
Abstract
The present pilot study included obese 21 patients (13 females and 8 males; mean age: 33.2 ± 11.0 years) who underwent bariatric surgery between December 2021 and June 2022. Echocardiographic evaluations and brain natriuretic peptide measurements were performed preoperatively and 3 months postoperatively. All patients underwent sleeve gastrectomy, and myocardial function was assessed using standard 2-dimensional M-mode Doppler echocardiography. The mean body mass index decreased from 44.8 ± 3.2 to 34.2 ± 2.9 kg/m2 (P < .001). Left ventricular (LV) ejection fraction increased from 62.5% ± 5.0% preoperatively to 64.8% ± 3.5% postoperatively (P = .003). Interventricular septum, posterior wall thickness, systolic pulmonary artery pressure, P max, and isovolumic relaxation time decreased significantly (P < .05). Left ventricular septal E′ and left ventricular lateral E′ values increased (P = .020 and .002, respectively). Although the mean pro- brain natriuretic peptide level decreased post-operatively, an increase was observed in 10 patients. Bariatric surgery significantly improves myocardial function, even in the absence of preoperative cardiac disease. However, given the short follow-up period, these findings reflect early myocardial changes. Further follow up with larger cohorts are warranted to interpret long-term clinical outcomes.
Introduction
Obesity is the most common chronic metabolic disease in the current era and its incidence is increasing.1,2 It is a major cause of the increased risk of cardiovascular disease, type 2 diabetes mellitus, dyslipidemia, and hypertension which are the components of the metabolic syndrome. 1 Individuals with metabolic syndrome tend to have cardio-metabolic pathologies more often than the normal population. 2
The metabolic conditions which are caused by obesity increase the risk of cardiovascular diseases and heart failure.3,4 Pulmonary and cardiac functions may be affected and as a result of the pulmonary and cardiac changes, right and/or left heart failure may occur in this population. 1
Body mass index (BMI) has been found to be directly associated with cardiac enlargement and left ventricular hypertrophy (LVH). 5 Every 1 kg/m2 increase in the BMI increases the risk of heart failure by >5%. 6 The increased risk of heart failure in people with obesity is mainly related with myocardial hypertrophy which leads to impaired left ventricular relaxation and also higher stroke volume and affected preload as a result of increased circulating blood volume. 6
In addition to structural changes, obesity is associated with neurohormonal activation, sympathetic nervous system stimulation, renin-angiotensin-aldosterone system activation, and adipokine-mediated myocardial remodeling, all of which contribute to both systolic and diastolic myocardial dysfunction. 7
Increased stroke volume and cardiac output cause left and right ventricular hypertrophy (LVH), systolic and diastolic dysfunction and left atrial dilatation by modifying cardiac structure. 5 Other than these factors; sympathetic and renin-angiotensin-aldosterone system activation, the release of myocardial growth factors from adipose tissue and metabolic changes increase the stiffness of great arteries. 5
In addition to promoting weight loss, bariatric surgery may also contribute to improvements in cardiac function. The procedure has beneficial effects on obesity-related metabolic conditions and may facilitate normalization of left ventricular diastolic dysfunction and improvement in heart rate variability, thereby contributing to a reduced risk of heart failure. 3
Although several studies have reported improvements in cardiac structure and function following bariatric surgery, most available data derive from mid- and long-term follow-up periods, while evidence from earlier postoperative evaluations remains relatively limited. 8
In the present a pilot study, we sought to evaluate the early effects of bariatric surgery on myocardial functions in obese patients by assessing the echocardiographic parameters before and 3 months after the operation.
Patients and Methods
This pilot study included 21 patients who underwent bariatric surgery between December 2021 and June 2022. There were 13 females and 8 males (33.2 ± 11.0 years). Patients were examined by echocardiography before and 3 months after bariatric surgery. Brain natriuretic peptide (proBNP) was measured in every patient preoperatively and 3 months after surgery.
Patients aged 18 to 55 years with obesity who were scheduled for primary sleeve gastrectomy were eligible for inclusion. Exclusion criteria included known coronary artery disease, heart failure, cardiomyopathy, moderate-to-severe valvular heart disease, atrial fibrillation, chronic kidney disease, chronic inflammatory disease, or inadequate echocardiographic image quality.
Patients were examined by echocardiography before and 3 months after bariatric surgery. proBNP was measured in every patient preoperatively and 3 months after surgery. This study was approved by the Institutional Research Ethics Committee of Istanbul Training and Research Hospital (Approval Number: 2875, date: June 18, 2021). The study was conducted in accordance with the principles outlined in the Declaration of Helsinki and adhered to local ethical guidelines. Written informed consent was obtained from all participants prior to their inclusion in the study.
Hypertension was present in 3 patients, diabetes mellitus in 1 patient, and insulin resistance (Insulin resistance = HOMA-IR index > 2.5; Homeostasis Model Assessment of Insulin Resistance [HOMA-IR] index calculated by fasting insulin [µU/mL] × fasting glucose [mg/dL]/405) in 4 patients. One patient had sleep apnea syndrome, 1 patient had hypothyroidism, 1 patient had history of deep vein thrombosis, and 1 patient was congenitally blind. All patients underwent sleeve gastrectomy.
Demographic features of the patients were recorded. Age, gender, body mass index (BMI), weight and height of the patients were analyzed. All patients underwent a transthoracic echocardiographic examination.
Standard two-dimensional (2D) M-mode Doppler echocardiography (PHILIPS AFFINITY 50C; Philips Healthcare, Bothell, Washington, WA, USA) was used for examination. All patients underwent a standardized examination by the same experienced cardiologist in the left-lateral decubitus position. All echocardiographic examinations were performed by the same experienced cardiologist using optimized imaging settings, including low-frequency transducers, harmonic imaging, and multiple acoustic windows to ensure adequate image quality to minimize variability related to body habitus and suboptimal acoustic windows, which are common challenges in obese patients.
A 2.5-MHz transducer was used for standard Doppler echocardiographic measurements, while tissue Doppler imaging was performed using a transducer operating within a frequency range of 2.5 to 3.5 MHz. The examination was based on the guidelines of the European Association of Cardiovascular Imaging. 9
The biplane Simpson method from the apical views (2- and 4-chamber) was used to measure left ventricular ejection fraction. Left ventricle end systolic diameter (LVESD), left ventricle end diastolic diameter (LVEDD), right ventricle end diastolic diameter (RV), interventricular septum (IVS), and posterior wall thickness (PW) were obtained from the parasternal long axis view. Left atrium diameter (LA), aortic valve maximum systolic flow velocity (Amax), systolic pulmonary arterial pressure (sPAP), pulmonary valve maximum systolic velocity (Pmax), early peak (E) and late peak (A) diastolic transmitral flow velocity, E/A ratio, deceleration time (DT), and isovolumic relaxation time (IVRT) were also measured.
LV pulsed tissue Doppler imaging (TDI) was performed on the apical 4-chamber view using a 5-mm pulsed Doppler sample volume. Septal, lateral left ventricular, and right ventricular annular velocities were measured.
Left ventricular hypertrophy was defined IVS and posterior wall thickness >1.10 cm.
According to the 2017 European Association of Cardiovascular Imaging Consensus Document, diastolic function was evaluated using transmitral flow parameters and tissue Doppler indices. 9
Measurement of natriuretic peptides (BNP/NT-proBNP) is recommended by current ESC and ACC/AHA heart failure guidelines 10 and was assessed preoperatively and 3 months postoperatively in our study.
The primary echocardiographic endpoints of the study were changes in left ventricular ejection fraction, ventricular wall thickness, and tissue Doppler-derived diastolic parameters.
Statistical Analysis
IBM SPSS Statistics Software 28 (SPSS Inc., Chicago, IL, USA) was used for statistical analyses. Descriptive statistics included mean, standard deviation, median, minimum, maximum, frequency, and ratio values.
The distribution of variables was assessed using the Kolmogorov–Smirnov test. Paired-sample t-test and Wilcoxon test were used for comparison of dependent quantitative data. A 2-sided P-value of <.05 was considered statistically significant.
No formal sample size calculation was performed, as this is a pilot study designed as an exploratory analysis to evaluate early postoperative myocardial changes rather than to test a predefined hypothesis.
Results
There were 13 female and 8 male patients included in the study. Mean age of the patients was 33.2 ± 11.0 years. Mean weight and height of the patients was 129.1 ± 15.1 kg and 169.6 ± 15.1 cm, respectively. Three months after bariatric surgery, mean weight of the patients was decreased to 98.3 ± 11.4 kg. Preoperative mean BMI was 44.8 ± 3.2 kg/m2 and postoperative 3rd month mean BMI was 34.2 ± 2.9 kg/m2. The patients were examined by echocardiography before the operation and left ventricular hypertrophy, impaired systolic or diastolic functions were not detected.
Sleeve gastrectomy method was performed in all patients. Mortality or morbidity did not occur in any of the patients. Major complications were not observed. Patients were taken to the ward following the operation and discharged from the hospital on the 3rd postoperative day.
As shown in Table 1, postoperative LVEF value increased significantly (P < .05) compared with the preoperative period. Postoperative LVESD, LVEDD, RV, Amax, MITRAL E, MITRAL A, DT, E/E′, LV Septal A′, LV Septal SM, LV Lateral SM, RV Lateral E′, LV Lateral A″ values did not differ significantly. Postoperative values of IVS, PW, sPAP, P max, LA, IVRT decreased significantly (P < .05). Postoperative LV Septal E′ value increased significantly (P < .05). LV Lateral E′ value increased significantly (P < .05) in the postoperative period. Postoperative proBNP value decreased significantly (P < .05) when compared with the preoperative period.
Pre- and Post-Operative Echocardiographic Parameters (Mean ± SD and Median) with Corresponding P-Values.
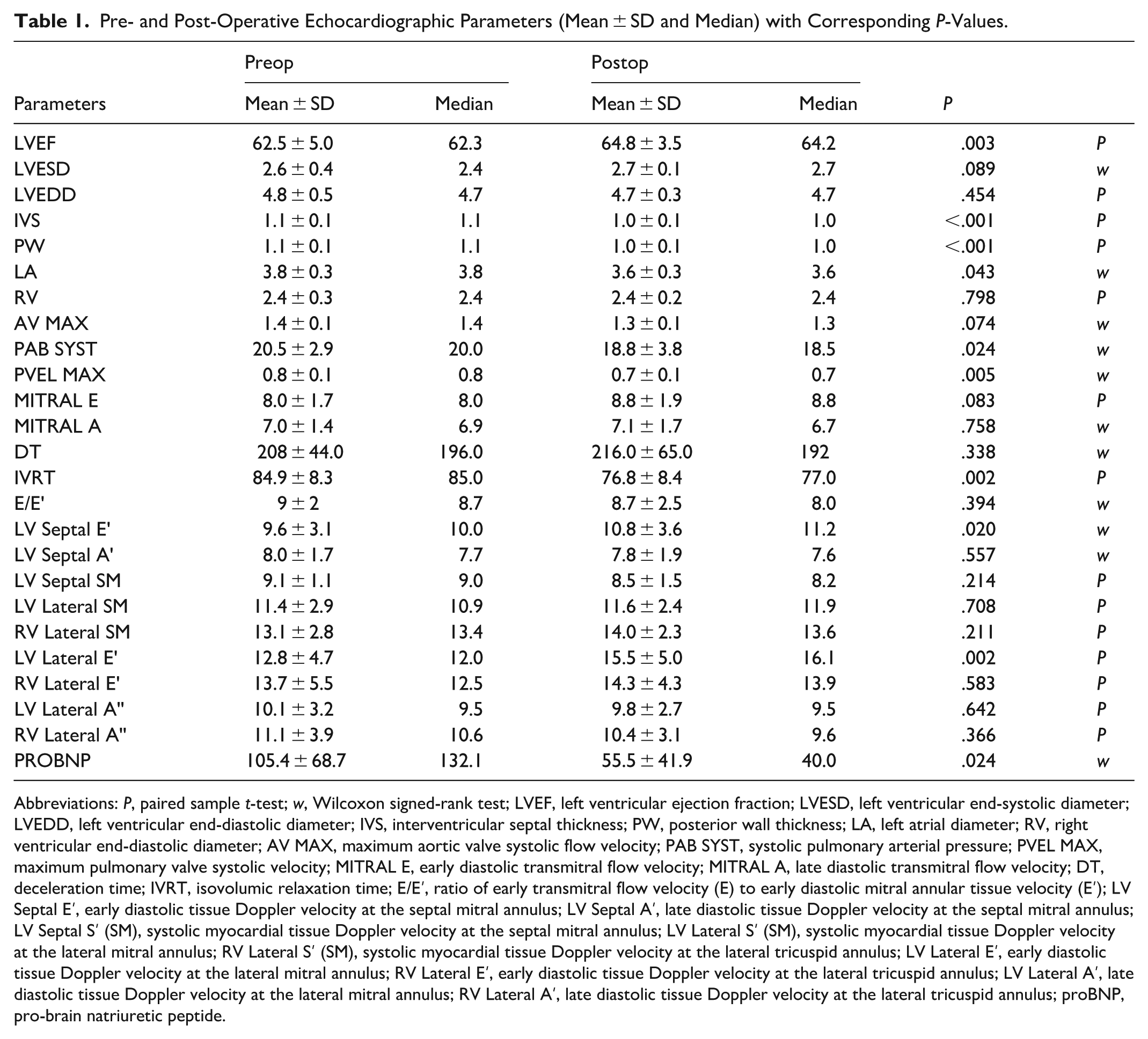
Abbreviations: P, paired sample t-test; w, Wilcoxon signed-rank test; LVEF, left ventricular ejection fraction; LVESD, left ventricular end-systolic diameter; LVEDD, left ventricular end-diastolic diameter; IVS, interventricular septal thickness; PW, posterior wall thickness; LA, left atrial diameter; RV, right ventricular end-diastolic diameter; AV MAX, maximum aortic valve systolic flow velocity; PAB SYST, systolic pulmonary arterial pressure; PVEL MAX, maximum pulmonary valve systolic velocity; MITRAL E, early diastolic transmitral flow velocity; MITRAL A, late diastolic transmitral flow velocity; DT, deceleration time; IVRT, isovolumic relaxation time; E/E′, ratio of early transmitral flow velocity (E) to early diastolic mitral annular tissue velocity (E′); LV Septal E′, early diastolic tissue Doppler velocity at the septal mitral annulus; LV Septal A′, late diastolic tissue Doppler velocity at the septal mitral annulus; LV Septal S′ (SM), systolic myocardial tissue Doppler velocity at the septal mitral annulus; LV Lateral S′ (SM), systolic myocardial tissue Doppler velocity at the lateral mitral annulus; RV Lateral S′ (SM), systolic myocardial tissue Doppler velocity at the lateral tricuspid annulus; LV Lateral E′, early diastolic tissue Doppler velocity at the lateral mitral annulus; RV Lateral E′, early diastolic tissue Doppler velocity at the lateral tricuspid annulus; LV Lateral A′, late diastolic tissue Doppler velocity at the lateral mitral annulus; RV Lateral A′, late diastolic tissue Doppler velocity at the lateral tricuspid annulus; proBNP, pro-brain natriuretic peptide.
While the increase of the postoperative EF value showed the improvement of systolic function, the significant decrease of IVS and PW values are in favor of improved left ventricular hypertrophy. The decrease of the IVRT value and increase of the septal and lateral E′ values were in favor of improvement of diastolic dysfunction. Although mean value of proBNP decreased postoperatively; it was found increased in 10 patients. Despite the observed increase in proBNP levels in these 10 patients, no clinical deterioration, echocardiographic worsening, perioperative complications, or signs of heart failure were detected during the follow-up period.
Although the patients were asymptomatic and were not diagnosed with heart failure or impaired left ventricular systolic or diastolic dysfunction before the operation, the increased LVEF showed improved systolic function after the bariatric surgery in the early follow-up period.
Patients were followed up for 5 months (mean: 5 ± 1.2), uneventfully. When all parameters were assessed at the post-operative 3rd month control, the myocardial functions were found improved. All patients described improved quality of life and there were no complications related to the surgery during the follow-up. The patients are still being followed at the outpatient clinics and are active and event free.
Given the absence of a control group and the short duration of follow-up, these findings should be interpreted as early postoperative myocardial changes rather than definitive evidence of long-term cardiac benefit.
Discussion
Obesity is defined as a body mass index (BMI) ≥ 30 kg/m2.which is further classified as Class I (BMI: 30.0-34.9 kg/m2), Class II (BMI: 35.0-39.9 kg/m2), and Class III (BMI: ≥40 kg/m2). It has become one of the epidemic problems affecting approximately 13% of the population. 11 The clinical evidence of heart failure is seen in one-third of adults with severe obesity and the prevalence of heart failure increases dramatically over time. It exceeds 70% at 20 years and 90% at 30 years of being obese. 3 One of the most common causes of heart failure with preserved EF is obesity. 6
The prevalence of abnormal subclinical myocardial function has been found to be between 37% and 54% in cases of obesity and metabolic disease. Such abnormalities may be associated with the development of heart failure and increased cardiovascular disease risk even in the absence of preexisting disease. 3 Subclinical myocardial changes may be detected with cardiac imaging tools such as echocardiography in the asymptomatic phase. 3
Recent studies have shown that additional body fat requires an extra blood flow of 2 to 3 mL/min/100 g. 1 This requirement is met by increased cardiac output and blood volume in individuals with moderate or severe obesity. Left ventricular preload and afterload increase to maintain higher cardiac output, which may lead to increased right and left ventricular filling pressures. 1 Chronic hypoxia and hypercapnia due to obstructive sleep apnea and obesity hypoventilation syndrome may also contribute to pulmonary vasoconstriction, resulting in pulmonary hypertension and increased transpulmonary pressure gradients. 1
Left ventricular hypertrophy, a strong predictor of sudden death, coronary artery disease, cerebrovascular events, and congestive heart failure, has been found to be directly associated with BMI and waist circumference. 5 Obesity-related LVH contributes to progressive systolic and/or diastolic dysfunction, 5 and diastolic dysfunction is therefore more prevalent in obese individuals. 6
proBNP is secreted from ventricular myocardium and is activated in the setting of heart failure. 12 Although proBNP levels are commonly used for diagnosis and prognostic stratification of heart failure, 7 levels may paradoxically increase following bariatric surgery. This phenomenon may reflect myocardial and metabolic remodeling rather than pathological deterioration. 13 In the present study, although mean proBNP levels decreased significantly, an increase was observed in 10 patients. The underlying mechanisms of this variability could not be determined within the scope of this study, as no clinical or echocardiographic deterioration was observed, and no postoperative complications were identified.
Several studies have demonstrated that bariatric surgery is associated with reduced cardiovascular mortality and improved cardiac structure and function. Aggarwal et al 14 reported significant improvement in cardiac morphology and function after bariatric surgery using echocardiography and cardiac magnetic resonance imaging. 5 Koshino et al 15 observed improvement after Roux-en-Y gastric bypass at a mean follow-up of 23 ± 10 months, while Tuluce et al 16 reported early improvement 1 month after sleeve gastrectomy.
In our study, patients were evaluated 3 months after sleeve gastrectomy and demonstrated significant improvements in echocardiographic parameters reflecting myocardial structure and diastolic function. Although the increase in left ventricular ejection fraction was statistically significant, the magnitude of change (approximately 2%) is modest and is unlikely to translate into meaningful short-term clinical outcomes in patients with preserved baseline systolic function. This finding likely represents early myocardial adaptation rather than definitive systolic recovery.
Therefore, the observed improvements should be interpreted cautiously, as potential postoperative confounding factors such as changes in medication use, physical activity levels, and dietary habits were not formally adjusted for and may have contributed to the observed echocardiographic changes.
From a biochemical perspective, glucagon-like peptide-1 (GLP-1) levels increase after bariatric surgery 17 and have been associated with improvements in left ventricular systolic function in experimental and clinical studies. 18 Additionally, adipokines such as leptin, TNF-α, and adiponectin, which influence cardiovascular physiology, decrease after bariatric surgery and may contribute to improved myocardial function. 12
Obese men predominantly exhibit concentric hypertrophy, whereas obese women demonstrate both concentric and eccentric hypertrophy 14 Aggarwal et al 14 reported an 11.2% reduction in left ventricular mass index following bariatric surgery, supporting reverse remodeling. Meta-analyses have shown regression of diastolic dysfunction and reduction in left atrial size after bariatric surgery. 4
In the present study, although overt LV hypertrophy or diastolic dysfunction was not present preoperatively, postoperative reductions in IVS, PW, sPAP, P max, and IVRT, along with increases in LV septal and lateral E′ values, support improvement in subclinical myocardial function and are consistent with the existing literature.
The major limitations of the study are the small sample size and short follow-up period. Additionally, due to the absence of clinical or subclinical myocardial dysfunction at baseline, we could not assess heart failure prevalence in obese patients or the long-term healing effects of bariatric surgery on the myocardium.
The absence of a non-surgical control group limits causal inference, and potential confounding factors such as postoperative medication use, physical activity levels, and dietary changes were not formally adjusted for in the analysis.
The relatively young age of the study population and predominance of mild-to-moderate obesity may have contributed to preserved myocardial function despite obesity, limiting generalizability to older patients or those with severe obesity or comorbid cardiovascular disease.
Conclusion
Our results indicate that even in patients without overt cardiac disease, bariatric surgery confers measurable benefits on myocardial structure and function. The reduction in left ventricular wall thickness supports early cardiac reverse remodeling, while improvements in diastolic indices reflect enhanced myocardial performance.
These findings represent early postoperative myocardial changes observed at 3 months and should not be interpreted as evidence of long-term clinical benefit. Larger, controlled studies with longer follow-up are needed to confirm the durability and clinical relevance of these observations.
Footnotes
Consent to Participate
All participants were thoroughly informed about the study protocol, procedures, potential risks and benefits, and their rights (including the right to withdraw at any time without affecting their medical care), and written informed consent was obtained prior to enrollment.
Author Contributions
Substantial contributions to conception and design: HO, DMO, SS, FD, KU, AT, and MU. Acquisition of data, or analysis and interpretation of data: HO and SS. Drafting the article: HO, DMO, and SS. Revising it critically for important intellectual content: HO, DMO, SS, FD, KU, AT, and MU. Final approval of the version to be published: HO, DMO, SS, FD, KU, AT, and MU.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data not available (To protect patient confidentiality and privacy, the data generated and/or analyzed during this study will not be publicly shared).