
Abstract
May-Thurner syndrome (MTS) is an anatomical variant involving compression of the left iliac vein, predisposing to proximal deep vein thrombosis (DVT). Despite its clinical significance, population-level data remain limited. Using the RIETE (Registro Informatizado Enfermedad Trombo-Embólica) registry (2009-2024), we analyzed proximal DVT patients who underwent advanced imaging (CT-venography, contrast-venography, or MRI). Among 2872 patients with advanced imaging-confirmed proximal DVT, 124 (4.3%) had MTS. MTS patients were more likely to be female (78% vs 52%), younger (mean age 42 vs 62 years), and to present with left-sided DVT (92% vs 46%). They had fewer comorbidities, but greater exposure to estrogen or pregnancy. Endovascular therapy was more frequently used in MTS patients (44% vs 3.5%), who also received longer median anticoagulation (365 vs 164 days). Despite this, MTS patients had a significantly higher rate of recurrent DVT (rate ratio: 2.37; 95% CI 1.09-4.70). Multivariable analysis confirmed MTS as an independent predictor of recurrent DVT (adjusted hazard ratio: 2.26; 95% CI: 1.02-5.01). Major bleeding was non-significantly less frequent (rate ratio: 0.42; 95% CI: 0.13-1.04), though retroperitoneal bleeding was more common. MTS is underdiagnosed, has distinct clinical features and is associated with increased DVT recurrence despite aggressive therapy. Improved recognition and tailored management strategies are needed.
Keywords
Introduction
May-Thurner syndrome (MTS), also known as iliac vein compression syndrome, is an anatomical variant in which the left common iliac vein is compressed between the overlying right common iliac artery and the underlying vertebral body.1,2 The resulting persistent pressure can lead to intimal hyperplasia, narrowing the venous lumen and precipitating venous hypertension and venous stasis ultimately predisposing affected individuals to iliofemoral deep vein thrombosis (DVT), particularly when combined with individual risk factors, such as immobility or a hypercoagulable state. Over time, the chronicity of this impaired venous return can contribute to the development of venous insufficiency, culminating in the progressive and debilitating post-thrombotic syndrome. Although classically described as left-sided condition, right-sided, or bilateral involvement has also been reported.1 -3
MTS is a recognized but often underdiagnosed contributor to DVT, particularly in young women and individuals with additional prothrombotic risk factors, such as pregnancy, estrogen use, inherited thrombophilia, scoliosis, or prior vascular stenting. 4 Its clinical presentation is variable, ranging from asymptomatic venous compression to symptomatic DVT, characterized by unilateral leg swelling, pain, and venous claudication.4 -6 Diagnosis of MTS is challenging and typically requires advanced imaging modalities beyond standard duplex ultrasonography. Techniques such as CT venography, contrast venography, or magnetic resonance venography are more effective in visualizing the iliac veins and confirming the diagnosis.6,7
Despite increasing awareness of MTS in recent years, large-scale data on its clinical characteristics, management strategies, and outcomes remain limited. The lack of specific treatment guidelines for DVT in the context of MTS contributes to the complexity of patient management. The existing literature suggests a potential role for endovascular therapy, yet evidence for its long-term impact is controversial.8 -10
A better understanding of the impact of MTS in patients with DVT is essential for guiding diagnosis, treatment decisions, and long-term management. In the present study, we used the extensive RIETE (Registro Informatizado Enfermedad Trombo-Embólica) registry 11 to evaluate the clinical profiles, therapeutic interventions, and anticoagulation outcomes of patients with MTS-associated proximal DVT, comparing them with those without MTS.
Methods
Study Design and Population
This cohort study obtained data from the RIETE registry, an international database of consecutive patients with objectively confirmed VTE. The RIETE registry is registered on ClinicalTrials.gov (NCT02832245) and, as of December 2024, included over 126 000 patients. Its methodology has been validated and benchmarked against large-scale administrative datasets, ensuring robustness, and reliability in clinical outcomes research. 11
We included patients enrolled between January 2009 and December 2024 who were diagnosed with proximal lower-limb DVT and underwent at least one advanced imaging modality (CT-venography, contrast venography, or magnetic resonance imaging [MRI]), in addition to standard duplex ultrasound, to evaluate the iliofemoral venous system. MTS was defined radiographically as extrinsic compression of the common iliac vein by the overlying common iliac artery, resulting in significant luminal narrowing, confirmed by cross-sectional or contrast imaging. Imaging interpretations were conducted locally by radiology teams at participating centers.
Study Outcomes
The primary objective was to compare the clinical characteristics, diagnostic approaches, treatment strategies, and VTE-related outcomes of patients with MTS-associated proximal DVT versus those without MTS. Secondary outcomes included: recurrent symptomatic DVT during anticoagulation, incidence of symptomatic pulmonary embolism (PE), major bleeding events (according to International Society on Thrombosis and Haemostasis criteria), and all-cause mortality. Patients were followed from the initiation of anticoagulation until discontinuation, the occurrence of a study outcome, or the end of the follow-up period.
Ethical Considerations
The RIETE registry protocol was approved by the Ethics Committee of the Hospital Universitari Germans Trias i Pujol (Badalona, Spain). All participating centers obtained approval from their respective institutional review boards and secured informed consent from patients in accordance with local regulatory requirements.
Statistical Analysis
Continuous variables were summarized as means with standard deviations (SD) or medians with interquartile ranges (IQR) and compared using Student t-tests or Mann-Whitney U tests, as appropriate. Categorical variables were expressed as counts and percentages and compared using Chi-square or Fisher’s exact tests. Standardized differences (STD) were used to calculate the effect size. Incidence rates for clinical outcomes were calculated per 100 patient-years, and comparisons between groups were made using rate ratios (RR) with 95% confidence intervals (CI). Fine-Gray competing risk regression models were used to assess time-to-event outcomes, with death treated as a competing risk. Adjusted hazard ratios (aHR) and corresponding 95% CIs were reported. P-values were 2-sided and a P < .05 was considered statistically significant. Univariable and multivariable analyses were performed for the identification of associated and independently associated variables with DVT recurrence. The multivariable model included the following variables: age, sex, body weight, left-sided location, MTS, and comorbidities. Statistical analyses were performed using IBM SPSS Statistics version 25.0 (IBM Corp., Armonk, NY, USA).
Results
From the total cohort of patients recorded in the RIETE registry in December 2024 (128 920), 2872 patients (2.2%) had been diagnosed with lower-limb proximal DVT and undergone advanced imaging in addition to ultrasound, and were included in the final analysis.
Among these 2872 patients with proximal lower-limb DVT and advanced imaging, 124 (4.3%) were diagnosed with MTS. CT venography was the most used diagnostic modality (77%), followed by contrast venography (19%) and MRI (5%). The frequency of MTS diagnoses increased over time, with 78% of cases identified after 2017 (Table 1).
Clinical Characteristics of Patients With Proximal DVT (Confirmed With CT-venography, MRI and/or Contrast Venography) According to the Presence or Absence of May-Thurner Syndrome.
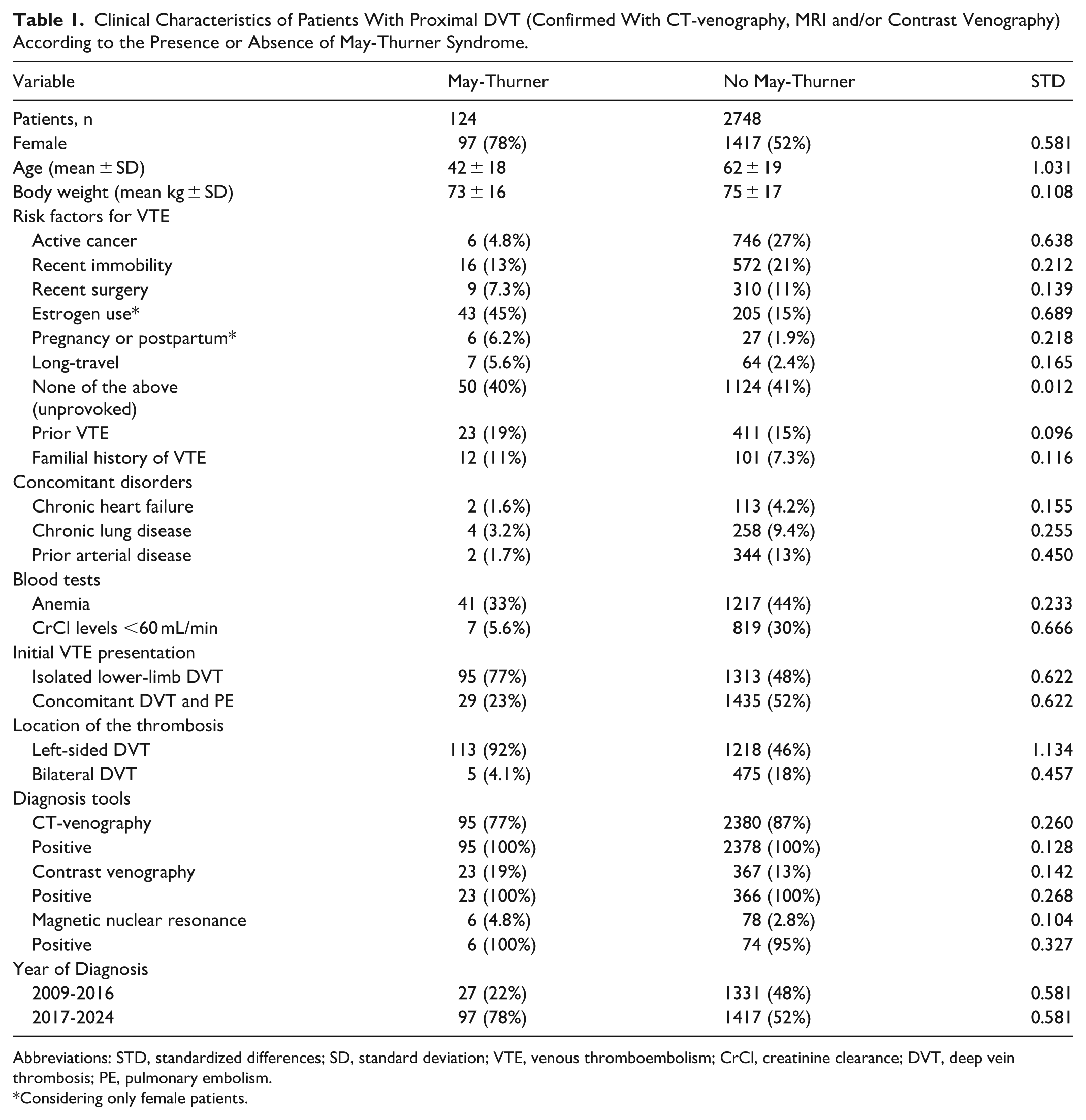
Abbreviations: STD, standardized differences; SD, standard deviation; VTE, venous thromboembolism; CrCl, creatinine clearance; DVT, deep vein thrombosis; PE, pulmonary embolism.
Considering only female patients.
Patients with MTS were more likely to be female (78% vs 52%) and younger (mean age: 42 ± 18 vs 62 ± 19 years) than those without MTS. They also had a significantly higher frequency of left-sided DVT (92% vs 46%) and were more often associated with estrogen use (45% vs 15%) and pregnancy or postpartum status (6.2% vs 1.9%). Conversely, they had lower rates of active cancer (4.8% vs 27%) and comorbid conditions such as arterial disease (1.7% vs 13%) and renal dysfunction (5.6% vs 30%). To assess the magnitude of the effect, we used these approximate thresholds for standardized differences (STD): 0.2 (small), 0.5 (medium), and 0.8 (large). Thus, younger age and left location were the variables most strongly associated with MTS (Table 1).
Endovascular therapy was used significantly more often in patients with MTS (44% vs 3.5%), and they received longer median periods of anticoagulation (365 vs 164 days). Using the thresholds mentioned above for STD, longer duration of anticoagulant treatment and the use of endovascular therapy (both catheter-guided thrombectomy and stent insertion) were the variables most strongly associated with MTS (Table 2).
Treatment Strategies. According to the Presence or Absence of May-Thurner Syndrome.
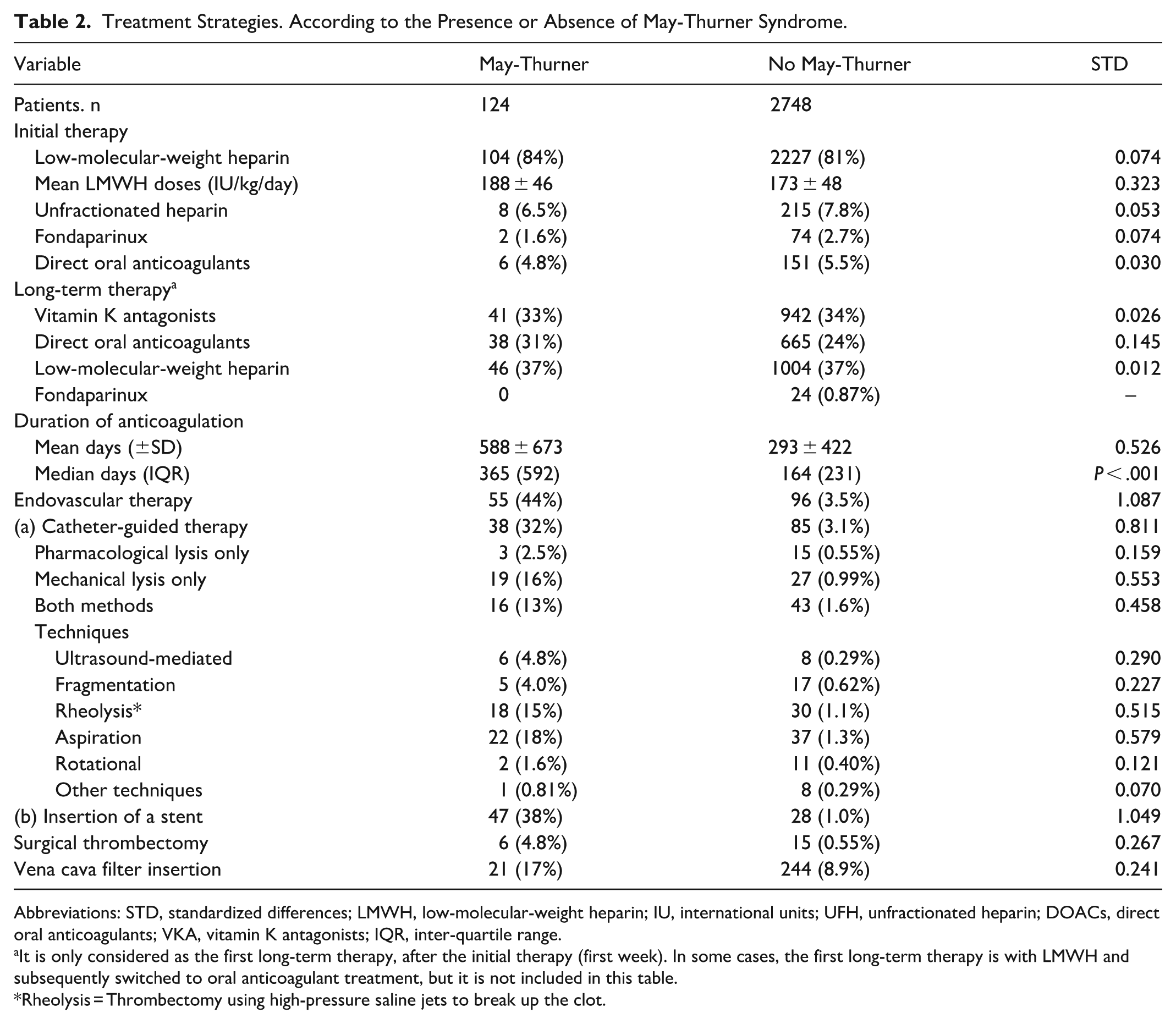
Abbreviations: STD, standardized differences; LMWH, low-molecular-weight heparin; IU, international units; UFH, unfractionated heparin; DOACs, direct oral anticoagulants; VKA, vitamin K antagonists; IQR, inter-quartile range.
It is only considered as the first long-term therapy, after the initial therapy (first week). In some cases, the first long-term therapy is with LMWH and subsequently switched to oral anticoagulant treatment, but it is not included in this table.
Rheolysis = Thrombectomy using high-pressure saline jets to break up the clot.
Despite these interventions, the rate of recurrent symptomatic DVT was notably higher among MTS patients (RR: 2.37; 95% CI: 1.09-4.70; Table 3). Multivariable analysis confirmed MTS as an independent predictor of recurrent DVT (aHR: 2.26; 95% CI: 1.02-5.01), even after adjusting for potential confounders such as age, sex, body weight, and comorbidities.
VTE-related Clinical Outcomes During Anticoagulation.
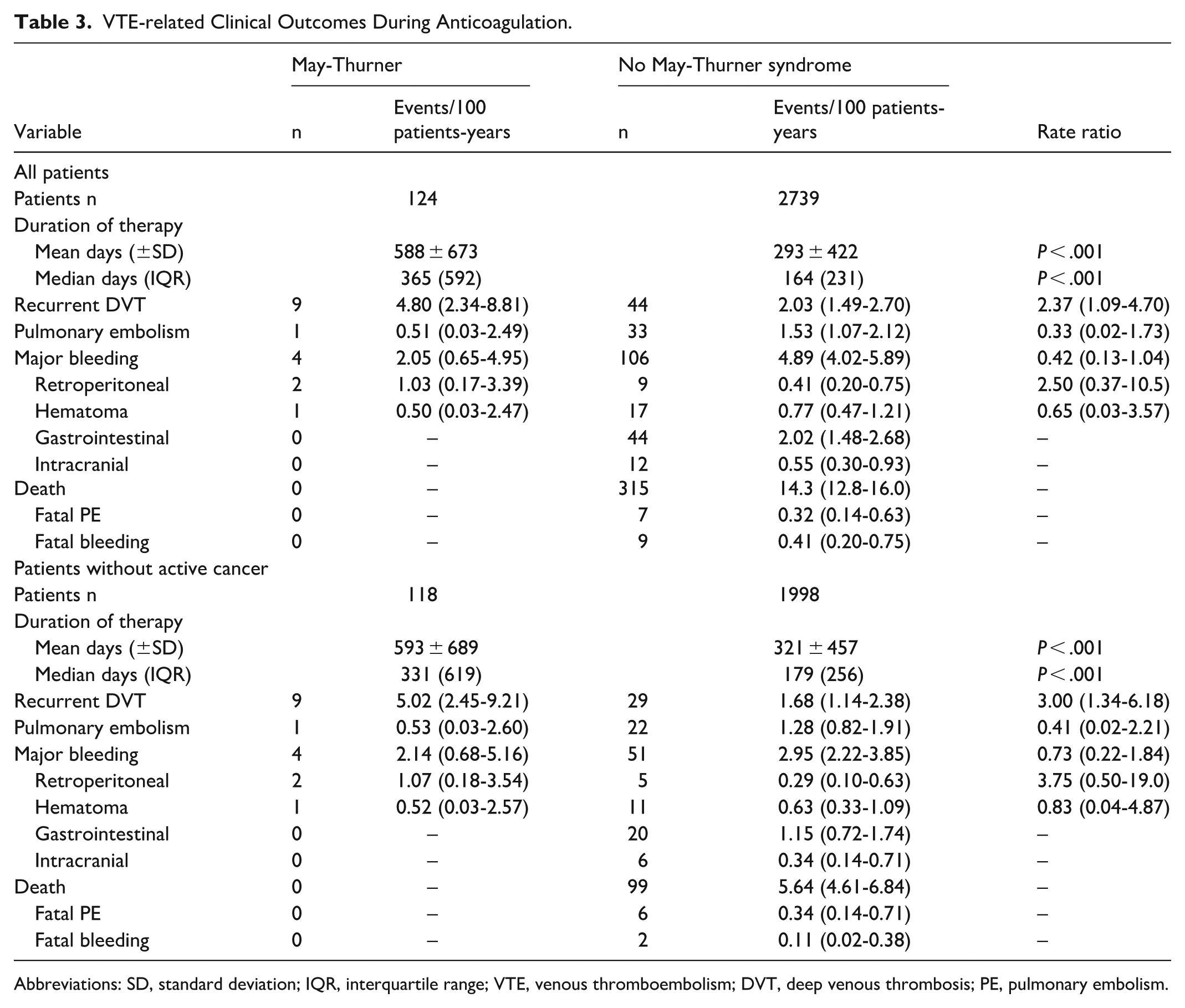
Abbreviations: SD, standard deviation; IQR, interquartile range; VTE, venous thromboembolism; DVT, deep venous thrombosis; PE, pulmonary embolism.
Although not statistically significant, MTS patients exhibited a trend toward fewer major bleeding events (RR: 0.42; 95% CI: 0.13-1.04). However, a non-significant higher proportion of retroperitoneal hematomas was observed in this group (RR: 2.50; 95% CI: 0.37-10.5; Table 3).
Discussion
This large, registry-based analysis highlights the distinct demographic and clinical profile of patients with MTS-associated proximal DVT. Importantly, MTS remains frequently unrecognized and underdiagnosed, largely due to its nonspecific symptoms and the limited use of advancing imaging in routine clinical practice. 7 In line with prior studies,4,12 we observed that MTS disproportionally affects younger women, particularly those with hormonal or pregnancy-related risk factors. The marked predominance of left-sided thrombosis further supports the anatomical basis of MTS.
One of the most important findings is the significantly higher risk of DVT recurrence in MTS patients (being even more relevant when only patients without active cancer are considered), despite a greater reliance on endovascular interventions and longer anticoagulation durations. All these findings support that anatomical compression may lead to persistent venous obstruction, contributing to ongoing thrombotic risk. While stenting and thrombolysis can relieve the underlying mechanical obstruction, our results raise concerns about their long-term effectiveness in fully mitigating recurrence. Additionally, the longer duration of anticoagulant therapy in MTS patients (median 365 vs 165 days) in our cohort could suggest that clinicians may already be recognizing an increased risk of DVT recurrence in this population, especially if endovascular therapy has not been performed.
Recent advances have highlighted the essential role of inflammation as a key factor in the DVT pathogenesis, intricately linked with coagulation through immunothrombosis. 13 In this context, additional factors related to anatomical compression could lead to greater endothelial damage, contributing to triggering inflammatory involvement. Thus, the active searching for clinical features and even specific cellular and molecular biomarkers linked to immunothrombosis may could be useful for identifying patients with MTS more prone to recurrence.
The trend toward lower rates of major bleeding in MTS patients likely reflects their younger age and lower burden of comorbidities. However, the observed increase in retroperitoneal bleeding events warrants caution, and might likely be associated with hypertension in the hypogastric veins in MTS patients under anticoagulant therapy in whom endovascular therapy is not performed to relieve venous compression.
Regarding to the lower incidence of symptomatic PE (both at presentation and during anticoagulation follow-up) in patients with MTS, this could potentially be attributed to the localization of the thrombosis due to anatomical changes related to MTS condition, as it has been yet described. 14
The main strengths of this study include the large, multicenter population and the use of advanced imaging to confirm MTS diagnoses. The extensive and diverse patient population within the RIETE registry lends considerable weight to our findings. Nevertheless, limitations must be acknowledged. The observational design introduces potential confounding and selection bias. Imaging strategies were not standardized across centers, and MTS diagnoses relied on local radiological assessment. It should also be considered that the use of advanced imaging likely led to underestimation of MTS prevalence, as many DVT patients do not undergo such evaluations. Furthermore, the decision on the use of endovascular treatment was not standardized, depending on specific characteristics of each subject (severity of the initial event, comorbidity, etc.) and each center (availability, angiology team behavior, etc.).
Prospective studies with diagnostic, treatment and follow-up protocols are needed to better define the optimal management of MTS. These protocols should ideally include standardized imaging, immunothrombosis biomarkers, long-term outcomes such as post-thrombotic syndrome, quality of life, the need for extended anticoagulation and/or other medication, etc. However, it is worth noting that these studies may still be limited by variability in radiological interpretation, imaging quality, and institutional diagnostic thresholds.
Until more reliable and universally accepted diagnostic criteria are established, heightened clinical suspicion (physicians should be more proactive in searching for and detecting this anatomic condition, particularly in patients with a potentially high-risk clinical profile) and an individualized treatment approach (including consideration of endovascular therapy and prolonged anticoagulation) are warranted for patients with MTS-associated DVT.
Footnotes
Contributions
Appendix
Acknowledgements
We thank the RIETE (Registro Informatizado Enfermedad Trombo-Embólica) investigators (a full list of the RIETE investigators is given in the ![]() ). We express our gratitude to SANOFI (Barcelona, Spain) and ROVI (Pozuelo de Alarcón, Madrid, Spain) for supporting this Registry with an unrestricted educational grant. We also thank the RIETE Registry Coordinating Center, S&H Medical Science Service, for their quality control data, logistic and administrative support and Prof. Salvador Ortiz, Universidad Autónoma Madrid, Statistical Advisor in S&H Medical Science Service for the statistical analysis of the data presented in this paper.
). We express our gratitude to SANOFI (Barcelona, Spain) and ROVI (Pozuelo de Alarcón, Madrid, Spain) for supporting this Registry with an unrestricted educational grant. We also thank the RIETE Registry Coordinating Center, S&H Medical Science Service, for their quality control data, logistic and administrative support and Prof. Salvador Ortiz, Universidad Autónoma Madrid, Statistical Advisor in S&H Medical Science Service for the statistical analysis of the data presented in this paper.
Author Contributions
All authors contributed to: (1) substantial contributions to conception and design, or acquisition of data, or analysis and interpretation of data, (2) drafting the article or revising it critically for important intellectual content, and (3) final approval of the version to be published.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.