
Abstract
The association between abnormal ankle-brachial index (ABI) and adverse prognosis in patients with acute coronary syndrome (ACS) remains insufficiently characterized. The present meta-analysis aims to assess this association. A systematic search of Web of Science, PubMed, and Embase databases was conducted to identify relevant studies. An abnormal ABI was usually defined as ≤0.9 or >1.4. Pooled adjusted hazard ratios (HR) with 95% confidence intervals (CI) were used to assess the prognostic value of the abnormal ABI. Nine studies comprising 5647 patients were included. Abnormal ABI was significantly associated with an increased risk of major adverse cardiovascular events (MACEs; HR 2.39; 95% CI 1.76-3.23), cardiovascular mortality (HR 2.19; 95% CI 1.27-3.78), and all-cause mortality (HR 2.00; 95% CI 1.57-2.55). An abnormal ABI appears to be a significant predictor for increased mortality and MACEs in ACS patients. While the evidence strongly associates a low ABI with this risk, the current literature lacks explicit comparative data on the prognostic value of a high ABI. A low ABI may help refine risk stratification in ACS patients but requires validation in prospective studies.
Keywords
Introduction
Acute coronary syndrome (ACS) encompasses a spectrum of life-threatening cardiovascular conditions, including unstable angina, non-ST-segment elevation myocardial infarction (NSTEMI), and ST-segment elevation myocardial infarction (STEMI). 1 Despite advances in therapeutic strategies, a substantial proportion of ACS patients continue to experience adverse cardiovascular events. 2 Effective risk stratification is essential for optimizing patient management and improving clinical outcomes. Enhancing prognostic markers to identify high-risk patients early in the disease course remains an ongoing challenge in ACS care. 3
Current prognostic scores for ACS primarily rely on clinical, biochemical, and angiographic data but often inadequately capture the systemic vascular disease burden, a critical determinant of long-term outcomes.4,5 The ankle-brachial index (ABI), a simple and non-invasive measure of peripheral arterial perfusion derived from the ratio of ankle to brachial systolic blood pressure, is widely used to diagnose peripheral artery disease (PAD) and assess cardiovascular risk. 6 While a normal ABI ranges from 0.9 to 1.4, values ≤0.9 typically indicate obstructive PAD, whereas values >1.4 often suggest arterial calcification and stiffness. 7 Incorporating ABI into coronary artery disease (CAD) risk assessment can enhance the identification of patients at moderate to high cardiovascular risk. 8
A previous meta-analysis indicated that an abnormal ABI in patients with CAD was associated with an increased risk of cardiovascular events and all-cause mortality. 9 Patients with ACS represent a distinct, high-risk subgroup characterized by heightened inflammatory and thrombotic activity, potentially modulating the ABI-relationship. Consequently, focusing specifically on the ACS subgroup, rather than a broader CAD population, is crucial for understanding these acute effects. However, the prognostic value of an abnormal ABI within the ACS subgroup itself has yielded controversial results.10 -14 These inconsistencies may stem from variable ABI measurement protocols or definitions, patient subtypes, and incomplete adjustment for confounders such as acute-phase markers or medication use. Moreover, a comprehensive quantitative synthesis examining the association between abnormal ABI and key adverse outcomes—such as major adverse cardiovascular events (MACEs) and all-cause mortality—in ACS patients has been lacking.
To address these critical knowledge gaps and clarify the prognostic value of an abnormal ABI in this high-risk population, we conducted a meta-analysis to evaluate the association between abnormal ABI and mortality and MACEs in patients presenting with ACS.
Methods
Data Sources and Literature Searches
To ensure methodological rigor and transparency, this study adhered to the principles of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement. 15 A comprehensive systematic literature search was performed across 3 major electronic medical databases: PubMed, and Embase, and Web of Science. The search terms combined keywords (Supplemental TextS1) related to (“acute coronary syndrome” OR “acute myocardial infarction” OR “unstable angina”) AND (“ankle-brachial index”) AND (“major adverse cardiovascular events” OR “mortality” OR “death”). The search was restricted to studies involving human subjects. The final search was completed on August 6, 2025. Additionally, we manually screened the reference lists of included studies, systematic reviews, and other relevant review articles to identify any potentially missing primary studies.
Study Selection
Studies were included if they met all the following criteria: (1) Population: Patients diagnosed with ACS, including STEMI, NSTEMI, and unstable angina, based on standard clinical diagnostic criteria; (2) Exposure: Abnormal ABI typically defined as ≤0.9 or >1.4; (3) Comparison: Individuals with normal ABI; (4) Outcome measures: Reporting data on at least one predefined adverse outcome, MACEs (typically including death, non-fatal myocardial infarction, heart failure, target vessel revascularization, cerebrovascular attack, and peripheral vascular surgery), cardiovascular mortality, or all-cause mortality; and (5) Study design: Observational studies (cohort studies or case-control studies) reporting adjusted risk estimates derived from multivariable models assessing the association between abnormal ABI and relevant outcomes. When multiple studies involved overlapping or duplicate patient populations, we prioritized the article presenting the most comprehensive and detailed data. Exclusion criteria included: (1) Participants not restricted to ACS; (2) PAD rather than abnormal ABI as the exposure; (3) Risk estimate results based on continuous variable analysis; (4) Studies lacking sufficient outcome data; and (5) Study protocols, review articles, or conference abstracts. Two reviewers independently screened the titles and abstracts of retrieved studies to identify potentially eligible articles. They then reviewed the full texts of these potential studies to determine final inclusion. Any discrepancies among the reviewers were resolved through discussion.
Data Extraction and Quality Assessment
Two reviewers independently extracted relevant data from the included studies using a standardized form. The extracted information included: general study characteristics (first author, publication year, region, study design, sample size, and follow-up duration), patient characteristics (age, gender distribution, and ACS subtype), ABI assessment (definition of abnormal ABI and the percentage of patients with abnormal ABI), and outcome data (fully adjusted risk estimate for MACEs and mortality associated with abnormal ABI, along with adjusted confounding variables). Study quality was assessed using the Newcastle-Ottawa Scale (NOS) for cohort studies, evaluating selection, comparability, and outcome assessment. 16 The methodological quality of the included studies was graded as high (7-9 points), moderate (4-6 points), or low (0-3 points). Any disagreements in data extraction or quality assessment were resolved through discussion between the 2 authors.
Statistical Analysis
All analyses were performed using STATA 12.0 (STATA Corp LP, College Station, TX, USA). The pooled adjusted hazard ratio (HR) and 95% confidence interval (CI) were calculated to quantify the association between abnormal ABI and the risk of MACEs and all-cause mortality. Heterogeneity among the included studies was assessed using the I² statistic and Cochran’s Q test. Given the apparent clinical heterogeneity across studies in terms of population diversity, ABI measurement protocols, and study designs, a random-effects model was applied throughout the manuscript, irrespective of I² values and Cochran’s Q test results. Sensitivity analyses, performed by sequentially excluding each individual study, were planned to evaluate the influence of any single study on the overall pooled effect. Subgroup analyses were conducted based on potential factors that might affect the association, including study design (prospective vs retrospective), geographical region (Asia vs others), ACS subtype (AMI vs all ACS), participants’ number (≥500 vs <500), and follow-up duration (>3 years vs ≤3 years). Publication bias was assessed visually using funnel plots and statistically using Begg’s test 17 and Egger’s test, 18 with a P < .1 indicating significant publication bias.
Results
Search Results
Our initial search identified 415 records, with 1 additional record found through hand searching. After removing duplicates, title and abstract screening, 377 records were excluded. The remaining 39 full-text articles were assessed for eligibility, resulting in 30 exclusions due to various reasons (Figure 1). Finally, 9 studies10,11,13,19 -24 met the inclusion criteria and were included in the meta-analysis.
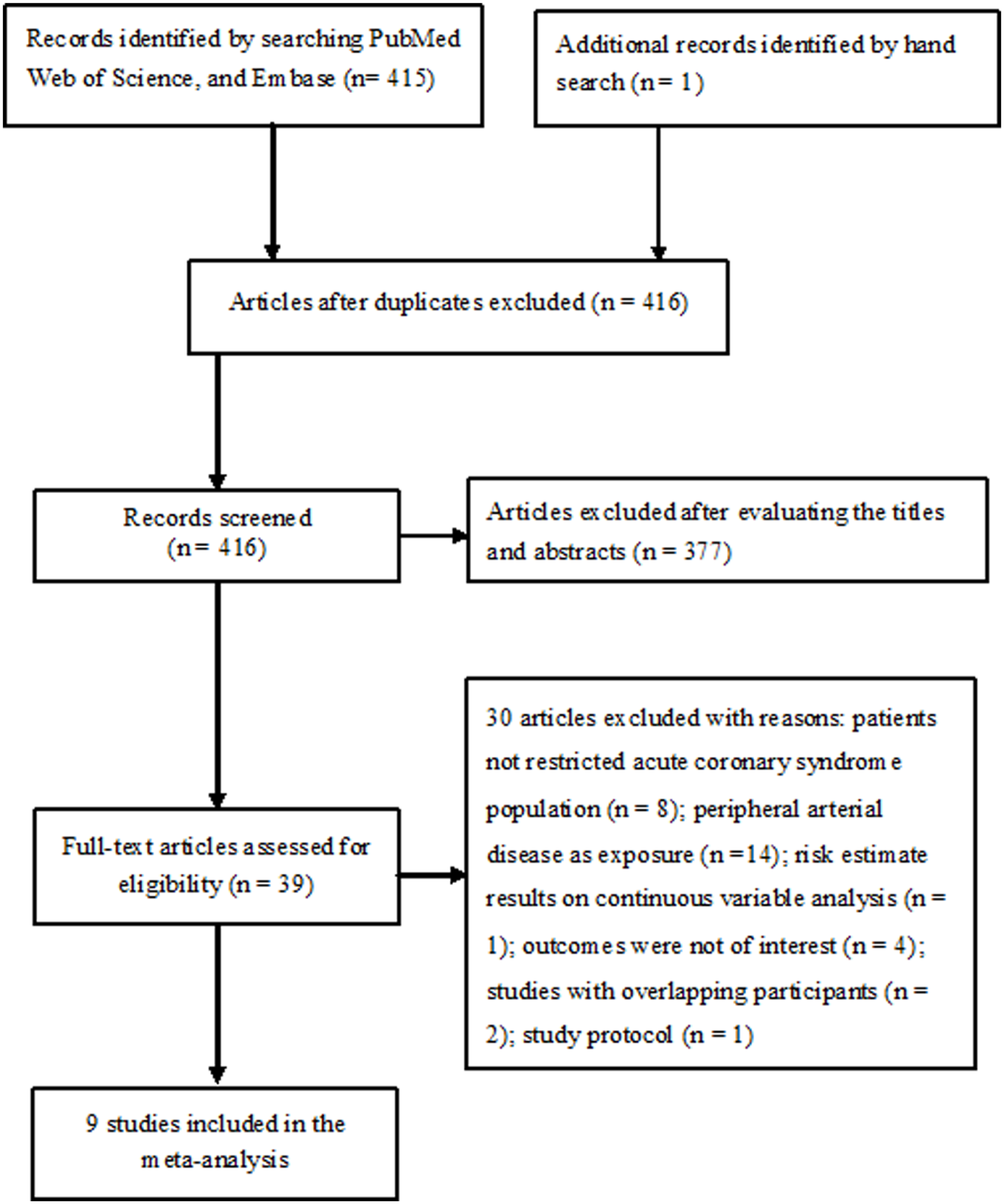
Study selection flowchart.
Study Characteristics
Table 1 presents the basic characteristic of the included studies. The included studies were published between 2009 and 2025, encompassing a total of 5647 patients. These studies were conducted across diverse regions, including China, 10 Japan,19,22 Taiwan, 20 Republic of Korea, 21 Spain, 11 France, 13 Italy, 23 and Greece. 24 Four studies13,19,20,22 were retrospective designs and the remaining were prospective studies. The mean age of participants ranged from 59.4 to 68.9 years, with a predominance of male patients (70.6%-80%). The prevalence of abnormal ankle-brachial index ranged from 10% to 44%. Follow-up durations varied from 0.95 to 5.3 years. All studies adjusted for potential confounders, with common covariates including age, sex, diabetes, hypertension, and left ventricular ejection fraction. Assessment using the NOS criteria indicated that the included studies exhibited moderate to high methodological quality (Supplemental Table S1).
Main Characteristic of the Included Studies.
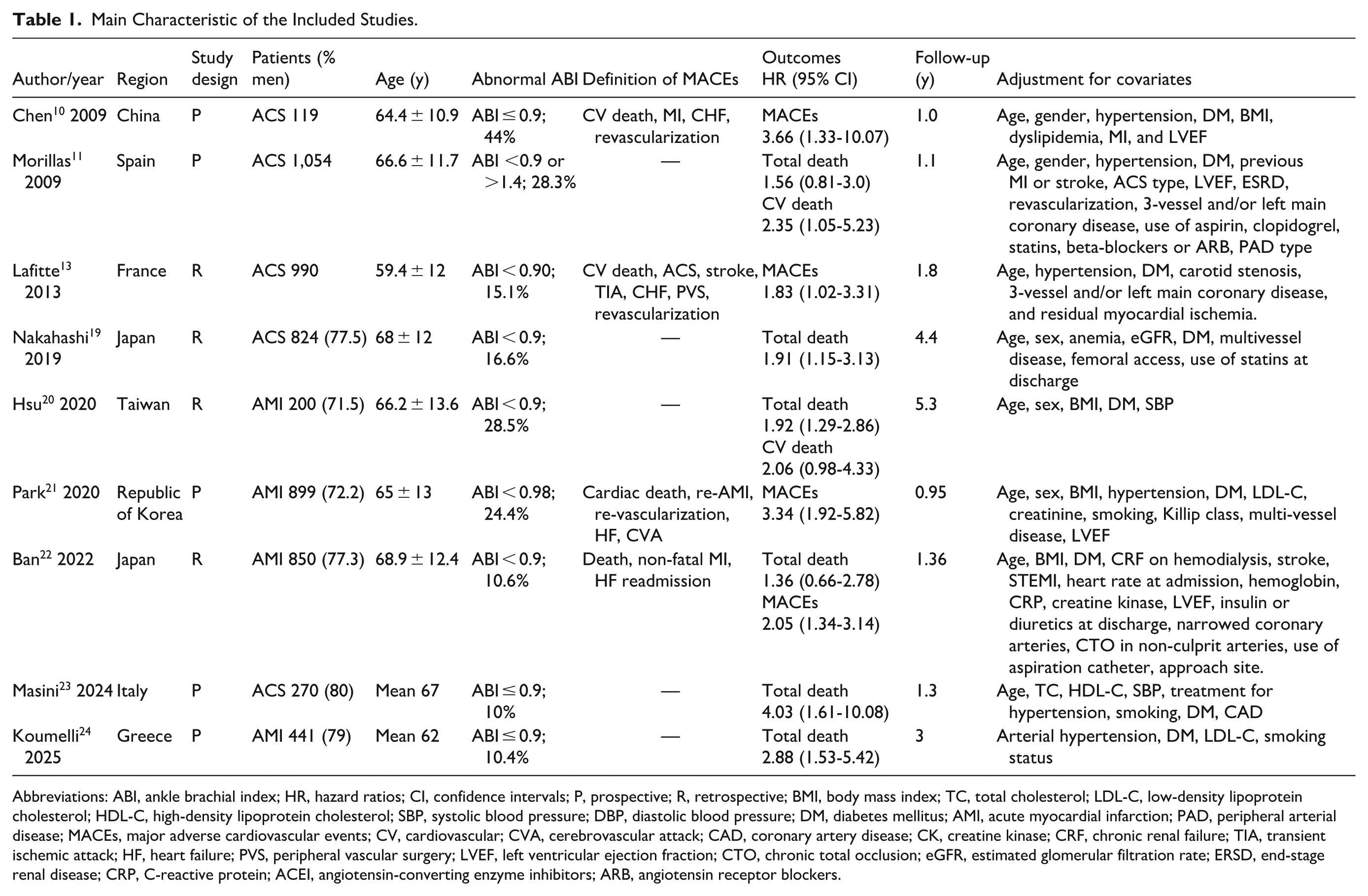
Abbreviations: ABI, ankle brachial index; HR, hazard ratios; CI, confidence intervals; P, prospective; R, retrospective; BMI, body mass index; TC, total cholesterol; LDL-C, low-density lipoprotein cholesterol; HDL-C, high-density lipoprotein cholesterol; SBP, systolic blood pressure; DBP, diastolic blood pressure; DM, diabetes mellitus; AMI, acute myocardial infarction; PAD, peripheral arterial disease; MACEs, major adverse cardiovascular events; CV, cardiovascular; CVA, cerebrovascular attack; CAD, coronary artery disease; CK, creatine kinase; CRF, chronic renal failure; TIA, transient ischemic attack; HF, heart failure; PVS, peripheral vascular surgery; LVEF, left ventricular ejection fraction; CTO, chronic total occlusion; eGFR, estimated glomerular filtration rate; ERSD, end-stage renal disease; CRP, C-reactive protein; ACEI, angiotensin-converting enzyme inhibitors; ARB, angiotensin receptor blockers.
All-cause Mortality
Six studies11,19,20,22 -24 evaluated the association between abnormal ABI and all-cause mortality risk. As shown in Figure 2, abnormal ABI was associated with a higher risk of all-cause mortality (HR 2.00; 95% CI 1.57-2.55) in a random-effects model, without significant heterogeneity (I2 = 4.8%; P = .386). Sensitivity analysis indicated that excluding any single did not significantly change the statistical significance of the overall pooled effect. The pooled HR of all-cause mortality was 1.99 (95% CI 1.54-2.57) after excluding 2 studies22,23 with NOS ≤6. Publication bias was not detected by visual inspection of funnel plots (Figure 3) and the Begg’s test (P = 1.000) as well as Egger’s test (P = .533). Beyond subgroups stratified by ACS subtypes, the significant association between an abnormal ABI and all-cause mortality was statistically significant across all predefined subgroups (Table 2). When the analysis (Figure S1) was restricted in studies defining abnormal ABI as ≤0.9, the pooled HR of all-cause mortality was 2.09 (95% CI 1.58-2.75).
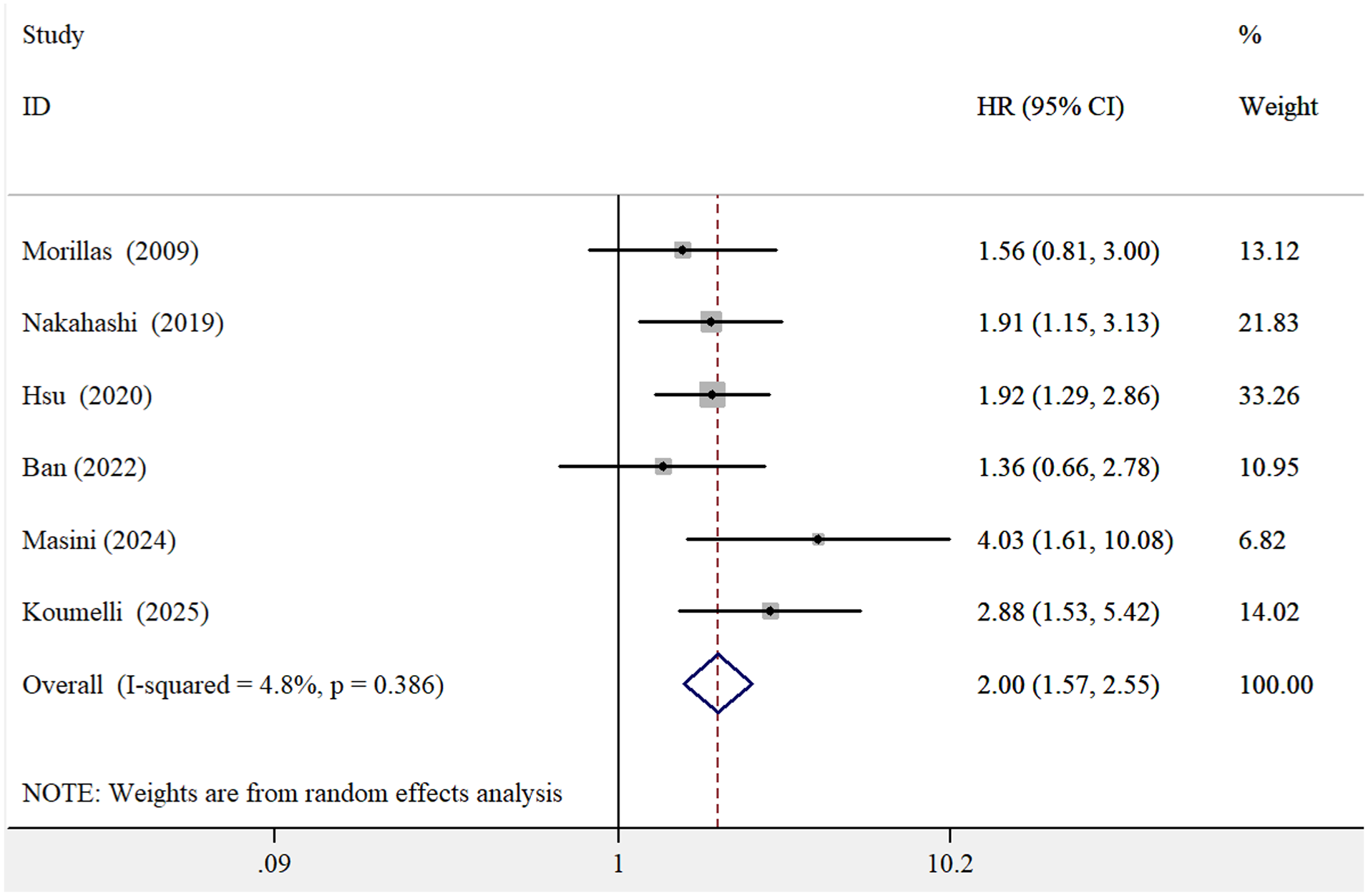
Forest plots showing the pooled HR and 95% CI of all-cause mortality for the abnormal versus normal ankle-brachial index.
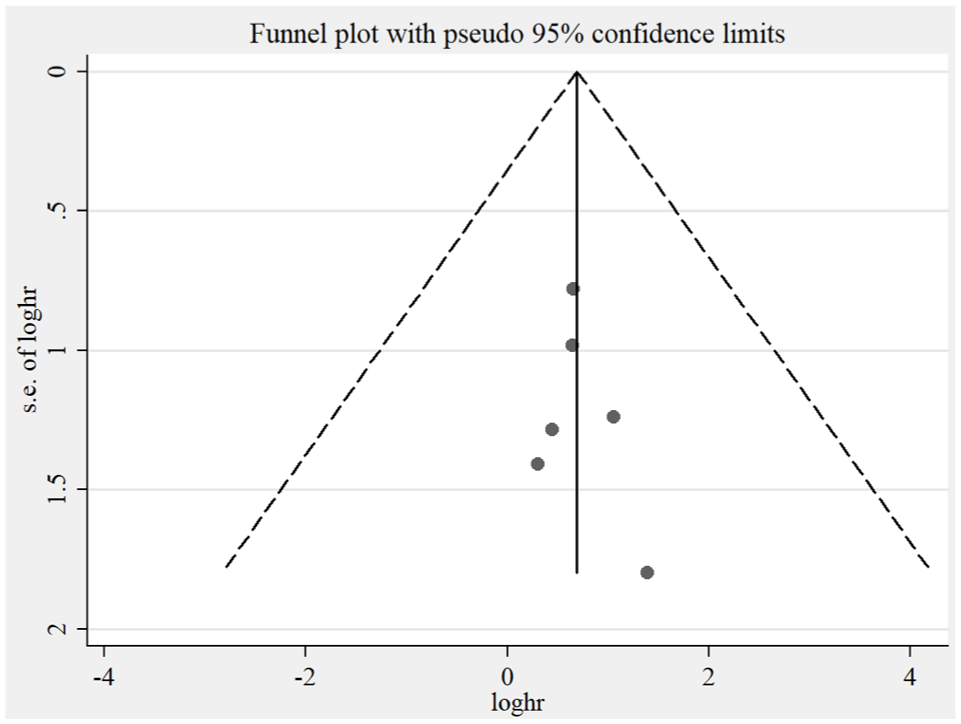
Funnel plots showing the association between abnormal ankle-brachial index and the risk of all-cause mortality.
Results of Subgroup Analysis on All-cause Mortality.
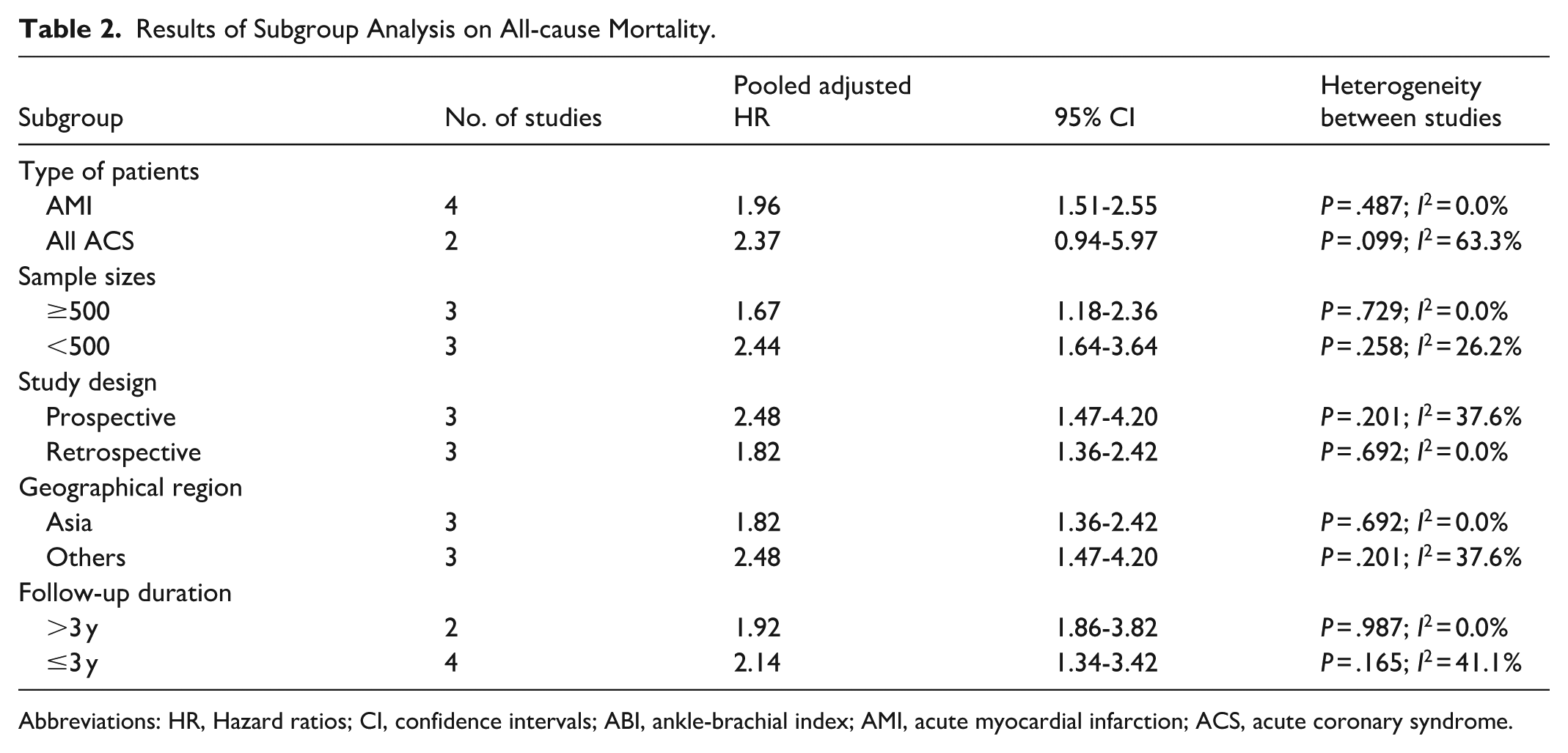
Abbreviations: HR, Hazard ratios; CI, confidence intervals; ABI, ankle-brachial index; AMI, acute myocardial infarction; ACS, acute coronary syndrome.
Major Adverse Cardiovascular Events
Four studies10,13,21,22 evaluated the association between abnormal ABI and MACEs risk. As shown in Figure 4, abnormal ABI was associated with a higher risk of MACEs (HR 2.39; 95% CI 1.76-3.23) in a random effects model, without significant heterogeneity (I2 = 10.9%; P = .339). Leave-one-out sensitivity analysis demonstrated the robustness of the overall pooled effect.
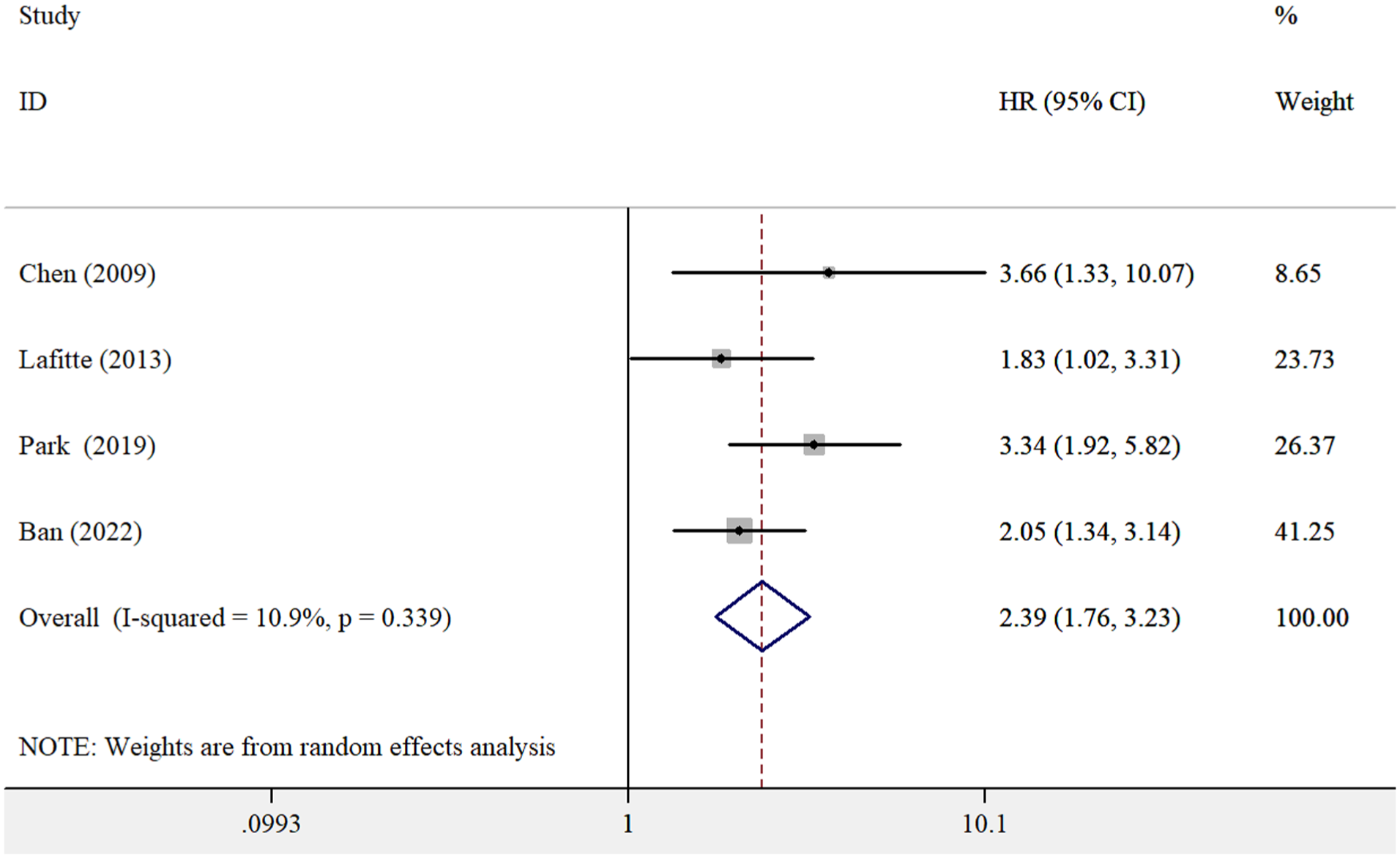
Forest plots showing the pooled HR and 95% CI of MACEs for the abnormal versus normal ankle-brachial index.
Cardiovascular Mortality
Two studies11,20 evaluated the association between abnormal ABI and cardiovascular mortality. The pooled analysis in a random-effects model indicated a 2.19-fold increased risk of cardiovascular mortality (HR 2.19, 95% CI 1.27-3.78; Figure S2) among patients with abnormal ABI, with no observed heterogeneity (I² = 0.0%, P = .813).
Discussion
The findings of this meta-analysis, which included 9 studies encompassing 5647 patients with ACS, provide preliminary evidence that an abnormal ABI is strongly associated with an increased risk of MACEs, cardiovascular mortality, and all-cause mortality. Notably, ACS patients with an abnormal ABI exhibited more than a twofold increased risk of MACEs, cardiovascular mortality, and all-cause mortality. These results underscore the potential clinical utility of ABI measurement for risk stratification in ACS populations.
Our findings reinforce and expand upon existing evidence linking abnormal ABI to adverse outcomes in CAD. A previous meta-analysis of CAD patients demonstrated that an abnormal ABI was associated with a 1.46-fold increased risk of MACEs and a 75% higher risk of all-cause mortality. 9 In contrast, our study revealed even stronger associations in patients with ACS, a more acute and high-risk CAD subgroup. This suggests that an abnormal ABI may confer a greater risk in the context of ACS. The heightened risk observed in ACS patients may result from their unique vulnerability, where underlying systemic atherosclerosis could exacerbate acute ischemic injury, predisposing them to more severe complications.
Furthermore, our subgroup analysis demonstrated that an abnormal ABI was a significant predictor of all-cause mortality across various study designs, sample sizes, geographical region, and follow-up durations. Notably, when the analysis was limited to studies involving patients with acute myocardial infarction, the association between abnormal ABI and all-cause mortality remained significant, reinforcing its prognostic value in this high-risk subgroup. Sensitivity analysis excluding studies with NOS ≤6 showed a slight decrease in the pooled HR for all-cause mortality to 1.99. This finding suggests that the pooled effect estimate is relatively robust to the inclusion of moderate quality studies. The lack of statistical significance observed across all ACS subgroups may be attributed to the limited statistical power inherent in these specific patient strata. However, since most included studies primarily examined abnormally low ABI, the observed association in our meta-analysis was predominantly driven by low ABI rather than high ABI.
According to current American Heart Association guidelines, an abnormal ABI is defined as a value <0.9 or >1.4. 25 An ABI value exceeding 1.4 often indicates arterial stiffness and medial calcification, 7 and an abnormally high ABI has been associated with an increased risk of cardiovascular disease and all-cause mortality in patients with suspected or established cardiovascular disease. 26 However, most studies included in our meta-analysis used a reference group with ABI > 0.9, rather than the conventional normal range of 0.9 to 1.4. This choice inflates the baseline risk of the reference group by including individuals with high ABI (>1.4), who are also at elevated mortality risk, potentially underestimating the true magnitude of risk associated with abnormally low ABI. Future research should further investigate the independent and combined effects of abnormally low and high ABI on adverse outcomes in ACS patients, perhaps employing a three-category approach (low, normal, high) to better delineate risk gradients.
The observed association between abnormal ABI and adverse outcomes in ACS patients likely reflects the presence of underlying systemic atherosclerosis, 27 endothelial dysfunction, 28 and heightened inflammatory responses. 29 Specifically, an abnormal ABI serves as a readily accessible marker of PAD, which frequently coexists with ACS and shares common risk factors—such as smoking, diabetes, and hypertension.30,31 The presence of PAD, as indicated by an abnormal ABI, suggests a more extensive atherosclerotic burden and severe coronary artery involvement.32,33
The results of this meta-analysis should be interpreted with caution due to several potential limitations. First, reliance on single time-point ABI measurements may have introduced selection bias. Second, heterogeneity existed in ABI measurement protocols across the included studies, encompassing variations in techniques and cutoff values. Third, the covariates used in multivariable models varied across the included studies. This inconsistency could introduce residual confounding and affect the reliability of the pooled effect estimates. Fourth, despite a seemingly symmetric funnel plot, the statistical power to reliably detect publication bias was limited due to fewer than 10 studies included. 34 Consequently, the potential for small-study effects cannot be ruled out and the pooled effect estimates should be interpreted with caution. Fifth, given the heterogeneity of ACS patients, the generalizability of our findings to specific ACS subtypes may be limited. Sixth, due to the lack of reporting on the prognostic impact of abnormally high ABI, our analysis could not separately quantify outcomes for this group. Finally, exclusion of the Cochrane Library and gray literature limits the comprehensiveness of our meta-analysis due to potential omission of relevant studies.
Despite these limitations, our findings have important clinical implications. The strong association between abnormal ABI and adverse outcomes suggests that routine ABI measurement could enhance risk stratification in ACS patients, potentially surpassing conventional scoring systems. Incorporating ABI assessment may improve the identification of high-risk individuals who could benefit from intensified, evidence-based therapies. However, prospective studies are necessary to determine whether ABI-guided interventions significantly improve clinical outcomes in this high-risk population. Furthermore, additional research is warranted to establish the optimal ABI cutoff values for risk stratification in ACS patients. Further investigation is also needed to elucidate the underlying mechanisms linking abnormal ABI to adverse cardiovascular events in ACS patients, with particular emphasis on the roles of inflammation, thrombosis, and microvascular dysfunction.
Conclusions
An abnormal ABI appears to be a significant predictor for increased mortality and MACEs in ACS patients. While the evidence strongly associates a low ABI with this risk, the current literature lacks explicit comparative data on the prognostic value of an abnormally high ABI. ABI may help refine risk stratification in ACS patients but requires validation in prospective studies.
Supplemental Material
sj-docx-1-ang-10.1177_00033197251407738 – Supplemental material for Impact of Abnormal Ankle-Brachial Index on Adverse Outcomes in Patients With Acute Coronary Syndrome: A Meta-Analysis
Supplemental material, sj-docx-1-ang-10.1177_00033197251407738 for Impact of Abnormal Ankle-Brachial Index on Adverse Outcomes in Patients With Acute Coronary Syndrome: A Meta-Analysis by Lijun Li and Xinhua Hu in Angiology
Supplemental Material
sj-docx-2-ang-10.1177_00033197251407738 – Supplemental material for Impact of Abnormal Ankle-Brachial Index on Adverse Outcomes in Patients With Acute Coronary Syndrome: A Meta-Analysis
Supplemental material, sj-docx-2-ang-10.1177_00033197251407738 for Impact of Abnormal Ankle-Brachial Index on Adverse Outcomes in Patients With Acute Coronary Syndrome: A Meta-Analysis by Lijun Li and Xinhua Hu in Angiology
Footnotes
Author Contributions
All authors contributed to: (1) substantial contributions to conception and design, or acquisition of data, or analysis and interpretation of data, (2) drafting the article or revising it critically for important intellectual content, and (3) final approval of the version to be published.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All data included in the article or supplemental material.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.