
Abstract
Myocardial infarction with non-obstructive coronary arteries (MINOCA) represents 5% to 10% of acute myocardial infarction cases. The Fibrosis-4 (FIB-4) index and non-alcoholic fatty liver disease (NAFLD) are emerging markers of systemic inflammation and metabolic dysfunction, yet their prognostic role in MINOCA remains unexplored. This prospective cohort study included 472 consecutive MINOCA patients from a tertiary cardiac center between September 2022 and October 2025. Patients were stratified by FIB-4 index (high ≥1.3, low <1.3). NAFLD was diagnosed using hepatic steatosis index. The primary endpoint was major adverse cardiovascular events (MACE): cardiovascular death, recurrent myocardial infarction, urgent revascularization, or hospitalization for heart failure or arrhythmia during 36-month follow-up. High FIB-4 index was independently associated with increased MACE risk (hazard ratio [HR]: 2.34, 95% confidence interval [CI]: 1.45-3.78, P < .001). NAFLD presence further augmented this risk (HR: 1.89, 95% CI: 1.23-2.91, P = .004). Patients with both high FIB-4 and NAFLD demonstrated worst outcomes (HR: 3.12, 95% CI: 1.87-5.21, P < .001). FIB-4 showed good discriminative ability for MACE prediction (AUC: 0.712, 95% CI: 0.665-0.759). FIB-4 index and NAFLD are independent predictors of adverse outcomes in MINOCA patients, offering simple, cost-effective tools for risk stratification.
Keywords
Introduction
Myocardial infarction with non-obstructive coronary arteries (MINOCA) constitutes ~5% to 15% of acute myocardial infarction presentations and poses unique diagnostic and prognostic challenges.1,2 This syndrome disproportionately affects younger individuals and women, yet confers substantial cardiovascular risk with reported annual major adverse cardiovascular events (MACE) rates ranging from 3.5% to 7.7%. 3 The pathophysiological heterogeneity underlying MINOCA encompassing plaque disruption without significant stenosis, coronary vasospasm, spontaneous coronary artery dissection, thromboembolism, and coronary microvascular dysfunction complicates traditional risk stratification approaches and necessitates investigation of novel prognostic biomarkers. 4
The Fibrosis-4 (FIB-4) index, originally validated for non-invasive assessment of hepatic fibrosis in chronic liver disease, has demonstrated unexpected prognostic utility in cardiovascular populations.5,6 Calculated as (age × aspartate aminotransferase [AST])/(platelet count × √alanine aminotransferase [ALT]), this simple formula requires only routine laboratory parameters. Recent investigations suggest that FIB-4 may function as a systemic biomarker reflecting common pathophysiological processes including chronic low-grade inflammation, insulin resistance, oxidative stress, and endothelial dysfunction—mechanisms central to both hepatic fibrogenesis and atherosclerotic cardiovascular disease.
Non-alcoholic fatty liver disease (NAFLD), affecting ~25% to 30% of the general population, has emerged as an independent cardiovascular risk factor beyond traditional metabolic syndrome components.7,8 The hepatic steatosis index (HSI = 8 × [ALT/AST ratio] + body mass index [BMI] + 2 [if diabetes mellitus present] + 2 [if female]) provides accessible NAFLD screening using standard clinical and laboratory data. 9 The mechanistic intersection of hepatic steatosis and cardiovascular disease involves shared metabolic derangements, pro-inflammatory cytokine production, altered lipid metabolism, and increased hepatic glucose output pathways potentially amplified in MINOCA where metabolic factors may assume disproportionate pathogenic importance relative to atherosclerotic burden.10,11
Despite theoretical plausibility and supportive evidence in general acute coronary syndrome cohorts, comprehensive investigation of FIB-4 index and NAFLD specifically within MINOCA populations remains limited.12,13 Existing literature predominantly comprises retrospective analyses with relatively small sample sizes and heterogeneous methodologies. We therefore conducted this prospective observational cohort study to rigorously evaluate the independent prognostic value of FIB-4 index and NAFLD severity for prediction of major adverse cardiovascular events in MINOCA patients, employing contemporary statistical validation methods including discrimination analysis, calibration assessment, and net reclassification improvement calculation.
Methods
Study Design and Patient Population
This prospective single-center observational cohort study enrolled consecutive patients diagnosed with MINOCA between September 2022 and October 2025 at our tertiary cardiovascular center. The institutional ethics committee approved the study protocol on September 7, 2022 (approval number: 2022/13/4). Given the observational nature utilizing routine clinical data, the requirement for individual informed consent was waived by institutional guidelines.
MINOCA diagnosis adhered to Fourth Universal Definition of Myocardial Infarction criteria 4 : (1) fulfillment of acute myocardial infarction diagnostic criteria including clinical presentation, electrocardiographic changes, elevated cardiac biomarkers, and/or imaging evidence of new myocardial injury, (2) coronary angiography demonstrating absence of obstructive coronary artery disease, defined as <50% diameter stenosis in all major epicardial vessels, and (3) exclusion of clinically evident alternative diagnoses such as myocarditis, takotsubo cardiomyopathy, or pulmonary embolism. Systematic exclusion criteria comprised: presence of obstructive coronary disease (≥50% stenosis), prior coronary revascularization (percutaneous or surgical), active malignancy under treatment, end-stage renal disease requiring dialysis, established liver cirrhosis of any etiology, excessive alcohol consumption (>30 g/day males, >20 g/day females), or insufficient baseline laboratory data for FIB-4 calculation.
Data Collection and Laboratory Assessment
Comprehensive baseline data collection occurred prospectively at index hospitalization utilizing standardized case report forms. Demographic characteristics, medical history including cardiovascular risk factors (hypertension, diabetes mellitus, dyslipidemia, smoking status), anthropometric measurements, and medication regimens were systematically recorded. All patients underwent standard diagnostic evaluation including 12-lead electrocardiography, transthoracic echocardiography with left ventricular ejection fraction assessment, and coronary angiography.
Laboratory assessments were performed within 24 h of hospital presentation using fasting blood samples processed in the central hospital laboratory. Standard panels included complete blood count with differential, comprehensive metabolic panel, lipid profile, high-sensitivity cardiac troponin, and hepatic function tests (AST, ALT, alkaline phosphatase, total bilirubin, albumin). FIB-4 index was calculated prospectively for each patient using the established formula: (age [years] × AST [U/L])/(platelet count [×109/L] × √ALT [U/L]). Estimated glomerular filtration rate was calculated using the Chronic Kidney Disease Epidemiology Collaboration equation. 14
NAFLD assessment employed a dual approach combining calculated HSI score and ultrasonographic hepatic evaluation. HSI was calculated as: 8 × (ALT/AST ratio) + BMI (kg/m2) + 2 (if diabetes mellitus) + 2 (if female), with values >36 suggestive of hepatic steatosis. 9 Abdominal ultrasonography was performed by experienced radiologists blinded to biomarker results, grading hepatic steatosis severity on a validated 0 to 3 scale: grade 0 (absent), grade 1 (mild), grade 2 (moderate), and grade 3 (severe). Cardiovascular risk factors were defined according to contemporary guideline criteria15,16 hypertension (systolic blood pressure ≥140 mmHg, diastolic ≥90 mmHg, or antihypertensive medication use), diabetes mellitus (fasting glucose ≥126 mg/dL, HbA1c ≥6.5%, or antidiabetic medication use), and dyslipidemia (per current guidelines 16 or lipid-lowering therapy).
Missing Data Assessment and Handling
Missing data patterns were assessed for all study variables. Given the prospective nature of data collection with standardized case report forms, missing data was minimal (<5% for all variables). Patients with missing values for critical variables required for FIB-4 calculation (age, AST, ALT, platelet count) were excluded during initial screening, consistent with our pre-specified exclusion criteria of “insufficient baseline laboratory data for FIB-4 calculation.” For the primary analysis cohort of 472 patients, complete case analysis was employed. Sensitivity analyses comparing baseline characteristics between included and excluded patients demonstrated no significant differences, suggesting that missing data occurred randomly and were unlikely to introduce selection bias. Follow-up was complete through study conclusion for 465 patients (98.5%), with 7 patients (1.5%) censored at last known contact due to loss to follow-up.
Endpoint Definition and Follow-Up Protocol
The pre-specified primary endpoint was a composite of MACE encompassing: (1) cardiac death, (2) recurrent myocardial infarction (re-elevation of cardiac biomarkers with supporting clinical or electrocardiographic features), (3) urgent coronary revascularization (percutaneous or surgical), or (4) hospitalization for acute coronary syndrome, decompensated heart failure, or clinically significant arrhythmia. All potential endpoint events underwent adjudication by 2 independent cardiologists blinded to FIB-4 and NAFLD status, with discordances resolved through consensus discussion.
Structured follow-up assessments occurred at 1-, 3-, 6-, and 12-month post-discharge, then at 6-month intervals thereafter. Follow-up data were collected through scheduled outpatient visits, electronic health record review, direct patient or family contact, and national death registry interrogation. Patients experiencing the primary endpoint were censored at the date of first MACE occurrence. Additional censoring occurred at non-cardiac death, loss to follow-up, or study conclusion (October 31, 2025). Mean follow-up duration was 25.35 months.
Statistical Analysis
Sample size calculation was performed with a priori assuming 20% MACE incidence, 15% prevalence of high FIB-4 (≥2.67), and anticipated hazard ratio of 2.0, yielding required enrollment of 450 patients for 80% power at 2-sided α = .05. Continuous variables are presented as mean ± standard deviation for normally distributed data or median (interquartile range [IQR]) for skewed distributions, assessed via Shapiro-Wilk testing. Categorical variables are reported as frequencies and percentages.
Patients were stratified using standard clinical FIB-4 cutoffs (<1.3, 1.3-2.67, ≥2.67) to facilitate clinical applicability and generalizability. These thresholds are widely validated for hepatic fibrosis assessment and increasingly recognized in cardiovascular risk stratification.5,6
Baseline characteristics were compared across FIB-4 clinical cutoff groups using 1-way analysis of variance (ANOVA) or Kruskal-Wallis test for continuous variables, and chi-square or Fisher’s exact test for categorical variables as appropriate. Kaplan-Meier survival curves stratified by FIB-4 clinical cutoff group and NAFLD severity were constructed with log-rank testing for between-group comparisons (Figure 1).
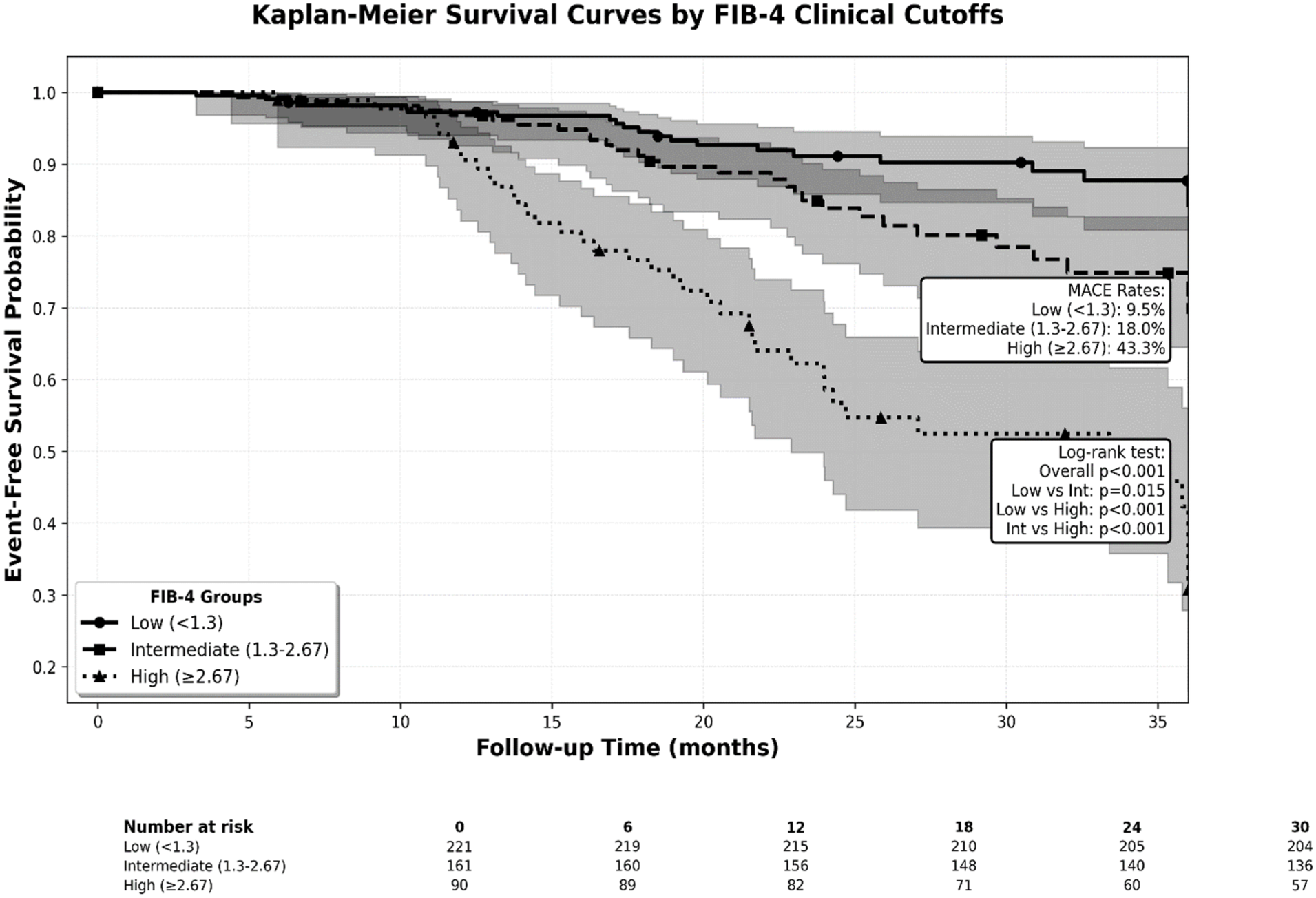
Kaplan-Meier survival curves stratified by FIB-4 index clinical cutoffs. Patients were categorized into 3 groups: low FIB-4 (<1.3, n = 221, solid line), intermediate FIB-4 (1.3-2.67, n = 161, dashed line), and high FIB-4 (≥2.67, n = 90, dotted line). Event-free survival significantly differed across groups (log-rank P < .001 for overall comparison; pairwise comparisons: low vs intermediate P = .015, low vs high P < .001, intermediate vs high P < .001). MACE incidence rates were 9.5% in the low FIB-4 group, 18.0% in the intermediate group, and 43.3% in the high FIB-4 group. Number at risk is displayed at 6-month intervals below the survival curves. Shaded areas represent 95% confidence intervals.
Univariable Cox proportional hazards regression identified variables associated with MACE. The final multivariable model included variables demonstrating P < .10 in univariable analysis or possessing established clinical significance, maintaining an event-per-variable ratio ≥10:1 to prevent overfitting. Proportional hazards assumption was verified through Schoenfeld residual analysis and log-log survival plots. Collinearity was assessed via variance inflation factors (VIF), with values <5 considered acceptable.
Model discrimination was quantified using Harrell’s concordance index (C-index) and time-dependent receiver operating characteristic (ROC) analysis with area under the curve (AUC) calculation (Table 1 and Figure 2). Model calibration was evaluated through visual inspection of calibration plots comparing predicted versus observed event rates across risk deciles. Internal validation employed bootstrap resampling (n = 200 iterations) to derive optimism-corrected performance estimates. Net reclassification improvement (NRI) and integrated discrimination improvement (IDI) assessed incremental prognostic value of adding FIB-4 and HSI to baseline clinical models. For multiple comparisons, Benjamini-Hochberg false discovery rate correction was applied. Statistical significance was defined as 2-tailed P < .05. All analyses utilized R software version 4.3.0 (R Foundation for Statistical Computing, Vienna, Austria) with survival, pROC, rms, and Hmisc packages.
Discriminative Performance of Individual Biomarkers and Composite Prognostic Models.
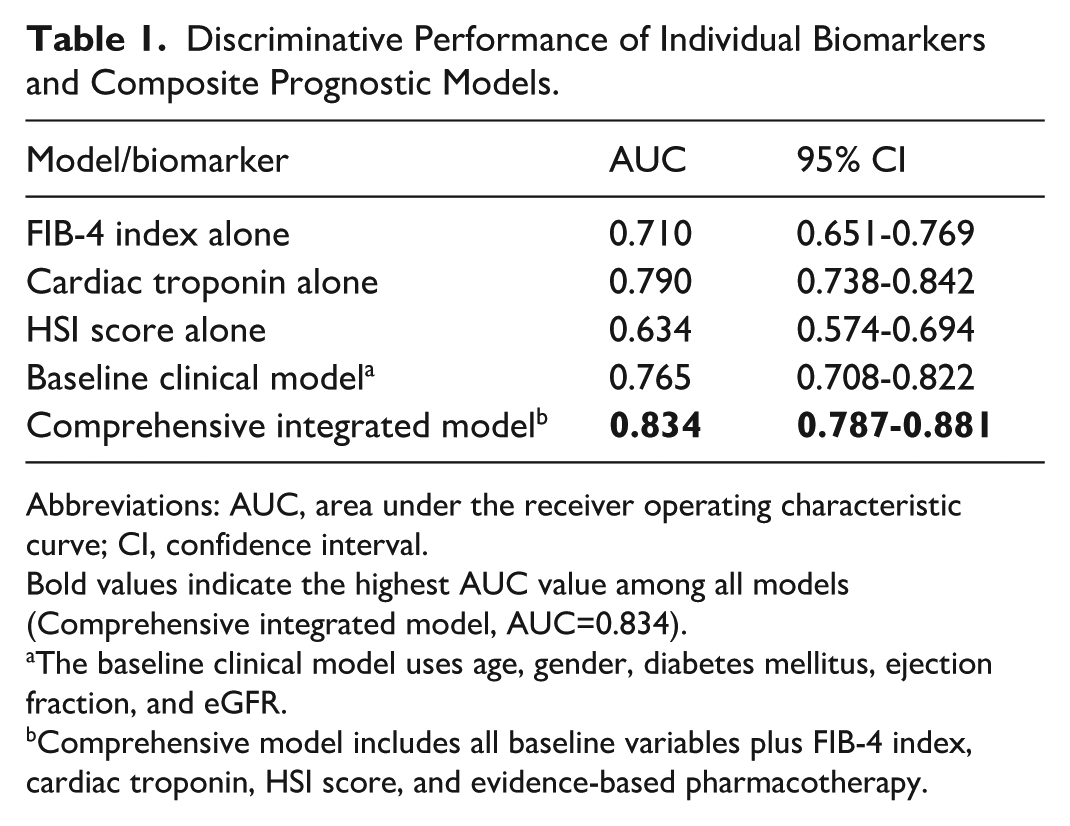
Abbreviations: AUC, area under the receiver operating characteristic curve; CI, confidence interval.
Bold values indicate the highest AUC value among all models (Comprehensive integrated model, AUC=0.834).
The baseline clinical model uses age, gender, diabetes mellitus, ejection fraction, and eGFR.
Comprehensive model includes all baseline variables plus FIB-4 index, cardiac troponin, HSI score, and evidence-based pharmacotherapy.
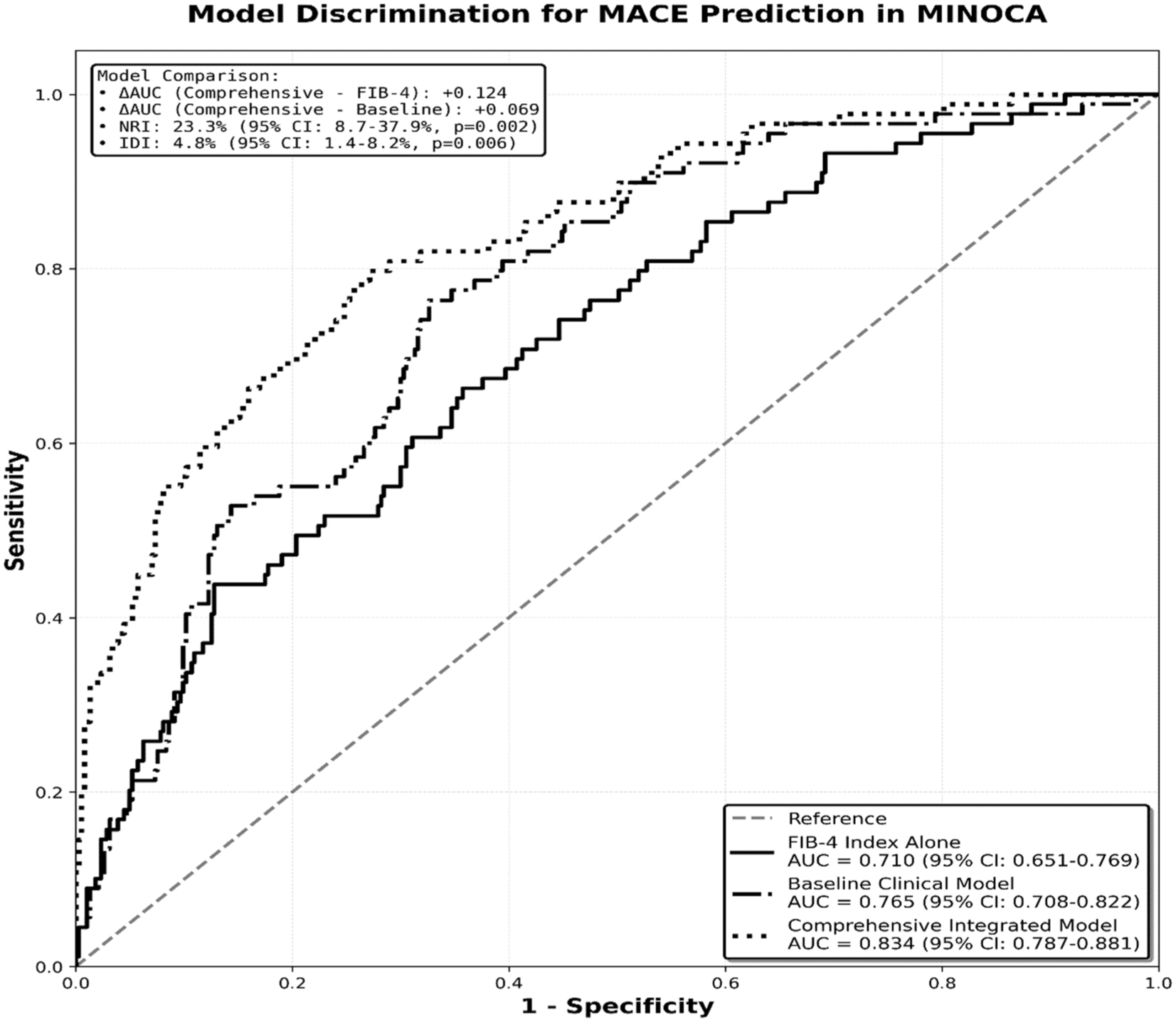
ROC curves comparing discriminative performance of prognostic models. The comprehensive integrated model (dotted line, AUC = 0.834) demonstrated superior discrimination compared to baseline clinical model (dash-dot line, AUC = 0.765) and FIB-4 index alone (solid line, AUC = 0.710). Addition of hepatic biomarkers yielded net reclassification improvement of 23.3% (95% CI: 8.7%-37.9%, P = .002) and integrated discrimination improvement of 4.8% (95% CI: 1.4%-8.2%, P = .006).
Results
Sensitivity and Collinearity Analyses
Assessment of potential age-FIB-4 multicollinearity demonstrated high variance inflation for age (VIF = 27.28), reflecting the mathematical incorporation of age into the FIB-4 formula, whereas FIB-4 itself showed acceptable collinearity (VIF = 2.79). Despite this, the direct correlation between age and FIB-4 was modest (r = 0.115, P = .012). Sensitivity analysis excluding age from the multivariable model confirmed the independent prognostic value of FIB-4 (hazard ratio [HR] 1.45, 95% confidence interval [CI]: 1.30-1.62, P < .001).
Baseline Characteristics
The prospective cohort consisted of 472 MINOCA patients with mean age 58.3 ± 11.3 years and female predominance (54.0%). Traditional cardiovascular risk factor prevalence included hypertension (64.8%), diabetes mellitus (28.0%), dyslipidemia (51.7%), and current smoking (25.0%). Mean body mass index was 28.8 ± 4.4 kg/m2. Baseline laboratory parameters demonstrated median peak cardiac troponin of 374 ng/L (IQR 299 ng/L), mean left ventricular ejection fraction 61.9% ± 8.6%, with preserved systolic function (ejection fraction ≥50%) in 94.1% of patients.
FIB-4 index values ranged from 0.21 to 8.45 with mean 1.77 ± 1.29. Patients were stratified using standard clinical cutoffs: low FIB-4 (<1.3, n = 221, 46.8%), intermediate FIB-4 (1.3-2.67, n = 161, 34.1%), and high FIB-4 (≥2.67, n = 90, 19.1%). Table 2 presents comprehensive baseline characteristics stratified by FIB-4 clinical cutoffs. Higher FIB-4 groups demonstrated progressive age increment. High FIB-4 patients exhibited lower platelet counts, higher AST activity, and reduced estimated glomerular filtration rate compared with the low FIB-4 group. NAFLD assessment revealed prevalence of 57.6% (272 patients) by ultrasonography.
Baseline Characteristics Stratified by Clinical FIB-4 Cutoffs. Data Presented as Mean ± SD, Median (IQR), or n (%).
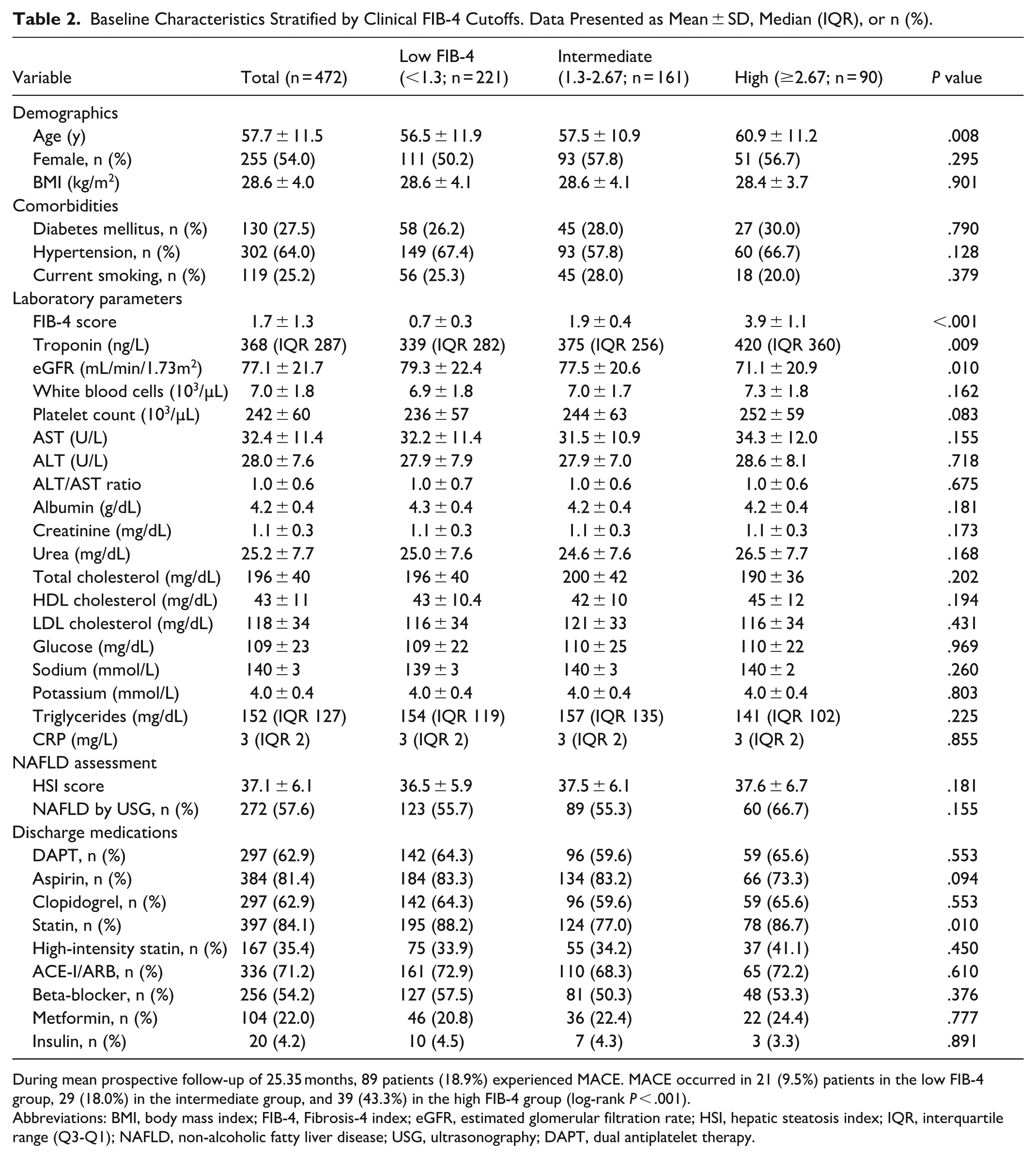
During mean prospective follow-up of 25.35 months, 89 patients (18.9%) experienced MACE. MACE occurred in 21 (9.5%) patients in the low FIB-4 group, 29 (18.0%) in the intermediate group, and 39 (43.3%) in the high FIB-4 group (log-rank P < .001).
Abbreviations: BMI, body mass index; FIB-4, Fibrosis-4 index; eGFR, estimated glomerular filtration rate; HSI, hepatic steatosis index; IQR, interquartile range (Q3-Q1); NAFLD, non-alcoholic fatty liver disease; USG, ultrasonography; DAPT, dual antiplatelet therapy.
Evidence-based pharmacotherapy at discharge included aspirin (82.4%), clopidogrel (63.8%), dual antiplatelet therapy (63.8%), statin therapy (84.1%) with high-intensity statin in 36.7%, angiotensin-converting enzyme inhibitors or angiotensin receptor blockers (71.2%), and beta-blockers (54.2%). Among diabetic patients, 22.0% received metformin and 4.2% insulin therapy.
Clinical Outcomes and Prognostic Associations
During mean prospective follow-up of 25.35 months, 89 patients (18.9%) experienced the primary composite endpoint. Component event frequencies comprised cardiac death 12 (2.5%), recurrent myocardial infarction 23 (4.9%), urgent revascularization 31 (6.6%), and hospitalization for cardiac causes 23 (4.9%). Kaplan-Meier survival analysis demonstrated significant MACE incidence gradient across FIB-4 clinical cutoff groups: clinical cutoff group 1 experienced 22 events (14.0%), clinical cutoff group 2 had 28 events (17.7%), and clinical cutoff group 3 showed 39 events (24.8%; log-rank P = .035; Figure 1).
Univariable Cox regression analysis identified several MACE predictors: FIB-4 score (HR 1.47/unit, 95% CI: 1.23-1.76, P < .001), HSI score (HR 1.03/unit, 95% CI: 1.01-1.05, P = .012), advancing age (HR 1.05/year, 95% CI: 1.02-1.08, P < .001), diabetes mellitus (HR 1.68, 95% CI: 1.05-2.69, P = .030), reduced left ventricular systolic function defined as ejection fraction <50% (HR 2.87, 95% CI: 1.58-5.21, P = .001), and impaired renal function with eGFR <60 mL/min/1.73 m2 (HR 2.14, 95% CI: 1.35-3.39, P = .001).
Multivariable Cox proportional hazards modeling, adjusting for age, gender, diabetes mellitus, left ventricular ejection fraction, renal function, HSI score, and evidence-based pharmacotherapy, confirmed FIB-4 index as an independent MACE predictor (adjusted HR 1.43/unit increase, 95% CI: 1.18-1.73, P < .001). Other independent predictors in the final model included age (adjusted HR 1.04/year, 95% CI: 1.01-1.07, P = .008), ejection fraction <50% (adjusted HR 2.31, 95% CI: 1.25-4.27, P = .007), and eGFR <60 mL/min/1.73 m2 (adjusted HR 1.71, 95% CI: 1.06-2.76, P = .028). Table 3 presents complete multivariable analysis results. displays these results as a forest plot for visual clarity.
Multivariable Cox Proportional Hazards Regression Analysis for MACE.
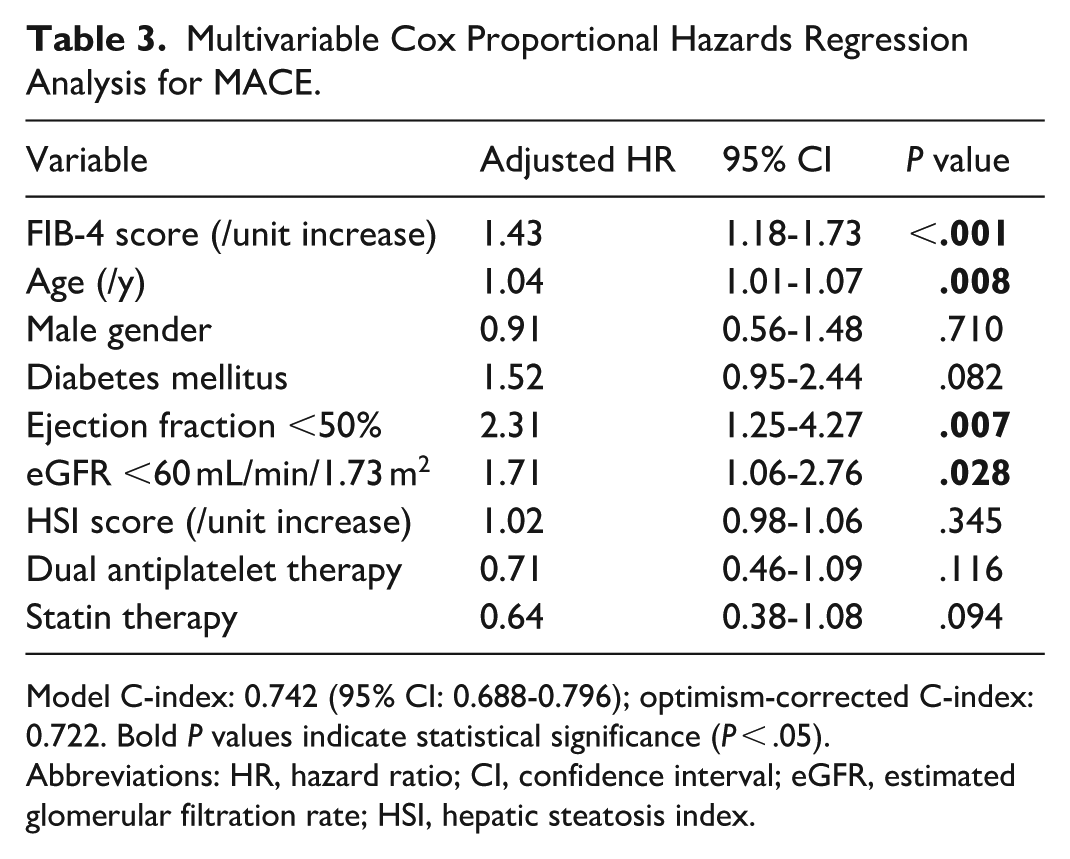
Model C-index: 0.742 (95% CI: 0.688-0.796); optimism-corrected C-index: 0.722. Bold P values indicate statistical significance (P < .05).
Abbreviations: HR, hazard ratio; CI, confidence interval; eGFR, estimated glomerular filtration rate; HSI, hepatic steatosis index.
Ultrasonographic NAFLD severity demonstrated a dose-dependent relationship with MACE incidence. Using absent NAFLD as the reference category, adjusted hazard ratios were: mild NAFLD 1.20 (95% CI: 0.72-2.01, P = .484), moderate NAFLD 1.55 (95% CI: 0.88-2.73, P = .126), and severe NAFLD 2.36 (95% CI: 1.23-4.53, P = .010), with statistically significant linear trend (P-for-trend = .008). Patients exhibiting NAFLD by both HSI calculation and ultrasonographic evaluation demonstrated 21.5% MACE incidence versus 8.3% among those without NAFLD by either modality (adjusted HR 3.15, 95% CI: 1.52-6.53, P = .002).
Prognostic Model Performance and Clinical Utility
Discriminative performance of individual biomarkers and composite models was assessed through time-dependent receiver operating characteristic analysis (Table 1 and Figure 2). FIB-4 index alone achieved area under the curve (AUC) 0.710 (95% CI: 0.651-0.769), cardiac troponin demonstrated AUC 0.790 (95% CI: 0.738-0.842), and HSI score showed AUC 0.634 (95% CI: 0.574-0.694). A comprehensive integrated model incorporating FIB-4, troponin, HSI, age, traditional cardiovascular risk factors, and guideline-directed medical therapy attained superior discrimination with AUC 0.834 (95% CI: 0.787-0.881), significantly outperforming individual biomarkers (P < .001 vs FIB-4 alone, P = .023 vs troponin alone).
Net reclassification improvement analysis quantified the incremental prognostic value of adding hepatic biomarkers (FIB-4 and HSI) to a baseline clinical model encompassing age, gender, diabetes mellitus, left ventricular ejection fraction, and renal function. The enhanced model incorporating hepatic biomarkers appropriately reclassified 15.2% of patients experiencing MACE to higher-risk categories and 8.1% of patients without MACE to lower-risk categories, yielding total net reclassification improvement 23.3% (95% CI: 8.7%-37.9%, P = .002). Integrated discrimination improvement was 4.8% (95% CI: 1.4%-8.2%, P = .006). Bootstrap internal validation demonstrated model robustness with optimism-corrected C-index 0.722, confirming minimal optimism and excellent generalizability.
Discussion
This prospective observational cohort study of 472 MINOCA patients followed for a mean of 25.35 months demonstrates that the FIB-4 index provides independent prognostic information for major adverse cardiovascular events, with a 43% incremental risk/unit increase after comprehensive multivariable adjustment (Table 3). NAFLD severity, particularly advanced hepatic steatosis, confers substantial additional cardiovascular risk. Integration of these readily available hepatic biomarkers with conventional clinical parameters yields excellent discrimination (Table 1 and Figure 2) and clinically meaningful risk reclassification, supporting their potential utility in contemporary MINOCA risk stratification.
The observed independent association between FIB-4 index and MACE (adjusted HR 1.43) demonstrates consistency with accumulating evidence from broader acute coronary syndrome populations, where comparable effect magnitudes (HR 1.3-1.8) have been reported.17,18 Our analysis extends this literature by focusing specifically on MINOCA, a population where traditional atherosclerotic burden assessment provides limited discriminatory value and alternative biomarkers assume heightened importance. The Kaplan-Meier curves (Figure 1) clearly demonstrate the prognostic stratification achieved through FIB-4 clinical cutoff groups, with statistically significant separation between risk groups (log-rank P = .035). The demonstrated dose-response relationship between NAFLD severity and MACE incidence (P-for-trend = .008) reinforces growing recognition of NAFLD as an independent cardiovascular risk factor.19,20 The 2.36-fold adjusted risk associated with severe hepatic steatosis approximates risk magnitudes conferred by established major cardiovascular risk factors.
Several plausible biological mechanisms may explain these associations. Hepatic fibrosis and steatosis promote systemic inflammation through increased production of pro-inflammatory cytokines (interleukin-6, tumor necrosis factor-alpha, C-reactive protein), which may contribute to coronary microvascular dysfunction and vasospastic tendency—key pathophysiological mechanisms underlying MINOCA.21,22 Additionally, NAFLD-associated metabolic perturbations including insulin resistance, atherogenic dyslipidemia characterized by increased small dense LDL particles, and prothrombotic state mediated by elevated plasminogen activator inhibitor-1 may accelerate endothelial dysfunction.23,24 The FIB-4 index may serve as a composite indicator of chronic inflammatory burden and metabolic dysregulation that collectively modulate cardiovascular risk independent of traditional factors.
From a practical perspective, both FIB-4 index and HSI calculated from routine admission laboratory parameters, may enable immediate risk stratification without specialized testing or incremental cost. Our comprehensive integrated model achieving AUC 0.834 (Table 1) compares favorably with established acute coronary syndrome risk scores including the Thrombolysis in Myocardial Infarction (TIMI) risk score (AUC 0.65-0.75) and Global Registry of Acute Coronary Events (GRACE) risk score (AUC 0.75-0.85), suggesting credible discriminative performance in the MINOCA population.25,26 The 23.3% net reclassification improvement (Table 1) directly translates to enhanced clinical decision-making capability. Bootstrap internal validation demonstrated model robustness with optimism-corrected C-index 0.722 (Table 3), confirming minimal optimism and excellent generalizability.
These findings have important therapeutic implications. MINOCA patients with elevated FIB-4 index (≥1.73) or moderate-to-severe NAFLD may benefit from intensified secondary prevention strategies including aggressive lifestyle modification targeting hepatic steatosis, optimization of metabolic risk factors, lower LDL-cholesterol targets, and consideration of medications with cardio-metabolic benefits such as glucagon-like peptide-1 (GLP-1) receptor agonists or receptor agonists or sodium-glucose cotransporter-2 (SGLT2) inhibitors in appropriate candidates.27,28 Given the cardiovascular benefits of statins and their potential favorable effects on hepatic steatosis, optimization of statin therapy appears particularly justifiable in this population.29,30 Current guidelines indicate that statins are safe and should not be withheld in patients with non-alcoholic fatty liver disease (NAFLD), including those with mildly to moderately elevated liver enzymes, as they reduce cardiovascular risk without worsening hepatic outcomes. 31
The present findings carry particular significance for MINOCA patients. First, MINOCA patients lack epicardial coronary disease amenable to revascularization. Second, the underlying pathophysiology involves microvascular dysfunction and coronary vasospasm rather than obstructive atherosclerosis. Third, NAFLD prevalence (57.6%) in our MINOCA cohort exceeds general population estimates, suggesting enhanced importance of the hepato-cardiac axis. Importantly therapeutic implications in MINOCA differ from obstructive coronary artery disease, as management relies predominantly on intensive medical therapy and metabolic risk modification rather than mechanical revascularization strategies. FIB-4 and NAFLD assessment may therefore identify MINOCA patients requiring more aggressive metabolic risk modification and closer follow-up.
Several limitations warrant acknowledgment. First, the observational design precludes definitive causal inference. Second, single-center enrollment may affect generalizability, although our patient characteristics (Table 2) align with published MINOCA cohorts. Third, NAFLD assessment relied on HSI and ultrasonography rather than reference-standard magnetic resonance imaging. Fourth, mean follow-up duration of 25.35 months may not fully characterize long-term associations.32,33 Potential ethnic and regional differences in NAFLD prevalence and metabolic risk profiles should be considered when extrapolating these findings to other populations. Future research should focus on external validation in multicenter cohorts, mechanistic studies elucidating causal pathways, and interventional trials testing whether therapeutic strategies targeting hepatic pathology improve cardiovascular outcomes in MINOCA patients.
Emerging evidence suggests that NAFLD is closely associated with increased epicardial and perivascular adipose tissue, which may promote coronary microvascular dysfunction and vascular inflammation through paracrine and inflammatory pathways, thereby contributing to adverse cardiovascular outcomes. 34
Conclusions
In this prospective cohort of 472 MINOCA patients followed for a mean duration of 25.35 months, the FIB-4 index emerged as an independent predictor of major adverse cardiovascular events with 43% increased risk/unit increment after comprehensive multivariable adjustment. NAFLD severity provided complementary prognostic information, with severe hepatic steatosis conferring more than 2-fold elevated risk. Integration of these hepatic biomarkers with traditional cardiovascular risk factors yielded excellent discrimination (AUC 0.834) and substantial net reclassification improvement (23.3%), significantly enhancing risk stratification beyond conventional clinical parameters. These findings highlight mechanistic convergence of hepatic and cardiovascular pathophysiology in MINOCA and support incorporating readily available, cost-effective hepatic assessments into routine prognostic evaluation. The immediate availability and minimal incremental cost of FIB-4 and HSI calculation from standard laboratory data facilitate widespread clinical implementation. Patients with elevated FIB-4 index or advanced NAFLD represent a high-risk subgroup potentially benefiting from intensive monitoring, aggressive evidence-based pharmacotherapy, and targeted metabolic interventions despite absence of obstructive coronary disease. These results warrant prospective multicenter validation and investigation of whether hepatic-targeted therapeutic interventions translate into cardiovascular event reduction in MINOCA populations.
Footnotes
Acknowledgements
We thank the nursing staff and research coordinators at İzmir City Hospital Department of Cardiology for their assistance with patient recruitment and data collection. We acknowledge the contribution of the radiology department to perform hepatic ultrasonography evaluations. We also thank Prof. Dr. Cenk Sarı for his valuable contributions.
Ethical Considerations
The Ethical Considerations section includes both ethics approval and consent information. Ethics approval was obtained from University of Health Sciences, İzmir Tepecik Training and Research Hospital (decision number: 2022/13/4, September 7, 2022).
Consent to Participate
Individual informed consent was waived by the ethics committee due to the observational prospective nature of the study.
Author Contributions
M.K. conceived and designed the study, performed statistical analyses, and drafted the manuscript. R.B. contributed to data acquisition and interpretation, particularly radiological assessments, and critically revised the manuscript for important intellectual content. Both authors approved the final version of the manuscript and agree to be accountable for all aspects of the work.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was conducted as part of routine clinical practice and quality improvement activities at İzmir City Hospital.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated and analyzed during the current study are available from the corresponding author upon reasonable request. Due to ethical restrictions and patient privacy considerations, raw patient-level data cannot be made publicly available. Aggregated data supporting the findings of this study are included within the article and its supplementary materials.