
Abstract
Contrast-induced nephropathy (CIN) poses a significant risk following primary percutaneous coronary intervention (pPCI) in patients with ST-Elevation Myocardial Infarction (STEMI). Magnesium (Mg²⁺) deficiency has been associated with renal dysfunction and cardiovascular diseases, yet its role in CIN development remains unclear. This study represents the first investigation exploring the relationship between Mg²⁺ levels and CIN in this context.
We conducted a retrospective study involving 2306 consecutive STEMI patients undergoing pPCI. Serum Mg²⁺ levels were measured on admission. Logistic regression and Receiver Operating Characteristic (ROC) analysis were employed to assess the association between Mg²⁺ levels and CIN development. Of the enrolled patients, 691 (30%) developed CIN post-pPCI. Mg²⁺ levels were significantly lower in the CIN group (P < .001). Multivariate analysis identified Mg²⁺ <2.03 mg/dL, age >68 years, left ventricular Ejection Fraction (EF) <49%, and post-procedure Thrombolysis In Myocardial Infarction (TIMI) flow grade <2 as independent predictors of CIN. ROC analysis revealed an Mg²⁺ cutoff of 2.03 mg/dL, Area Under the Curve (AUC): 0.711, sensitivity: 69%, specificity: 68%). Our study demonstrates a significant correlation between low Mg²⁺ levels and CIN in STEMI patients undergoing pPCI, highlighting Mg²⁺ <2.03 mg/dL as an independent risk factor for CIN.
Keywords
Introduction
The primary method for enhancing survival rates in individuals with ST-elevation myocardial infarction (STEMI) is prompt primary percutaneous coronary intervention (pPCI). Nevertheless, this strategy poses a potential danger of causing contrast-induced nephropathy (CIN). Even though PCI is the main treatment for STEMI patients, around 15%–35% of individuals might experience CIN after undergoing the procedure. 1 CIN is becoming a more prevalent cause of iatrogenic acute kidney injury, leading to greater utilization of healthcare resources due to prolonged hospital stays, heightened short- and long-term mortality rates, and hastened progression of pre-existing chronic kidney disease. 2 Furthermore, CIN, regardless of its severity, has been associated with an increased long-term risk of major adverse cardiovascular events (MACE), extending its impact beyond renal outcomes. 3
The term CIN is also commonly referred to as “Contrast-induced Acute Kidney Injury (CI-AKI).” 4 The most commonly used definition of CIN in clinical trials involves an increase in serum creatinine of 0.5 mg/dL (44 µmol/L), or a 25% elevation from the initial level, occurring within 48-72 h following the procedure. 5 However, alternative descriptions have been proposed to clarify the term CI-AKI. According to the European Renal Best Practice (ERBP) position statement on the Kidney Disease Improving Global Outcomes (KDIGO) guidelines, CI-AKI is defined as a rise of over 50% from the baseline within 7 days post-contrast exposure, or an increase of more than 0.3 mg/dL (26.5 µmol/L) from baseline within 48 h post-contrast exposure. 6
CIN typically ranges from 0.6% to 2.3% in the general population, but its prevalence significantly increases in certain patient subsets, notably those with cardiovascular conditions. 7 In a registry of 7586 patients undergoing interventional cardiology procedures, the incidence of CIN was 3.3%, with 0.7% requiring dialysis due to CIN. 8 Notably, the risk of CIN escalates dramatically, reaching 19%, particularly in the context of pPCI for acute myocardial infarction. 9
Magnesium (Mg²⁺), the second most abundant cation, is indispensable for cellular function, playing a vital role in numerous physiological processes across all cell types. 10 It serves as a cofactor in numerous enzymatic reactions, encompassing energy metabolism, DNA and protein synthesis and plays a pivotal role in regulating ion channels. 11 Prior studies have indicated that Mg²⁺ hampers the differentiation of inflammatory cells, diminishes the synthesis of inflammatory cytokines, lessens inflammation, and diminishes the generation of reactive oxygen species and oxidative stress. 12 These effects indicate that deficiencies in Mg²⁺ have been associated with several diseases, including hypertension, atherosclerosis, dyslipidemia, insulin resistance, metabolic syndrome, osteoporosis, and neuropsychiatric disorders, as well as increased mortality rates. 13 Adding that studies have shown a close relationship between Mg²⁺ levels and renal function. Numerous pieces of evidence highlight magnesium’s involvement in preventing or reversing renal damage following the therapeutic use of contrast agents and other nephrotoxic drugs commonly employed in clinical practice. 14
Drawing upon the aforementioned data, our objective was to examine the correlation between the occurrence of CIN and Mg²⁺ levels among patients subjected to pPCI for STEMI.
Methods
Study Population
We enrolled 2306 consecutive patients admitted to our coronary care unit for STEMI patients with symptoms (characteristic chest pain lasting for at least 30 min, not responsive to nitrates, with electrocardiographic ST-segment elevation of at least 0.2 mV in two or more contiguous leads, or left bundle branch block) who were treated with pPCI. Our study population excluded patients with severe valvular heart disease, congestive heart failure with an ejection fraction <40%, who have had coronary artery bypass grafting (CABG) surgery, chronic kidney disease with an estimated glomerular filtration rate (eGFR) below 60 mL/min/1.73 m², recent intravenous contrast administration within the previous 10 days, and a diagnosed metabolic disorder impacting serum Mg²⁺ levels. Individuals who experienced cardiogenic shock either upon admission or during subsequent monitoring, as well as those who suffered severe hypotension necessitating inotropic support, were not included in the research. The patients were categorized into two groups based on the occurrence of CIN.
The research received authorization from the Ethical Committee of Turkey, with approval number 2013/KK/98, and adhered to the principles outlined in the Helsinki Declaration during its execution.
Biochemical Analysis
Before coronary angiography, venous blood samples were obtained from an antecubital vein upon admission for hematologic and biochemical evaluations. A Roche Diagnostics Cobas 8000 c502 analyzer (Roche Diagnostics, Indianapolis, USA) was used to perform the biochemical assays. Over the course of 72 h after PCI, creatinine levels were monitored to track the development of CIN.
Primary PCI (pPCI)
Every procedure involving pPCI was carried out after aspirin and a P2Y12 antagonist, which was selected according to the operator’s discretion. The percutaneous femoral approach was used to do coronary angiography. At the time of the initial assessment of coronary anatomy, 100 U/kg of heparin was delivered. For every procedure, a contrast agent containing iohexol (Omnipaque, GE Healthcare, Cork, Ireland) was used.
Definitions
In the study, CIN was defined as either an elevation in serum creatinine of 0.5 mg/dL (44 µmol/L) or a 25% increase from the baseline level, occurring within 48–72 h after the procedure. 5 The Modification of Diet in Renal Disease research equation was used to compute eGFR. 15 Blood pressure higher than 140/90 mmHg was considered hypertension, as was the use of antihypertensive medications. Further criteria for diabetes mellitus (DM) included fasting blood glucose levels greater than 126 mg/dL or the use of insulin or oral anti-diabetic medications.
Statistical Analysis
The results were reported as the mean ± standard deviation for data that followed a normal distribution, as the median with the interquartile range (IQR) for data that did not follow a normal distribution, and as a percentage for categorical data. The Kolmogorov–Smirnov test for normalcy was used to ascertain the distribution pattern. The continuous variables were compared between the two groups using independent-samples t tests, the chi-square test was used to compare categorical data. The study utilized binary logistic regression analysis to compute the odds ratio (ORs) and 95% confidence intervals (CIs) in order to evaluate the influence of various factors on the development of CIN. The univariate regression model was used to evaluate possible confounding variables, and any confounders with a P-value below .1 were included in the multivariate analysis. The Hosmer-Lemeshow test was employed as a statistical tool to assess the goodness of fit and calibration in logistic regression models. Receiver operating characteristic (ROC) curve analysis was employed to calculate the area under the curve (AUC) and identify the appropriate cutoff value for Mg²⁺ in predicting the occurrence of CIN using the Youden index. A variable with a P-value less than .05, without any adjustments, was deemed statistically significant. The data underwent analysis utilizing SPSS 22 software package (SPSS Inc., Chicago, IL, USA).
Results
In the study, the average age of the 2306 patients enrolled was 56.7 ± 11.9 years; 1897 (83%) were male. The prevalence of diabetes mellitus (DM), hypertension (HT), and hyperlipidemia (HL) was 26%, 44%, and 38%, respectively. A total of 8% of participants had a history of prior PCI. CIN was diagnosed in 691 (30%) patients within 48–72 h post-pPCI. Patients who developed CIN tended to be older and had higher rates of DM, HT, and Killip score >2 were more frequently observed upon admission. An important finding was the significant difference in Mg²⁺ levels between groups; notably lower in patients who developed CIN (P < .001). Other laboratory findings indicated elevated glucose and leukocyte levels. Additionally, coronary procedures revealed larger stent sizes, slower TIMI flows, higher incidence of proximal lesions, and increased use of contrast among patients who developed CIN. The demographic data, medication records, laboratory results, and coronary angiography details of the patients are presented in Table 1, segregated by groups.
Baseline Clinical and Procedural Characteristics of the Study Patients.
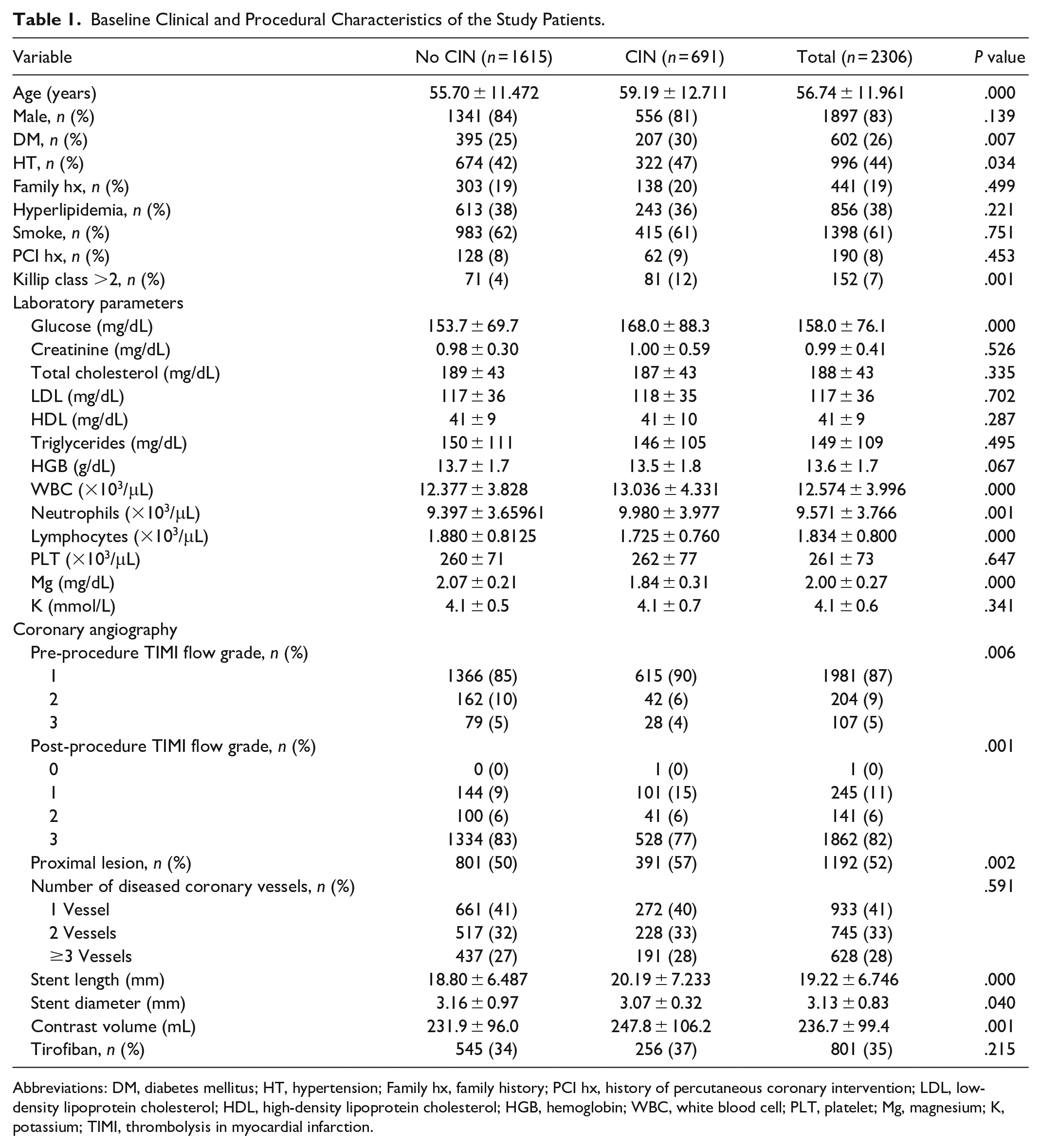
Abbreviations: DM, diabetes mellitus; HT, hypertension; Family hx, family history; PCI hx, history of percutaneous coronary intervention; LDL, low-density lipoprotein cholesterol; HDL, high-density lipoprotein cholesterol; HGB, hemoglobin; WBC, white blood cell; PLT, platelet; Mg, magnesium; K, potassium; TIMI, thrombolysis in myocardial infarction.
It was found that there was a notably higher occurrence of in-hospital complications in the group that experienced CIN. Cardiac death, MACE, recurrent myocardial infarction, stroke, revascularization procedures, and arrhythmic events were more frequent in the CIN-developing group (P < .001). A total of 19 patients required hemodialysis, 16 of whom were in the CIN group. In the remaining three patients, dialysis was due to acute tubular necrosis caused by hemodynamic instability and high-dose aminoglycoside exposure, developing after 72 h post-PCI, suggesting a non-CIN origin. There was no disparity observed between the two groups regarding the length of hospital stay. The distribution of in-hospital events across the groups is detailed in Table 2.
In-Hospital Clinical Complications.
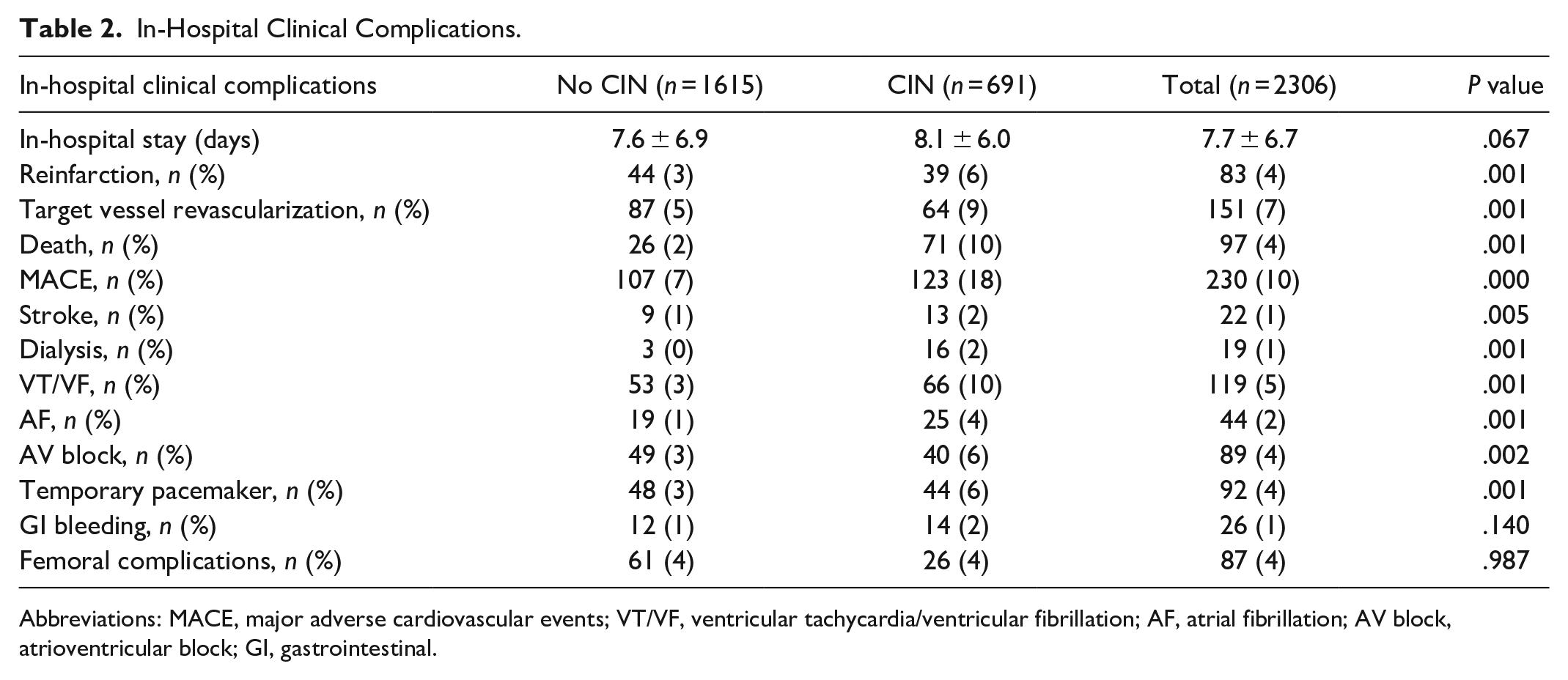
Abbreviations: MACE, major adverse cardiovascular events; VT/VF, ventricular tachycardia/ventricular fibrillation; AF, atrial fibrillation; AV block, atrioventricular block; GI, gastrointestinal.
Univariate regression analysis was conducted to identify factors associated with CIN. The analysis included parameters that were statistically significant between the groups, as well as risk factors documented in the literature. Variables with P-values below .1 in the univariate analysis were included in the multivariate analysis. Mg²⁺ <2.03 mg/dL (OR = 3.634; CI = 2.761–4.785), Age > 68 years (OR = 1.06; CI = 1.00–1.024; P = .048), Ejection fraction (EF) <49% (OR = 0.985; CI = 0.972–0.998; P = .028), and post-procedure TIMI flow grade <2 (OR = 0.585; CI = 0.391–0.877; P = .009) were identified as independent variables. (Table 3) (Multivariate logistic regression analysis statistical values; Hosmer–Lemeshow test: 18.021; −2 Log likelihood: 2550.391; Nagelkerke R2: 0.116; P = .021). The threshold values for the parameters considered in the analysis were determined using ROC analysis and the Youden index. By including the Mg²⁺ value in the model alongside the independent variables, the percentage of correct prediction value of the model was observed to rise from 68.3% to 73.9%.
Univariate and Multivariate Logistic Regression Analysis for Contrast-Induced Nephropathy.
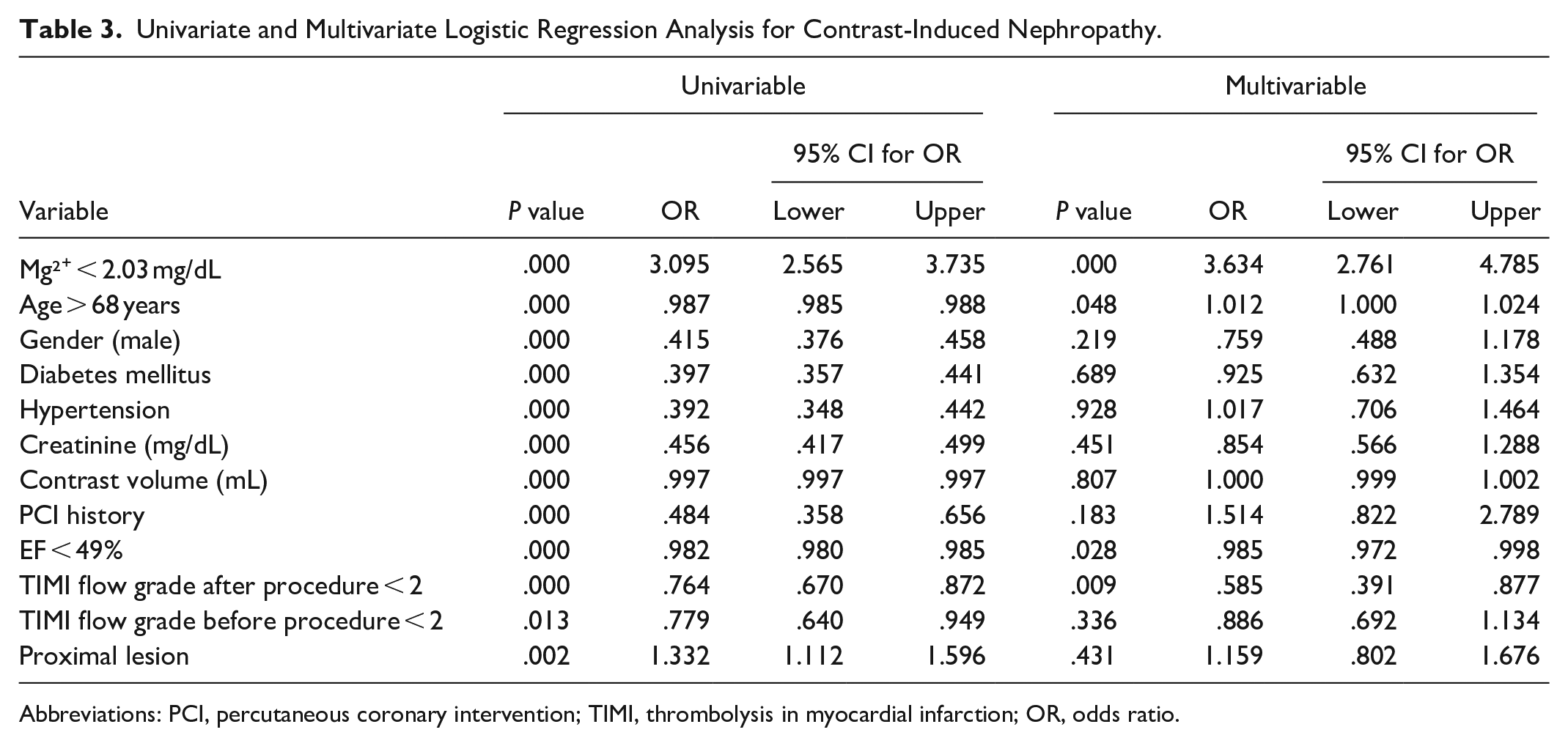
Abbreviations: PCI, percutaneous coronary intervention; TIMI, thrombolysis in myocardial infarction; OR, odds ratio.
ROC analysis was conducted to determine the Area Under the Curve (AUC) for the Mg²⁺ value in predicting CIN. An Mg²⁺ value of 2.03 mg/dL was established as a significant cutoff point for CIN prediction (AUC = 0.711, CI = 0.687–0.735, P = .001), exhibiting a sensitivity of 69% and a specificity of 68% (Figure 1). In the ROC analysis, a Mg²⁺ level <2.03 mg/dL was identified as a superior predictor compared with other independent predictors. Specifically, the AUC values for age, EF, and TIMI flow grade were found to be 0.581, 0.564, and 0.531, respectively.
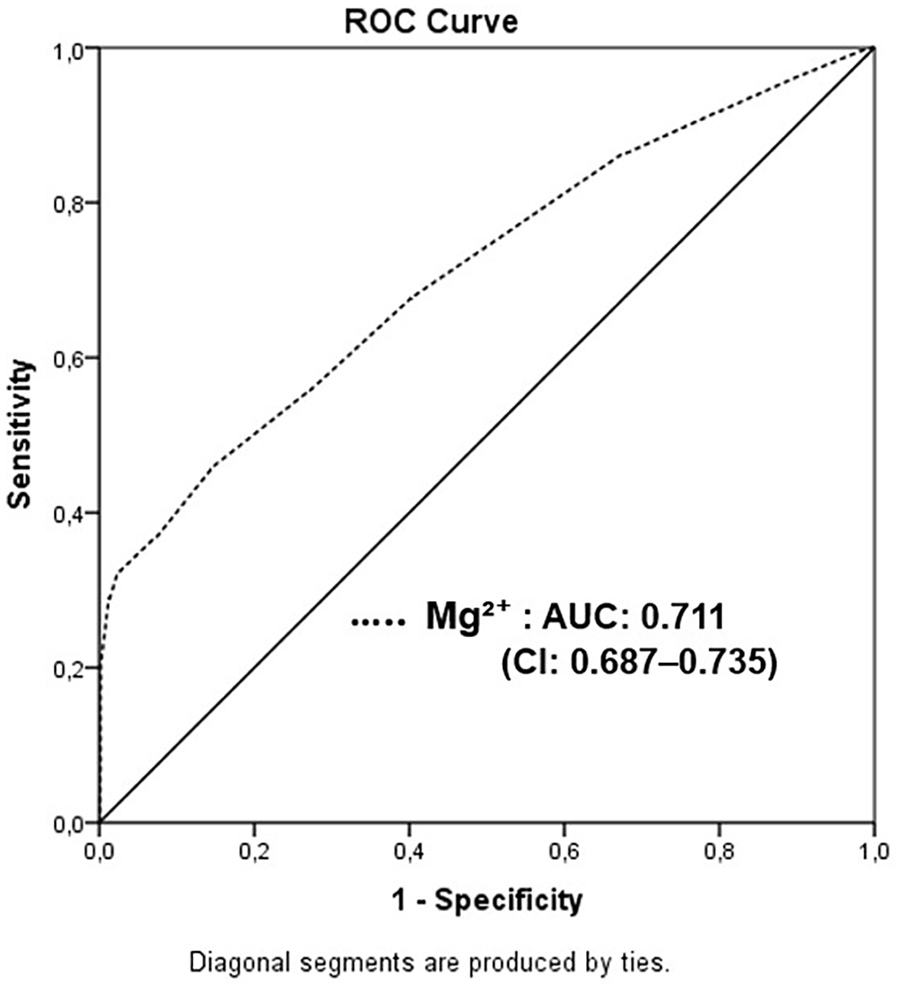
Receiver operating characteristic (ROC) analysis to evaluate the predictive capability of magnesium levels in forecasting contrast-induced nephropathy.
Discussion
In this study, we identified a correlation between decreased Mg²⁺ levels and the development of CIN in STEMI patients who underwent pPCI, and Mg²⁺ emerged as one of the independent risk factors predicting CIN. Additionally, we determined the cutoff value for Mg²⁺ levels that predicts the development of CIN. To the best of our knowledge, our study holds significance as it marks the first investigation in the literature to explore the impact of Mg²⁺ levels on the development of CIN in STEMI patients.
CIN is a potential complication arising from coronary diagnostic and interventional procedures. Its occurrence has been linked to heightened in-hospital and long-term morbidity and mortality rates, prolonged hospital stays, and lasting renal dysfunction. 16 Various risk factors contribute to its development, including chronic renal insufficiency, diabetes mellitus, congestive heart failure, intravascular volume depletion, and the administration of significant quantities of contrast agent. 17
The pathophysiology of CIN is intricate and not fully understood. Multiple mechanisms work together to induce CIN, with intrarenal vasoconstriction, the generation of reactive oxygen species, and direct tubular damage being the primary factors involved. 18 Another contributor to CIN development is the immediate vasoconstriction and reduction in renal blood flow following the administration of contrast medium. 19 Numerous studies in animal models have demonstrated that intra-arterial infusion of ionic contrast medium leads to a transient initial increase in blood flow followed by a significant and prolonged constriction of the renal vasculature. 20
Patients diagnosed with STEMI who undergo pPCI may constitute a population at a heightened risk for CIN compared with those undergoing elective PCI procedures. Several factors may contribute to renal injury in this scenario. Notably, hypotension or shock, the administration of a large volume of contrast media, and the inability to initiate renal prophylactic therapy are among the primary factors likely to be involved. 9 Renal insufficiency combined with acute myocardial infarction represents a high-risk combination. A study revealed that among acute myocardial infarction patients, the in-hospital mortality rates were 2% in individuals with normal renal function, but significantly higher at 30% in those with end-stage renal disease (P < .001). 21 In a meta-analysis investigating factors predicting the development of CIN in STEMI patients, it was found that the overall incidence of CIN in patients undergoing PCI was not low and was closely associated with hypertension, diabetes mellitus, history of prior myocardial infarction, age, damaged left anterior descending artery, Killip class >2, lower estimated glomerular filtration rate, and left ventricular ejection fraction <40%. 22
Mg²⁺ is a crucial cation found abundantly in organisms, playing roles in various physiological processes such as enzymatic reactions and structural functions within membranes. The largest reservoir of magnesium is in bone (60%–65%), which helps buffer changes in magnesium levels. 14 Studies suggest that magnesium possesses anti-inflammatory properties, as it can inhibit macrophage activation and reduce the production of inflammatory cytokines like IL-1ß, IL-6, and IL-10. 23 Hypomagnesemia, or low magnesium levels, is a significant pathogenic factor associated with increased oxidative stress. 13 This condition enhances oxidation, leading to the production of reactive oxygen species, elevated circulating lipid and lipoprotein levels in uremic patients, and increased lipid peroxidation, which can result in cytotoxicity and DNA damage in endothelial cells. 24
Numerous studies have linked Mg²⁺ deficiency with adverse cardiovascular outcomes, with evidence suggesting that exacerbated oxidative stress is one of the mechanisms contributing to these harmful effects. Magnesium exhibits vasodilatory, anti-inflammatory, anti-ischemic, and antiarrhythmic properties, making it a potentially valuable therapeutic agent in cardiovascular medicine. 14 Recent studies suggest that low serum Mg²⁺ levels may increase the risk of cardiovascular disease. Conversely, higher Mg²⁺ intake and elevated serum Mg²⁺ levels have been associated with a reduced risk of fatal coronary heart disease. 25 Elevated plasma Mg²⁺ levels were linked to a 29% reduction in the risk of all-cause mortality and also a prospective study indicates that adults at high risk of cardiovascular disease who consumed the highest levels of Mg²⁺ experienced a 37% decrease in the risk of all-cause mortality.26,27 In a meta-analysis, Mg²⁺ levels were associated with a 22% decrease in the risk of heart failure and a 7% decrease in the risk of stroke, diabetes, and all-cause mortality. 28 Another study revealed that serum Mg²⁺ levels are independently associated with the risk of acute stent thrombosis in patients with STEMI who undergo pPCI. 29
Multiple pieces of evidence suggest that Mg²⁺ plays a role in preventing or reversing renal damage caused by nephrotoxic agents commonly used in clinical practice. Administration of Mg²⁺ supplementation, either alone or combined with potassium, has been demonstrated to protect against nephrotoxicity induced by medications like cyclosporine. 30 Additionally, in another study, acute markers of kidney damage improved following Mg²⁺ replacement when administered alongside cisplatin. 31 Furthermore, low Mg²⁺ levels have been linked to a heightened risk of incident CKD in a population of individuals with an eGFR higher than 60 mL/min/1.73 m2. 32 In diabetic nephropathy, low plasma Mg²⁺ levels have been correlated with a faster decline in renal function and with progression to end-stage renal disease. 33 The mechanism by which Mg²⁺ levels affect renal damage involves Mg²⁺ preventing the downregulation of renal the transient receptor potential subfamily Melastatin 6 (TRPM6) and inhibiting the organic cation transporter 2 (Oct2). These actions collectively contribute to the prevention of Mg²⁺ wasting, thereby mitigating renal damage. 34
There is limited literature on the relationship between serum Mg²⁺ levels and CIN. In the sole conducted investigation, 122 patients who underwent primary PCI were randomly divided into two groups: one receiving intravenous magnesium treatment and the other saline. The research focused on examining the occurrence of CIN. Results showed a significant reduction in the occurrence of CIN in the group receiving Mg²⁺ treatment (P = .01). 35 Consistent with existing literature, our study revealed a significantly higher incidence of CIN in patients with low Mg²⁺ levels. Patients with heart failure, chronic kidney disease, and those who experienced shock and hypotension during admission and hospitalization—factors known to increase the risk of hypoperfusion leading to CIN—were excluded from the study. However, the present findings were despite the group experiencing CIN being older, having more comorbidities, and their procedures were also deemed to be at higher risk. One can speculate that these factors might have contributed to the development of CIN. Nonetheless, in multivariate analysis, these factors were not identified as significant predictors of CIN development. Only age, left ventricular EF, TIMI flow grade, along with Mg²⁺ level, emerged as independent predictors. Additionally, in the ROC analysis conducted among these independent markers, Mg²⁺ level exhibited the highest predictive power.
Study Limitations
This study has several limitations. Firstly, it is a single-center retrospective study, which may restrict the generalizability of the findings. Additionally, the retrospective nature of our study prevents us from establishing causality. Secondly, various studies in the literature have defined CIN and CI-AKI based on different cutoff values and time periods. According to the Kidney Disease Improving Global Outcomes (KDIGO) definition, CI-AKI is characterized by a creatinine level increase of more than 50% from baseline within 7 days after contrast exposure, or an increase of 0.3 mg/dL (26.5 µmol/L) from baseline within 48 h after contrast exposure. However, our study could not establish CI-AKI based on these definitions due to obtaining control creatinine values after 48 h. Moreover, important risk factors for CIN, such as proteinuria and exposure to nephrotoxic agents, could not be thoroughly evaluated due to data limitations inherent in retrospective analyses. Furthermore, the lack of post-discharge patient monitoring, including assessment of medication usage and follow-up on all-cause mortality, limits our understanding of long-term outcomes and potential intervention effects beyond the hospitalization period. These limitations emphasize the necessity for further research with larger, multicenter cohorts and prospective study designs to validate and extend the findings of this study.
Conclusion
We report a crucial relationship between Mg²⁺ levels and the occurrence of CIN in patients who undergo primary PCI for STEMI. Our findings clearly indicate that lower levels of Mg²⁺ are significantly linked to a higher risk of developing CIN, underscoring the essential role of this mineral in maintaining kidney function during intense cardiac procedures. Furthermore, our study has identified a specific threshold for Mg²⁺ levels that can predict the onset of CIN, providing clinicians with a practical tool for potentially assessing risk and implementing targeted interventions. Additionally, this study lays the groundwork for future research in this area.
Footnotes
Acknowledgements
None.
Author Contributions
All authors contributed to: (1) substantial contributions to conception and design, or acquisition of data, or analysis and interpretation of data, (2) drafting the article or revising it critically for important intellectual content, and (3) final approval of the version to be published. Specifically, conceptualization: A.İ.D., A.M.; methodology: A.İ.D., A.M.; investigation: A.İ.D., A.M., G.Ç.; writing—original draft preparation: A.İ.D., A.M., G.Ç.; visualization: A.İ.D.; supervision: G.Ç. All authors approved the final version of this paper.
Data Availability Statement
Data are available on request due to privacy and ethical restrictions.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
This paper has not been published elsewhere in whole or in part. All authors have read and approved the content, and agree to submit it for consideration for publication in your journal. There are no ethical/legal conflicts involved in the article. The research received authorization from the Ethical Committee of Turkey, with approval number 2013/KK/98, and adhered to the principles outlined in the Helsinki Declaration during its execution.
Informed Consent
The need for a written informed consent form from each participant was waived due to the study’s retrospective nature.