratio (NLR) is an easily available inflammatory biomarker in peripheral blood, which combines both innate immunity, primarily due to neutrophils, and adaptive immune response, supported by lymphocytes.6,7 Previous studies demonstrated that NLR could reflect elevations in C-reactive protein (CRP) and interleukin-6 (IL-6) in both acute and chronic inflammatory conditions.8,9 Cumulative evidence has shown that baseline NLR could independently predict cardiovascular (CV) events and mortality in both primary and secondary prevention scenarios. 9 Notably, the relationship between NLR and prognosis persisted even after adjustment for high-sensitivity CRP (hsCRP), which conveys the information that an elevated NLR potentially has inflammatory atherosclerotic process additional to cytokines or hsCRP. 10 However, to date, there is a scarcity of literature investigating the association of Lp(a) and NLR with adverse clinical events in patients with coronary artery disease (CAD). Therefore, this study aimed to explore the combined impact of Lp(a) and NLR on risk of adverse events in CAD patients undergoing percutaneous coronary intervention (PCI).
Methods
Study Design
This study was a prospective, observational cohort study, which consecutively screened 10,724 patients undergoing PCI at Fuwai Hospital between January 2013 and December 2013. Patients with age >18 years who underwent PCI were included in this study. Patients with missing baseline complete blood count and Lp(a) measurements, and/or other exclusion criteria were excluded (Figure 1). This study complied with the Declaration of Helsinki and was approved by the Institutional Review Board at our hospital. Each participant provided informed written consent before intervention. Study flowchart. Abbreviations: PCI, percutaneous coronary intervention; NLR, neutrophil to lymphocyte ratio; Lp(a), lipoprotein (a).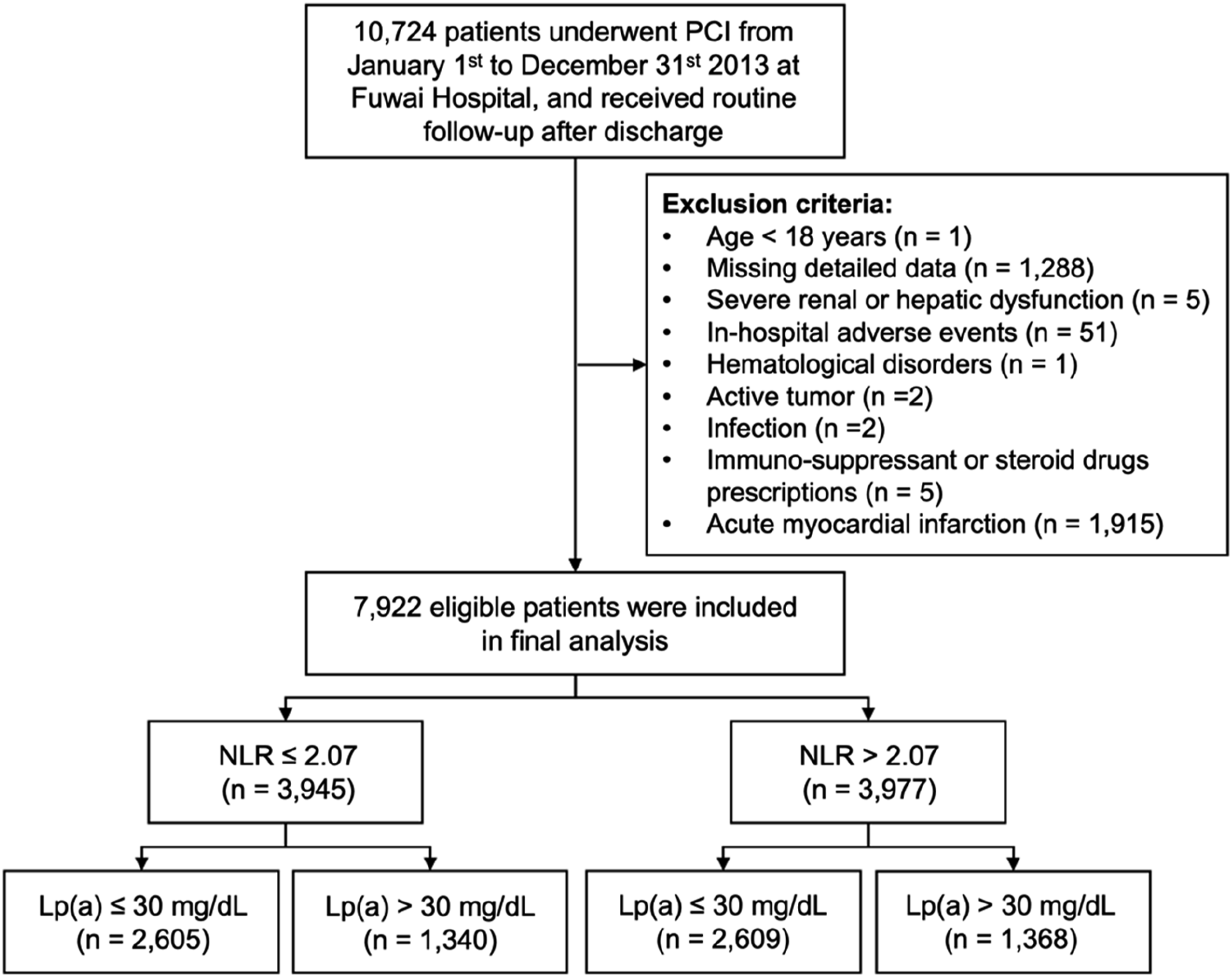
Interventional Procedures
PCI was performed by experienced cardiologists in compliance with standard techniques. The choice of devices, additional examinations (i.e., intravascular ultrasound and optical coherence tomography), and detailed approach were left to the discretion of operators. Before the index procedure, aspirin (300 mg) and a P2Y12 inhibitor (clopidogrel 300–600 mg or ticagrelor 180 mg) were administered to all participants. Procedural anticoagulation was achieved with unfractionated heparin or bivalirudin. After the catheterization, aspirin 100 mg/day was prescribed lifelong and clopidogrel 75 mg/day typically for 12 months. Data were subsequently entered in a dedicated database by independent research personnel.
Coronary angiographic and procedural information was reviewed and recorded by two independent experienced observers and disagreement was resolved by consulting other experts. Accordingly, left main (LM) disease was defined as stenosis of ≥50% in LM coronary artery and three-vessel disease was diagnosed by stenosis of ≥50% in all three main coronary arteries (i.e., left anterior coronary artery, left circumflex artery, and right coronary artery). Chronic total occlusion (CTO) was defined as total obstruction of a native coronary artery for >3 months with thrombolysis in myocardial infarction (TIMI) flow grade of 0. The synergy between PCI with taxus and cardiac surgery (SYNTAX) score was estimated using an online calculator (https://www.syntaxscore.com/) to assess the lesion complexity by interventionists unaware of the clinical information.
Laboratory Tests, Echocardiography, and Definitions
On admission, fasting venous blood was regularly drawn from each participant and tested by the clinical chemistry department at Fuwai Hospital. Complete blood count was performed using an automatic blood cell analyzer (XT-1800i; Sysmex Corporation, Kobe, Japan). Consistent with previous similar research, 11 the concentrations of Lp(a) were measured by an immunoturbidimetry method based on the manufacturer’s guide, a latex turbidimetric method [LASAY Lp(a) auto; SHIMA laboratories; Tokyo, Japan]. The hsCRP levels were estimated by immunoturbidimetry (Beckmann Assay 360, Bera, Calif., USA). A Tosoh Automated Glycohemoglobin Analyzer (HLC-723G8, Tokyo, Japan) was utilized to assay HbA1c levels. Measurements of other laboratory indexes, including lipid profiles, fasting blood glucose (FBG), and serum creatinine were performed at the core laboratory in our hospital, according to the standard techniques. 12 Left ventricular ejection fraction (LVEF) was measured from two-dimensional echocardiography according to the modified Simpson’s rule.
NLR was calculated using the following formula: plasma neutrophil count (*109/L) divided by plasma lymphocyte count (*109/L). The cut-off value of NLR was determined according to the median of NLR (2.07). The threshold value was set at the 30 mg/dL for Lp(a) according to the recent European Atherosclerosis Society Lp(a) consensus statement. 13
Diabetes mellitus was determined by FBG ≥7.0 mmol/L (126 mg/dL), or hemoglobin A1c (HbA1c) levels ≥6.5%, or 2-h blood glucose of oral glucose tolerance test ≥11.1 mmol/L (200 mg/dL), or previous definite diagnosis with hypoglycemic drugs treatment. 14 Hypertension was defined as newly confirmation more than twice on different days by systolic blood pressure ≥140 mmHg and/or diastolic blood pressure ≥90 mmHg during the baseline hospitalization or known hypertension with antihypertensive medication. Patients with fasting total cholesterol (TC) ≥5.2 mmol/L, LDL cholesterol (LDL-C) ≥3.4 mmol/L, high density lipoprotein cholesterol (HDL-C) <1.0 mmol/L, triglycerides (TG) ≥1.7 mmol/L, and/or receiving lipid-lowering medications were diagnosed as dyslipidemic. Body mass index (BMI) was calculated as weight (kg) divided by height (m). 2
Study Endpoints
The clinical status was followed up at 1, 6, 12, and 24 months by outpatient visits or telephone contact. The primary endpoint was major adverse cardiac events (MACEs), defined as all-cause mortality and myocardial infarction (MI). Secondary endpoints were all-cause mortality, CV death, MI, and target-vessel revascularization (TVR). Death was considered CV-caused unless unequivocal non-cardiovascular cause could be established. MI was determined based on clinical manifestation and laboratory tests, according to the third universal definition of MI. 15 TVR was defined as repeat PCI or coronary artery bypass graft (CABG) in the target vessel according to the first Academic Research Consortium recommendations. 16 All clinical events were adjudicated by two independent experienced cardiologists, blinded to this study. Inconsistencies were resolved by consulting other experts.
Statistical Analyses
Continuous variables were described as mean with standard deviation and compared using Student’s t test, or analysis of variance, as appropriate. Categorical variables were summarized as frequency with percentage and compared using Chi-square test or Fisher’s exact test, as appropriate.
In survival analysis, linearity assumptions of NLR and Lp(a) for the MACE risk were illustrated by restricted cubic splines (RCS) adjusted for age and male sex. The risks of MACEs in different groups were depicted by Kaplan–Meier survival curves and compared by log-rank test. Proportional hazards assumption was determined by Schoenfeld residuals. The impact of NLR and Lp(a) on adverse clinical events was estimated by univariable and multivariable Cox regression analyses. Hazard ratios (HRs) and 95% confidence intervals (CIs) were presented. In the multivariable Cox analysis, age, male sex, BMI, hypertension, diabetes mellitus, current smoker, previous MI, previous PCI/CABG, previous stroke, LVEF, TC, LDL-C, hsCRP, serum creatinine, LM/three-vessel disease, CTO lesion, and SYNTAX score, were included due to their statistical significance in univariable analysis or clinical importance. Additionally, we carried out subgroup analyses for the risk of MACEs among four different subsets and exhibited as the forest plot. A two-tailed P < .05 was considered as statistically significant. All statistical analyses were performed using RStudio software (version 2021.09.0; https://www.rstudio.org/).
Results
Patients and Baseline Characteristics
Baseline Characteristics of Study Population by Different Levels of Lp(a) and NLR.
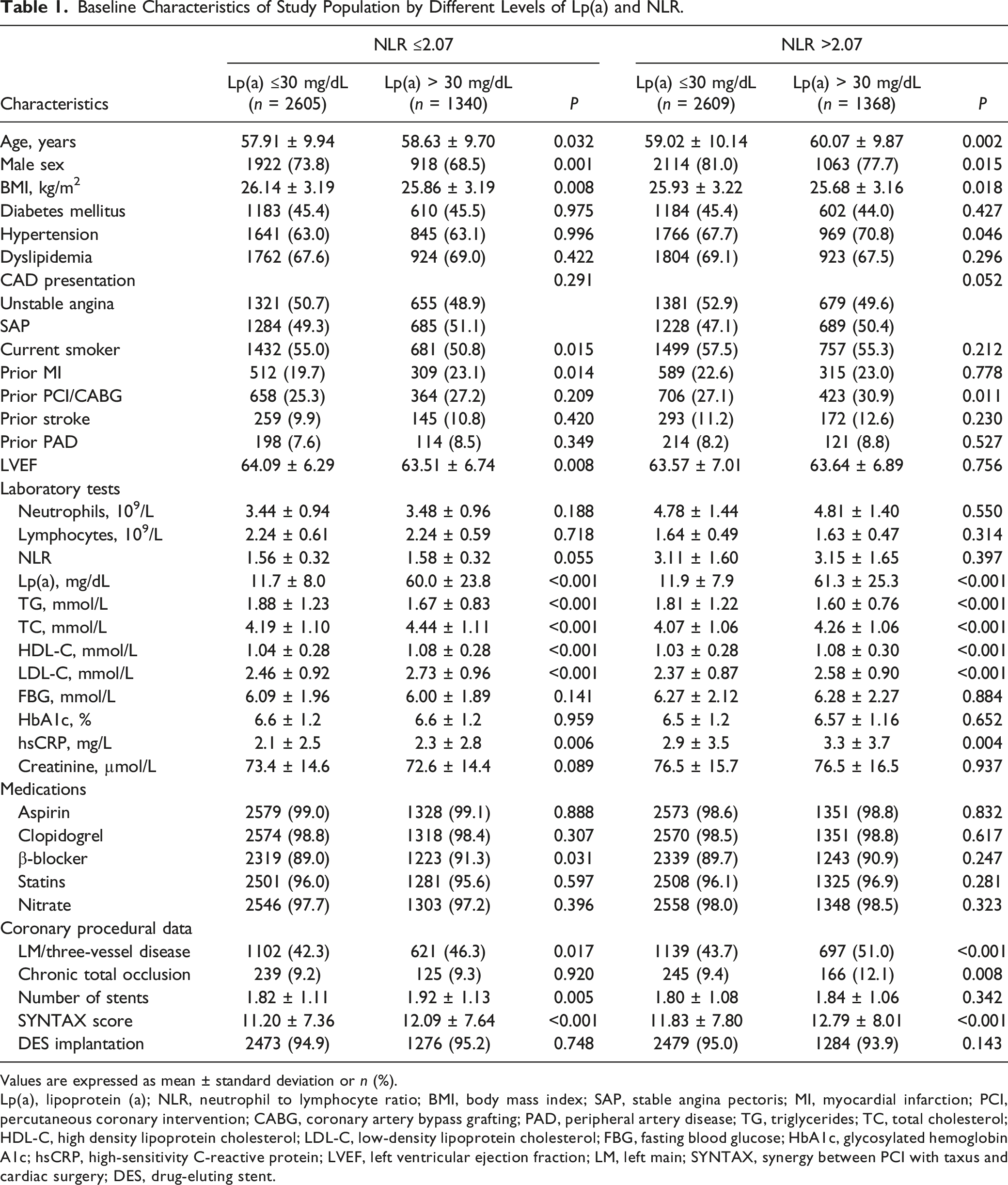
Values are expressed as mean ± standard deviation or n (%).
Lp(a), lipoprotein (a); NLR, neutrophil to lymphocyte ratio; BMI, body mass index; SAP, stable angina pectoris; MI, myocardial infarction; PCI, percutaneous coronary intervention; CABG, coronary artery bypass grafting; PAD, peripheral artery disease; TG, triglycerides; TC, total cholesterol; HDL-C, high density lipoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol; FBG, fasting blood glucose; HbA1c, glycosylated hemoglobin A1c; hsCRP, high-sensitivity C-reactive protein; LVEF, left ventricular ejection fraction; LM, left main; SYNTAX, synergy between PCI with taxus and cardiac surgery; DES, drug-eluting stent.
Association of Lp(a) with MACEs according to Different NLR Levels
Lp(a) in relation to clinical event rates according to different level of NLR.
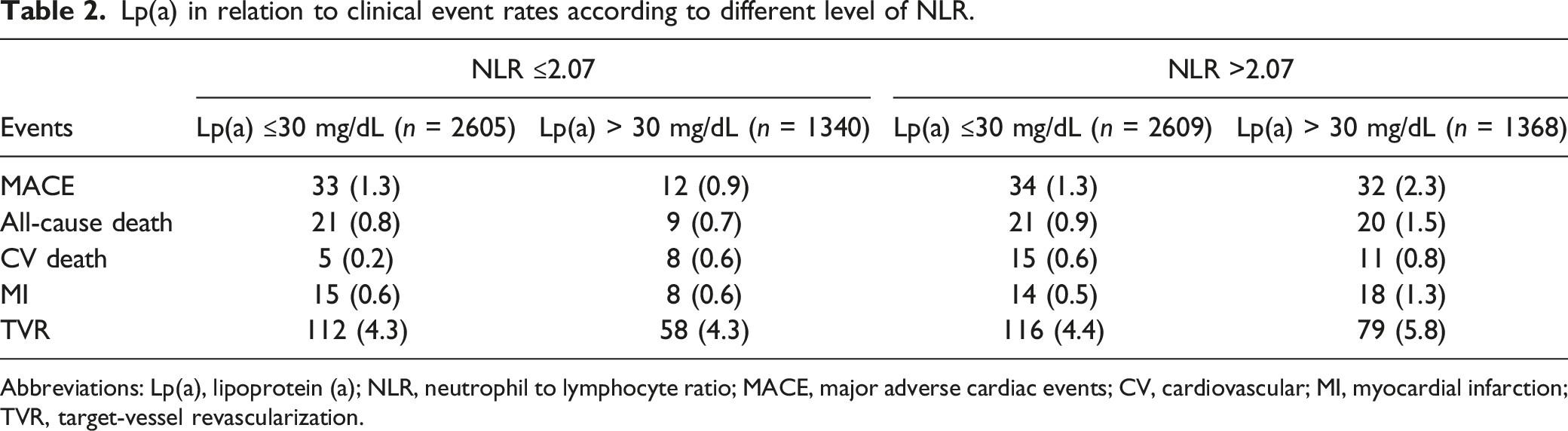
Abbreviations: Lp(a), lipoprotein (a); NLR, neutrophil to lymphocyte ratio; MACE, major adverse cardiac events; CV, cardiovascular; MI, myocardial infarction; TVR, target-vessel revascularization.
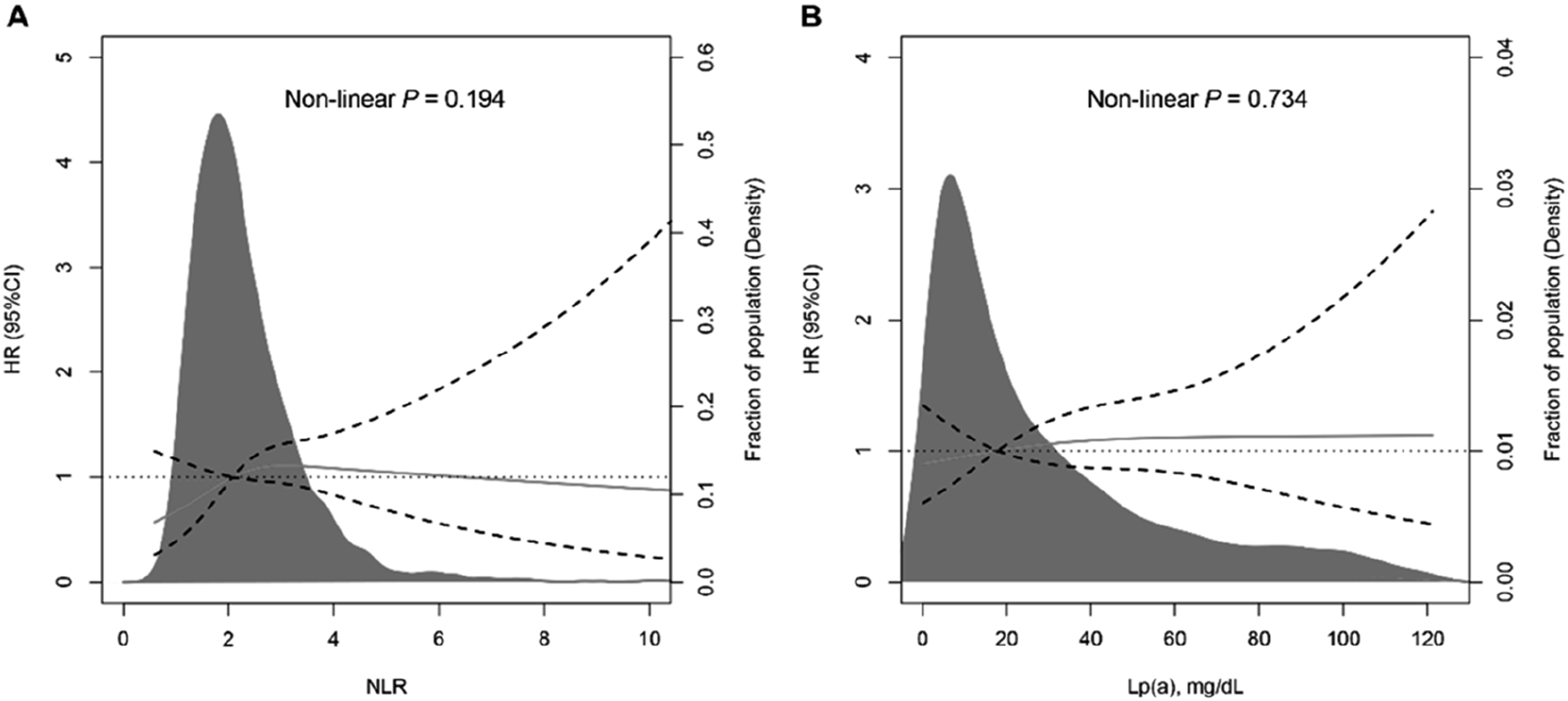
Restricted cubic spline curves for (A) the association between NLR and the 2-year risk of MACEs; (B) the association between Lp(a) and the 2-year risk of MACEs. Models adjusted for age and male sex. HRs are indicated by blue solid lines and 95%CIs by light-blue dotted line. Abbreviations: Lp(a), lipoprotein (a); NLR, neutrophil to lymphocyte ratio; HR, hazard ratio; CI, confidence interval; MACE, major adverse cardiac events.
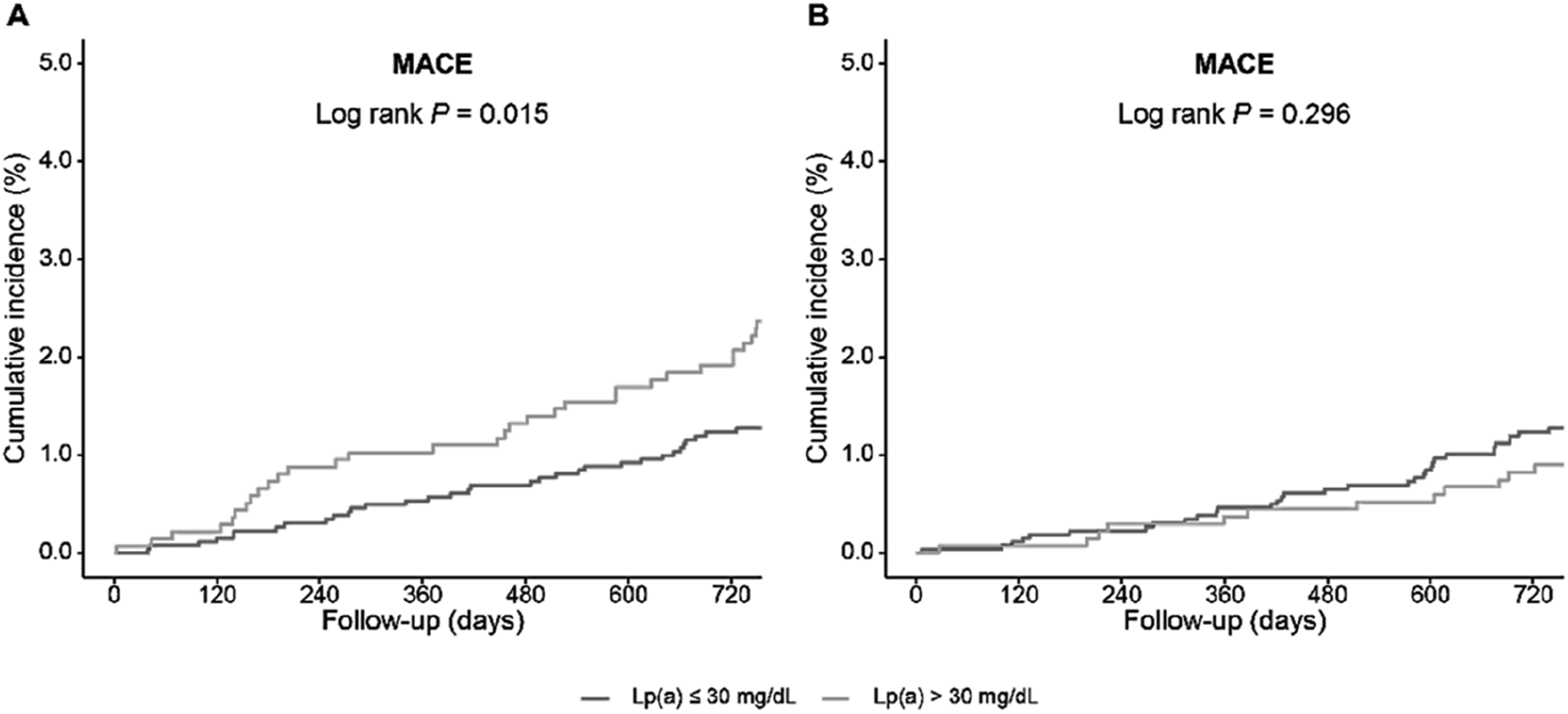
Kaplan–Meier curves for cumulative incidence of MACEs across clinical strata of Lp(a) in patients with NLR >2.07 (A) and NLR ≤2.07 (B). Abbreviations: MACEs, major adverse cardiac events; Lp(a), lipoprotein (a); NLR, neutrophil to lymphocyte ratio.
Cox regression analysis of Lp(a) > 30 mg/ml versus Lp(a) ≤30 mg/ml with clinical endpoints.
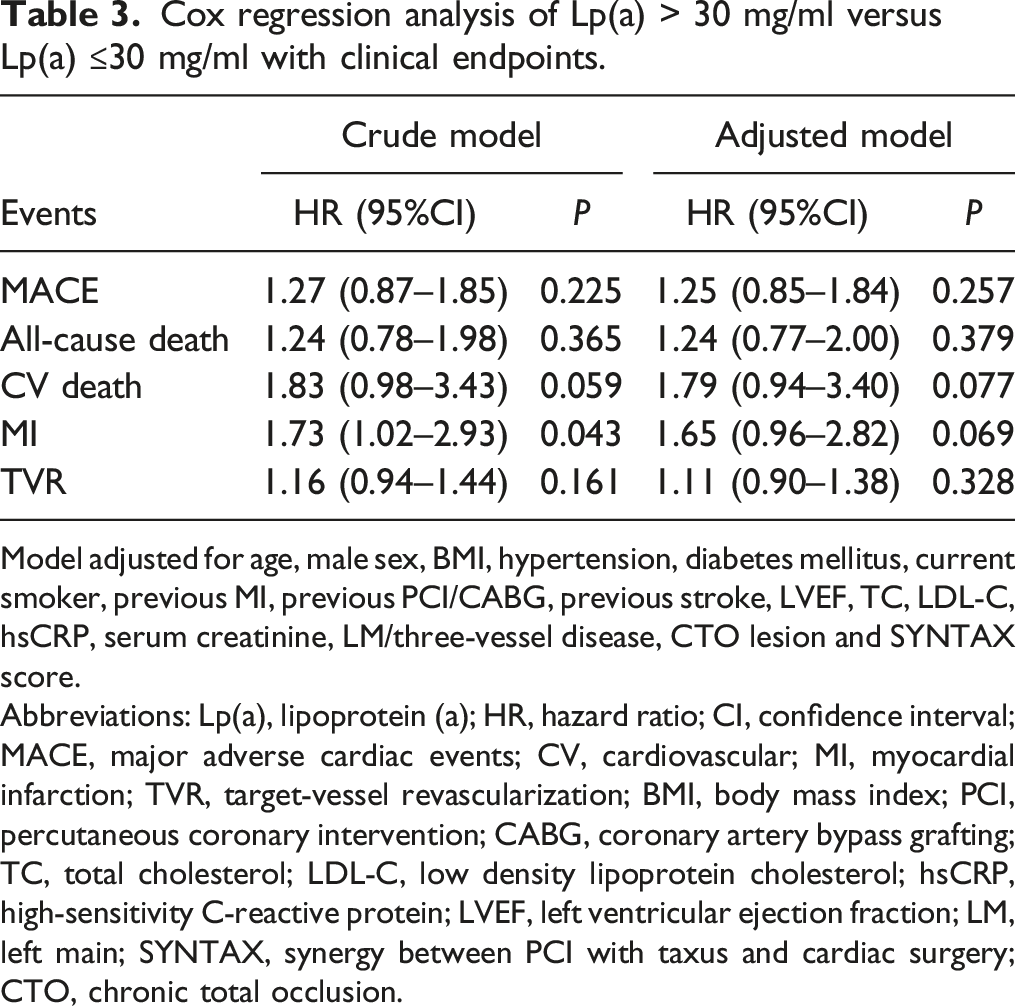
Model adjusted for age, male sex, BMI, hypertension, diabetes mellitus, current smoker, previous MI, previous PCI/CABG, previous stroke, LVEF, TC, LDL-C, hsCRP, serum creatinine, LM/three-vessel disease, CTO lesion and SYNTAX score.
Abbreviations: Lp(a), lipoprotein (a); HR, hazard ratio; CI, confidence interval; MACE, major adverse cardiac events; CV, cardiovascular; MI, myocardial infarction; TVR, target-vessel revascularization; BMI, body mass index; PCI, percutaneous coronary intervention; CABG, coronary artery bypass grafting; TC, total cholesterol; LDL-C, low density lipoprotein cholesterol; hsCRP, high-sensitivity C-reactive protein; LVEF, left ventricular ejection fraction; LM, left main; SYNTAX, synergy between PCI with taxus and cardiac surgery; CTO, chronic total occlusion.
Cox regression analysis of Lp(a) > 30 mg/ml versus Lp(a) ≤30 mg/ml with clinical endpoints according to different levels of NLR.
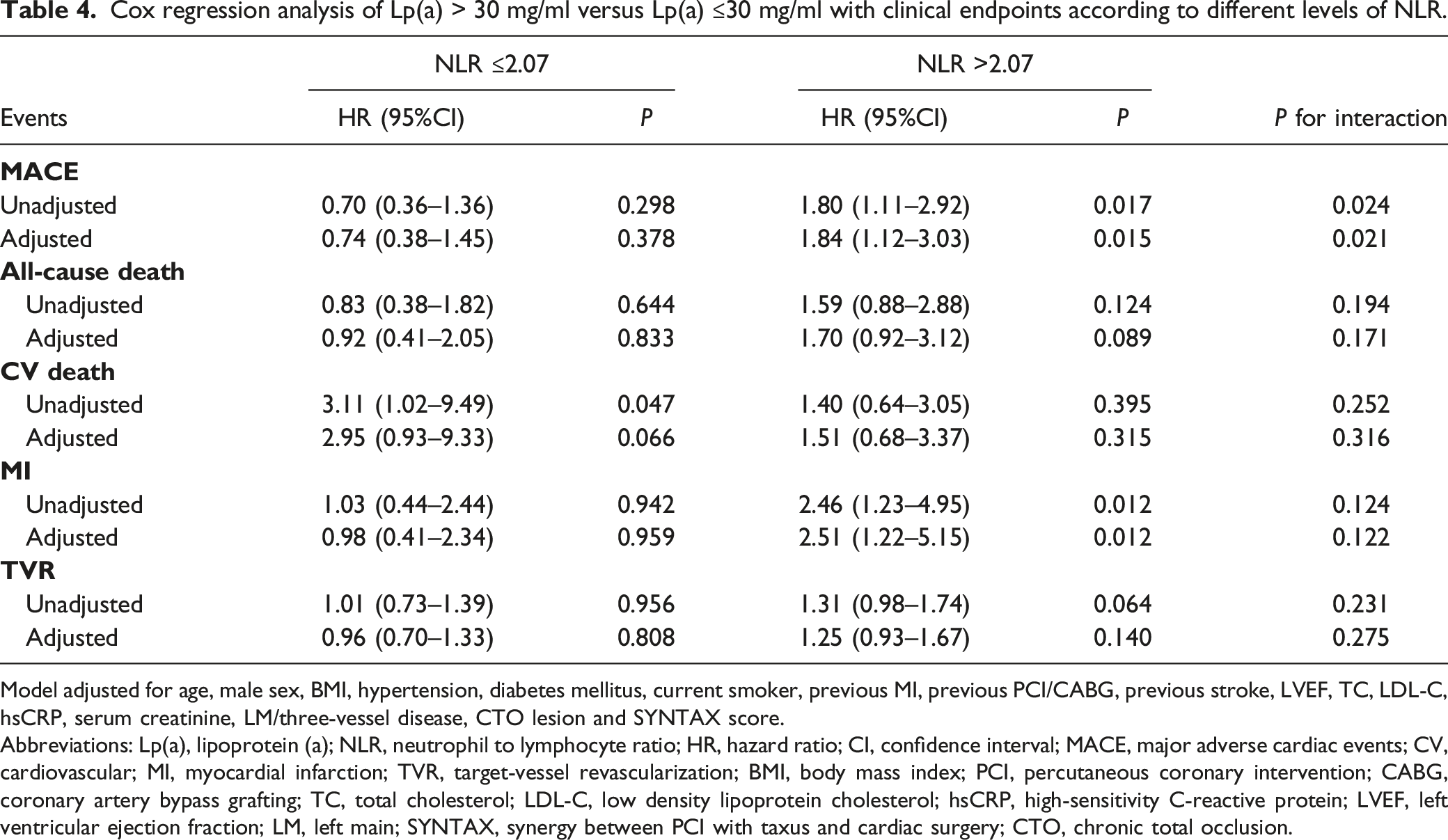
Model adjusted for age, male sex, BMI, hypertension, diabetes mellitus, current smoker, previous MI, previous PCI/CABG, previous stroke, LVEF, TC, LDL-C, hsCRP, serum creatinine, LM/three-vessel disease, CTO lesion and SYNTAX score.
Abbreviations: Lp(a), lipoprotein (a); NLR, neutrophil to lymphocyte ratio; HR, hazard ratio; CI, confidence interval; MACE, major adverse cardiac events; CV, cardiovascular; MI, myocardial infarction; TVR, target-vessel revascularization; BMI, body mass index; PCI, percutaneous coronary intervention; CABG, coronary artery bypass grafting; TC, total cholesterol; LDL-C, low density lipoprotein cholesterol; hsCRP, high-sensitivity C-reactive protein; LVEF, left ventricular ejection fraction; LM, left main; SYNTAX, synergy between PCI with taxus and cardiac surgery; CTO, chronic total occlusion.
Subgroup Analysis
Subgroup analysis was performed to evaluate the association between risk groups and MACEs across different subgroups (age, sex, and CAD presentations). The synergistic effect of Lp(a) and NLR on clinical outcomes was more pronounced in female patients (adjusted HR, 5.93; 95%CI, 1.59–22.17; Pinteraction = 0.008). Elderly patients (age ≥65) combined with elevated Lp(a) and NLR were associated with poor clinical outcome (adjusted HR, 2.72; 95%CI, 1.34–5.52), and the interaction was borderline statistically significant (Pinteraction = 0.063). While consistent associations of risk groups with MACE risk were observed regardless of CAD presentations (Supplemental Table 2).
Discussion
In this real-world, large-scale cohort study, the prognosis of CAD patients undergoing PCI with different Lp(a) and NLR levels was evaluated. The major findings were: (1) There was an apparent interaction between Lp(a) and NLR for poor prognosis. Only in patients with high NLR levels was elevated Lp(a) associated with adverse clinical events after PCI. While in patients with low NLR levels, no significant association between Lp(a) and MACE risk was found. (2) Dual elevation in Lp(a) and NLR conferred higher risk of poor prognosis. (3) Patients with elevated Lp(a) and NLR tended to have increased lesion complexity, assessed by SYNTAX score. (4) The associations of concurrent elevations of Lp(a) and NLR with worse clinical outcomes were more pronounced in female patients. Our study supports that elevated Lp(a) was associated with a higher risk of clinical events only in CAD patients with increased levels of NLR.
Several studies had indicated a role for Lp(a) in the development of MI, stroke, and aortic valve stenosis.17–20 Recently, a patient-level meta-analysis involved 29,069 patients treated with statin, 20 indicating that elevated Lp(a) (>50 mg/dL) was an independent risk factor for ASCVD (HR, 1.47; 95%CI, 1.25–1.73) even after adjusting for established or history of CV disease, diabetes mellitus, smoking, LDL-C, and HDL-C. Li et al. also found high Lp(a) level (≥30 mg/dL) was associated with high CV risk (HR, 1.40; 95%CI, 1.05 to 1.86) in a Chinese population with stable angina pectoris. 21 However, there existed heterogeneity in the change of ASCVD risk corresponding with the increment of Lp(a) levels. A meta-analysis defended Lp(a) levels ≥50 mg/dL might reach a significant increase of ASCVD risk (approximately 47%) compared with Lp(a) levels <50 mg/dL, 20 while Puri et al., 22 reported that Lp(a) levels in 25–30 mg/dL might also associated with 42–50% increased ASCVD risk. Therefore, it was important to discriminate patients who might have higher ASCVD risk, with same level of elevated Lp(a). Systematic inflammation had been recognized as a crucial component of residual ASCVD risk. Recent randomized clinical trials (RCTs), including the Canakinumab Anti-Inflammatory Thrombosis Outcomes Study (CANTOS), 23 Colchicine Cardiovascular Outcomes Trial (COLCOT), 24 and the IL-6 inhibition with ziltivekimab in patients at high atherosclerotic risk (RESCUE) trials, 25 had demonstrated the role of anti-inflammatory treatment in the improvement of CV outcomes for patients with established ASCVD. For these patients, parallel prevalence for increased Lp(a) level (30%) 26 and proinflammatory IL-1 genotype (60%) 27 was observed.
In 1998, Dangas et al., 28 first put forward the connection between Lp(a) and inflammation in a vivo study, which observed strongest correlation between plaque KP-1 and Lp(a) area in atherectomy specimens from patients with unstable angina. Recent studies had also demonstrated the association between ASCVD risk and elevated Lp(a) might be modified by the presence of inflammation in both primary and secondary prevention.22,29 Zhang et al., 29 conducted a post hoc analysis involving 4,679 patients without established ASCVD from the Multi-Ethnic Study of Atherosclerosis (MESA) dataset. They found the combination of elevated Lp(a) (≥50 mg/dL) and hsCRP (≥2 mg/L) was independently associated with 1.62-fold ASCVD risk. Similar results were found in the sub analysis of the Assessment of Clinical Effects of Cholesteryl Ester Transfer Protein Inhibition with Evacetrapib in Patients at a High Risk for Vascular Outcomes (ACCELERATE) Trial, which involved 10,503 patients with established ASCVD, 22 suggesting that each unit increase in log Lp(a) levels was associated with a 13% increased risk of CV death, nonfatal MI, or stroke only in those with hsCRP levels of ≥2 mg/L (P = .008 for interaction). In accordance with these findings, the present study found that elevated Lp(a) levels (≥30 mg/dL) accompanied by systematic inflammation were associated with higher ASCVD risk than those without systematic inflammation. However, unlike previous hsCRP-based studies, NLR was chosen to evaluate the systematic inflammatory status in the present study. The above evidence is consistent with our findings.
Several Lp(a)-lowering pharmacological treatment methods are being developed and evaluated in going RCTs. We look forward to the evidence of those treatments in patients with different inflammatory status. 30
A primary prevention study provided evidence on the prognostic value of Lp(a) in younger patients. 31 However, limited data explored the relationship between Lp(a) concentration and elderly patients with established CAD. 32 In our study, we found elderly patients with elevated Lp(a) with elevated NLR were associated with poor clinical outcome, which showed borderline-significant interaction. Our study indicated age and systematic inflammatory status should be considered when assessing the role of Lp(a) in patients with established ACSVD.
The present study found that the synergistic effect of Lp(a) and NLR on clinical outcomes was more pronounced in female patients. In the Copenhagen General Population Study, men and women aged 20 to 49 had Lp(a) levels that were typically comparable, whereas women over 50 had an average 17% higher level. 33 While both sexes exhibit comparable relationships between high Lp(a) (>40 mg/dL) and cardiovascular morbidity and death after the age of 50, greater levels in women imply that Lp(a) is a more prevalent cardiovascular risk factor in women than in men at this age. 34 The experimental findings agreed with the fact that after menopause, when estrogen levels fall, post-menopausal women have a worse lipid profile than pre-menopausal women, have less efficient vasodilation, and reduce inflammation less effectively. 34
Currently, several CAD-related inflammatory biomarkers had been investigated. 8 Compared with other inflammatory biomarkers (i.e., hsCRP and IL-6), NLR was cheaper, simpler, and more available in clinical scenarios. Previous studies had indicated the satisfactory accuracy of NLR to reflect the degree of inflammation in patients with ASCVD.35,36 Adamstein et al., 37 conducted a post hoc analysis based on 5 RCTs, which involved 60,087 participants with or without established ASCVD. They found high baseline NLR levels (at the fourth quartile) could predict increased CV events and all-cause mortality than the low baseline NLR level (at the first quartile) in the population from CANTOS, Justification for the Use of Statins in Prevention: an Intervention Trial Evaluating Rosuvastatin (JUPITER), Studies of PCSK9 Inhibition and the Reduction of Vascular Events (SPIRE) in two separate trials (SPIRE-1 and SPIRE-2), and the Cardiovascular Inflammation Reduction Trial (CIRT). Additionally, in the CANTOS trial, 23 the NLR level decreased in a dose-dependent manner with increasing doses of canakinumab, which indicated that NLR could be used as a therapeutic target to monitor responses to anti-inflammatory treatments. Of note, in our study, we found the synergic relationship of NLR and Lp(a) with prognosis persisted even after adjustment for hsCRP, which conveyed the additional information that an elevated NLR potentially has inflammatory atherosclerotic process which is not mirrored by cytokines or hsCRP. 10
The interaction between NLR and Lp(a) might be explained by their co-proatherosclerotic and co-prothrombosis effects. Firstly, the structure of Lp(a) particle consists of a LDL-like particle and a single copy of apolipoprotein (a). 30 In the apolipoprotein (a), there are 10 subtypes of kringle domain IV (KIV), kringle domain V (KV), and an inactive protease domain (P). 38 In KIV10, there is a site often covalently attached with oxidized phospholipids. 38 Previous studies have indicated the Lp(a) kringles of could attach to fibrin and generate a quaternary complex which could impair the activation of plasminogen. 38 The oxidized phospholipids have proinflammatory role to promote atherosclerosis via immune-mediated mechanisms. 39 Secondly, neutrophilia might play a crucial role in the promoting of atherothrombosis by several mechanisms: (1) In coronary lesions, neutrophils could be observed near the plaques, especially the rupture-prone ones. 40 (2) Neutrophils could enhance the adhesion of monocyte, which might transform to foam cells and form the lipid core of vulnerable plaques. 41 Neutrophils also contribute to endothelial cell dysfunction and oxidative stress via releasing myeloperoxidase, lipoxygenases, and neutrophil extracellular traps (NETs).41,42 NETs can also promote atherothrombosis and present tissue factor at sites of infarction. 42 (3) Neutrophils could promote fibrous cap rupture by releasing of proteases that degrade matrix elements. 40 (4) Neutrophils also participate in superficial plaque erosion by promoting endothelial cell death and desquamation. 43 (5) Early massive neutrophil influx into ischemically injured myocardium can cause collateral damage and impair myocardial healing. 41 Finally, lymphopenia is caused by elevated levels of cortisol, catecholamines, and proinflammatory cytokines in stress reaction, which leads to reduced production, redistribution in tissues, or death of lymphocytes. 44 Acute lymphopenia might be associated with the poor prognosis in ST-segment elevated MI patients. 45
This study had several strengths, including a large sample size, high follow-up quality, evidence of an apparent interaction between NLR and Lp(a), and evidence of prognostic differences between Lp(a) and NLR between male and female patients. However, this study also has several limitations. First, approximately 13.5% of study patients were excluded and selection bias may exist. Second, potential confounding factors, medications at discharge, and adherence to pharmacological therapy during follow-up were not adjusted and collected due to the design of this observational study. Third, Lp(a) concentrations were inversely correlated with apo(a) isoform size. 46 This could possibly impair the accuracy of the measurement of the true Lp(a) burden due to lack of genetic characterization data and limitation of measurement methodology (by mass concentration rather than molar concentration). Fourth, data regarding Lp(a) and NLR levels were unavailable at follow-up. Future well-designed prospective studies are warranted to confirm our findings.
Conclusions
Individuals with concurrent elevations of Lp(a) and NLR have worse outcomes after PCI, suggesting that combining Lp(a) and NLR may be useful for risk stratification in this population.
Supplemental Material
Supplemental Material - The Neutrophil to Lymphocyte Ratio Modifies Lipoprotein (a)-Related Poor Prognosis in Patients After Percutaneous Coronary Intervention
Supplemental Material for The Neutrophil to Lymphocyte Ratio Modifies Lipoprotein (a)-Related Poor Prognosis in Patients After Percutaneous Coronary Intervention by Zhangyu Lin, Jining He, Chenxi Song, Rui Zhang, Sheng Yuan, Xiaohui Bian, and Kefei Dou in Angiology.
Footnotes
Acknowledgments
We thank all staff members for data collection and data analysis, who made efforts and were cooperative with each other to finish the study.
Author Contributions
All authors contributed to: (1) substantial contributions to conception and design, or acquisition of data, or analysis and interpretation of data, (2) drafting the article or revising it critically for important intellectual content, and, (3) final approval of the version to be published.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Chinese Academy of Medical Sciences Innovation Fund for Medical Sciences (CIFMS) [grant number, 2021-I2M-1-008], and the Beijing Municipal Science and Technology Project [grant number, Z211100002921009].
Data Availability Statement
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.