
Abstract
The present review aimed to evaluate the prognostic value of inflammatory biomarkers in patients undergoing endovascular aortic aneurysm repair (EVAR). A systematic review of relevant studies was performed according to PRISMA guidelines. Articles assessing associations of inflammatory biomarkers with the post-EVAR outcomes were considered. After screening, 34 studies were included (7019 patients were reviewed; mean age: 73.6 years; 91.6% were men); 22 different inflammatory biomarkers were identified among the included studies. Neutrophil-to-lymphocyte ratio (NLR), platelet-to-lymphocyte ratio (PLR), and lymphocyte-to-monocyte ratio (LMR) were investigated in 11, 4, and 3 studies, respectively. Nine studies evaluated the post-implantation syndrome (PIS) and examined its role in post-EVAR outcomes. Increased preoperative NLR was associated with all-cause mortality and acute kidney injury after EVAR. NLR was also reported as an independent risk factor for aneurysm sac regression failure. High preoperative PLR and low preoperative LMR were correlated with acute kidney injury and overall mortality, respectively. PIS was associated with a lower type 2 endoleak rate but had no impact on mortality rates. NLR may be a useful predictor for mortality and poor prognosis in EVAR populations. This may have clinical implications in post-EVAR surveillance programs.
Keywords
Introduction
Appropriate surveillance and lifelong patient monitoring following endovascular abdominal aortic aneurysm repair (EVAR) are necessary to minimize subsequent aneurysm-related morbidity and mortality. Early detection of postoperative endoleaks provides the rationale for thorough follow-up after the procedure. 1 A pro-inflammatory state along with vascular wall inflammatory activity might be associated with post-EVAR outcomes. 2 Thus, the identification of inflammatory biomarkers for the prognosis following EVAR remains an area of active investigation.
Recently, it has been shown that inflammatory biomarkers might have a predictive value in oncologic patients and in patients with ST-segment elevation myocardial infarction, especially those undergoing percutaneous coronary intervention.3 -6 More specifically, an elevated neutrophil-to-lymphocyte ratio (NLR) was reported to increase mortality and rehospitalization after transcatheter or surgical aortic valve replacement for aortic stenosis. 7 Post-implantation syndrome (PIS) is also a marker of systemic inflammatory response following EVAR that may lead to high rates of 30-day mortality and major adverse cardiovascular events (MACE). 8 However, published data are scarce regarding the potentially prognostic role of various inflammatory markers in post-EVAR outcomes. This information is vital for the vascular surgeon and can help recognizing EVAR patients at highest risk of developing postoperative complications.
The present study aimed to perform a systematic review of the available literature to document the predictive value of the existing inflammatory biomarkers in patients undergoing elective EVAR.
Methods
Study Design, Eligibility Criteria, and Patient Inclusion
This systematic review was undertaken according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. 9 Before the full-text screening, a predefined detailed protocol of our systematic review was prospectively registered in the International Prospective Register of Systematic Reviews (PROSPERO, registration number: CRD420261293893). No institutional review board (IRB) approval was required since the present review utilized published work.
Articles assessing the possible association of inflammatory biomarkers with clinical outcomes following endovascular repair of intact abdominal aortic aneurysms (AAA) in the elective setting, irrespective of study design, were examined for inclusion. Exclusion criteria were: (i) studies including <20 patients, (ii) studies reporting on ruptured AAAs, (iii) articles referring to thoracic endovascular aortic repair (TEVAR), (iv) studies including patients undergoing complex EVAR procedures (eg, fenestrated/branched EVAR), (v) studies describing open surgical repair (OSR) of AAAs, (vi) articles reporting on pararenal or juxtarenal AAAs, (vii) inflammatory biomarkers derived from the cerebrospinal fluid, (viii) studies including patients suffering from aortic dissection, (ix) experimental animal studies or virtual aneurysm models, (x) patients undergoing endovascular aneurysm sealing (EVAS), (xi) studies including patients with a known history of systemic inflammatory disease or with clinical or laboratory evidence of an active infection preoperatively or postoperatively, and (xii) meta-analyses, systematic reviews, editorials, letters to the editor, or comments. Studies with overlapping populations were excluded unless they investigated different biomarkers or reported on different outcomes.
Information Sources and Search Strategy
We searched the MEDLINE (PubMed), Scopus, and Cochrane Library databases (last search: January 27, 2026) applying the algorithm: ((“inflammat* biomarker*”) OR (“inflammat* index*”) OR (“inflammat* indicator*”) OR (“inflammat* marker*”) OR (“systemic inflammat*”) OR (“NLR”) OR (“PLR”) OR (“LMR”) OR (“inflammat* status”) OR (“post-implantation syndrome”)) AND ((“endovascular abdominal aortic aneurysm repair”) OR (“endovascular aneurysm repair”) OR (EVAR) OR (“endovascular aortic aneurysm repair”)). No time, gender, or geographic limitations were used. The study selection process involved 2 authors (G.K., O.L.), blind to each other, inspecting the titles and abstracts of the retrieved literature. Publications with titles and abstracts satisfying the inclusion criteria were collected in full-text and analyzed. The full-text screening was performed by the same 2 authors. When studies from the same institution were identified, the most recent or the most relevant one was examined for inclusion. Any disagreement was resolved through discussion with a third investigator. We also hand-searched all studies for potentially eligible articles applying the snowball methodology. 10
Data Extraction, Processing, and Definitions
Two authors independently extracted the data into a spreadsheet. The extracted information included the study author(s), publication year, study period, study design, number of patients, type of inflammatory biomarker examined, patient demographics, aneurysm-related details, and main findings of each study. The primary outcome was the perioperative inflammatory biomarkers and their correlation with the post-EVAR outcomes, as reported in the included studies.
The inflammatory biomarkers were defined as those measured in the perioperative period and included the NLR, platelet-to-lymphocyte ratio (PLR), lymphocyte-to-monocyte ratio (LMR), red blood cell distribution width (RDW), RDW-to-albumin ratio (RAR), hemoglobin-to-RDW ratio (HRR), white blood cells (WBC), platelets (PLT), C-reactive protein (CRP), procalcitonin (PCT), interleukin-1 (IL-1), IL-2, IL-6, IL-8, intercellular adhesion molecule-1 (ICAM-1), monocyte chemoattractant protein-1 (MCP-1), tumor necrosis factor alpha (TNF-a), systemic immune inflammatory index (SIII), systemic inflammatory response index (SIRI), volume of newly formed thrombus after the deployment of the endograft (fresh thrombus), fibrinogen, and PIS. PIS was defined across the included studies as an early systemic inflammatory response following EVAR and was characterized by flu-like symptoms, changes in temperature, and laboratory findings of inflammation, in the absence of infection. 11 Notably, PIS was considered either as inflammatory marker or as post-EVAR outcome in this review. The volume of fresh thrombus was defined as the volume of contrast filling the aneurysmal sac in the preoperative computed tomography angiography (CTA) after subtracting the endograft volume following device deployment, and was observed in the first postoperative CTA. The remaining biomarkers were measured perioperatively in blood samples. A proposed calculation formula for these biomarkers is shown in Table 1.
Calculation Formulas for Inflammatory Biomarkers.
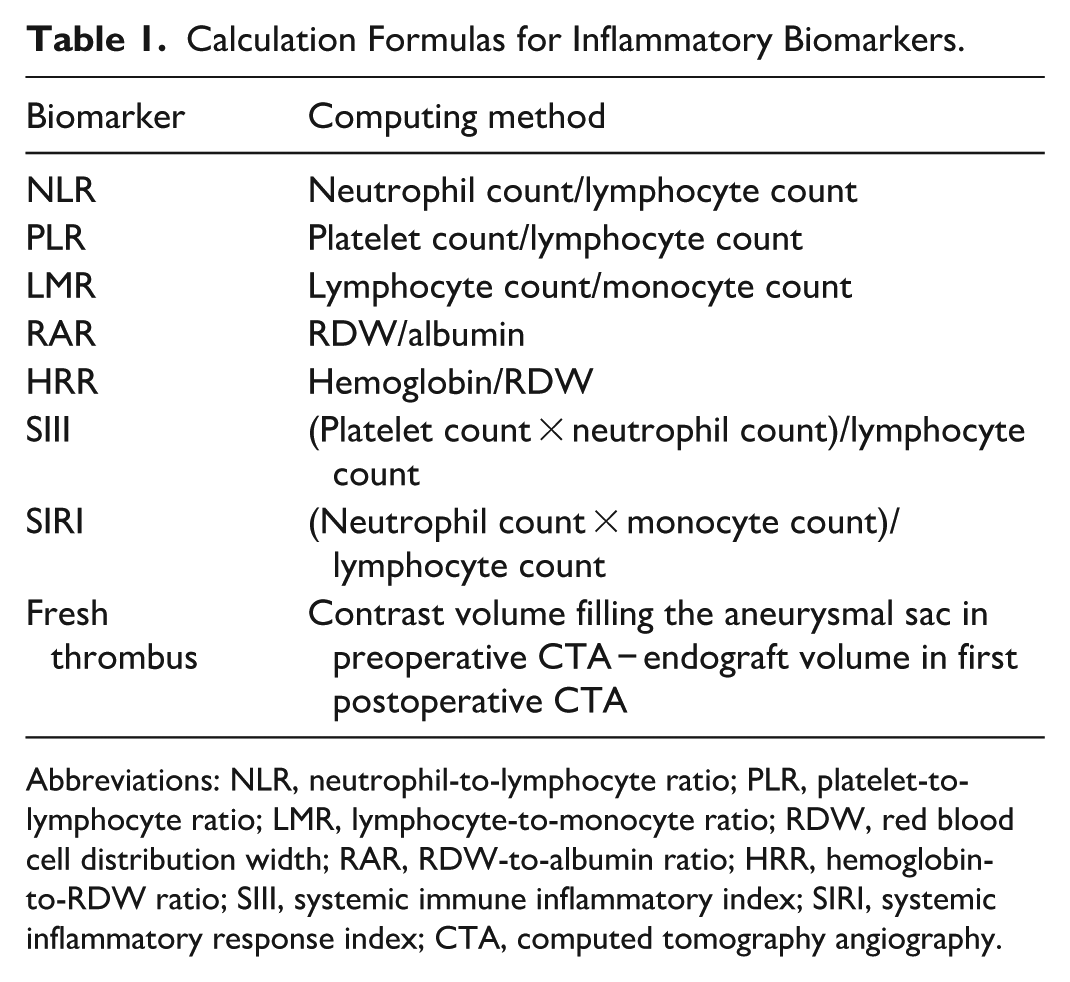
Abbreviations: NLR, neutrophil-to-lymphocyte ratio; PLR, platelet-to-lymphocyte ratio; LMR, lymphocyte-to-monocyte ratio; RDW, red blood cell distribution width; RAR, RDW-to-albumin ratio; HRR, hemoglobin-to-RDW ratio; SIII, systemic immune inflammatory index; SIRI, systemic inflammatory response index; CTA, computed tomography angiography.
The clinical outcomes following EVAR included all-cause mortality, perioperative mortality, endoleak, MACE, reintervention, AAA shrinkage/growth, acute kidney injury, and PIS rates. To increase data completeness, whenever necessary, an email was sent to the corresponding author of the study requesting the missing information.
Assessment of Study Quality and Risk of Bias
The risk of bias and study quality of the included studies was evaluated using the methodological index for non-randomized studies (MINORS) tool. 12 Scoring quality of non-comparative studies was defined as low (0-8), moderate (9-12), and high (13-16). Scoring quality for comparative studies was labeled as low (0-12), moderate (13-18), and high (19-24). The intraclass correlation coefficient (ICC) and the 2-way mixed model were applied to estimate inter-observer agreement.
Results
Study and Patient Characteristics
The literature search yielded 253 potentially eligible articles after duplicates were removed. Following full-text screening, 34 studies met our eligibility criteria, as summarized in the PRISMA flow diagram (Figure 1).11,13 -45 These were 29 retrospective and 5 prospective cohort studies. A total of 7019 patients undergoing EVAR were identified. One study included 24 EVAR patients out of 75 patients scheduled to undergo non-cardiac vascular surgery procedures and underscored the predictive value of inflammatory status in outcomes following these procedures. 13 The mean MINORS score for the non-comparative studies was 10.9 ± 0.7 (range: 10-12; moderate quality). The mean score for the comparative studies was 18.1 ± 1.8 (range: 14-20; moderate quality). Interobserver agreement in the assessment of study methodology was excellent (ICC: 0.97; 95% confidence interval: 0.95-0.98). The baseline characteristics of the included studies are outlined in Table 2. The mean age of the cohort was 73.6 ± 2.1 years (range: 70.3-78.5 years), and 5155 of the 5627 patients (91.6%) were men. Of those with available data (n = 4832), their mean AAA diameter was 56 ± 2.8 mm (range: 49.9-61 mm). Additionally, the patients shared the usual atherosclerotic risk factors of a population with AAA. The extracted data on patient demographics are presented in Table 3.
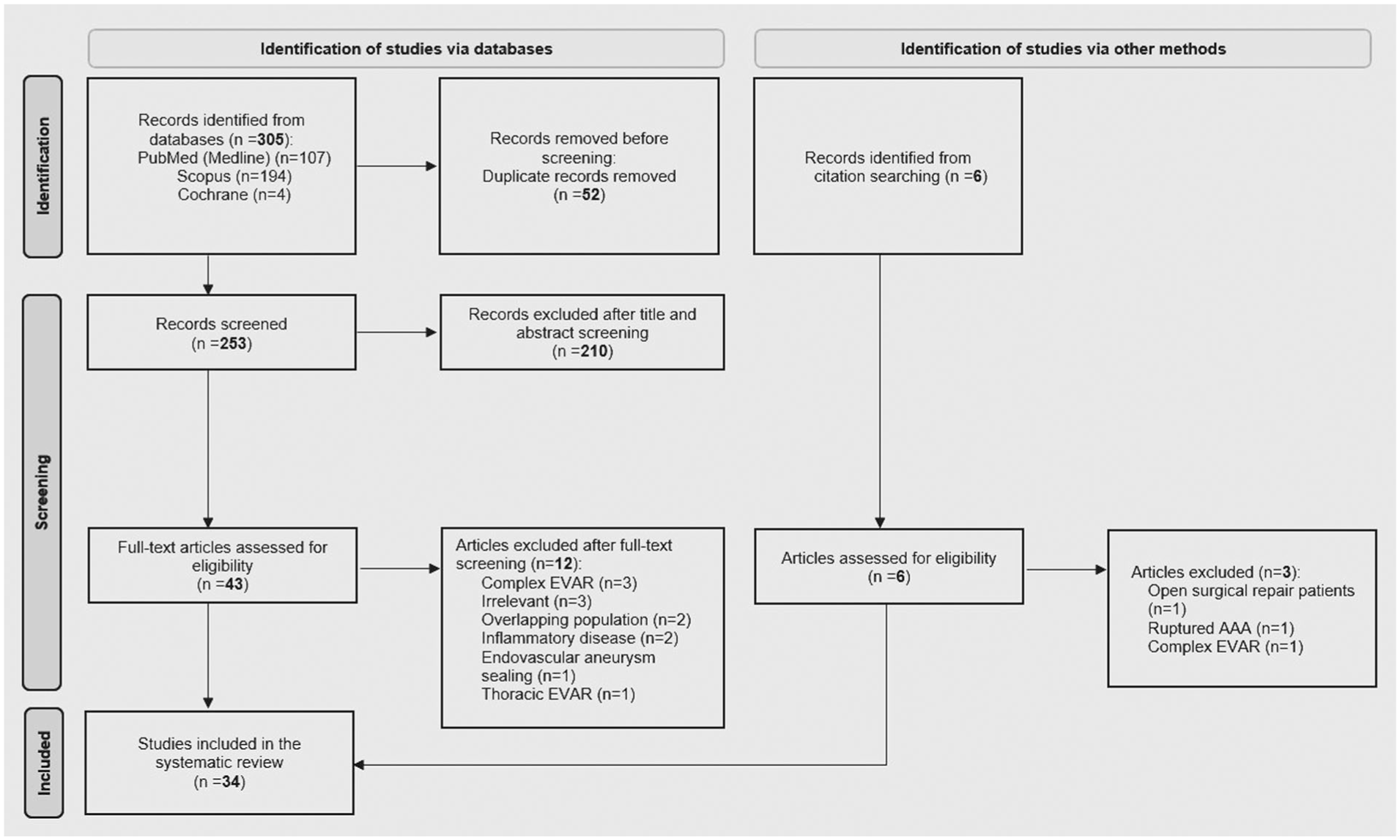
PRISMA flowchart (last search: January 27, 2026).
Baseline Characteristics of the Included Studies. Studies Appear in Reverse Chronological Order (Publication Year).
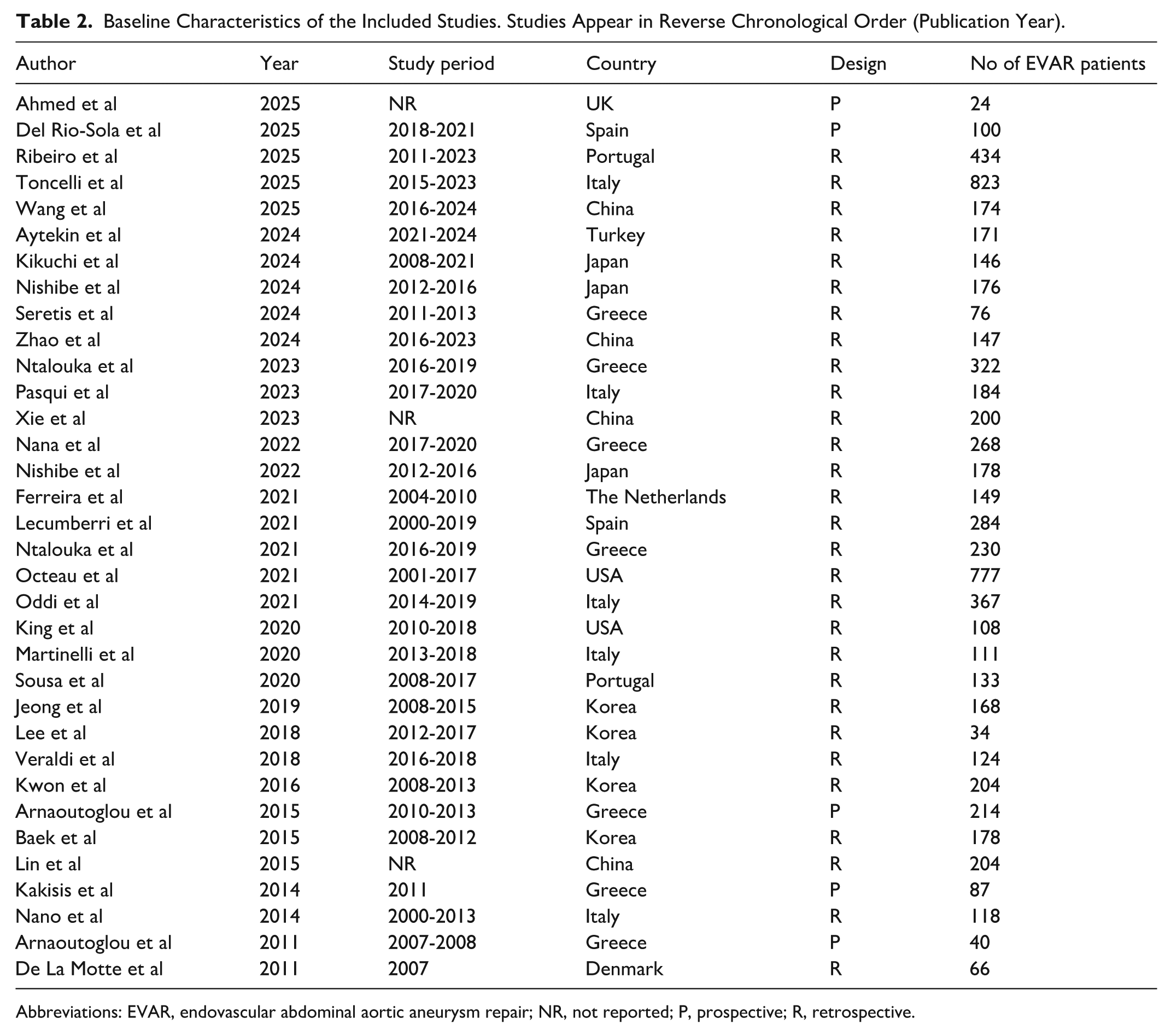
Abbreviations: EVAR, endovascular abdominal aortic aneurysm repair; NR, not reported; P, prospective; R, retrospective.
Patient Demographics and Comorbidities.
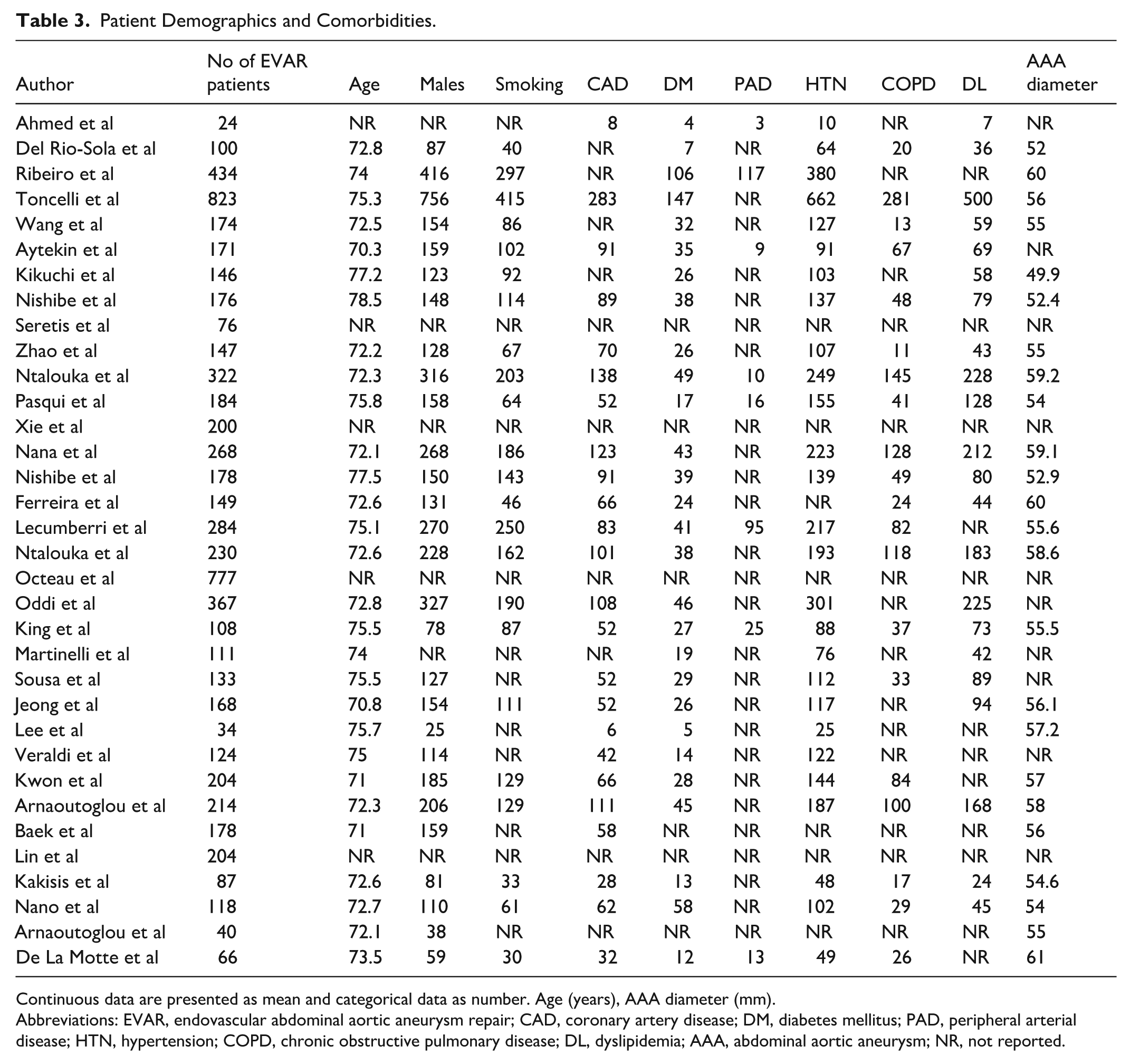
Continuous data are presented as mean and categorical data as number. Age (years), AAA diameter (mm).
Abbreviations: EVAR, endovascular abdominal aortic aneurysm repair; CAD, coronary artery disease; DM, diabetes mellitus; PAD, peripheral arterial disease; HTN, hypertension; COPD, chronic obstructive pulmonary disease; DL, dyslipidemia; AAA, abdominal aortic aneurysm; NR, not reported.
Inflammatory Biomarkers and Post-EVAR Outcomes
The associations of various inflammatory biomarkers with the clinical outcomes following EVAR are described in detail in Table 4. A total of 22 different inflammatory biomarkers were investigated in the 34 studies. NLR, PLR, and LMR were investigated in 11, 4, and 3 articles, respectively. Nine studies considered the PIS as a marker of inflammatory status in the immediate postoperative period and examined its role in post-EVAR outcomes. Increased preoperative NLR was found to be a significant predictor of all-cause mortality and acute kidney injury in EVAR patients.15,16,22,23,27 This predictive value remained even when NLR was measured postoperatively.28,29 With regards to the impact of NLR on the reintervention rate, mixed results were found. Octeau et al indicated that high NLR values >3.6 were an independent predictor of reinterventions at 30 days, 1, and 5 years. 30 Nevertheless, a single-center, retrospective analysis of 108 patients undergoing elective EVAR failed to detect any association with reintervention rate or sac enlargement. 32 NLR was reported as an independent risk factor for no shrinking AAA with no effect, though, on the endoleak rate.19,24 Additionally, low preoperative LMR <3.21 was correlated with overall mortality, whereas, high postoperative PLR >22.8 was associated with acute kidney injury.20,29 Mortality rates were similar between patients who experienced PIS and those who did not, while PIS was significantly associated with a lower type 2 endoleak rate.11,18,34,38 There was also a considerable controversy among the included studies as to whether PIS could be predictive or not of the adverse events following EVAR.11,33,34,38,39,43
Inflammatory Biomarkers and Their Association With Post-EVAR Outcomes.
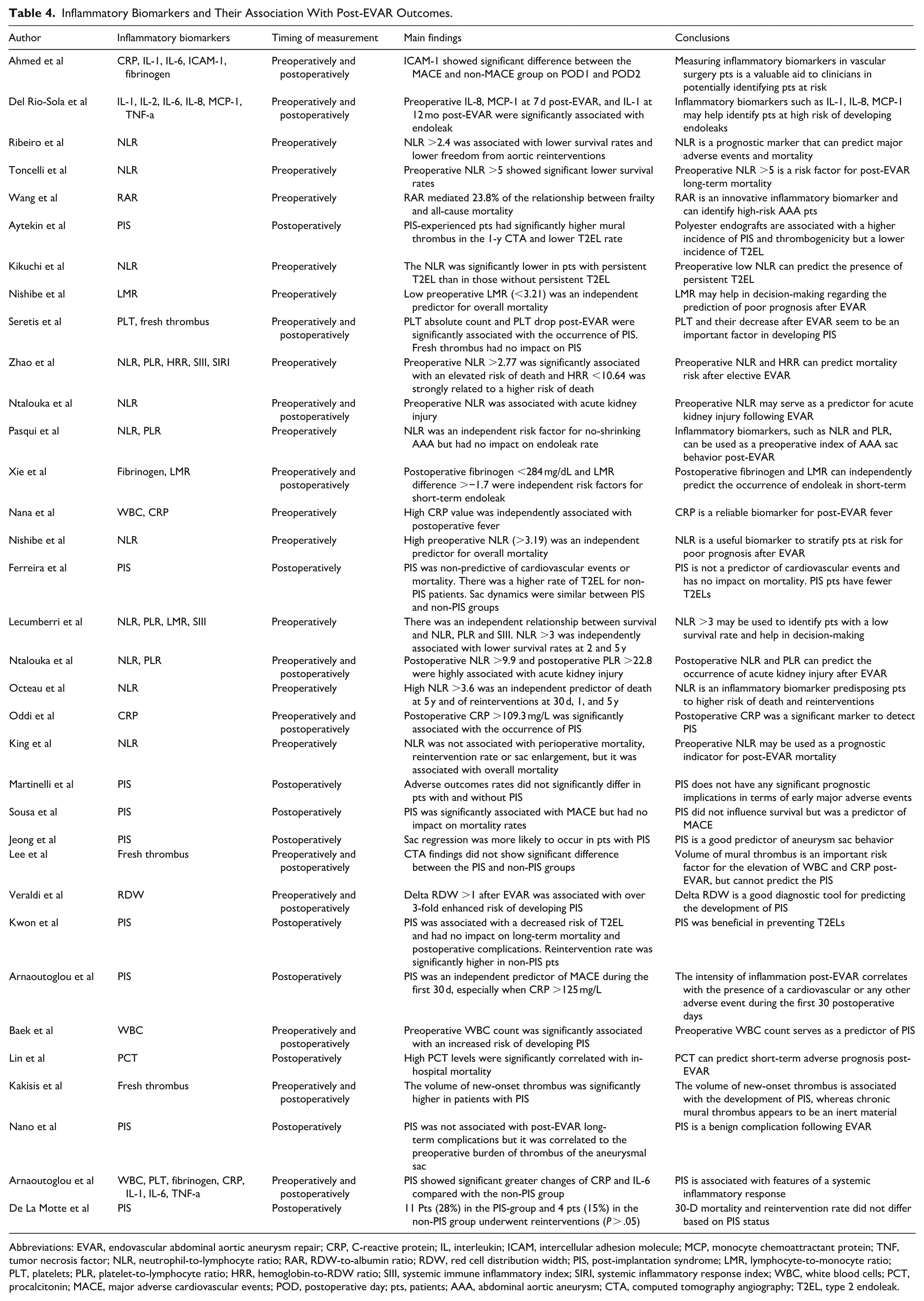
Abbreviations: EVAR, endovascular abdominal aortic aneurysm repair; CRP, C-reactive protein; IL, interleukin; ICAM, intercellular adhesion molecule; MCP, monocyte chemoattractant protein; TNF, tumor necrosis factor; NLR, neutrophil-to-lymphocyte ratio; RAR, RDW-to-albumin ratio; RDW, red cell distribution width; PIS, post-implantation syndrome; LMR, lymphocyte-to-monocyte ratio; PLT, platelets; PLR, platelet-to-lymphocyte ratio; HRR, hemoglobin-to-RDW ratio; SIII, systemic immune inflammatory index; SIRI, systemic inflammatory response index; WBC, white blood cells; PCT, procalcitonin; MACE, major adverse cardiovascular events; POD, postoperative day; pts, patients; AAA, abdominal aortic aneurysm; CTA, computed tomography angiography; T2EL, type 2 endoleak.
Discussion
The present systematic review summarizes the evidence base reporting on the prognostic value of 22 inflammatory biomarkers in patients scheduled to undergo endovascular intervention for intact infrarenal AAA. The majority of studies investigating NLR demonstrated an association between increased NLR and low survival rates after EVAR. Furthermore, elevated NLR and PLR seemed promising for predicting acute kidney injury postoperatively, although these were only investigated by a few studies. The impact of LMR on post-EVAR outcomes is less well described, with fewer studies suggesting a decreased LMR be a predictor of poor prognosis following EVAR. Additionally, the presence of PIS was not predictive of mortality but was correlated with a decreased risk of type 2 endoleak.
The prognostic value of NLR in an EVAR population has been supported by several of the included studies. High preoperative NLR values have been independently associated with an elevated overall mortality risk and acute kidney injury after EVAR.15,16,22,23,27 Octeau et al evaluated 777 EVAR patients and showed that NLR levels were related to increased 5-year mortality, as well as higher reintervention rates at 30 days, 1, and 5 years. 30 Similar conclusions have been reached by other investigators supporting that NLR elevation might predict increased secondary aortic interventions. 15 However, King et al showed that although NLR is a good prognostic marker for mortality, it cannot predict reinterventions or sac behavior. 32 This discrepancy might be the result of low numbers of patients and events in the last study or differences in follow-up duration. A multicentric retrospective study of 823 EVAR patients validated the predictive value of NLR in post-EVAR long-term mortality and showed that only 9.5% of deaths were attributed to AAA-related causes. 16 This possibly explains that elevated NLR mainly reflects the patient’s overall clinical frailty and systemic vulnerability. Thus, the adverse events and poor prognosis following EVAR, observed in the high-NLR cohort, are primarily due to the patients’ overall frail health status rather than to EVAR technical failure. Patient comorbidities, age, smoking status, and baseline frailty, often revealing an inflammatory background, may be potential confounding factors that obviously influence the values of inflammatory biomarkers and, thus, may affect the clinical course of EVAR patients.
The precise mechanism by which chronic systemic inflammation contributes to clinical outcomes following EVAR is poorly described. There is an established relationship between chronic inflammation and cardiovascular long-term mortality.46,47 Chronic systemic inflammation also serves as a key etiological component of the development and progression of atherosclerotic disease. 48 AAA patients, as in our patient cohort, often present risk factors and systemic features of atherosclerosis. Therefore, it is reasonable to assume that chronic inflammatory response, expressed by inflammatory biomarkers, might predispose EVAR patients to increased mortality risk. However, it remains unclear whether systemic inflammation drives the progression of aneurysmal disease, or whether aneurysm-related factors drive the systemic inflammation. 49 Apparently, an increased NLR indicates an immune profile of chronic low-grade inflammatory state. Neutrophilia might be related to endothelial cellular injury, microvascular plugging, and hypercoagulability. 50 The other component, lymphopenia may be associated with adverse physiological stress, possibly leading to systemic susceptibility. 51
Additionally, the optimal cutoff value of NLR with the strongest association with post-EVAR outcomes varies across the included studies and ranges from 2.4 to 5.0 preoperatively, whereas, it can reach up to 9.9 in cases of postoperative measurement.15,16,29 This fluctuation could be partially justified by the differences in study design, patient selection, sample size, and timing of measurement. One of the highest-quality studies uncovered a cutoff point of 3.6 in a training set of 388 patients showing that patients with a preoperative NLR <3.6 had improved mortality rates. 30 Another recent study with high methodological quality suggested a 2.4 NLR cutoff as a fair discriminator for long-term mortality. 15 The prospective UK Biobank cohort study of ~440 000 participants reported that in cancer-free controls the “normal” mean value of NLR was 2.35. 52 Taking these data into consideration, we suggest that a cutoff point of 2.5 to 3 regarding preoperative NLR may be a good risk stratification tool to guide clinicians in perioperative decision-making.
Predicting aneurysm sac behavior following EVAR is of paramount importance if high clinical success rates are to be achieved. A large retrospective analysis of Vascular Quality Initiative (VQI) data underlined that sac behavior is associated with the development of new endoleaks, reintervention, and long-term mortality. Not only sac expansion but also sac regression failure is correlated with lower long-term survival, independent of reinterventions or endoleaks. 53 Notably, high preoperative PLR and NLR values have been linked to no-shrinking AAA post-EVAR. In particular, a PLR <104.8 and an NLR <3.81 were selected as the cutoff values for AAA shrinkage. 24 Another study showed that high PLR and NLR levels, measured in the immediate postoperative period, can predict the occurrence of acute kidney injury after EVAR, 29 establishing their role as biomarkers both preoperatively and postoperatively. Although PLR was found to be linear and independently related to long-term survival following EVAR, only NLR moderately enhanced the discriminative power of a survival predictive model. 28 The association of PLR with survival rates, however, could not be confirmed in a more recent study, probably reflecting differences in follow-up duration and number of enrolled patients. 22 Regarding LMR, a low preoperative value might predict overall mortality and poor prognosis after EVAR. A higher number of monocytes compared to lymphocytes might be suggestive of impaired immune response and poor post-EVAR outcomes. 20
The precise effect of PIS on clinical outcomes following EVAR remains debatable. Several of the included studies have documented that PIS is a benign condition and does not appear to have a major prognostic value or impact on survival rates in an EVAR population.11,43,45 Patients experiencing PIS, though, had a decreased risk of developing type 2 endoleaks.18,38 One possible explanation for this finding could be that PIS, reflecting a systemic inflammatory response, may eradicate low pressure arteries which potentially can be responsible for type 2 endoleaks. Furthermore, Kakisis et al reported that the volume of new-onset thrombus is associated with the occurrence of PIS. 42 Therefore, PIS patients have greater volume of new-onset thrombus and might experience more frequently total sac thrombosis, thereby minimizing type 2 endoleak rate. There is also inconsistency throughout the literature regarding the prognostic implications of PIS in terms of MACE.33,34 Nevertheless, a recent systematic review evaluating 309 patients experiencing PIS demonstrated an association between 30-day mortality and MACE and PIS. 8 Again, this discrepancy may be justified by the differences in follow-up duration and sample size.
According to the Society for Vascular Surgery (SVS) guidelines on the care of patients with AAA, biomarkers such as fibrinogen, D-dimer, and IL-6 have been consistently correlated with the presence of AAA in multiple studies.1,54 However, these biomarkers have been used primarily aiming to detect the presence of an aortic aneurysm rather than predict clinical outcomes following EVAR. No relevant recommendation exists incorporating inflammatory indicators for post-EVAR surveillance. To address this gap, our systematic review presents reliable indexes that could be used to estimate the patient perioperative inflammatory status and correlate it with outcomes after EVAR. We suggest that inflammatory biomarkers, especially NLR, could serve as predictors of clinical sequelae following EVAR. It is a simple and inexpensive test derived from a complete blood count, that is, measured as part of the perioperative work-up. Incorporating such biomarkers in sophisticated EVAR follow-up algorithms may result in early detection of complications and improve post-EVAR surveillance programs. However, further well-designed studies with prospective data collection and low risk of bias are warranted to validate these findings, shed light on topics of debate, and determine the optimal cutoff values for the aforementioned inflammatory biomarkers, before these markers can be reliably incorporated into routine post-EVAR surveillance algorithms.
Study Limitations
The results of the present study should be interpreted in the context of several limitations. First, this review is limited by the retrospective design and non-blinded nature of the included studies. The predominance of retrospective studies and moderate methodological quality of included data might affect the strength of conclusions. The heterogeneity across studies in terms of biomarker cutoff values, timing of measurement, and outcome definitions may also limit the applicability of our results. Additionally, overlapping populations from the same centers might have been included occasionally but the relevant authors either investigated different biomarkers or reported on different clinical outcomes. The prognostic role of some biomarkers might have been discussed only by a few studies, thereby reducing the validity and preventing from drawing conclusions for these biomarkers. Given the large variety of inflammatory biomarkers and associated outcomes examined, no quantitative synthesis of results could be performed, further restricting the impact of our findings. Lastly, complex EVAR procedures possibly associated with more intense inflammatory response were excluded.
Conclusions
This study summarizes the available literature regarding the prognostic value of 22 inflammatory biomarkers in outcomes after elective EVAR. NLR seems to be a good predictor for mortality and adverse events following EVAR. Additionally, PIS was found to be associated with a lower type 2 endoleak rate. Current evidence is insufficient to substantially support the role of other biomarkers. Further studies are needed to validate these findings and refine post-EVAR surveillance policy.
Footnotes
Author Contributions
All authors contributed to: (1) substantial contributions to conception and design, or acquisition of data, or analysis and interpretation of data, (2) drafting the article or revising it critically for important intellectual content, and (3) final approval of the version to be published.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data associated with the paper are available from the corresponding author on reasonable request.