
Abstract
Aortic arch atherosclerosis is a marker of systemic vascular disease and may contribute to adverse cardiovascular outcomes. The modified Glasgow Prognostic Score (mGPS), reflecting systemic inflammation, may influence plaque vulnerability. The present study aimed to investigate the relationship between aortic arch calcification (AAC), aortic arch morphology (AAM), and mGPS, and to evaluate their prognostic significance for major adverse cardiovascular events (MACE). A total of 516 patients who underwent computed tomography angiography (CTA) were retrospectively analyzed. AAC was categorized as none, small, or considerable, and AAM as none, smooth, ulcerated, or protruding. MACE was defined as all-cause mortality, myocardial infarction, or stroke. Kaplan-Meier survival analysis and Cox proportional hazards regression were used to identify predictors of MACE. During a median follow-up 42 MACE occurred. Event-free survival progressively declined with increasing AAC and AAM severity (log-rank P < .001 for both). In multivariable Cox analysis, small and considerable AAC independently predicted MACE (P = .007 and P = .005). Similarly, smooth, ulcerated, and protruding plaques were associated with significantly higher risk (all P < .01). Although mGPS correlated with plaque complexity, it was not an independent predictor of MACE. CTA-based assessment of aortic arch features may enhance long-term cardiovascular risk stratification.
Keywords
Introduction
Aortic arch atherosclerosis, characterized by calcification and complex plaque morphology, has been increasingly recognized as a marker of systemic vascular pathology and an important contributor to embolic events.1 -3 With the widespread use of computed tomography angiography (CTA), the detection of both aortic arch calcification (AAC) and plaque morphology has become more accessible and reliable, allowing for improved risk stratification beyond traditional cardiovascular risk factors.4 -7
Inflammation is a key driver in both the initiation and destabilization of atherosclerotic plaques. The modified Glasgow Prognostic Score (mGPS), a composite index derived from serum albumin and C-reactive protein (CRP) levels, reflects systemic inflammatory status and has been established as a prognostic indicator across multiple chronic inflammatory and malignant conditions.8 -12 However, its role in cardiovascular disease, particularly in relation to aortic arch atherosclerotic burden, remains underexplored.
Recent evidence suggests that aortic arch pathology not only reflects cumulative atherosclerotic burden but also correlates with systemic inflammatory status and clinical outcomes.13,14 Complex plaque morphology, especially ulcerated or protruding lesions, has been linked to embolic events and adverse cardiovascular prognosis.13 -15 Nevertheless, the prognostic relevance of combining imaging-derived markers such as AAC and morphology with systemic inflammatory indices such as mGPS has not been clearly defined.
The relationship between AAC and morphology with systemic inflammation, evaluated using the mGPS, as well as their prognostic value for predicting major adverse cardiovascular events (MACE) during follow-up, was assessed in the present study. By integrating morphologic, calcific, and inflammatory parameters, we sought to identify imaging and laboratory markers that could enhance long-term cardiovascular risk stratification in patients undergoing cardiac CTA.
Methods
Study Population
Consecutive patients who underwent clinically indicated cardiac and thoracic computed tomography (CT) imaging between February 2021 and March 2023 were included in this retrospective observational study. Cardiac CTA was performed for standard clinical indications, including evaluation of suspected coronary artery disease, atypical chest pain, and cardiovascular risk assessment in patients with intermediate pre-test probability, according to institutional practice. All scans were performed at a single tertiary care center. Adult patients (≥18 years) were eligible if CT images provided adequate visualization of the ascending aorta and the aortic arch. Patients with prior aortic interventions (e.g., stent grafts or surgical repairs), known aortic dissection, or poor image quality due to motion or artifact. The exclusion criteria encompassed age < 18 years, pregnancy, and incomplete clinical data. Patients with chronic kidney disease (Cockcroft-Gault 16 eGFR <60 mL/min/1.73 m2), hepatic failure (ALT or AST >3 × upper limit of normal), active malignancy, acute coronary syndrome, heart failure with reduced ejection fraction, ongoing infection, malnutrition, or autoimmune/autoinflammatory disease were also excluded. The final cohort comprised 516 patients. Baseline demographic information, conventional cardiovascular risk factors, laboratory findings, and current medications were obtained from the hospital’s electronic medical record system. The mGPS was calculated based on serum C-reactive protein (CRP) and albumin levels. Patients with elevated CRP (>1 mg/dL) and hypoalbuminemia (serum albumin <3.5 g/dL) were assigned a score of 2. Those with elevated CRP alone or hypoalbuminemia alone were assigned a score of 1, while patients with normal CRP and albumin levels were assigned a score of 0. Patients were stratified into three categories based on the mGPS. All-cause mortality, myocardial infarction (nonfatal), or stroke were defined as MACE. Clinical events were identified through review of hospital records and follow-up visits. The median duration of follow-up was 32 months, with an interquartile range of 13-44 months. The flow chart summarizing patient selection and follow-up is presented in Figure 1.
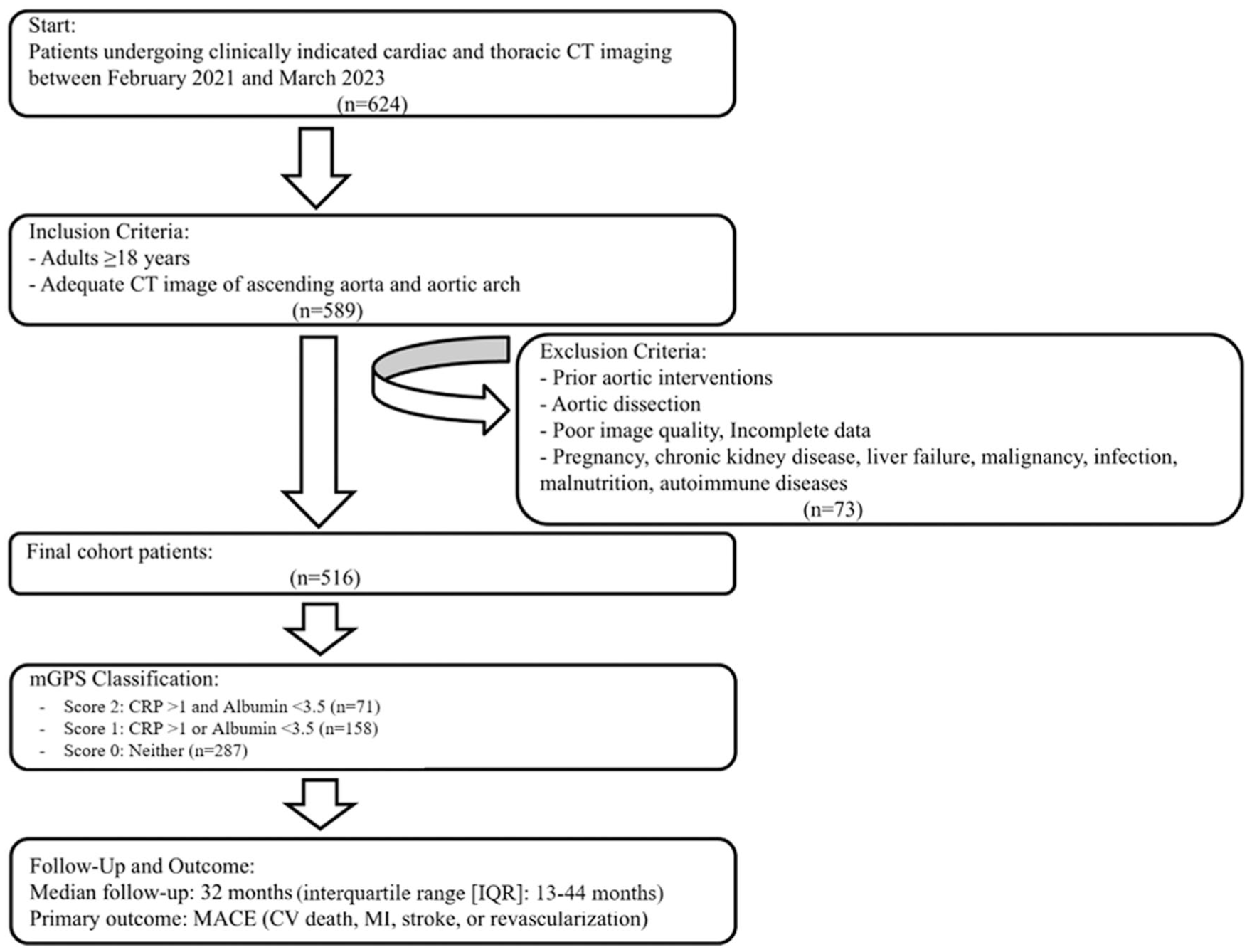
Study flow chart summarizing patient inclusion, exclusion, mGPS classification, and follow-up for major adverse cardiovascular events (MACE).
Ethical Considerations
The authors accept full accountability for the accuracy and reliability of the study, ensuring that any issues regarding data integrity or validity are carefully reviewed and resolved. In accordance with the ethical standards set forth in the Declaration of Helsinki and its subsequent revisions, this research received approval from the Corporate Ethics Committee of Medline Hospitals (Approval No: 05; Date: May 20, 2025). Owing to the retrospective design, a waiver of informed consent was obtained.
Computed Tomography Angiography (CTA) and Aortic Arch Assessment
CTA was performed using a 64-detector Optima CT660 scanner (GE Healthcare, Chicago, IL, USA). An iodinated contrast medium (iobitridol, Xenetix 350; Guerbet, France) was administered (100 mL) intravenously through an 18-gauge antecubital catheter at a rate of 5.5 mL/s, immediately followed by a 35 mL saline chaser. Acquisition proceeded in the craniocaudal orientation during a mid-inspiratory breath-hold under ECG gating. The scanning protocol consisted of 120 kV tube voltage, 300 mA tube current, and 0.4-second gantry rotation time. Reconstruction was performed at the optimal cardiac phase using 0.625-mm slices and 0.3-mm intervals, and images were analyzed on a dedicated Volume Viewer 4.6 workstation (GE Healthcare, Chicago, IL).
The aortic arch was systematically assessed for both calcification and plaque morphology using axial and multiplanar reformatted images. Morphological classification was based on visual characteristics and categorized into four groups: None: normal contour without irregularities, smooth: intimal thickening without surface disruption, ulcerated: plaques with localized intimal breaks or crater-like depressions, and protruding: plaques extending into the lumen ≥4 mm (Figure 2).17,18 Calcification severity was stratified into three categories based on extent and density: None: no visible calcification, small: focal calcification limited to a single region, and considerable: confluent calcifications involving extensive portions of the arch (Figure 3). 19 Two experienced radiologists, blinded to all clinical data, independently evaluated the CT images. Disagreements were resolved by consensus.
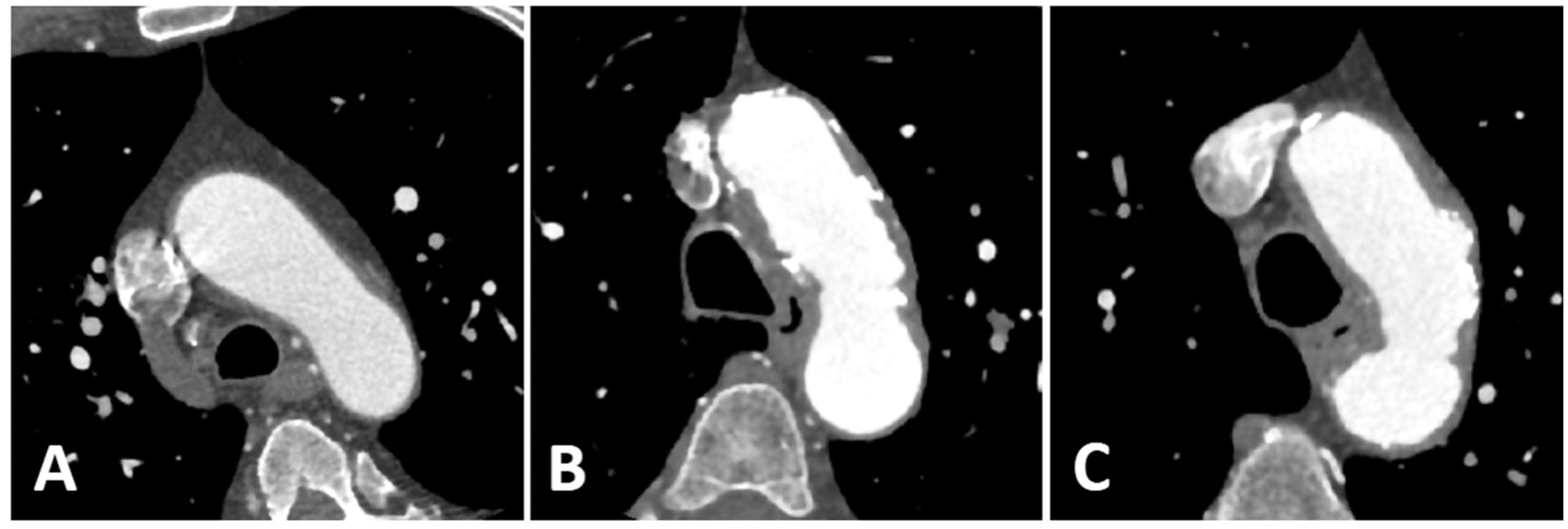
Representative computed tomography angiography (CTA) images demonstrating the classification of aortic arch plaque morphology. The figure includes three panels illustrating the distinct morphological categories: (A) smooth intimal thickening without surface disruption, (B) ulcerated plaque characterized by localized intimal breaks or crater-like depressions, and (C) protruding plaque extending into the lumen ≥4 mm. Images were obtained using multiplanar reformatted CTA reconstructions.
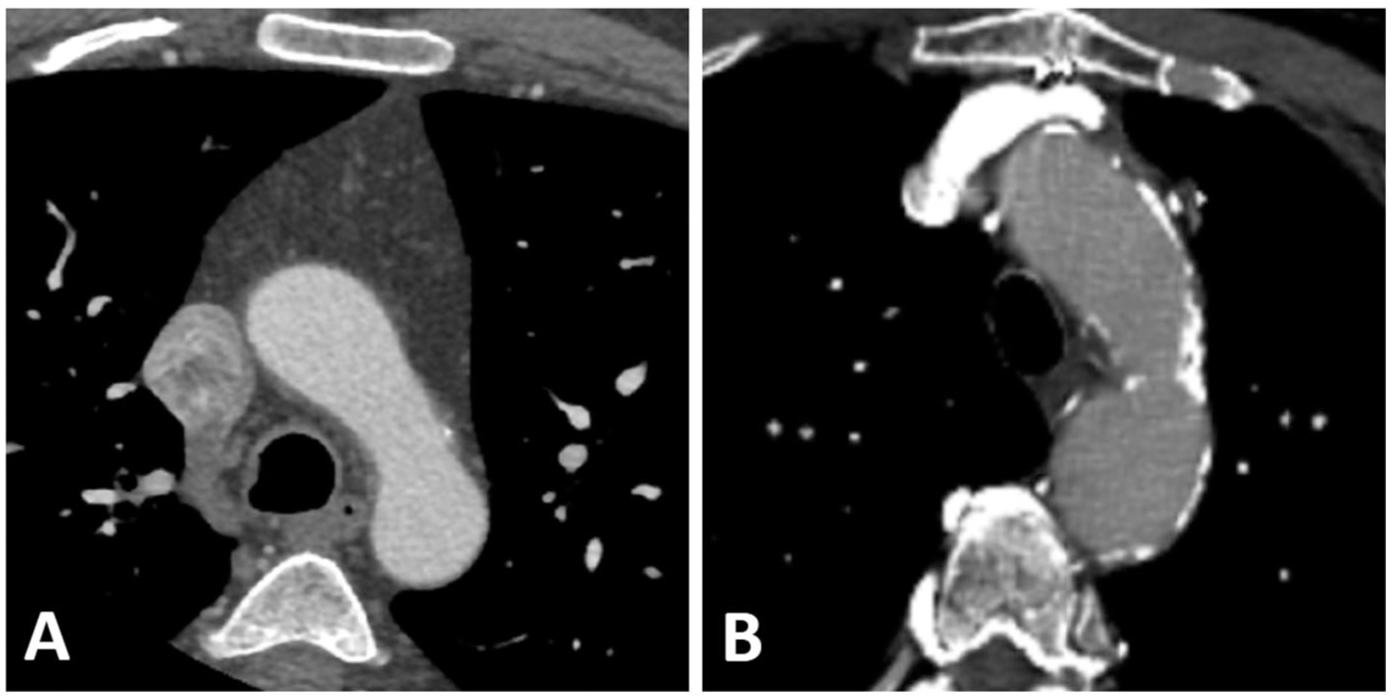
Representative computed tomography angiography (CTA) images demonstrating the classification of aortic arch calcification. The figure shows two panels illustrating calcification severity: (A) small, focal calcification limited to a single region, and (B) considerable, confluent calcifications involving extensive portions of the aortic arch. Images were acquired using axial and multiplanar reformatted CTA views.
Statistical Analysis
Continuous variables were summarized as mean ± standard deviation or median (interquartile range) according to the Shapiro-Wilk test, while categorical variables were expressed as frequencies (%) and compared using the chi-square or Fisher’s exact test. Between-group comparisons for continuous data used one-way ANOVA or the Kruskal-Wallis test as appropriate. The mGPS was analyzed as an ordinal categorical variable (scores 0-2), in accordance with its original definition. Univariable ordinal logistic regression identified factors associated with increasing AAC and aortic arch morphology (AAM); variables with P < .10 or clinical relevance were entered into multivariable models. Event-free survival was estimated by the Kaplan-Meier method, and subgroup differences were assessed with the log-rank test. Predictors of MACE were evaluated by Cox proportional hazards regression, reporting hazard ratios (HRs) with 95% confidence intervals (CI). The proportional hazards assumption was evaluated using log-log survival plots and was not violated. To reduce model overfitting, multivariable Cox regression models were constructed using a limited number of clinically relevant covariates identified a priori and through univariable analysis. All analyses were performed using IBM SPSS Statistics v22 (IBM Corp., Armonk, NY, USA), and a 2-tailed P < .05 was considered statistically significant.
Results
A total of 516 patients (mean age 57.8 ± 10.8 years, 39.5% female) were included in the final analysis. Baseline characteristics stratified by AAC and AAM are presented in Tables 1 and 2, respectively.
Baseline Characteristics of the Study Population According to the Degree of Aortic Arch Calcification.
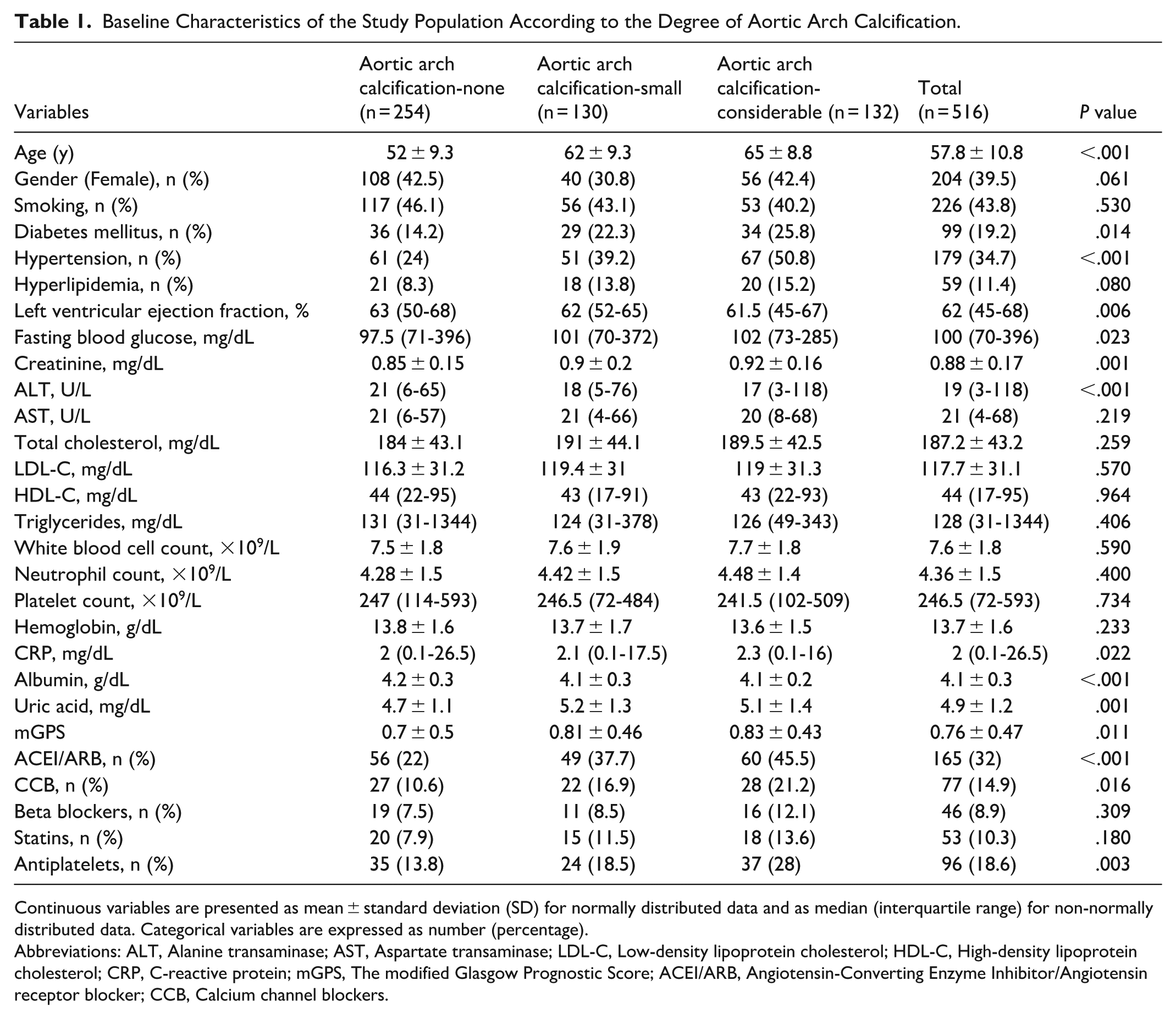
Continuous variables are presented as mean ± standard deviation (SD) for normally distributed data and as median (interquartile range) for non-normally distributed data. Categorical variables are expressed as number (percentage).
Abbreviations: ALT, Alanine transaminase; AST, Aspartate transaminase; LDL-C, Low-density lipoprotein cholesterol; HDL-C, High-density lipoprotein cholesterol; CRP, C-reactive protein; mGPS, The modified Glasgow Prognostic Score; ACEI/ARB, Angiotensin-Converting Enzyme Inhibitor/Angiotensin receptor blocker; CCB, Calcium channel blockers.
Baseline Characteristics of the Study Population According to Aortic Arch Plaque Morphology Categories.
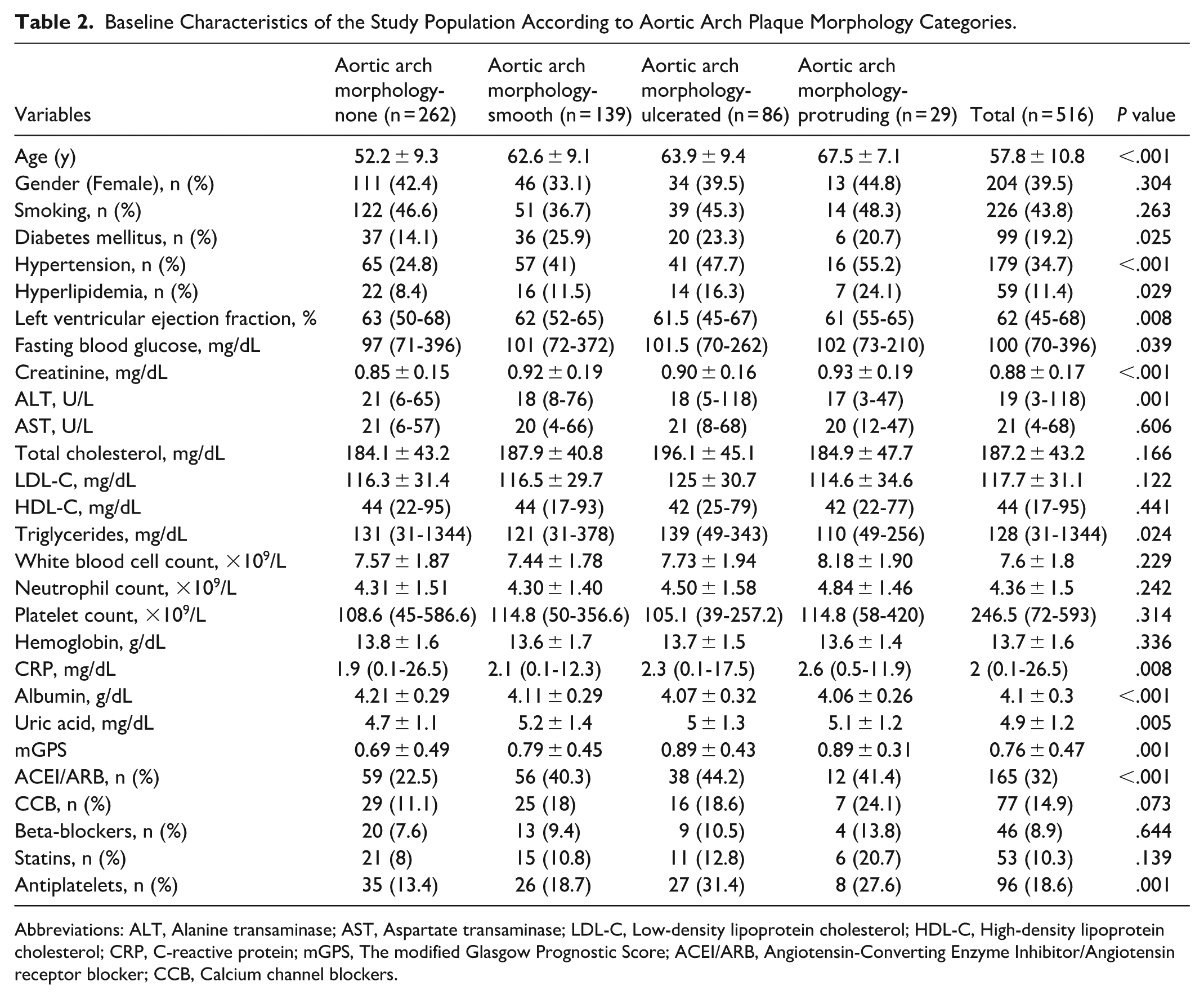
Abbreviations: ALT, Alanine transaminase; AST, Aspartate transaminase; LDL-C, Low-density lipoprotein cholesterol; HDL-C, High-density lipoprotein cholesterol; CRP, C-reactive protein; mGPS, The modified Glasgow Prognostic Score; ACEI/ARB, Angiotensin-Converting Enzyme Inhibitor/Angiotensin receptor blocker; CCB, Calcium channel blockers.
Patients were categorized into three groups based on the degree of AAC: none (n = 254, 49.2%), small (n = 130, 25.2%), and considerable (n = 132, 25.6%). The prevalence of cardiovascular risk factors, including hypertension and diabetes mellitus, progressively increased with higher calcification severity. Specifically, hypertension was observed in 24% of patients without calcification and increased to 50.8% in those with considerable calcifications (P < .001). Similarly, the proportion of diabetes mellitus rose from 14.2% in the non-calcified group to 25.8% in the considerable calcification group (P = .014). Mean serum creatinine and uric acid levels were significantly higher in patients with considerable calcifications (both P ≤ .001). The mGPS also demonstrated a modest but significant trend across calcification categories (P = .011).
In multivariable ordinal logistic regression analysis (Table 3), age (OR: 1.11, 95% CI: 1.08-1.13, P < .001) and hypertension (OR: 1.69, 95% CI: 1.15-2.48, P = .007) were independently associated with increasing calcification severity.
Univariable and Multivariable Ordinal Logistic Regression Analysis for Predictors of Aortic Arch Calcification Severity.
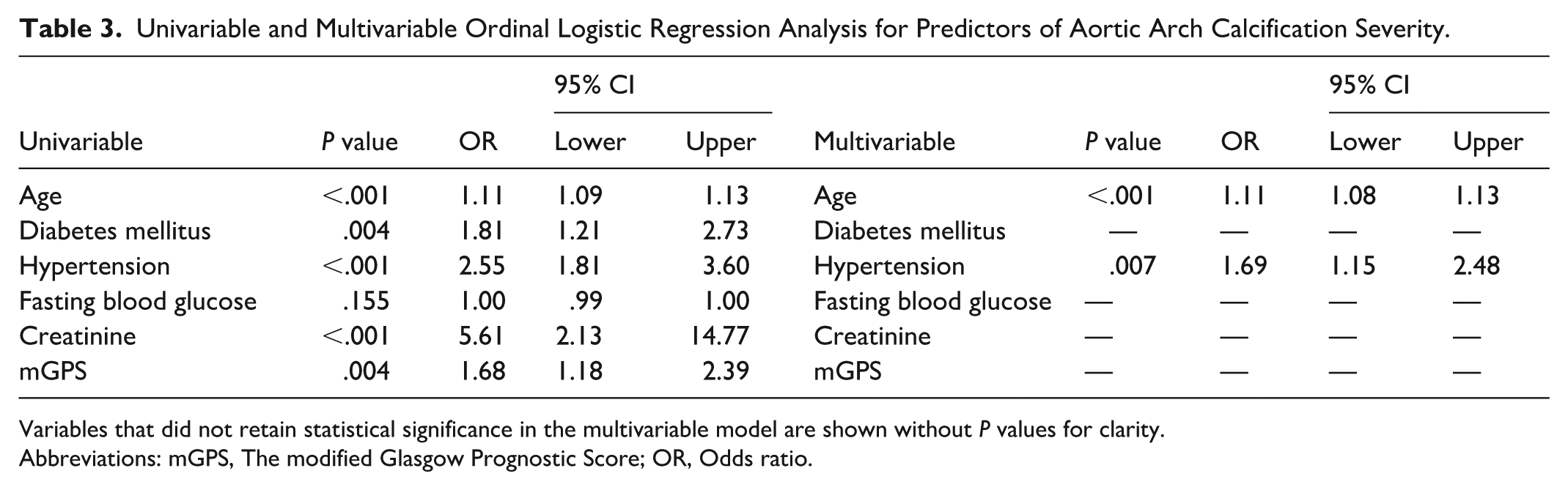
Variables that did not retain statistical significance in the multivariable model are shown without P values for clarity.
Abbreviations: mGPS, The modified Glasgow Prognostic Score; OR, Odds ratio.
Assessment of plaque morphology revealed that 262 patients (50.8%) had no detectable plaque, 139 (26.9%) had smooth plaques, 86 (16.7%) had ulcerated plaques, and 29 (5.6%) exhibited protruding plaques. Increasing plaque complexity was associated with older age (mean age ranging from 52.2 ± 9.3 years in the “none” group to 67.5 ± 7.1 years in the “protruding” group, P < .001). The prevalence of hypertension increased significantly across morphology categories, from 24.8% in patients without plaques to 55.2% in those with protruding plaques (P < .001). Serum creatinine and CRP levels were also higher in patients with advanced plaque morphology (P< .001 and P = .008, respectively).
In univariable regression analyses (Table 4), age, hypertension, hyperlipidemia, creatinine, and mGPS were significantly associated with more advanced plaque morphology. After adjustment for confounders in multivariable ordinal logistic regression, age (OR: 1.10, 95% CI: 1.08-1.12, P < .001), hypertension (OR: 1.48, 95% CI: 1.01-2.18, P = .045), hyperlipidemia (OR: 2.04, 95% CI: 1.17-3.54, P = .011), and mGPS (OR: 1.58, 95% CI: 1.07-2.34, P = .021) remained significant independent predictors of plaque morphology severity.
Univariable and Multivariable Ordinal Logistic Regression Analysis for Predictors of Aortic Arch Plaque Morphology Severity.
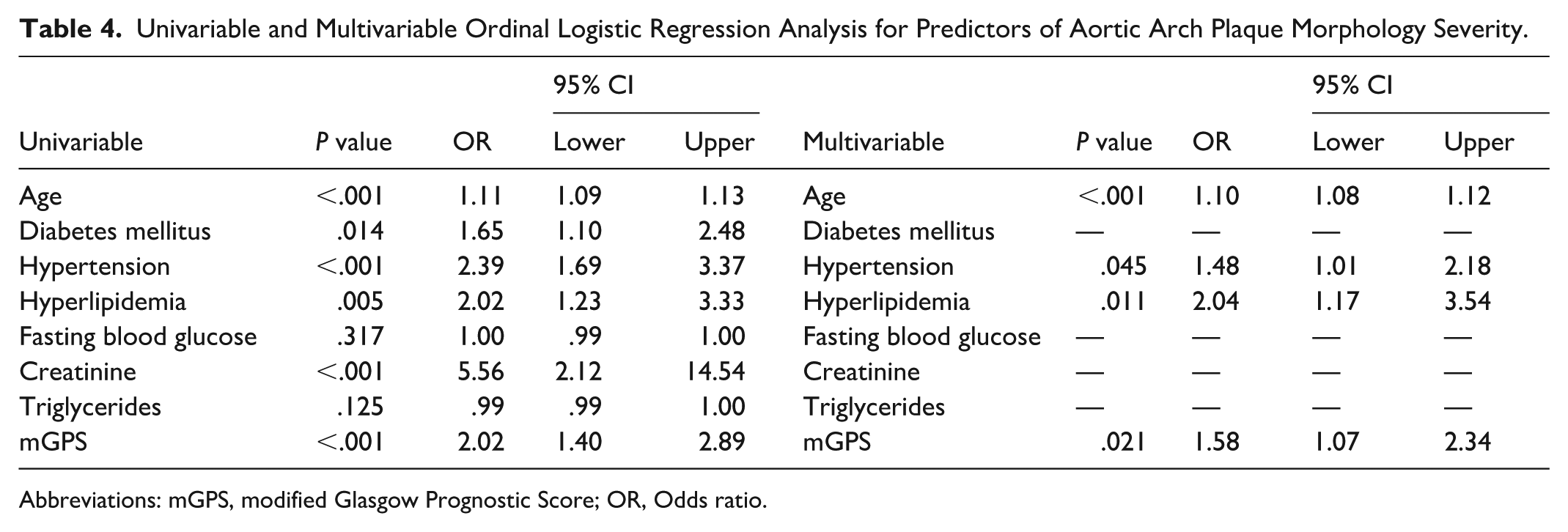
Abbreviations: mGPS, modified Glasgow Prognostic Score; OR, Odds ratio.
During a median follow-up of 32 months, 42 MACE occurred. Kaplan-Meier survival analysis demonstrated a stepwise reduction in event-free survival across AAC categories (log-rank P < .001; Figure 4). In univariable Cox regression, both small and considerable AAC were strongly associated with higher risk of MACE (HR 7.40 [95% CI 2.73-20.04], P < .001; and HR 8.54 [3.21-22.70], P < .001, respectively). After adjustment for age, diabetes mellitus, hypertension, hyperlipidemia, sex, creatinine, and mGPS, AAC remained an independent predictor of adverse outcomes. Compared with patients without visible calcification, those with small and considerable calcifications had 4.3-fold and 4.6-fold higher risks of MACE, respectively (HR 4.26 [1.48-12.26], P = .007; HR 4.61 [1.60-13.31], P = .005; Table 5).
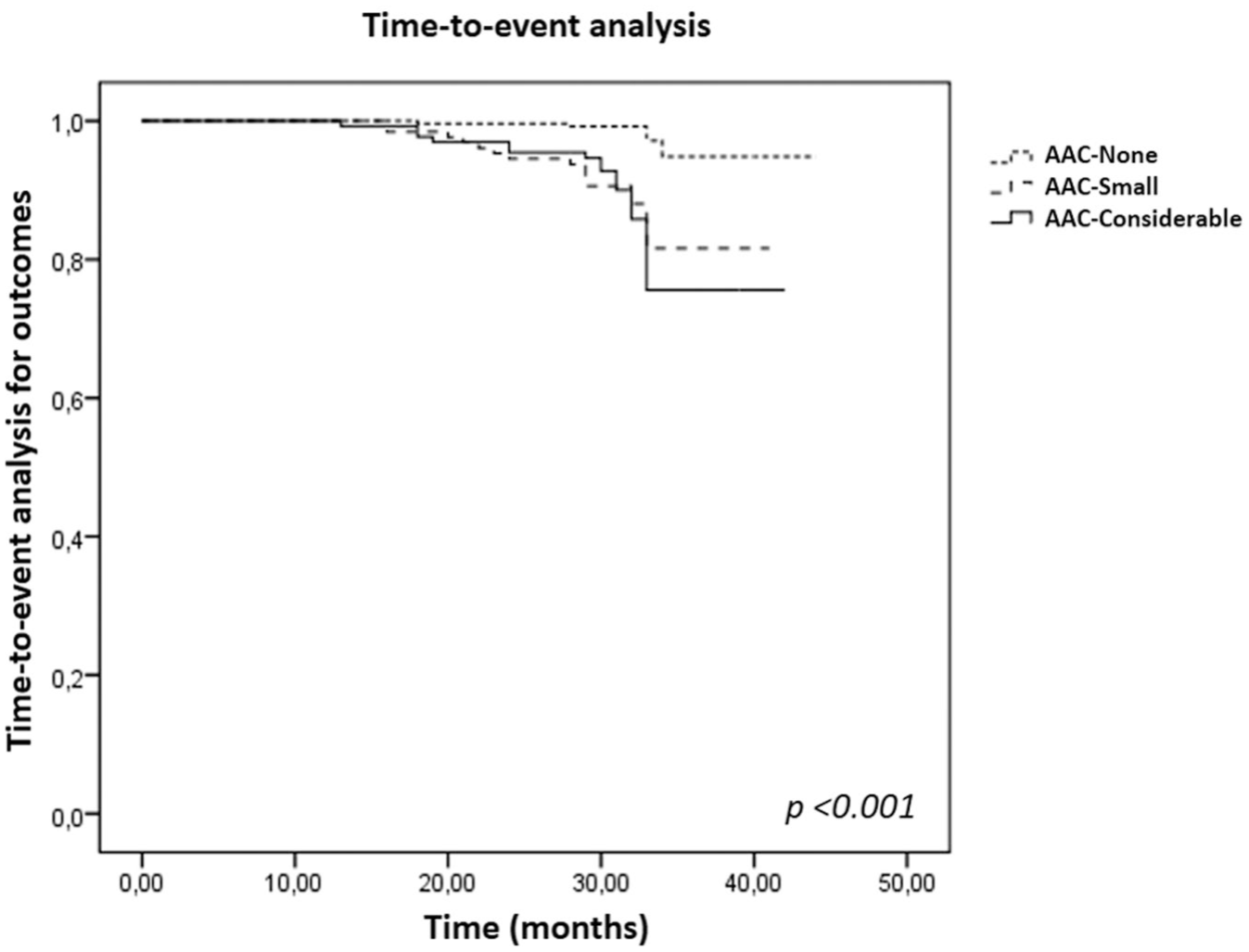
Kaplan-Meier curves showing cumulative event-free survival according to aortic arch calcification categories (none, small, and considerable).
Univariable and Multivariable Cox Regression Analyses for Predictors of Major Adverse Cardiovascular Events According to Aortic Arch Calcification.
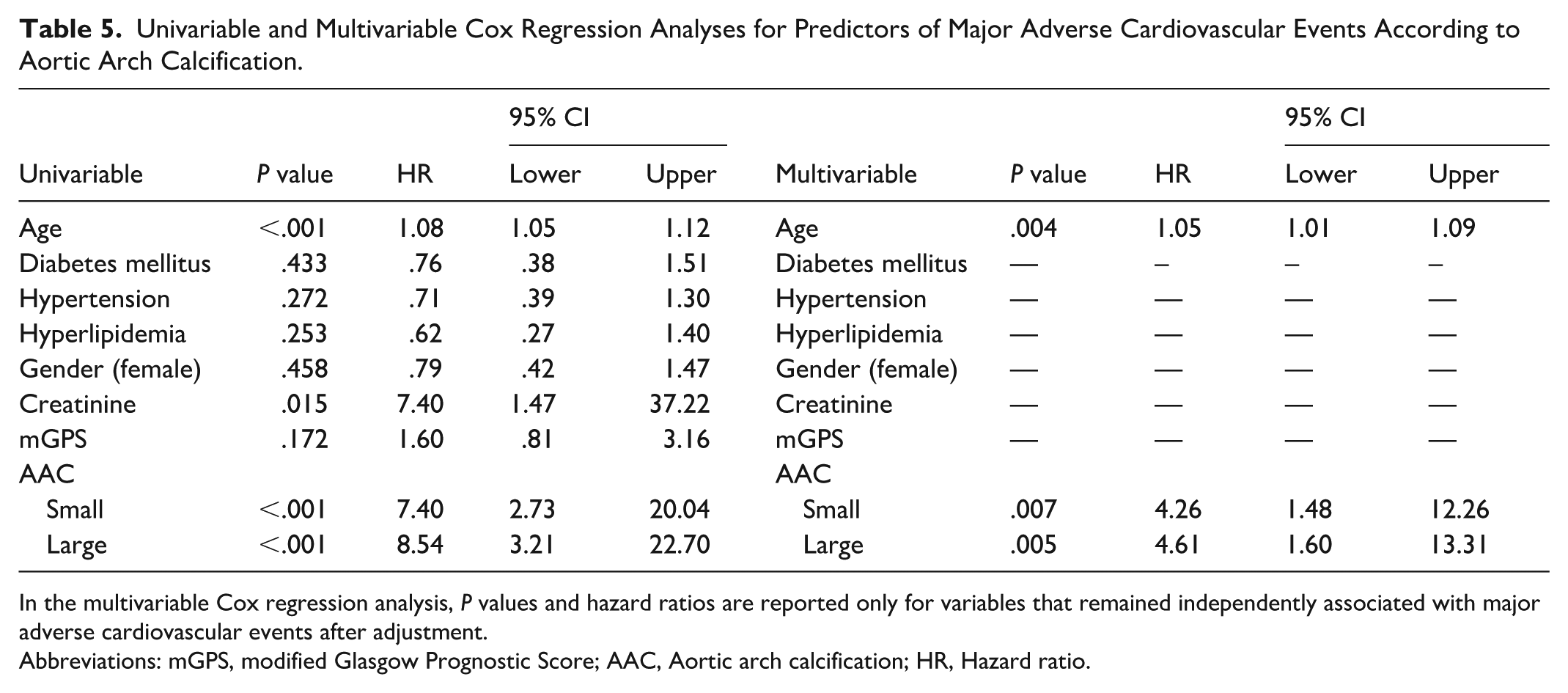
In the multivariable Cox regression analysis, P values and hazard ratios are reported only for variables that remained independently associated with major adverse cardiovascular events after adjustment.
Abbreviations: mGPS, modified Glasgow Prognostic Score; AAC, Aortic arch calcification; HR, Hazard ratio.
Event-free survival progressively worsened with increasing aortic arch plaque complexity on Kaplan-Meier analysis (log-rank P < .001; Figure 5). In univariable Cox analysis, smooth, ulcerated, and protruding plaques were all associated with markedly elevated risk of MACE (HR 7.90 [2.95-21.17], HR 7.62 [2.68-21.64], and HR 14.32 [4.54-45.12]; all P < .001). After multivariable adjustment, AAM remained a powerful independent prognostic marker: compared with patients without detectable plaque, those with smooth, ulcerated, and protruding morphologies had higher risks of MACE (HR 4.69 [1.65-13.37], P = .004; HR 4.56 [1.49-13.97], P = .008; HR 6.85 [1.93-24.36], P = .003, respectively; Table 6).
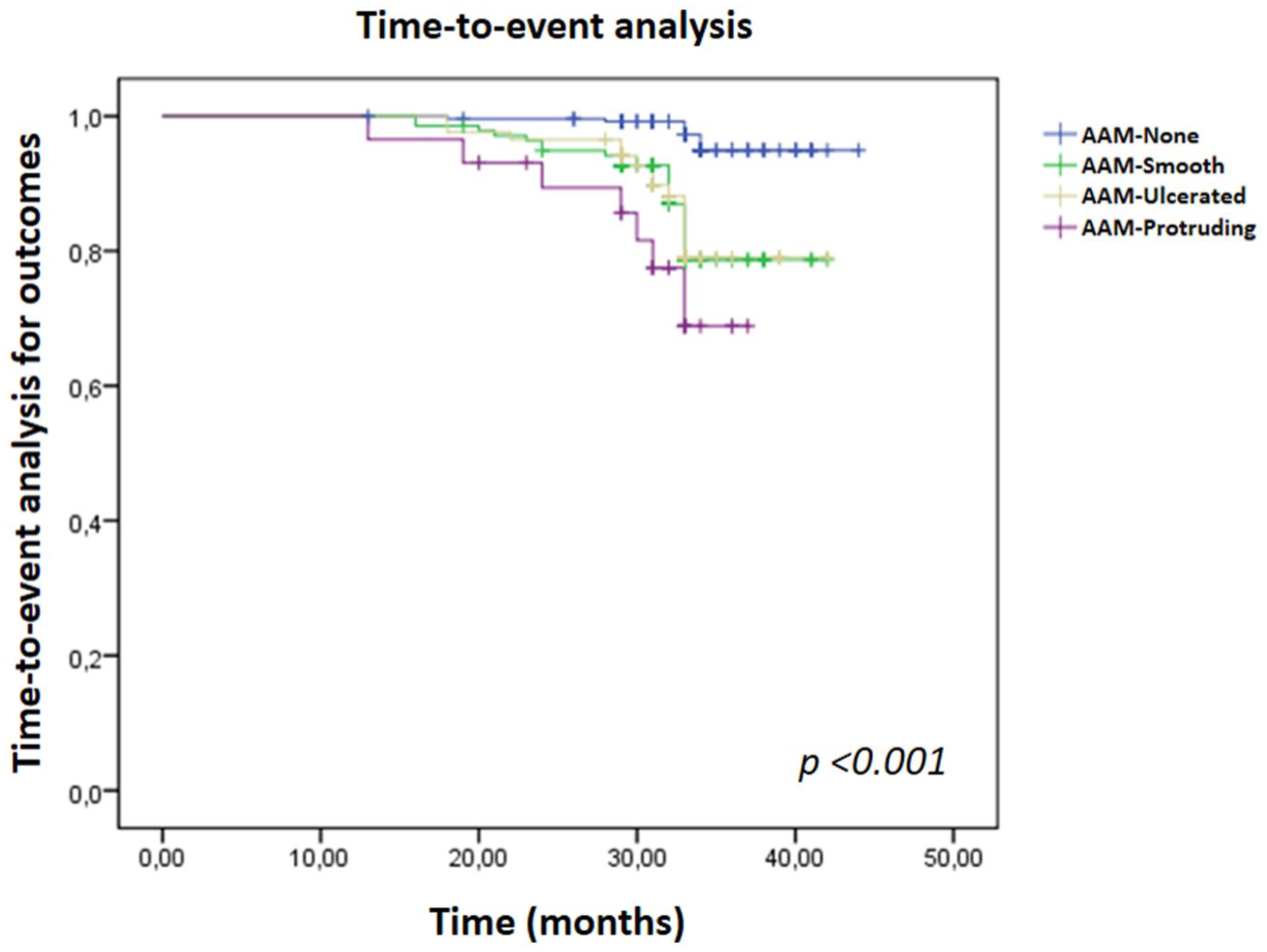
Kaplan-Meier curves showing cumulative event-free survival according to aortic arch morphology categories (none/smooth/ulcerated/protruding).
Univariable and Multivariable Cox Regression Analyses for Predictors of Major Adverse Cardiovascular Events According to Aortic Arch Morphology.
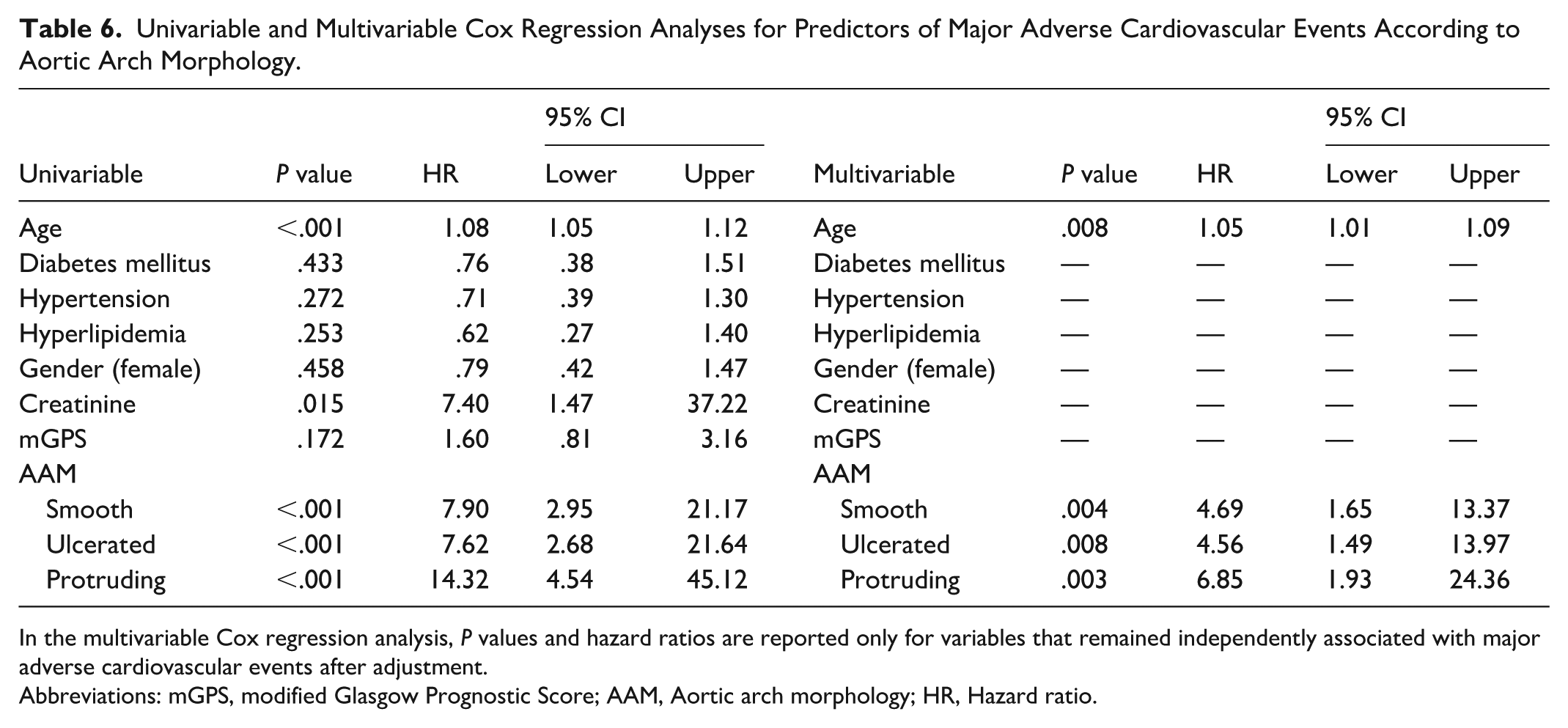
In the multivariable Cox regression analysis, P values and hazard ratios are reported only for variables that remained independently associated with major adverse cardiovascular events after adjustment.
Abbreviations: mGPS, modified Glasgow Prognostic Score; AAM, Aortic arch morphology; HR, Hazard ratio.
Although higher mGPS values showed a trend toward increased event rates, this association did not remain statistically significant after multivariable adjustment in either model. Among conventional risk factors, only age retained independent prognostic value (HR 1.05 [1.01-1.09], P = .008).
Discussion
In this retrospective study evaluating the relationship between systemic inflammation, aortic arch atherosclerosis, and long-term cardiovascular outcomes, we found that both the extent of AAC and the complexity of AAM were independently associated with MACE during a median follow-up of 32 months. Notably, patients with even small calcifications or smooth plaques had substantially higher event risk, which further increased with large or protruding plaques. Although mGPS demonstrated a trend toward higher event rates, it did not retain independent prognostic significance after multivariable adjustment.
Our findings extend previous observations that AAC serves as a marker of cumulative vascular injury and systemic atherosclerotic burden.13,20,21 Prior studies have shown that advanced AAC correlates with increased mortality and cardiovascular events,17,18 while complex plaque morphology is strongly linked to embolic stroke and recurrent ischemia.13 -19 Consistent with these data, our study demonstrates that both calcific and morphologic features of the aortic arch identified by CTA provide powerful prognostic information beyond traditional cardiovascular risk factors.
Age emerged as the most consistent determinant of adverse outcomes, reflecting the progressive and multifactorial nature of vascular aging and its impact on arterial stiffness and calcification.20 -23 The independent predictive value of AAC supports the concept that calcific aortic burden represents a marker of systemic arteriosclerosis and chronic hemodynamic stress. In contrast, the prognostic importance of AAM, particularly ulcerated and protruding plaques, likely reflects an active inflammatory and thrombogenic process associated with plaque instability.17,18,24 -26 Together, these observations indicate that calcific and morphologic characteristics of the aortic arch capture distinct but complementary aspects of systemic atherosclerosis: AAC may represent chronic structural degeneration, whereas AAM reflects dynamic inflammatory remodeling.
Although the mGPS, which integrates CRP and serum albumin levels, was not an independent predictor of MACE in our cohort, its association with more advanced plaque morphology suggests that systemic inflammation contributes to plaque complexity rather than calcification27 -29 This aligns with mechanistic insights highlighting inflammation-driven endothelial dysfunction, monocyte activation, and matrix degradation as hallmarks of plaque destabilization.24 -26 Therefore, mGPS may still serve as a surrogate marker of inflammatory activity underlying morphologic plaque evolution. The observation that mGPS was associated with plaque morphology but not independently with clinical events suggests that systemic inflammation may primarily modulate plaque complexity rather than act as a direct determinant of adverse outcomes. The loss of independent prognostic significance in multivariable models may also reflect the relatively limited number of events and collinearity between mGPS, age, and comorbid conditions, which are major drivers of both inflammatory burden and cardiovascular risk.
Beyond its prognostic implications, AAC represents a complex biological process driven by chronic inflammation, endothelial dysfunction, and vascular remodeling. Systemic inflammatory activation promotes endothelial permeability, facilitates monocyte recruitment, and accelerates macrophage infiltration within the arterial wall, contributing to plaque progression and morphological complexity. Inflammatory cytokines and proteolytic enzymes further weaken the fibrous cap through extracellular matrix degradation, increasing plaque vulnerability and the likelihood of surface disruption. 30 Recent evidence has underscored the active role of the adventitia in atherosclerosis, particularly through expansion of the vasa vasorum and the formation of artery tertiary lymphoid organs (ATLOs), which sustain chronic inflammatory signaling within the vessel wall. Adventitial inflammation may promote vascular remodeling by facilitating immune cell trafficking, enhancing oxidative stress, and activating fibroblasts and smooth muscle cells. These processes can induce osteogenic differentiation of vascular smooth muscle cells via inflammatory mediators, ultimately contributing to medial and intimal calcification. In the aortic arch, where hemodynamic stress is pronounced, such adventitia-driven inflammatory and osteogenic pathways may accelerate structural remodeling and calcific burden, linking chronic inflammation to progressive aortic arch calcification.31,32
Calcification and plaque morphology may reflect distinct but interconnected stages of atherosclerotic evolution. While calcification is often regarded as a marker of cumulative and long-standing vascular injury, complex plaque morphology such as ulcerated or protruding lesions may represent a more active inflammatory and thrombogenic state. Our findings support this concept, as systemic inflammation assessed by the modified Glasgow Prognostic Score was independently associated with plaque morphology severity but did not directly predict clinical events. This suggests that inflammation may primarily influence plaque characteristics rather than act as an immediate trigger of adverse cardiovascular outcomes.
The clinical implications of these findings merit consideration. Routine CTA-based assessment of AAC and AAM provides not only anatomical characterization but also potentially relevant prognostic information. Patients exhibiting extensive calcification or complex plaque morphology may represent a subgroup at higher risk and could be considered for closer clinical surveillance and intensified risk factor management. In addition, the integration of imaging-derived aortic arch features with systemic inflammatory markers such as mGPS may offer a more comprehensive framework for cardiovascular risk assessment. However, as formal evaluation of incremental prognostic performance beyond traditional risk factors was not performed, these observations should be regarded as hypothesis-generating. Prospective studies specifically designed to assess incremental predictive value and clinical utility are required before these findings can be translated into routine preventive strategies.
This study has several limitations. Its retrospective, single-center design and inclusion of patients referred for clinically indicated CTA may introduce selection bias and limit external validity. Although extensive exclusion criteria were applied to reduce confounding and better isolate the associations between aortic arch characteristics, systemic inflammation, and outcomes, these criteria may restrict generalizability to broader cardiovascular populations. In addition, the relatively limited number of outcome events raises concerns regarding model stability and potential overfitting in multivariable Cox regression analyses; therefore, hazard ratio estimates should be interpreted with caution, considering the events-per-variable ratio. While covariate selection was restricted to clinically relevant variables, larger studies with greater event numbers and alternative modeling strategies are needed for confirmation. Blood cell-based inflammatory indices such as the neutrophil-to-lymphocyte and platelet-to-lymphocyte ratios were not evaluated due to the lack of consistently available differential blood count data, and their integration with protein-based scores such as mGPS warrants investigation in future studies. Finally, detailed echocardiographic data enabling classification of left ventricular geometry were unavailable, precluding assessment of its potential relationship with aortic arch remodeling and calcification. Prospective, multicenter studies incorporating comprehensive imaging and inflammatory profiling are required to validate and extend these findings.
Conclusion
Both AAC and complex AAM independently predicted major adverse cardiovascular events during a 32-month follow-up. While mGPS correlated with plaque complexity, it was not an independent prognostic factor. Routine assessment of aortic arch features on CTA may provide valuable prognostic information and contribute to cardiovascular risk assessment and hypothesis-generating risk stratification strategies.
Footnotes
Acknowledgements
The authors would like to thank the radiology and cardiology teams of Medline Hospitals for their support in image acquisition and clinical data collection. We also acknowledge the contribution of the hospital information systems staff for their assistance with data management.
Abbreviations and acronyms
Author Contributions
All authors contributed to: (1) substantial contributions to conception and design, or acquisition of data, or analysis and interpretation of data, (2) drafting the article or revising it critically for important intellectual content, and (3) final approval of the version to be published.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.