
Abstract
The Atherogenic Index of Plasma (AIP) is associated with coronary artery disease (CAD) and acute coronary syndrome (ACS), but the relationship between AIP and ACS in elderly patients remains unclear. We investigated the prognostic capability of AIP for in-hospital and long-term mortality in elderly patients with ACS undergoing coronary angiography (CA). We analyzed 627 patients with ACS over 75 years of age who were admitted to our clinic between April 2015 and December 2022 and underwent CA. The primary clinical endpoints were in-hospital, 30-day, 1-year, and long-term mortality. The median follow-up time was 27 months. AIP was defined as log (triglyceride/high-density lipoprotein cholesterol). In-hospital mortality rates for patients with AIP ≤.1 and AIP >.1 were 4.7% and 17.6% (P < .001), 30-day mortality rates were 8.7% and 32.2% (P = .01), 1-year mortality rates were 12.1% and 45.1% (P < .001), and long-term mortality rates were 47.3% and 67.5% (P < .001), respectively. Multivariate Cox regression analysis revealed AIP, age, left ventricle ejection fraction (LVEF), admission creatinine, and Killip ≥2 as independent predictors for long-term mortality. AIP can predict in-hospital and long-time all-cause mortality in elderly patients with ACS undergoing CA. Age, LVEF, admission creatinine, and Killip ≥2 are additional factors that predict long-term all-cause mortality.
Introduction
The average life expectancy of humankind is increasing. Various studies have revealed that approximately 20% of the population will be over the age of 65 in the near future. 1 Coronary artery disease (CAD) is one of the leading causes of mortality and morbidity in the general population. 2 The number of elderly patients presenting with acute coronary syndrome (ACS) is also increasing as the population ages. 3 Although it is well known that an increased frequency of comorbidities in the elderly may increase the severity of ACS, there are no specific recommendations for this subgroup in the current guidelines. 4 The comorbidities often include renal failure, anemia, frailty, and malignancy, and elderly patients presenting with such cases require a unique approach in daily practice. 5
ACS is a serious health problem despite the widespread use of invasive revascularization modalities along with advanced oral medications. It might result in a poor outcome despite the best medical care. 6 Models to differentiate high-risk groups of ACS with poor outcomes are designed for this purpose. Scoring systems widely used to predict clinical outcomes and determine disease severity, including the Global Registry of Acute Coronary Events (GRACE) and Thrombolysis in Myocardial Infarction risk scores are such examples.7,8 Herein, predictive modalities specific for elderly patients with ACS are needed, considering the unique risk factors and comorbidities.
The Atherogenic Index of Plasma (AIP) is related to low-density lipoprotein cholesterol (LDL-C) particle size and reflects the level of atherogenic small-dense LDL-C. AIP is calculated by the logarithm of the molar ratio of triglyceride (TG) to high-density lipoprotein cholesterol (HDL-C) level; hence, it is a simple and accessible biomarker without cost, given that only a standard lipid profile is needed for its calculation. 9 A high AIP value is a risk factor for CAD, being associated with both disease severity and the occurrence of major adverse cardiac events. 10
Although the association of AIP with CAD and ACS has been reported in several studies, the relationship between AIP and ACS in elderly patients remains unclear. In addition, elderly patients are generally underrepresented in such trials. 11 Here, we aimed to investigate the prognostic capability of AIP for in-hospital and long-term mortality among elderly patients with ACS undergoing coronary angiography (CA).
Methods
Patients and Study Design
The present study retrospectively analyzed 5273 patients who were admitted to our clinic with ACS between April 2015 and December 2022. Among these, 858 patients over 75 years of age were identified. 12 The exclusion criteria were treatment with thrombolytics, conservative management, and end-stage malignancy. The remaining 627 patients over 75 years of age who met the inclusion criteria of having CA for ACS were included in the study. Ethical board approval was obtained from the local ethics committee.
Clinical Evaluation
ACS was classified as ST-segment elevation myocardial infarction (STEMI) or non-STEMI (NSTEMI). The diagnosis of ACS was based on the Fourth Universal Definition of myocardial infarction. 13 Clinical and laboratory information was obtained from hospital records, and the data were compared between the groups according to long-term all-cause mortality. The clinical evaluation consisted of baseline demographic and clinical characteristics, including age, sex, presence of hypertension, diabetes mellitus, hypercholesterolemia, accompanying comorbidities, and stroke; previous myocardial infarction (MI), percutaneous coronary intervention (PCI), and coronary artery bypass grafting (CABG); and subgroup of ACS, Killip score, left ventricle ejection fraction (LVEF), and in-hospital medications. Laboratory data included hemoglobin, white blood cell (WBC), platelet, and admission creatinine (Cr) levels; estimated glomerular filtration rate (eGFR), admission C-reactive protein (CRP) level, hemoglobin A1c, total cholesterol, LDL-C, HDL-C, and TG levels; and AIP.
Venous blood samples were taken following 10–12 h of fasting at the time of hospital admission. Serum concentrations of the fasting lipid panel, including total cholesterol, TG, LDL-C, and HDL-C, as well as other biochemical and hematological parameter levels, were determined using standard laboratory techniques. eGFR was calculated using the Levey-modified Modification of Diet in Renal Disease formula: (186.3 × serum Cr [mg/dL]-1.154) × (age [years]-0.203) × (0.742 if female). 14 The AIP was calculated as the logarithm of the molar ratio of TG to HDL-C.
Data Analysis
Previous studies demonstrated that AIP >.1 represented intermediate and high-risk patients.15,16 In this respect, the study population was divided into two groups according to AIP values: AIP ≤.1 (n = 298) and AIP >.1 (n = 329). The primary clinical endpoints of the study were in-hospital mortality, 30-day mortality, 1-year mortality, and long-term mortality during follow-up. In-hospital mortality rates were obtained through the review of the hospital’s electronic database, whereas 30-day, 1-year, and long-term mortality rates were acquired via the national death notification system. The median follow-up time was 27 (range, 1–82) months.
Statistical Analysis
The distribution of data was evaluated using the Kolmogorov–Smirnov test. Continuous variables were compared between groups using an independent sample t-test or Mann–Whitney as appropriate, and the data are expressed as means ± standard deviation. Nonparametric values are given as median (interquartile range). Categorical data were compared using the chi-square or Fisher exact test, and the data are reported as numbers and percentages. Event-free survival curves were created using the Kaplan–Meier method. Differences in survival curves among the groups were evaluated using the log-rank test. A two-tailed P < .05 was considered statistically significant.
To assess the impact of AIP on long-term mortality at the long-term follow-up, we developed a model using the Cox regression analysis, where we included age, previous cerebrovascular disease, DM, admission Cr, admission WBC, LVEF, and admission Killip ≥2 as covariates. When building the model, covariates that were found to be statistically significant in the univariate analysis or those that were believed to have clinical significance were entered into the multivariate model. Receiver-operating characteristic (ROC) curve analysis was used to assess the sensitivity and specificity of AIP in predicting mortality. A two-sided P < .05 was considered statistically significant. Statistical analysis was performed using the SPSS 20 software (SPSS Inc., Chicago, Illinois).
Results
Baseline clinical and demographic characteristics of study group according to long-term all-cause mortality. a
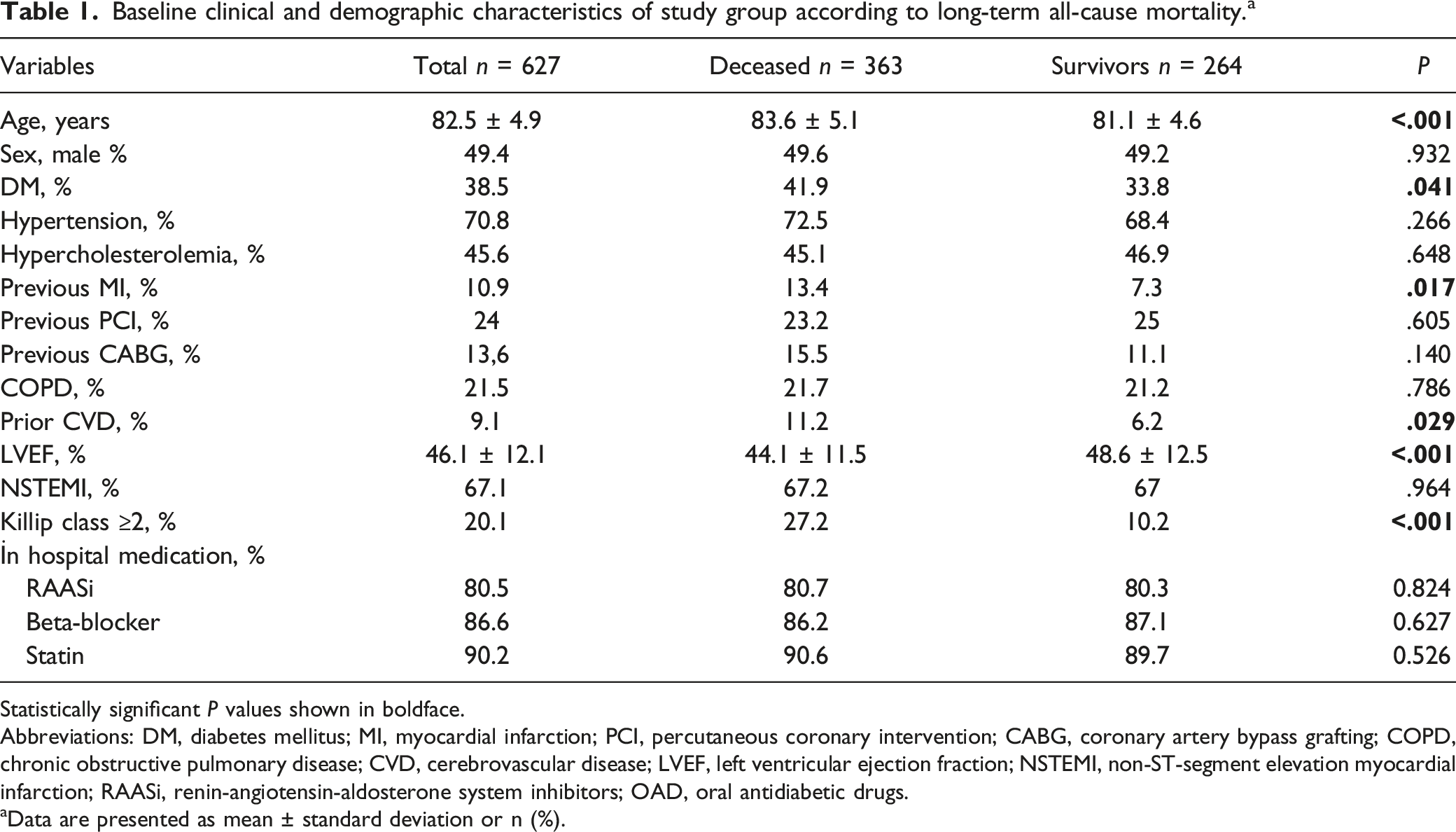
Statistically significant P values shown in boldface.
Abbreviations: DM, diabetes mellitus; MI, myocardial infarction; PCI, percutaneous coronary intervention; CABG, coronary artery bypass grafting; COPD, chronic obstructive pulmonary disease; CVD, cerebrovascular disease; LVEF, left ventricular ejection fraction; NSTEMI, non-ST-segment elevation myocardial infarction; RAASi, renin-angiotensin-aldosterone system inhibitors; OAD, oral antidiabetic drugs.
aData are presented as mean ± standard deviation or n (%).
Biochemical and hematological parameters of study group according to long-term all-cause mortality. a
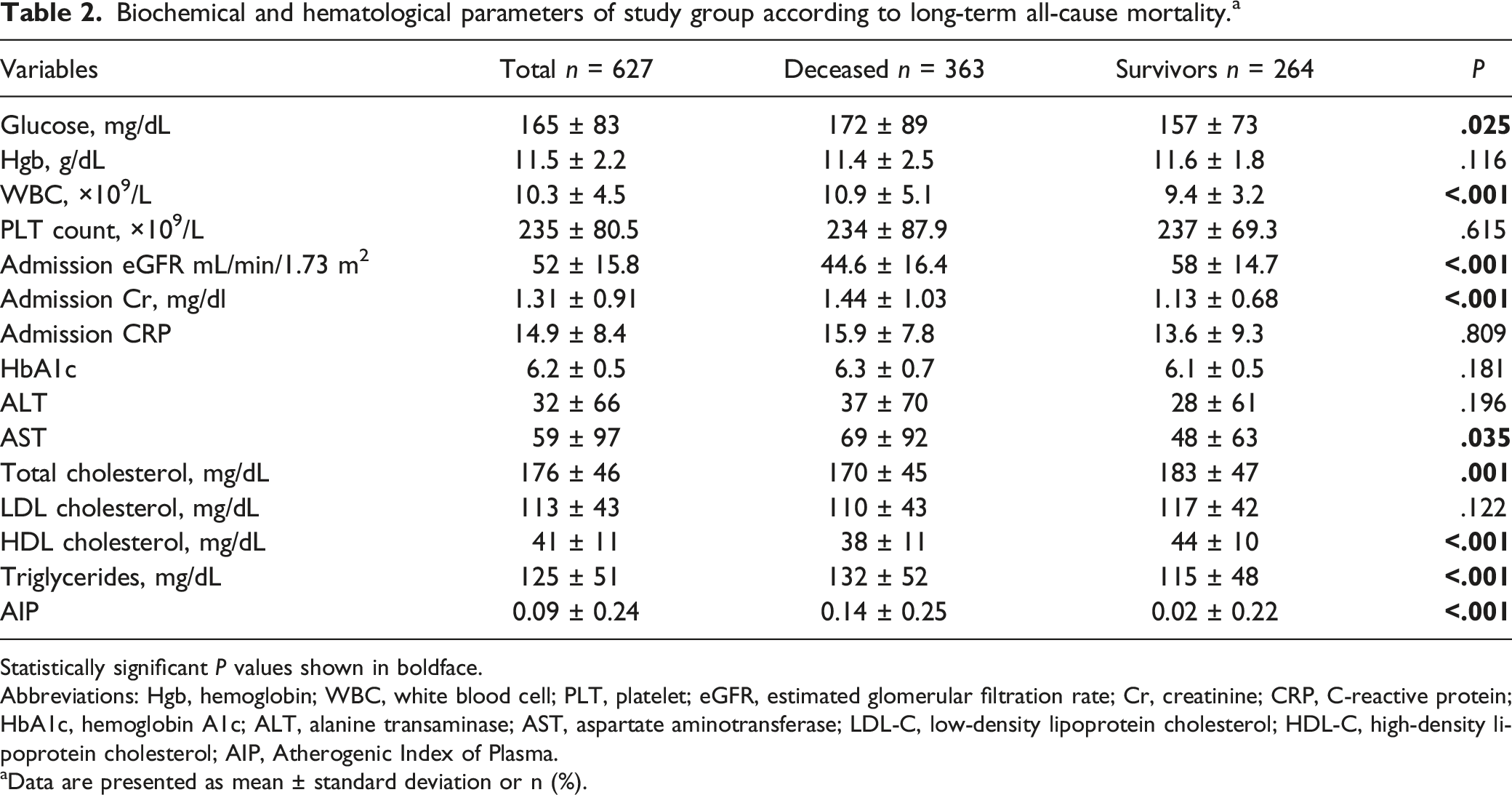
Statistically significant P values shown in boldface.
Abbreviations: Hgb, hemoglobin; WBC, white blood cell; PLT, platelet; eGFR, estimated glomerular filtration rate; Cr, creatinine; CRP, C-reactive protein; HbA1c, hemoglobin A1c; ALT, alanine transaminase; AST, aspartate aminotransferase; LDL-C, low-density lipoprotein cholesterol; HDL-C, high-density lipoprotein cholesterol; AIP, Atherogenic Index of Plasma.
aData are presented as mean ± standard deviation or n (%).
All-cause mortality rates.
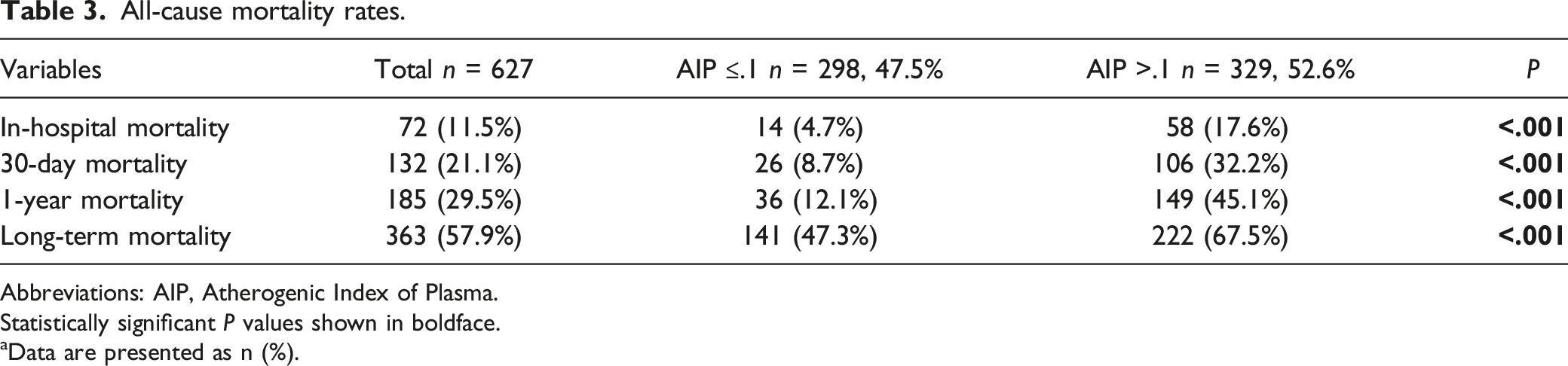
Abbreviations: AIP, Atherogenic Index of Plasma.
Statistically significant P values shown in boldface.
aData are presented as n (%).
The ROC curve for the diagnostic accuracy of AIP in long-term mortality is shown in Figure 1. The area under the curve (AUC) of AIP values for predicting long-term mortality was 0.640 (95% confidence interval [CI], 0.594–0.680; P < .001). A serum AIP value of 0.100 had 64% sensitivity and 63% specificity for predicting long-term mortality. Receiver-operating characteristic (ROC) curve analysis of Atherogenic Index of Plasma (AIP) for long-term mortality.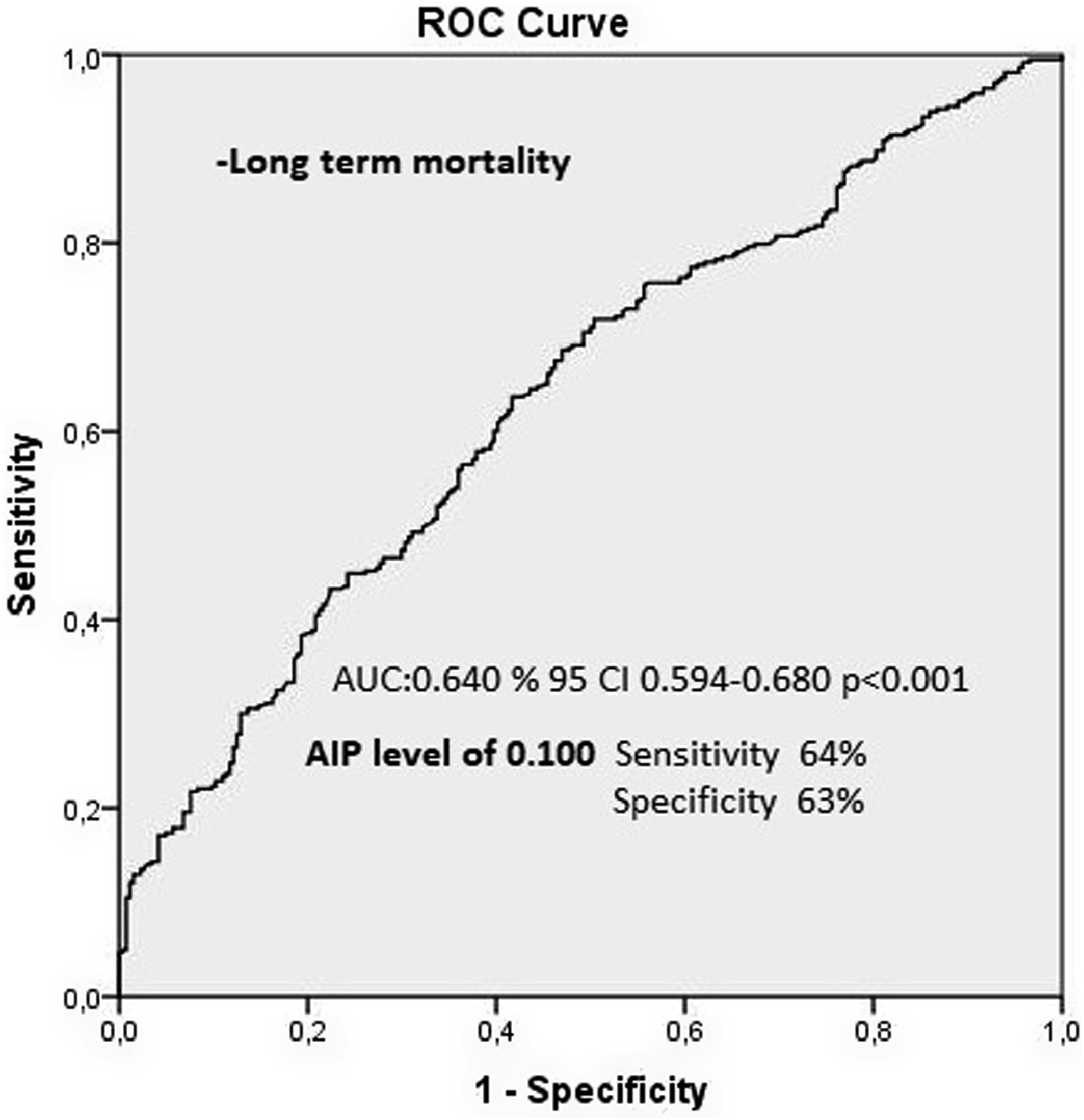
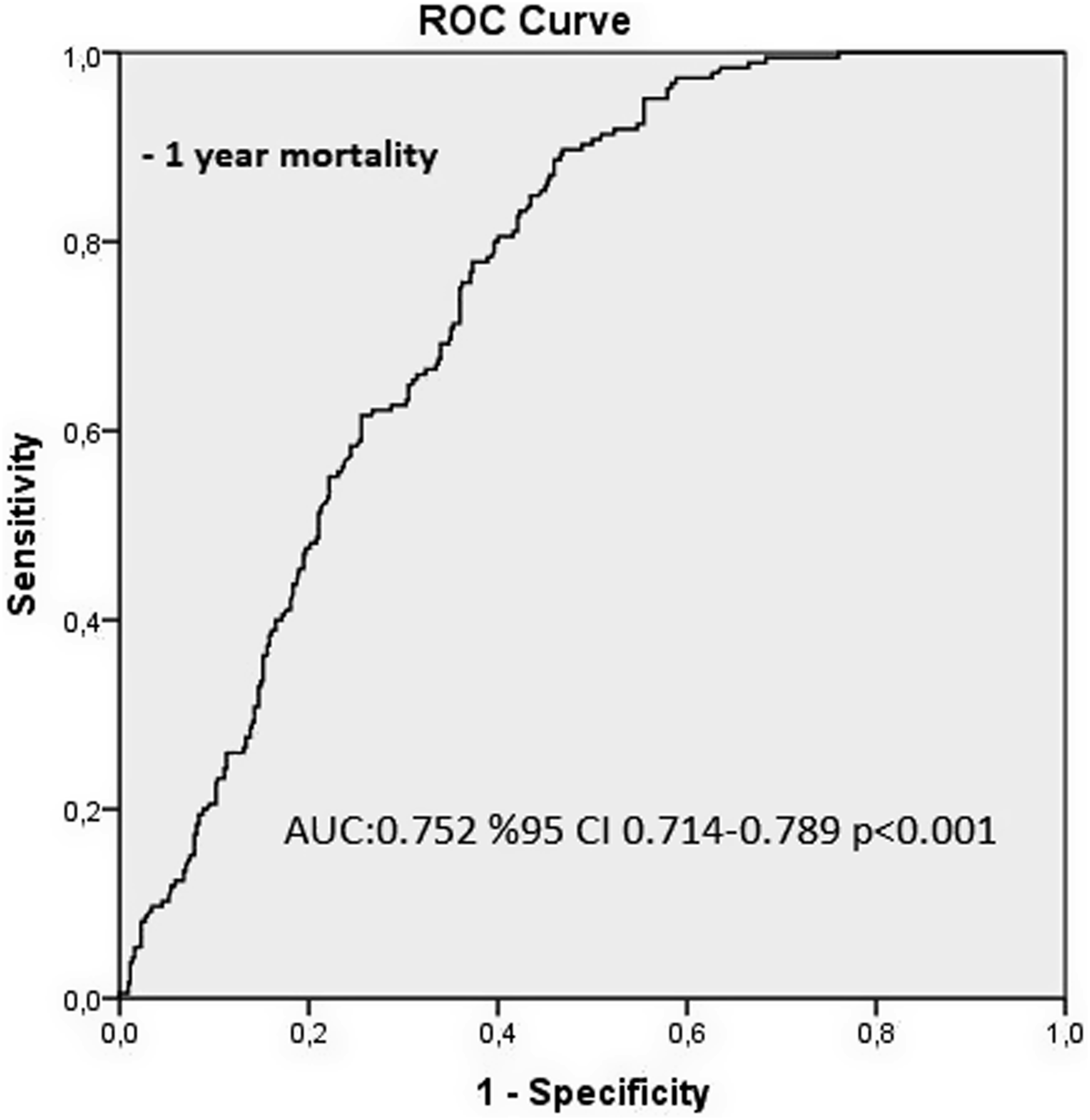
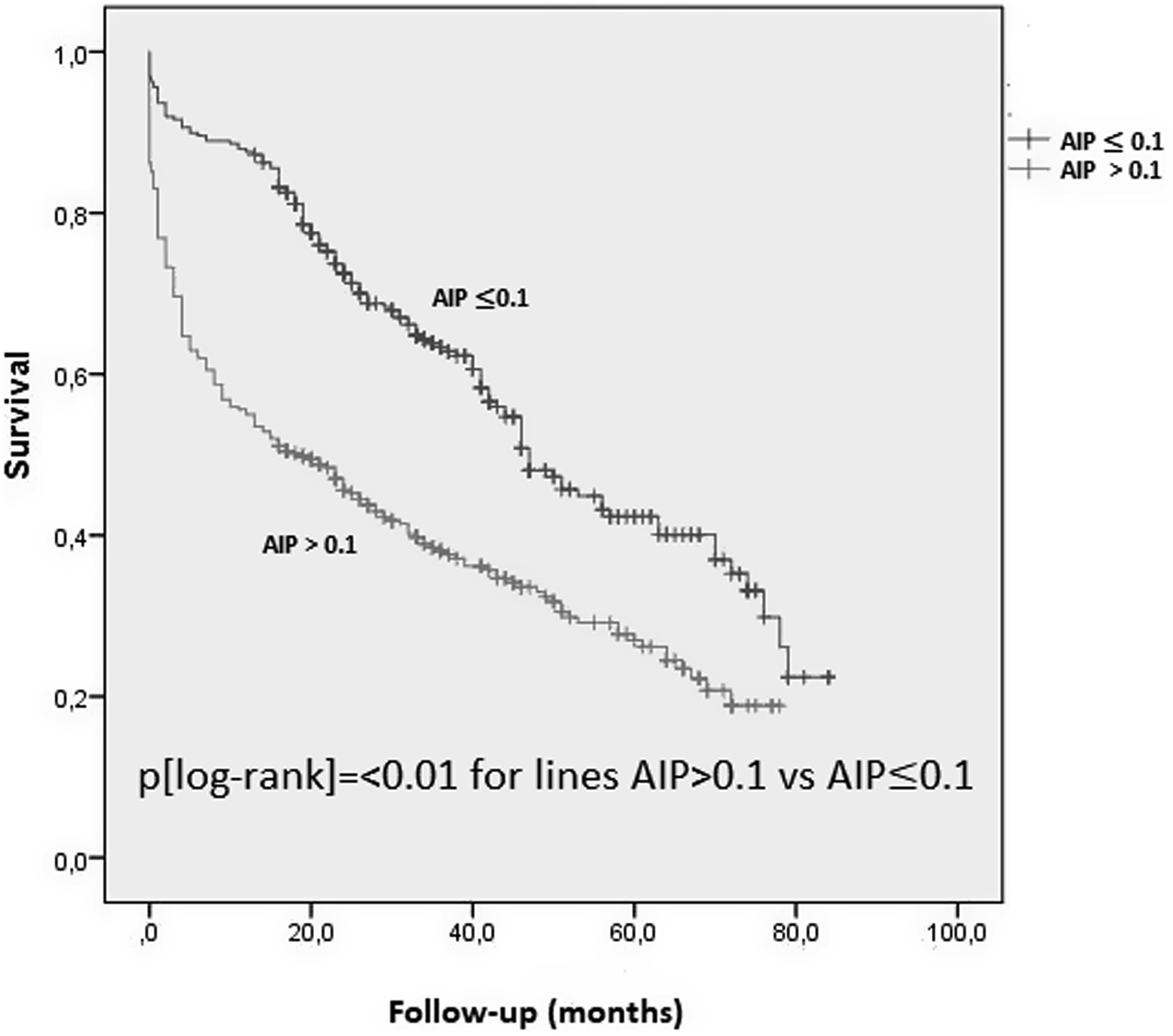
The AUC of AIP values in predicting in-hospital mortality was 0.692 (95% CI, 0.640–0.744; P < .001; Figure 2), and that in predicting 1-year mortality was 0.752 (95% CI, 0.714–0.789; P < .001; Figure 3). Kaplan–Meier analysis revealed that patients with AIP ≤.1 had higher survival rates than those with AIP >.1 (P [log-rank] = <0.01, Figure 4). Receiver-operating characteristic (ROC) curve analysis of Atherogenic Index of Plasma for in-hospital mortality. Receiver-operating characteristic (ROC) curve analysis of Atherogenic Index of Plasma for 1-year mortality. Long-term survival of elderly patients with acute coronary syndrome according to the level of Atherogenic Index of Plasma (AIP).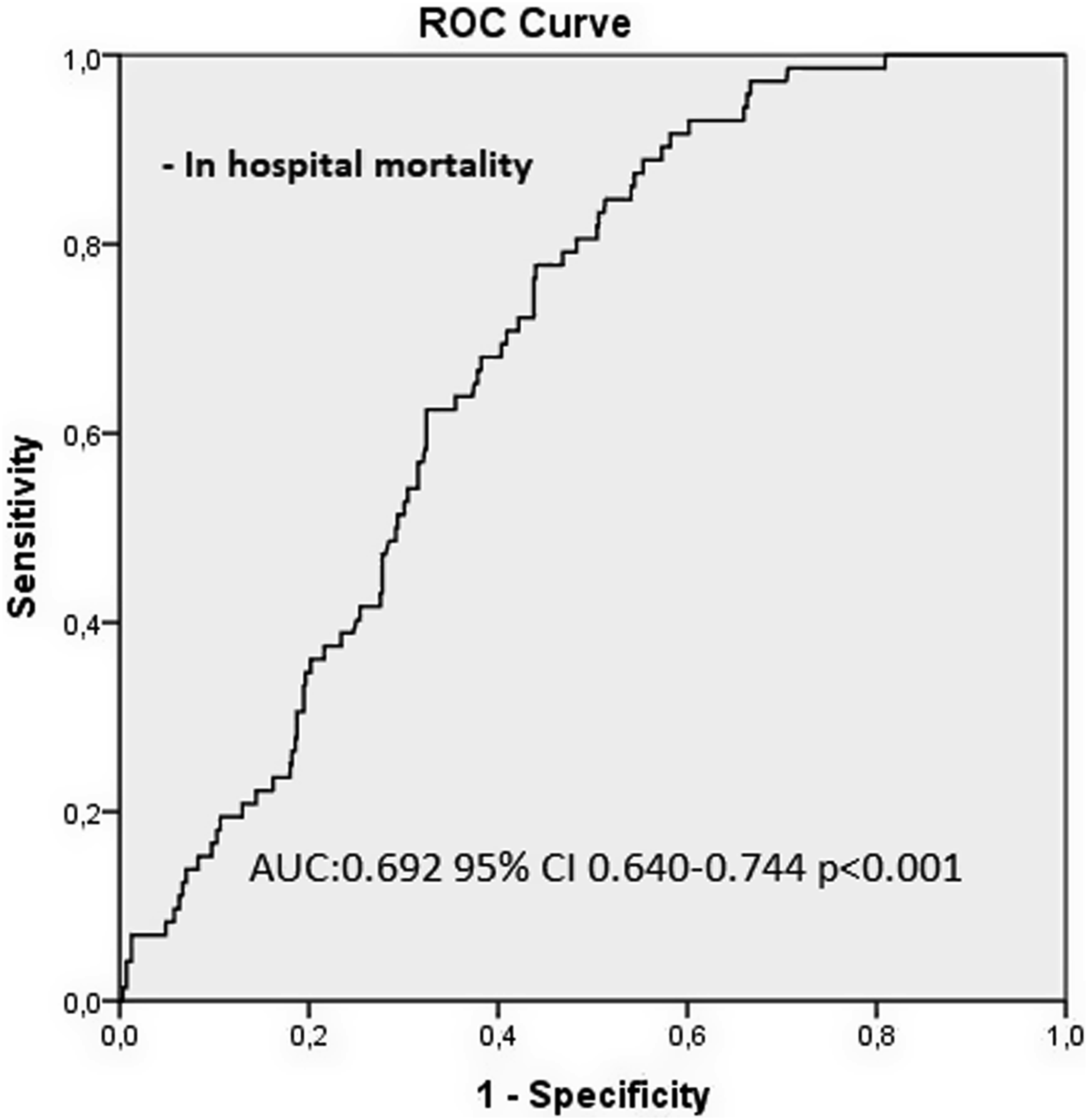
Cox regression analysis to detect the independent predictors of long-term all-cause mortality.
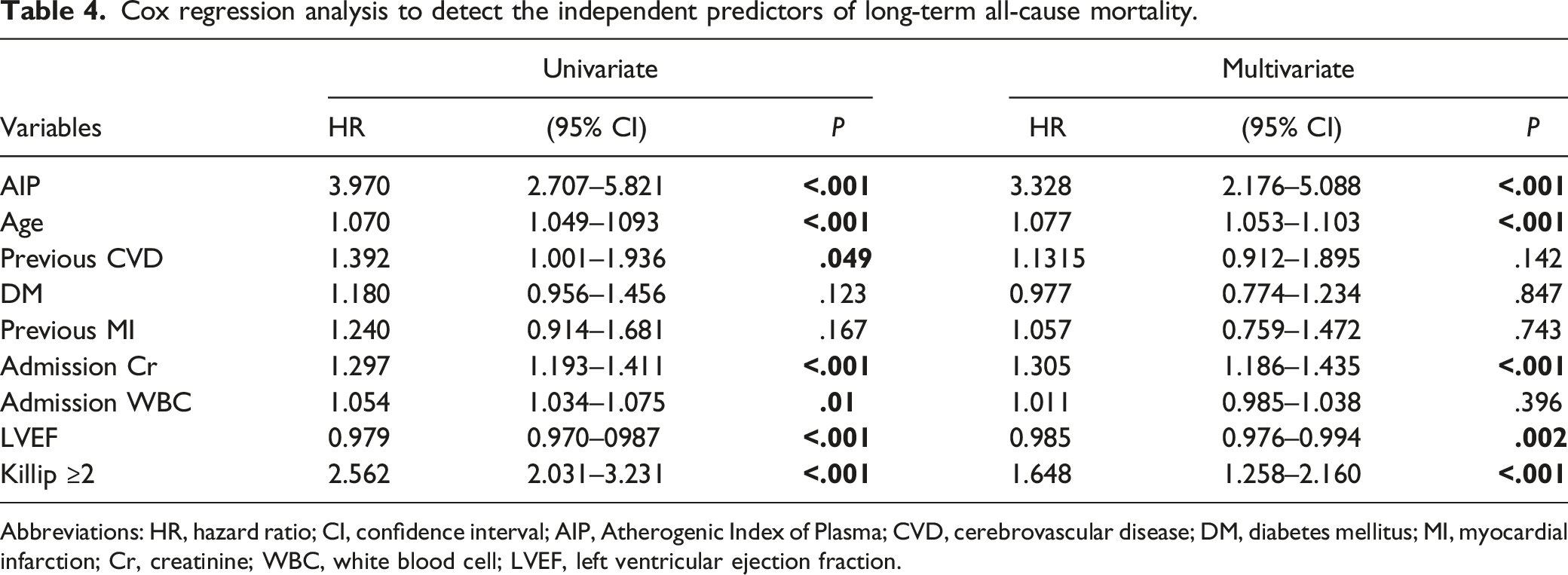
Abbreviations: HR, hazard ratio; CI, confidence interval; AIP, Atherogenic Index of Plasma; CVD, cerebrovascular disease; DM, diabetes mellitus; MI, myocardial infarction; Cr, creatinine; WBC, white blood cell; LVEF, left ventricular ejection fraction.
Discussion
This study demonstrates that long-term mortality rates are high (57.9%), and high AIP values, older age, lower LVEF, higher admission Cr, and Killip ≥2 are independent predictors of long-term mortality in elderly patients with ACS undergoing CA. Second, AIP values are positively correlated with mortality rates among different time-sets of mortality in this subgroup, and it is a reliable predictor of long-term mortality with a 64% sensitivity and 63% specificity in elderly patients.
AIP was proposed by Dobiasova et al. as a useful tool to indirectly determine the level of oxidized small-dense LDL-C, which has a significant impact on the formation of atherosclerotic plaques. 17 In addition, studies have shown that elevated AIP values are correlated with other risk factors in the pathogenesis of atherogenic cardiovascular disease, including diabetes, hypertension, abdominal obesity, and physical inactivity.18,19 Therefore, AIP reflects metabolic impairment more comprehensively than a singular parameter such as LDL-C due to its association with traditional cardiovascular disease risk factors. However, AIP failed to correlate with the aforementioned diseases in patients >65 years of age, leaving the role of AIP in elderly patients with ACS obscure. 18 Elevated AIP values are determined to be an independent risk factor for CAD, in addition to traditional risk factors. 18 High AIP values were found to correlate with the severity of CAD. 20 Moreover, Wu et al. demonstrated a relationship between AIP and the accelerated progression of CAD that was independent of conventional risk factors. This study demonstrated that accelerated progression of plaque is more prevalent at higher AIP values. 21 In a separate study conducted by Fernández-Macas et al., it was determined that elevated AIP values have a strong predictive value for CAD. 22 However, elderly patients >75 years of age were not included in those studies.
In a meta-analysis by Wu et al., it was determined that elevated AIP values have a prognostic value for CAD. 23 In addition, according to a study by Sadeghi et al., elevated AIP values are associated with recurrent cardiovascular events. This study also demonstrated that recurrent cardiovascular events increased patient mortality over a 15-year follow-up period. 24 In addition, when Cai et al. examined patients with ACS under 35 years of age in a separate study, they discovered that elevated AIP values indicate the severity of clinical processes and CAD more accurately than LDL-C. 25 In a study by Tamosiunas et al., it was determined that elevated AIP values were associated with all-cause mortality in people aged 45–72. 26 However, there is no long-term study demonstrating the association between AIP and all-cause mortality in patients older than 75. The present study demonstrated that long-term mortality rates are high (57.9%) in elderly patients with ACS undergoing CA, and AIP value >.1 is an independent predictor of long-term mortality, supporting its role in the elderly.
In a study conducted in the general population, within 10 years of follow-up, high AIP values were associated with increased rates of all-cause mortality in female patients >60 years old. 27 This sex disparity was explained by the significantly higher prevalence of comorbid diseases such as diabetes and prior MI in male patients. In contrast, while the prevalence of comorbid factors was comparable between the sexes in our cohort, our study found that elevated AIP values were predictive of mortality both in male and female patients. In addition, this study targeted the general population rather than those with ACS, unlike our investigation. In a study by Drwila et al., AIP values in NSTEMI patients older than 60 years were not found to be predictive of major adverse cardiovascular events and all-cause mortality at 1-year follow-up. 28 This result contradicts ours, as our patient cohort included both STEMI and NSTEMI patients, albeit with an extended follow-up period. In the study by Drwila et al., only 1-year follow-up results were available; in-hospital and 1-month outcomes for all-cause mortality were unavailable. Patients with a high AIP value at admission were at a clear survival disadvantage during the follow-up period of the present study. Nonetheless, significant increases in mortality among individuals with high AIP values at the beginning of the study decreased progressively over the course of the follow-up. This result is plausible in that, regardless of the initial ratio of AIP, a number of other factors can cause death.
Increased duration of each PCI and the amount of contrast agent used, increased risk of contrast nephropathy, and bleeding may accompany elderly patients with ACS. 29 Accordingly, Keskin et al. demonstrated in a separate study that acute renal failure and bleeding are two of the leading causes of in-hospital mortality among elderly patients. 29 These obstacles demonstrate that, despite the current treatment guidelines being valid for elderly patients, they are treated inadequately. 30 Personalization of treatment is one of the most effective methods to overcome these treatment obstacles.
We acknowledge certain limitations of our study. It was a retrospective, single-center, sampled investigation with a relatively small sample size. Consequently, our results may not be representative of the general population, as the levels of these variables may vary by ethnicity. Also, the retrospective design of the study may have introduced selection bias. In addition, frailty could not be evaluated as functional and psychosocial parameters were not available. Although we assessed all-cause mortality as an endpoint, major adverse cardiac events were not evaluated separately.
In conclusion, the results of our study demonstrate that AIP is an independent predictor of in-hospital and long-time all-cause mortality in elderly patients with ACS undergoing CA. Age, LVEF, admission Cr, and Killip ≥2 are additional factors that predict long-term all-cause mortality. In addition, the use of these easily calculated prognostic biomarkers may enable early risk stratification in elderly ACS patients. Consequently, their extensive use in daily clinical practice may reduce the risk of subsequent adverse events.
Footnotes
Author Contributions
Özgür Selim Ser, Kudret Keskin, and Gökhan Çetinkal contributed to the acquisition of data, the analysis and interpretation of data, revising the manuscript critically for important intellectual content, and the final approval of the version to be published. Tümay Celbiş Geçit, Furkan Dolap, Cüneyt Koçaş, and Hakan Kilci contributed to the acquisition of data, the analysis and interpretation of data, the drafting of the article, and the final approval of the version to be published. Betül Balaban Koçaş, Erol Kalender, and Kadriye Kılıçkesmez made substantial contributions to conception and design, drafting the article, and final approval of the version to be published.
Author’s Note
This manuscript has not been published or presented elsewhere in part or in entirety and is not under consideration by another journal.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.