
Abstract
The role of inflammation in carotid plaque formation and instability has been highlighted in recent studies. We assessed the significance of smoking status on systemic inflammation and their relationships with carotid stenosis and carotid plaque surface characteristics. A total of 822 patients diagnosed with carotid artery stenosis were recruited and evaluated with systemic inflammation indices according to smoking status. Subgroups were balanced in terms of gender, age, and additional diseases. Systemic inflammation indices were found to be substantially higher in smokers (P < .001) and in patients with irregular-ulcerated surface plaques (P < .001). Plaque surfaces were more irregular and ulcerated in smokers (P < .001). No difference was detected between stenosis degree and smoking status or with systemic inflammation (P > .05). Pan-immune-inflammatory value (PIV) had a strong correlation with both smoking and plaque instability (P < .001, r = .771). Additionally, high PIV levels displayed a significant risk augmentation for irregular/ulcerated surface plaques (P < .001, Odds Ratio (OR):13.796; 95%CI, 5.647-33.701). These findings suggest that in patients with carotid atherosclerotic stenosis, systemic inflammatory markers especially PIV, alongside with plaque surface characteristics, may serve as valuable tools for evaluating and monitoring plaque inflammation. This may lead to more personalized and effective treatment strategies, particularly in smokers.
Keywords
Introduction
In addition to increasing stroke risk, carotid atherosclerosis is often related to other vascular events, such as coronary and peripheral artery diseases. 1 The main pathophysiological mechanism involves the formation of atherosclerotic plaques due to arterial wall damage and lipid accumulation. 2 This process is triggered and promoted by factors such as aging, diabetes mellitus, hypertension, hyperlipidemia, and especially smoking. 3 In recent decades, considerable evidence has highlighted the role of inflammation in plaque formation and instability. Many proteins, cells, and biomarkers have been proposed as indicators of inflammation, either through blood tests or by analyzing endarterectomy specimens.4-6
To quantitatively assess systemic inflammation in an easily accessible way, markers such as neutrophil-to-lymphocyte ratio (NLR), monocyte-to-lymphocyte ratio (MLR), platelet-to-lymphocyte ratio (PLR), C-reactive protein (CRP), and the systemic immune-inflammatory index (SII) have been proposed and studied in vascular events, particularly in coronary atherosclerotic diseases.7,8 Recently, two relatively new indices—systemic inflammatory response index (SIRI) and pan-immune-inflammatory value (PIV)—have been evaluated in atherosclerosis to monitor inflammatory burden and prognosis.9,10
The aim of this study was to examine the implications of smoking status on inflammatory indices and their relationships with carotid stenosis and carotid plaque surface characteristics, rather than directly correlating these systemic inflammation indices with the severity of carotid stenosis.
Materials and Methods
Retrospective Screening of Patients with Carotid Stenosis
The present study involved a retrospective evaluation of patients diagnosed with carotid artery stenosis (≥50% luminal narrowing, based on the North American Symptomatic Carotid Endarterectomy Trial (NASCET) criteria) 11 at the Gazi University Faculty of Medicine, Department of Neurology, Stroke Unit, between January 2014 and January 2024. Patients with inaccessible data, or those diagnosed with systemic infections, malignancies, autoimmune-inflammatory diseases, non-arteriosclerotic extracranial carotid artery stenosis (e.g., dissection, vasculitis), or restenosis following carotid artery interventions, were excluded. Out of 963 patient records screened, 822 met the inclusion criteria and were recruited in the analysis. The study protocol was approved by the Gazi University Ethics Committee in July 2024 (Approval Number: 2024-1180).
Data Collection and Evaluation
The following clinical data were collected: patient age, gender, stroke and transient ischemic attack (TIA) history attributable to large artery atherosclerosis at the time of admission, and the presence of other medical conditions such as diabetes mellitus, hyperlipidemia, hypertension, coronary, and peripheral artery diseases, heart failure, and atrial fibrillation. Smoking status was categorized as non-smoker, ex-smoker, or active smoker. Additionally, the use of antithrombotic and cholesterol-lowering medications was recorded.
Radiological evaluations were performed to evaluate the degree of carotid artery stenosis and atherosclerotic plaque surface characteristics (smooth, irregular, or ulcerated). 12 Other variables included the side of carotid artery stenosis, the presence of intracranial atherosclerotic disease, and co-existing vertebral artery stenosis. Imaging modalities utilized included cranial computed tomography (CT; 16-detector General Electric, Milwaukee, WI, USA) and magnetic resonance imaging (MRI; 1.5 Tesla Siemens Magnetom Aera, Erlangen, Germany). Neurovascular imaging was performed using either CT angiography, MRI angiography, or carotid-vertebral ultrasound (Logic S8 and S9, General Electric, Milwaukee, WI, USA), with selection based on renal function, level of consciousness, and the presence of electronic devices (such as pacemakers or incompatible orthopedic implants). Each patient underwent vascular imaging using at least two modalities, with stenosis degree and plaque surface characteristics determined from reports by radiology specialists. Serum biochemical values were obtained from routine venous blood samples collected at admission to our department.
Systemic Inflammation Indices
Systemic inflammation was assessed using four indices: neutrophil-to-lymphocyte ratio (NLR), systemic immune-inflammatory index (SII), systemic inflammatory response index (SIRI), and pan-immune-inflammatory value (PIV). These indices were calculated as follows:
NLR = neutrophil count (10⁹/L)/lymphocyte count (10⁹/L). 13
SII = platelet count (10⁹/L) × neutrophil count (10⁹/L)/lymphocyte count (10⁹/L). 14
SIRI = neutrophil count (10⁹/L) × monocyte count (10⁹/L)/lymphocyte count (10⁹/L). 9
PIV = neutrophil count (10⁹/L) × platelet count (10⁹/L) × monocyte count (10⁹/L)/ lymphocyte count (10⁹/L). 10
These indices were analyzed both as continuous variables and as quartiles.
Statistical Analysis
Descriptive statistics were performed. Categorical variables were represented as frequencies and percentages, while continuous variables were presented as means ± standard deviations or medians with interquartile ranges (IQR), depending upon the data distribution. The normality of the data was valuated using skewness, kurtosis, Shapiro-Wilk, and Kolmogorov-Smirnov tests. For comparisons between two groups, the independent samples t-test was used for normally distributed continuous variables, while the Mann-Whitney U test was used for non-normal distributed ones. Variables that have more than two groups, ANOVA and Kruskal-Wallis tests were applied.
Variables with statistically significant differences in univariate analyses (P < .01) were further evaluated using correlation analyses: Pearson correlation used for parametric variables and Spearman correlation performed for non-parametric variables. Significance was set at the .01 level (two-tailed). Additionally, multivariate logistic regression models were employed to evaluate potential predictors of outcomes. Statistically appropriate sample size was analyzed using the G-Power 3.1.9.7 and other analyses were performed using the SPSS® version 22.0 (IBM Corp., Armonk, NY, USA). A P < .05 (two-sided) was considered as statistically significant.
Results
Demographic, Clinical, and Radiological Evaluation
A total of 822 patients (607 males and 215 females), aged between 36 and 94 years (mean age: 68.3 ± 8.9 years, IQR: 62-75 years), were recruited. The clinical features of the patients were detailed in Table 1. There were no notable imbalance differences in age, gender, comorbid conditions (diabetes mellitus, hypertension, hyperlipidemia, coronary, or peripheral artery disease) among the subgroups analyzed. To examine the NLR, SII, SIRI, and PIV values, these were divided into quartiles and analyzed as Q1, Q2, Q3, and Q4.
Demographic, Clinical, and Radiological Features Comparison Between Smokers, Ex-smokers, and Nonsmokers in Patients with Carotid Stenosis (≥50% Luminal Narrowing).
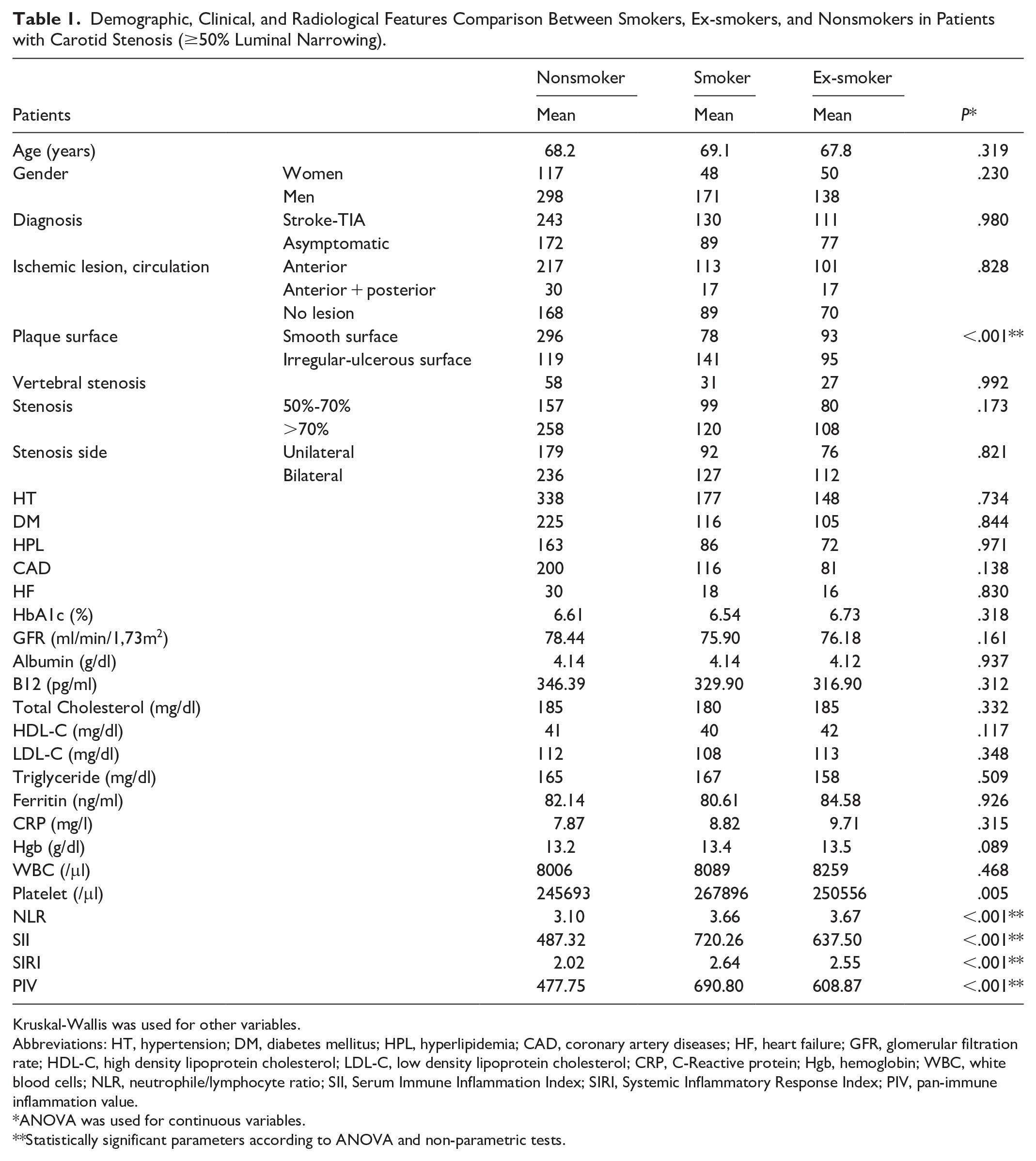
Kruskal-Wallis was used for other variables.
Abbreviations: HT, hypertension; DM, diabetes mellitus; HPL, hyperlipidemia; CAD, coronary artery diseases; HF, heart failure; GFR, glomerular filtration rate; HDL-C, high density lipoprotein cholesterol; LDL-C, low density lipoprotein cholesterol; CRP, C-Reactive protein; Hgb, hemoglobin; WBC, white blood cells; NLR, neutrophile/lymphocyte ratio; SII, Serum Immune Inflammation Index; SIRI, Systemic Inflammatory Response Index; PIV, pan-immune inflammation value.
ANOVA was used for continuous variables.
Statistically significant parameters according to ANOVA and non-parametric tests.
Association of Carotid Stenosis and Plaque Surface Characteristics with Systemic Inflammation
Patients were initially grouped into three categories based on the carotid artery stenotic plaque surface characteristics: smooth, irregular, and ulcerated surfaces. However, since the distribution of patients across these groups was 467 (56.8%), 275 (33.5%), and 80 (9.7%), respectively, the groups were reclassified into two subgroups: smooth surface (467 patients, 56.8%) and irregular-ulcerated surface (335 patients, 43.2%) to improve statistical power.
A comparison between these two groups was made based on age, gender, stenosis severity, white blood cell (WBC) count, NLR, SIRI, and PIV values according to plaque morphology. No significant differences were found in terms of age, gender, or stenosis degree (P > .05). However, WBC count, NLR, SIRI, and PIV values were significantly higher in patients with irregular-ulcerated surface plaques compared with those with smooth surface plaques (P < .001) (Figure 1). In the non-parametric analysis, performed due to the non-normal distribution of SII, irregular-ulcerated plaques were significantly different from smooth surface plaques (P < .05).
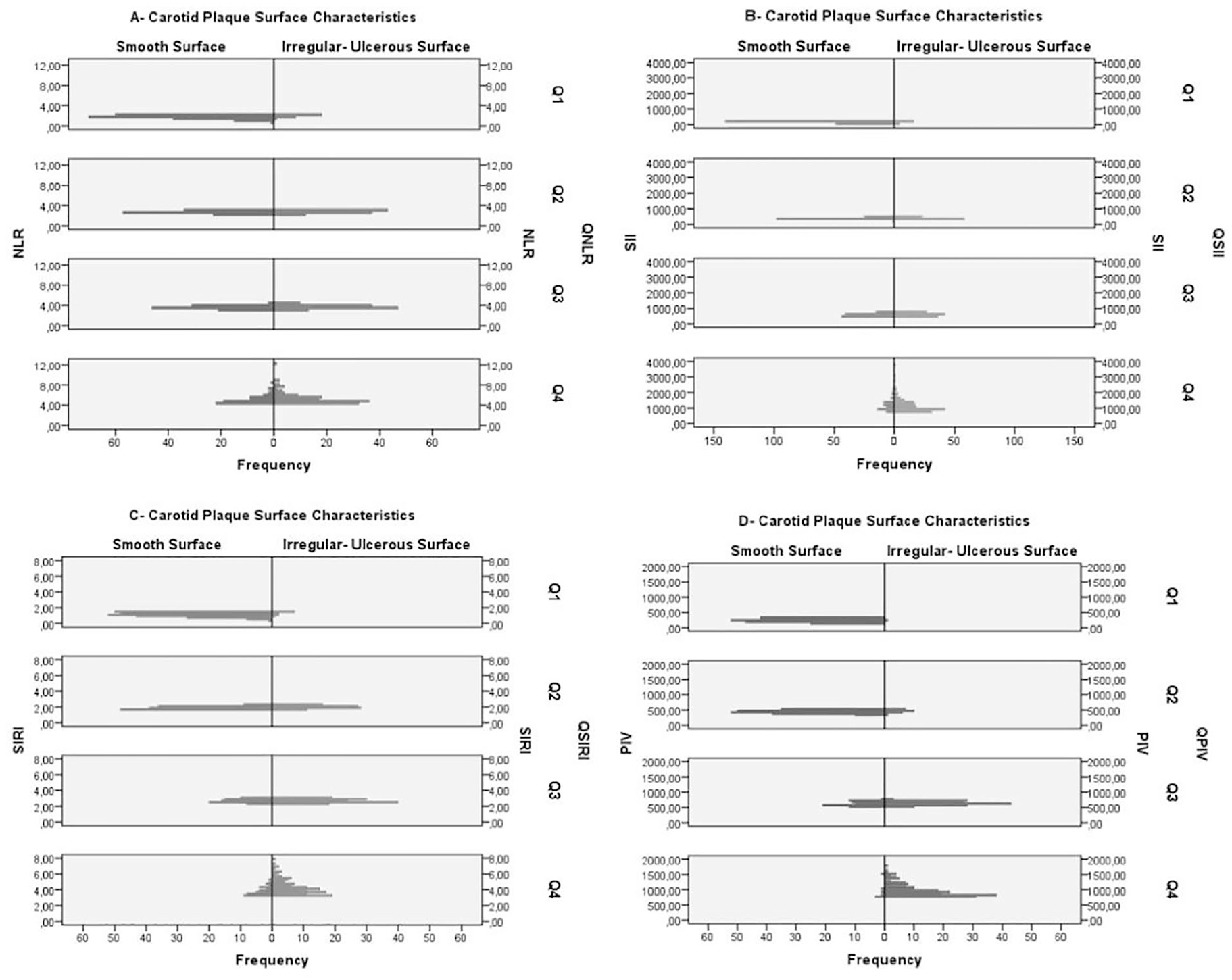
Population pyramid graphs of NLR (neutrophil-to-lymphocyte ratio), systemic immune-inflammatory index (SII), systemic inflammatory response index (SIRI), and PIV (pan-immune-inflammatory) values and their quartiles according to plaque surface characteristics of carotid stenosis patients. In each graph, smooth surface plaques have lower levels of NLR (A), SII (B), SIRI (C), and PIV (D); and higher in irregular-ulcerous surface plaques.
Carotid stenosis severity was analyzed both as a continuous variable and by categorizing it into two groups: 50%-70% stenosis (336 patients) and >70% stenosis (486 patients). When stenosis was assessed as a continuous variable, or in non-parametric analysis, no significant differences were detected between the degree of stenosis, and plaque surface characteristics, WBC count, NLR, SII, SIRI, PIV values, gender, age, or comorbid conditions (P > .05).
Association of Carotid Stenosis and Plaque Surface Characteristics with Smoking Status
When comparing stenotic plaque surface characteristics with smoking status, plaque surfaces were significantly more irregular and ulcerated in smokers and ex-smokers (P < .001). Systemic inflammation markers such as NLR, SII, SIRI, and PIV were significantly higher in smokers, followed by ex-smokers, and lowest in non-smokers (P < .001). No significant difference was observed between stenosis degree and smoking status (P > .05) (Table 1).
Association of Systemic Inflammation with Smoking Status
When comparing serum inflammation markers (NLR, SII, SIRI, PIV) based on smoking status, these were significantly higher in smokers (P < .001). In multivariate analyses harmonized for age, gender, symptomatic carotid stenosis, stenosis percentage, and plaque surface characteristics, a significant interaction was observed only with plaque surface characteristics (P < .05), while no significance was observed for other parameters (P > .05) (Figure 2).
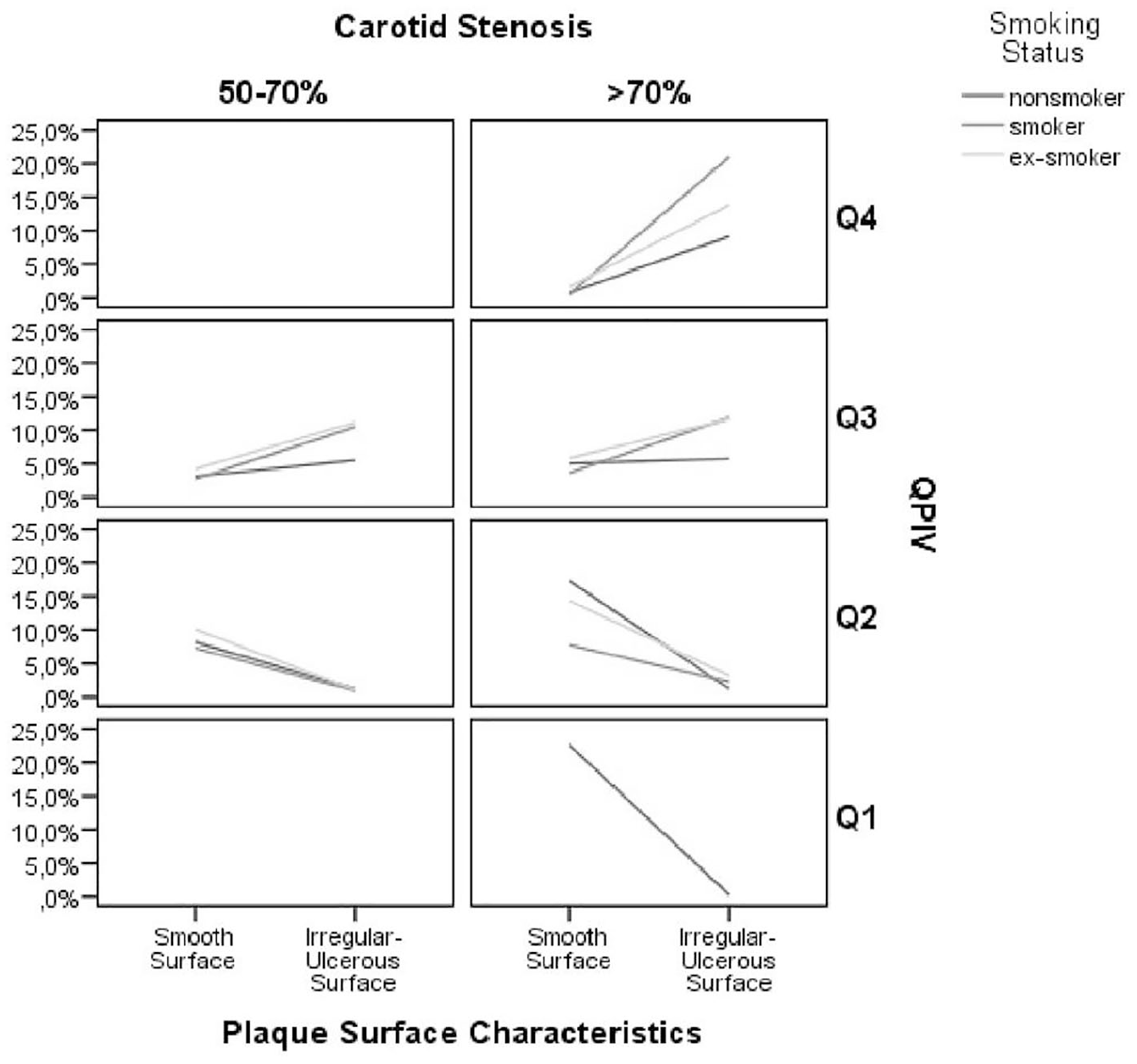
Multivariate line charts illustrate PIV (pan-immune-inflammatory value) quartiles (Q) in relation to plaque surface characteristics, degree of carotid stenosis, and smoking status. No significant relationship was observed between the degree of carotid stenosis and plaque surface characteristics in Q1 and Q2 patients. In Q3 and Q4, patients exhibited a higher prevalence of irregular or ulcerated plaque surfaces across both carotid stenosis groups, though differences by stenosis degree were not statistically significant. Among Q3 and Q4 patients, smokers and ex-smokers displayed a higher occurrence of irregular or ulcerated plaque surfaces compared with non-smokers. Notably, in the Q4 group, all patients exhibited >70% stenosis and a history of smoking, which was associated with an increase in irregular or ulcerated plaque surfaces.
Correlation, Regression, and Receiver Operating Characteristic Analysis
In both univariate and multivariate analyses, parameters with P < .01 were involved in the correlation analysis and multinomial logistic regression analysis (Table 2). Non-parametric correlation analyses revealed no significant correlation with stenosis percentage. A weak correlation was found with smoking status (P < .001, r = .235), and a weak correlation was observed with NLR (P < .001, r = .381). A moderate correlation was seen with SII (P < .001, r = .466) and SIRI (P < .001, r = .572), and a strong correlation with PIV (P < .001, r = .771).
Independent Significance of Factors Distinguishing the Irregular-Ulcerous Surface Carotid Plaques from Smooth Plaques; and Smokers from Nonsmokers.
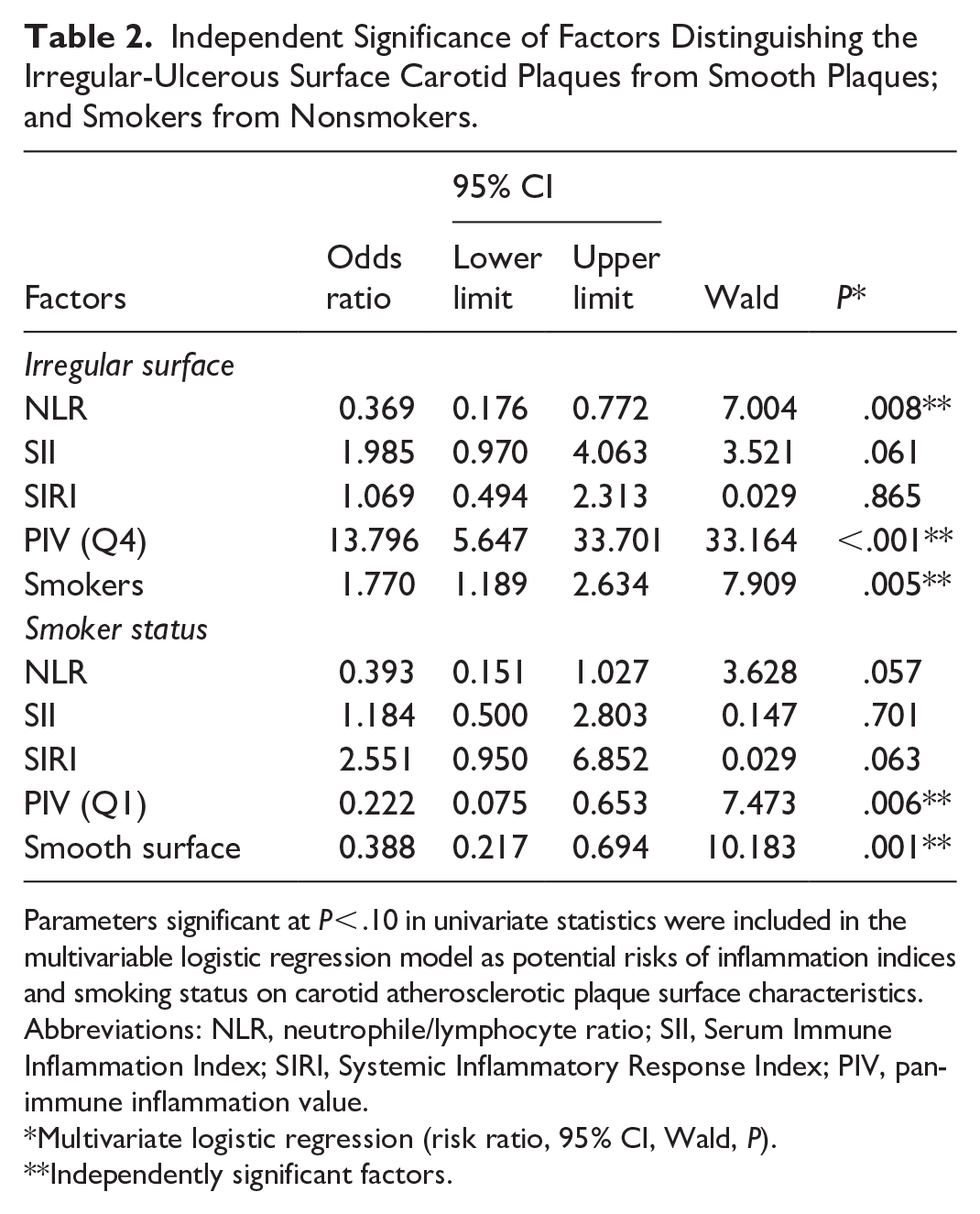
Parameters significant at P < .10 in univariate statistics were included in the multivariable logistic regression model as potential risks of inflammation indices and smoking status on carotid atherosclerotic plaque surface characteristics.
Abbreviations: NLR, neutrophile/lymphocyte ratio; SII, Serum Immune Inflammation Index; SIRI, Systemic Inflammatory Response Index; PIV, pan-immune inflammation value.
Multivariate logistic regression (risk ratio, 95% CI, Wald, P).
Independently significant factors.
In the logistic regression analysis, the two significant factors that distinguished non-smokers from smokers were high quartile PIV (P = .006, Odds Ratio: 0.222; 95% Confidence Interval (CI), 0.075-0.653) and irregular-ulcerated plaque surface (P = .001, OR: 0.388; 95%CI, 0.217-0.694). Additionally, factors that distinguished irregular/ulcerated surface plaques from smooth surface plaques were lower quartiles of NLR (P = .008, OR: 0.369; 95%CI, 0.176-0.772), high quartile of PIV (P < .001, OR: 13.796; 95%CI, 5.647-33.701), and smokers (P = .005, OR: 1.770; 95%CI, 1.189-2.634). According to the multivariate analysis, both being in the first quartile (Q1) of the Pan-Immune-Inflammation Value (PIV) and having a smooth-surfaced carotid plaque were significantly associated with non-smoker status (PIV Q1: OR = 0.222, 95% CI: 0.075-0.653, P = .006; Smooth surface: OR = 0.388, 95% CI: 0.217-0.694, P = .001) (Table 2).
Receiver Operating Characteristic (ROC) analyses of PIV are shown in Figure 3. The cut off value of PIV for plaque irregularity was found as 529.8 (Area under the curve (AUC): 0.945, sensitivity = 92.7%, specificity = 84.4%) and the cut off value of PIV for distinguishing the smokers was 701.7 (AUC: 0.661, sensitivity = 48.9%, specificity = 78.1%) respectively.
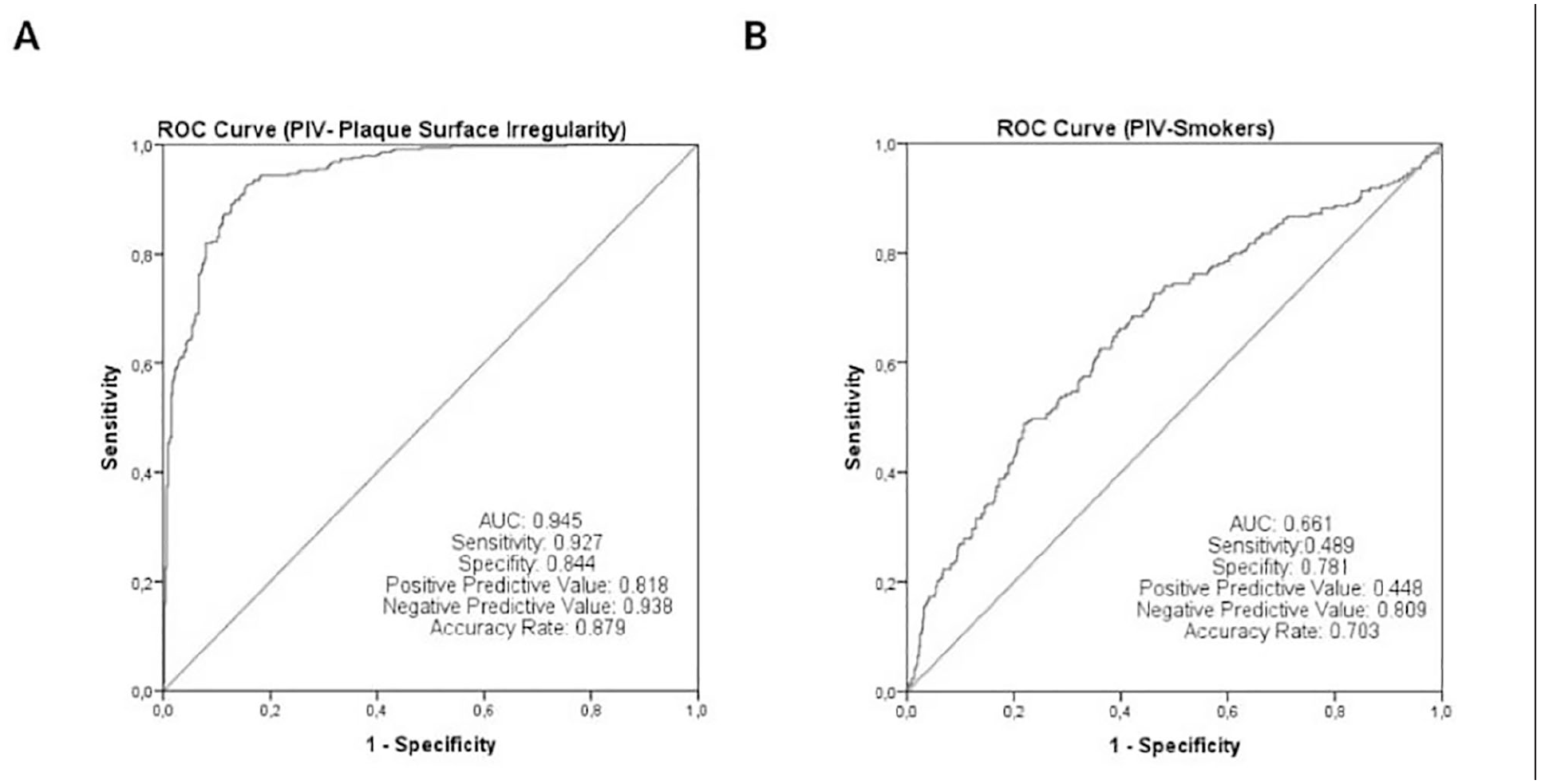
Receiver operating characteristic curves (ROC) of PIV (pan-immune-inflammatory value) and their respective areas under the curves (AUC) for irregularity of the plaque surface and smokers. (A) ROC curve of PIV (AUC = 0.945) for irregularity of plaque surface. (B) ROC curve of PIV (AUC = 0.661) for smokers.
Discussion
This study was conducted to explore the relation between plaque surface characteristics and systemic inflammation markers (SIRI and PIV) in the context of smoking. The findings indicate that systemic inflammation increases with smoking and adversely affects plaque surface characteristics, without a significant impact on the degree of stenosis. Notably, the PIV marker emerged as a significant predictor in both comparative analyses and advanced statistical evaluations.
Inflammation contributes an essential role in the pathogenesis of carotid atherosclerosis. 15 The most established risk factors include diabetes mellitus, hyperlipidemia, hypertension, and smoking.15,16 However, the specific impact of smoking on atherosclerosis has not been extensively scrutinized. 17 In this present research, participants were categorized based on carotid artery stenosis severity, grouped as 50% to 70% and ≥70% stenosis. No significant differences were identified between these groups concerning age, sex, comorbidities, blood parameters, or medication use. Importantly, systemic inflammation, particularly PIV, was significantly associated with smoking and the surface characteristics of atherosclerotic plaques. Active smokers exhibited a significantly higher prevalence of irregular and ulcerated plaque surfaces compared with both non-smokers and former smokers. Additionally, ex-smokers showed greater plaque surface irregularity and higher systemic inflammation levels than never-smokers. Although the duration of smoking cessation among ex-smokers was not included in the analysis, this finding suggests that plaque instability and/or vascular inflammation may persist after smoking cessation.
This observation underscores the potential role of smoking in the development of plaque instability, which extended the stroke risk. Approximately 25% of patients with asymptomatic carotid stenosis harbor unstable plaques. 18 The instability of atherosclerotic plaques is a well-established risk factor for stroke. 19 Smoking exacerbates plaque instability by promoting endothelial damage, largely through inflammatory pathways. 20 At the cellular level, inflammation, lipid metabolism disruption, and extracellular matrix degradation are considered key mechanisms in the formation of unstable plaques.21,22
Elevated levels of inflammatory biomarkers have been detected both in the circulation and within plaque material during atherosclerotic plaque formation and ulceration.3,19 Although much of the research on these mechanisms has focused on coronary atherosclerosis, similar processes have been studied in carotid and intracranial arteries.23,24 The present study sought to assess the PIV, a relatively novel index that has shown promise as a more sensitive indicator of systemic inflammation. First introduced by Fucà et al 10 for prognosis prediction in metastatic colorectal cancer, PIV was found to be more predictive than other indices, such as SII, NLR, and individual counts of monocytes and platelets.
Notably, PIV has not been previously investigated concerning smoking or carotid artery atherosclerosis. This study provides novel insights into its potential application in these contexts. Inflammatory indices reflect secondary changes in blood cell subpopulations, which occur in response to altered inflammatory states. 7 Monocytes are the predominant inflammatory cells during the early stages of plaque formation, while neutrophils are more frequently observed on the plaque surface in cases of instability. 25 The accumulation of macrophages and neutrophils in unstable plaques promotes further leukocyte and lymphocyte migration, which activates platelets. 26 Enzymes secreted by neutrophils, such as myeloperoxidase, gelatinase, collagenase, and elastase, contribute to plaque vulnerability by degrading the extracellular matrix.26,27
An increase in platelet count and activation is commonly observed in patients with carotid stenosis, particularly in those with microembolic signals. 28 Platelets may play a role in symptomatic plaque ulceration through inflammation-driven mechanisms. 28 Smoking has also been shown to increase the risk of plaque ulceration and calcification. In an autopsy-based study, nicotine was found to stimulate oxidative damage by elevating intracellular calcium levels in vascular smooth muscle cells, thus contributing to plaque instability. 29 In asymptomatic carotid stenosis patients, systemic inflammation markers, such as the CRP-Albumin ratio, have been shown to be more elevated in individuals with unstable plaques. 30 Although no definitive predictive cutoff values for PIV and SIRI have been established, studies regarding NLR have highlighted noteworthy findings related to carotid plaque presence.31,32 Corriere et al 33 demonstrated that NLR values exceeding 2.4 predict the presence of carotid plaques with an 80% probability, while values over 3.68 increase this predictive probability to 97%. In a review, NLR was described as a marker reflecting the balance between innate and adaptive immune systems; thus, elevated NLR values may indicate disruption of this immune balance. Notably, NLR has been identified as a highly predictive marker of immune response in various contexts, including progression to sepsis and shock in infections, progression-free survival rates in cancer, mortality in COVID-19 patients, and both severity and mortality in atherosclerotic conditions. 34 Furthermore, studies have examined NLR in both stroke—a condition with atherosclerotic and thrombotic components—and in stroke-related pneumonia, one of the most common infections in stroke patients, where NLR values have been shown to predict both mortality and pneumonia severity. Although smoking was not directly analyzed in the models of Nam et al 35 or Wang et al, 36 its known pro-inflammatory and pro-thrombotic effects likely contribute to elevated NLR, SII, and SIRI levels. Chronic exposure to tobacco smoke may therefore potentiate systemic immune dysregulation and platelet activation, predisposing stroke patients to complications such as pneumonia.
The present study has various limitations. It is a cross-sectional, retrospective observational study. To better establish causal relationships, future research should involve longitudinal analyses of patient blood and radiological parameters over a specified time period. Restricting the cohort to patients with >50% carotid stenosis may have introduced selection bias due to the cross-sectional design of the study. Additionally, the smoking cessation period for ex-smokers was not considered, which may have influenced the results. Nevertheless, ex-smokers continue to exhibit higher levels of systemic inflammatory markers and a greater prevalence of irregular or ulcerated surface plaques.
Conclusion
The findings of the present study propose that in patients with carotid atherosclerotic stenosis, systemic inflammatory markers such as PIV, alongside plaque surface characteristics, may serve as valuable tools for evaluating and monitoring plaque inflammation, particularly in smokers. Elevated PIV levels were consistently observed in both current and former smokers, and plaques with irregular or ulcerated surfaces were significantly more prevalent in these patients.
Given the well-established association between plaque instability and stroke risk, incorporating these markers into routine clinical assessment could significantly enhance our understanding of stroke risk beyond stenosis severity alone. In particular, the identification of irregular or ulcerated plaque surfaces, especially in smokers, highlights the importance of adopting a more nuanced approach to risk stratification and patient management.
Integrating inflammatory markers and plaque characteristics into clinical decision-making algorithms may lead to more personalized and effective treatment strategies for carotid artery stenosis, ultimately improving stroke prevention and patient outcomes.
Footnotes
Author Contributions
All authors contributed to: (1) substantial contributions to conception and design, or acquisition of data, or analysis and interpretation of data, (2) drafting the article or revising it critically for important intellectual content, and, (3) final approval of the version to be published.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.