
Abstract
No-reflow is a serious complication of PPCI in STEMI. Systemic inflammation plays a role, but simple prognostic tools are needed. The Scottish Inflammatory Prognostic Score (SIPS), combining neutrophil count and serum albumin, shows promise in other areas but hasn’t been tested for no-reflow. The present study aimed to investigate the association between admission SIPS and angiographic no-reflow in STEMI patients undergoing PPCI. One thousand eighteen consecutive STEMI patients undergoing PPCI between 2020 and 2025 were analysed. SIPS was calculated on admission. No-reflow was defined as post-procedural thrombolysis in myocardial infarction (TIMI) flow <3 without mechanical obstruction. Associations were assessed using chi-square, receiver operating characteristic (ROC) analysis, and multivariate logistic regression. No-reflow occurred in 132 patients (13.0%), increasing with SIPS: 10.2% (low), 15.9% (moderate), 16.5% (high; P = .022). SIPS had modest discriminative ability (area under Curve [AUC] = 0.563, P = .019), similar to neutrophil count. Diabetes was independently linked to no-reflow (OR 1.30, P = .032); SIPS categories were not. Higher admission SIPS was associated with increased no-reflow risk in a graded pattern but did not emerge as an independent predictor after multivariable adjustment. DM was the sole independent predictor identified.
Keywords
Introduction
Primary percutaneous coronary intervention (PPCI) is the cornerstone of ST-segment elevation myocardial infarction (STEMI) reperfusion therapy, improving clinical outcomes. Despite epicardial coronary artery patency restoration, many patients still have no-reflow, compromising myocardial perfusion. 1 This condition increases the risk of heart failure, recurrent ischaemic episodes, and mortality due to bigger infarcts, detrimental left ventricular remodelling, and lower ejection fraction.2,3
The pathophysiology of no-reflow is multifactorial, involving distal atherothrombotic embolisation, microvascular spasm, reperfusion injury, and endothelial dysfunction. Among these mechanisms, systemic and local inflammation play a central role by promoting neutrophil activation, the release of proinflammatory cytokines, oxidative stress, and microvascular obstruction.4,5 Elevated admission neutrophil counts have consistently been linked to a higher incidence of no-reflow, reflecting neutrophilic infiltration and degranulation that exacerbate ischaemic and reperfusion injury in the microvascular bed.6,7
In contrast, hypoalbuminemia, as a negative acute-phase reactant, is indicative of heightened systemic inflammation and is associated with endothelial impairment, increased oxidative stress, and worse reperfusion outcomes in acute coronary syndromes. 8 Composite markers incorporating albumin, such as the uric acid-to-albumin ratio or haemoglobin-albumin-lymphocyte-platelet (HALP) score, have recently demonstrated predictive value for no-reflow in STEMI patients undergoing PPCI.9,10
Several inflammation-based indices, including the systemic immune-inflammation index (SII), neutrophil-to-lymphocyte ratio (NLR), and derived NLR, have shown utility in predicting no-reflow, highlighting the prognostic importance of inflammatory burden in this setting.7,11
The Scottish Inflammatory Prognostic Score (SIPS), a simple categorical score based on admission neutrophil count (>7.5 × 109/L) and serum albumin (<3.5 g/dL), integrates these 2 biologically relevant markers into low- (0 points), moderate- (1 point), and high-risk (2 points) categories. Originally validated in oncological populations, SIPS has recently emerged as an independent predictor of in-hospital mortality in patients with acute heart failure with reduced ejection fraction. 12 To date, no study has explored the potential association of SIPS with the no-reflow phenomenon in STEMI.
Given the established roles of neutrophilic inflammation and hypoalbuminemia in microvascular dysfunction, SIPS is a pragmatic, readily available tool for risk assessment. The present study aimed to investigate the relationship between admission SIPS and angiographic no-reflow in patients with STEMI undergoing PPCI.
Materials and Methods
Study Design and Setting
This was a retrospective cohort study of consecutive patients admitted with acute ST-segment elevation myocardial infarction (STEMI) who underwent primary percutaneous coronary intervention (PPCI) at our institution between January 2020 and December 2025.
Inclusion and Exclusion Criteria
Patients were eligible if they presented within 12 hours of symptom onset (or up to 48 hours if there was evidence of ongoing ischaemia) and met the diagnostic criteria for STEMI according to the Fourth Universal Definition of Myocardial Infarction. Eligibility also required that all patients had undergone attempted revascularisation of the infarct-related artery via primary percutaneous coronary intervention performed through radial or femoral access.
Patients were excluded if they had active infection or inflammatory disease at admission, chronic liver or kidney disease requiring dialysis, known malignancy, haematological disorders, severe valvular heart disease, cardiogenic shock on presentation (Killip class IV), rescue PCI after failed thrombolysis, or if essential labouratory (including serum albumin or complete blood count) or angiographic data were unavailable. The study was conducted in accordance with the principles of the Declaration of Helsinki and was approved by the local institutional ethics committee (date: 5 February 2026, no: ESH/BAEK 2026/306). Because of the retrospective design and the use of anonymised data, the requirement for informed consent was waived.
Data Collection and Procedural Details
Baseline demographic, clinical, and labouratory data were retrieved from the hospital’s electronic medical records. Comorbidities (hypertension, diabetes mellitus, smoking status, prior coronary artery disease, atrial fibrillation) and presentation characteristics (Killip class, blood pressure, culprit vessel inferred from ST-segment elevation location) were recorded.
Labouratory parameters obtained on admission included complete blood count (with neutrophil count), serum albumin, glucose, kidney function (creatinine and estimated glomerular filtration rate [eGFR] using the CKD-EPI formula), lipid profile, troponin, and other routine biomarkers. All blood samples were drawn before PPCI.
Coronary angiography and PPCI were performed using standard techniques via radial or femoral access. Angiographic data, including the culprit vessel, presence of thrombus (defined as a visible filling defect on contrast imaging), stent length, and final coronary flow, were assessed by experienced interventional cardiologists blinded to clinical data. Cross-reference: PPCI via radial or femoral access was also a prerequisite for study eligibility (see Section 2.2).
Definition of the No-Reflow Phenomenon
The thrombolysis in myocardial infarction (TIMI) flow grading system is a standardised angiographic scale used to assess coronary perfusion: TIMI 0 denotes complete absence of antegrade flow beyond the point of occlusion; TIMI 1 indicates penetration of contrast beyond the occlusion without perfusion of the distal coronary bed; TIMI 2 reflects partial perfusion with delayed or sluggish antegrade flow; and TIMI 3 represents normal, brisk antegrade flow with complete perfusion of the distal vessel. The no-reflow phenomenon was defined as a post-procedural TIMI flow grade <3 in the infarct-related artery despite successful restoration of vessel patency (no residual stenosis >50%, dissection, spasm, or mechanically resolvable distal embolisation).
Scottish Inflammatory Prognostic Score Calculation
The Scottish Inflammatory Prognostic Score (SIPS) was calculated based on admission serum albumin and neutrophil count using established cutoffs. One point was assigned for serum albumin <3.5 g/dL and 1 point for neutrophil count >7.5 × 109/L, resulting in a score of 0 (low risk: both normal), 1 (moderate risk: 1 abnormal), or 2 (high risk: both abnormal).
Statistical Analysis
Continuous variables are presented as mean ± standard deviation and were compared using the independent samples Student’s t-test. Categorical variables are expressed as counts and percentages and were compared using the chi-square test or Fisher’s exact test as appropriate.
The association between SIPS categories and the no-reflow phenomenon was assessed using the chi-square test, with P for trend where applicable. Receiver operating characteristic (ROC) curve analysis was performed to evaluate the discriminative ability of SIPS and other potential predictors (eg, neutrophil count) for no-reflow, with area under the curve (AUC) and 95% confidence intervals reported.
Univariate logistic regression was used to identify variables associated with no-reflow. Variables with P < .10 in univariate analysis or those deemed clinically relevant were entered into a multivariate logistic regression model (enter method) to identify independent predictors of no-reflow. Odds ratios (OR) with 95% confidence intervals were calculated. Model performance was assessed using the Hosmer-Lemeshow goodness-of-fit test, −2 log likelihood, and Nagelkerke R2.
A 2-sided P < .05 was considered statistically significant. All analyses were performed using SPSS software (version 26.0; IBM Corp, Armonk, NY, USA).
Results
Patient Characteristics
A total of 1018 consecutive STEMI patients met eligibility criteria and were included in the final analysis. The no-reflow phenomenon occurred in 132 patients (13.0%). Baseline demographic, clinical, and labouratory characteristics stratified by no-reflow status are presented in Table 1. Key differences between groups are also summarised in Table 1.
Baseline Demographic, Clinical, and Labouratory Characteristics According to No-Reflow Status.
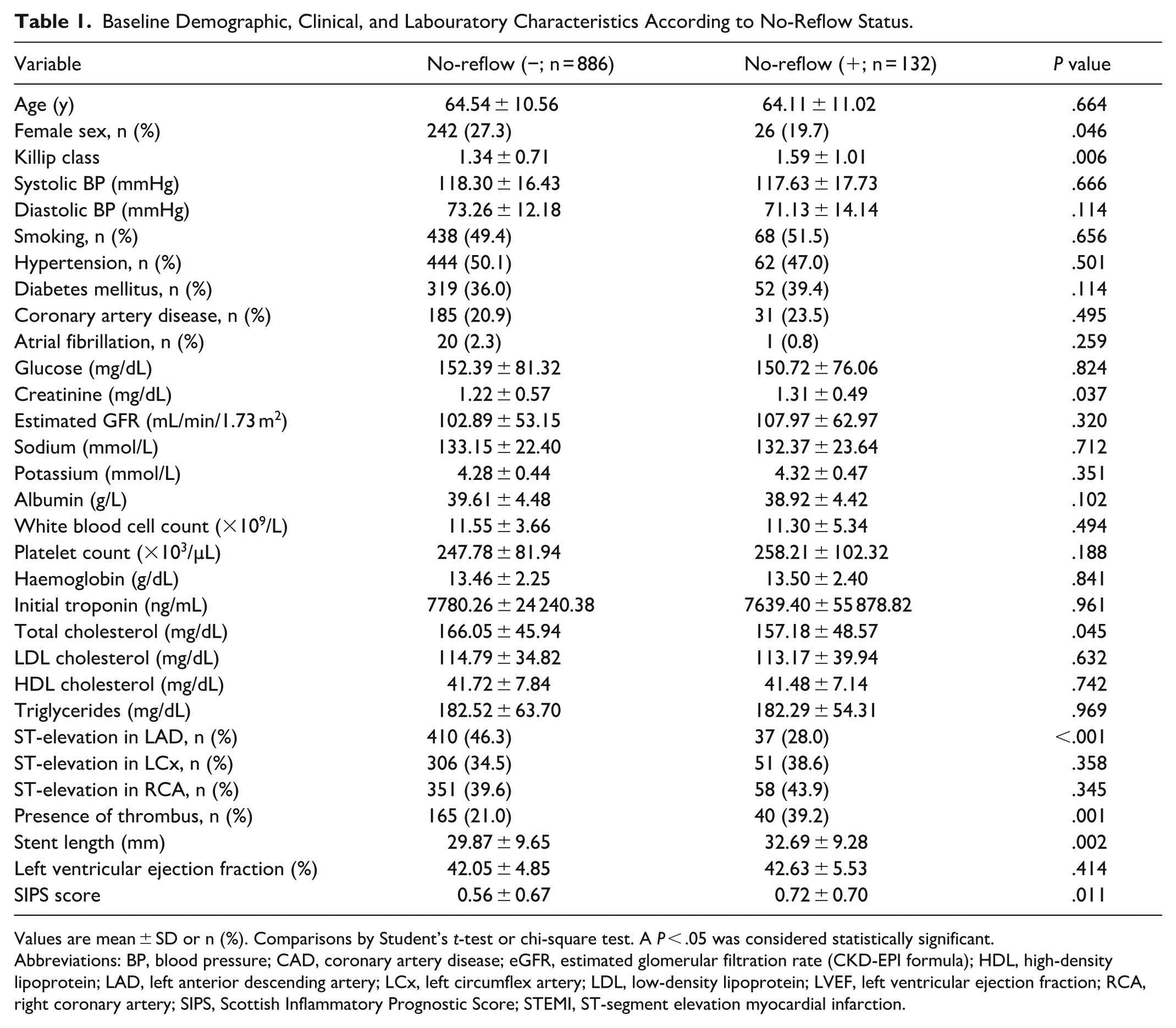
Values are mean ± SD or n (%). Comparisons by Student’s t-test or chi-square test. A P < .05 was considered statistically significant.
Abbreviations: BP, blood pressure; CAD, coronary artery disease; eGFR, estimated glomerular filtration rate (CKD-EPI formula); HDL, high-density lipoprotein; LAD, left anterior descending artery; LCx, left circumflex artery; LDL, low-density lipoprotein; LVEF, left ventricular ejection fraction; RCA, right coronary artery; SIPS, Scottish Inflammatory Prognostic Score; STEMI, ST-segment elevation myocardial infarction.
Association Between SIPS Score and No-Reflow Phenomenon
Patients were stratified into SIPS categories: low risk (score 0, n = 538), moderate risk (score 1, n = 365), and high risk (score 2, n = 115). The incidence of no-reflow increased progressively across SIPS categories: 10.2% in the low-risk, 15.9% in the moderate-risk, and 16.5% in the high-risk groups (P = .022; Table 2). Chi-square analysis confirmed a significant association between a higher SIPS score and no-reflow (Pearson χ2 = 7.641, df = 2, P = .022).
Association Between SIPS Score and No-Reflow Phenomenon.
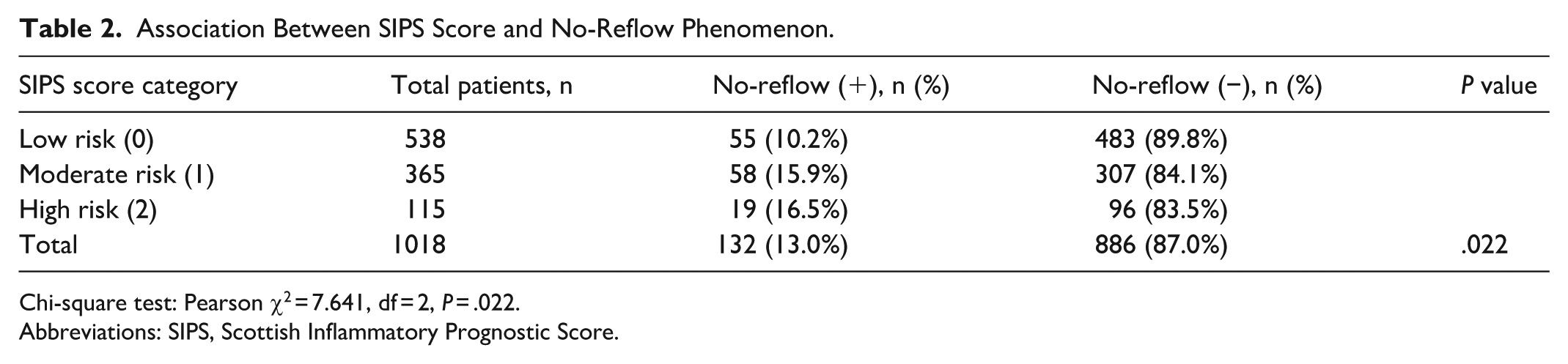
Chi-square test: Pearson χ2 = 7.641, df = 2, P = .022.
Abbreviations: SIPS, Scottish Inflammatory Prognostic Score.
Discriminative Performance of SIPS and Other Variables
Receiver operating characteristic (ROC) curve analysis was performed to assess the ability of selected variables to predict no-reflow (Table 3 and Figure 1). The area under the curve (AUC) for the SIPS score was 0.563 (95% CI 0.511-0.616; P = .019), indicating poor but statistically significant discrimination. Neutrophil count showed similar performance (AUC 0.561, 95% CI 0.510-0.612; P = .024). Diabetes mellitus, hypertension, and gender did not demonstrate significant discriminative ability (AUC 0.521, 0.484, and 0.462, respectively; all P > .05).
ROC Analysis for Variables Predicting No-Reflow.
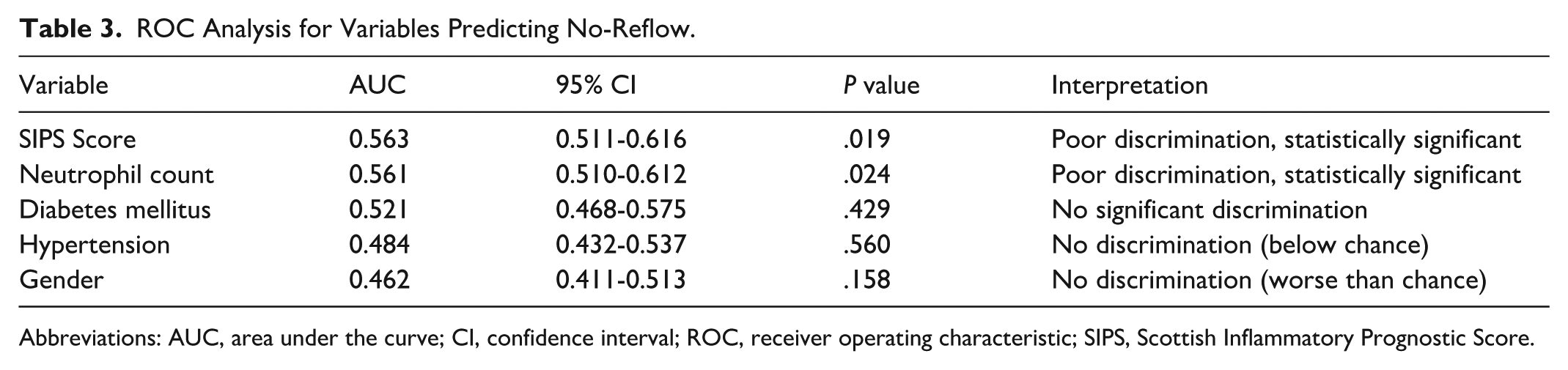
Abbreviations: AUC, area under the curve; CI, confidence interval; ROC, receiver operating characteristic; SIPS, Scottish Inflammatory Prognostic Score.
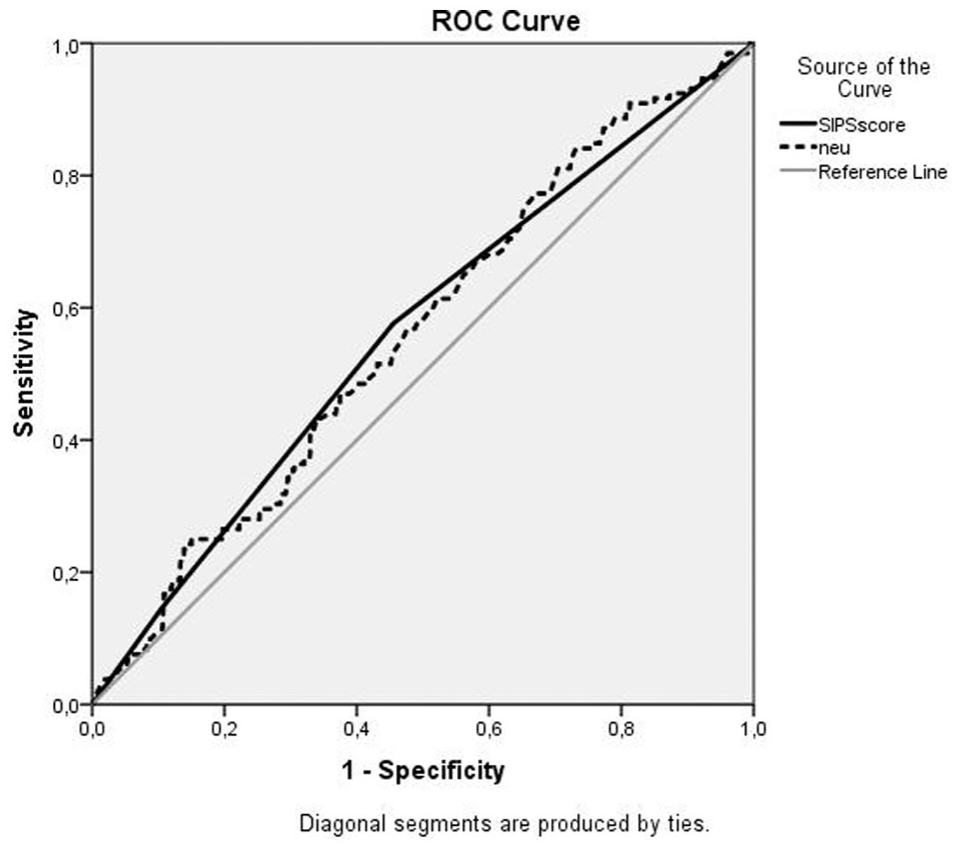
ROC curves of SIPS and neutrophil count for predicting no-reflow. The AUC was 0.563 for SIPS and 0.561 for neutrophil count. The diagonal line indicates no discrimination.
Predictors of No-Reflow Phenomenon
Univariate logistic regression analysis identified female sex (OR 1.65, 95% CI 1.01-2.70; P = .044) as significantly associated with no-reflow, while other variables, including SIPS score, did not reach significance (Supplementary Table S1).
In multivariate logistic regression analysis adjusting for female sex, age, hypertension, diabetes mellitus, neutrophil count, and albumin (Table 4), diabetes mellitus emerged as an independent predictor of no-reflow (OR 1.30, 95% CI 1.02-1.64; P = .032). Female sex showed a trend toward lower risk (OR 0.62, 95% CI 0.38-1.01; P = .053). SIPS categories (moderate vs low risk: OR 1.52, 95% CI 0.87-2.65, P = .139; high vs low risk: OR 1.46, 95% CI 0.60-3.55, P = .401) were not independently associated with no-reflow.
Multivariate Logistic Regression Analysis for Predictors of No-Reflow.
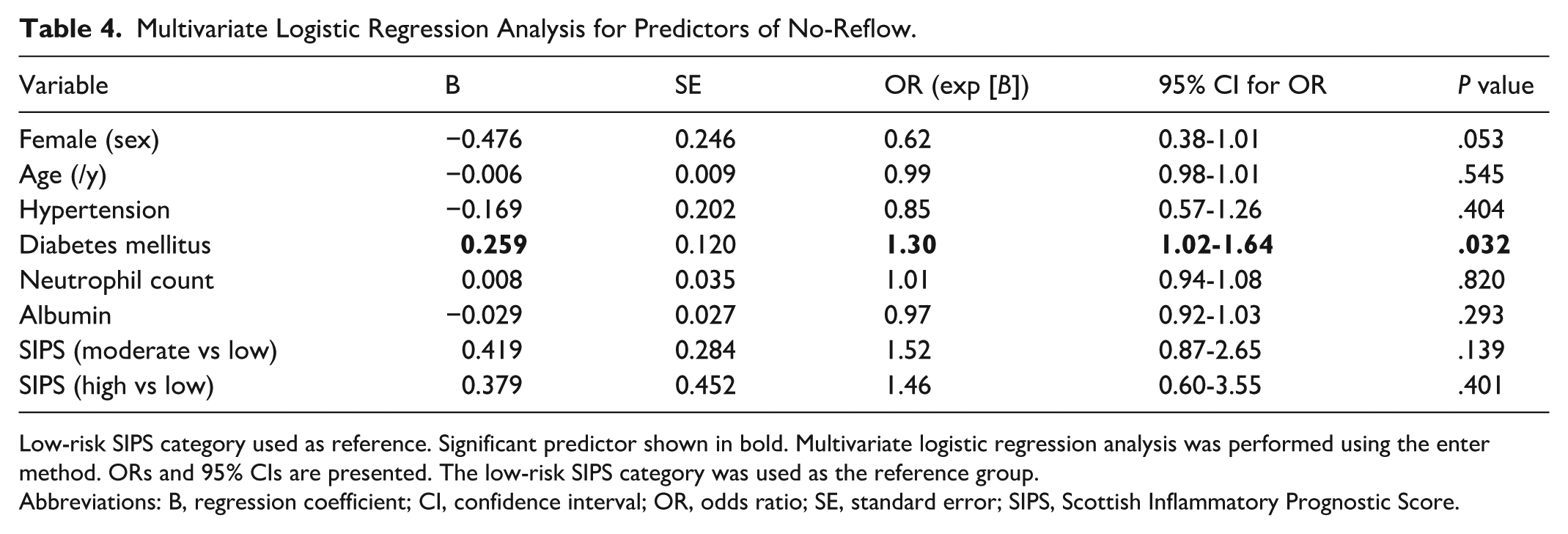
Low-risk SIPS category used as reference. Significant predictor shown in bold. Multivariate logistic regression analysis was performed using the enter method. ORs and 95% CIs are presented. The low-risk SIPS category was used as the reference group.
Abbreviations: B, regression coefficient; CI, confidence interval; OR, odds ratio; SE, standard error; SIPS, Scottish Inflammatory Prognostic Score.
The multivariate model demonstrated acceptable calibration (Hosmer-Lemeshow χ2 = 10.62, df = 8, P = .224) and overall classification accuracy of 87.0% (Table 5). The model explained a modest proportion of variance (Nagelkerke R2 = 0.030).
Performance of the Multivariate Logistic Regression Model.
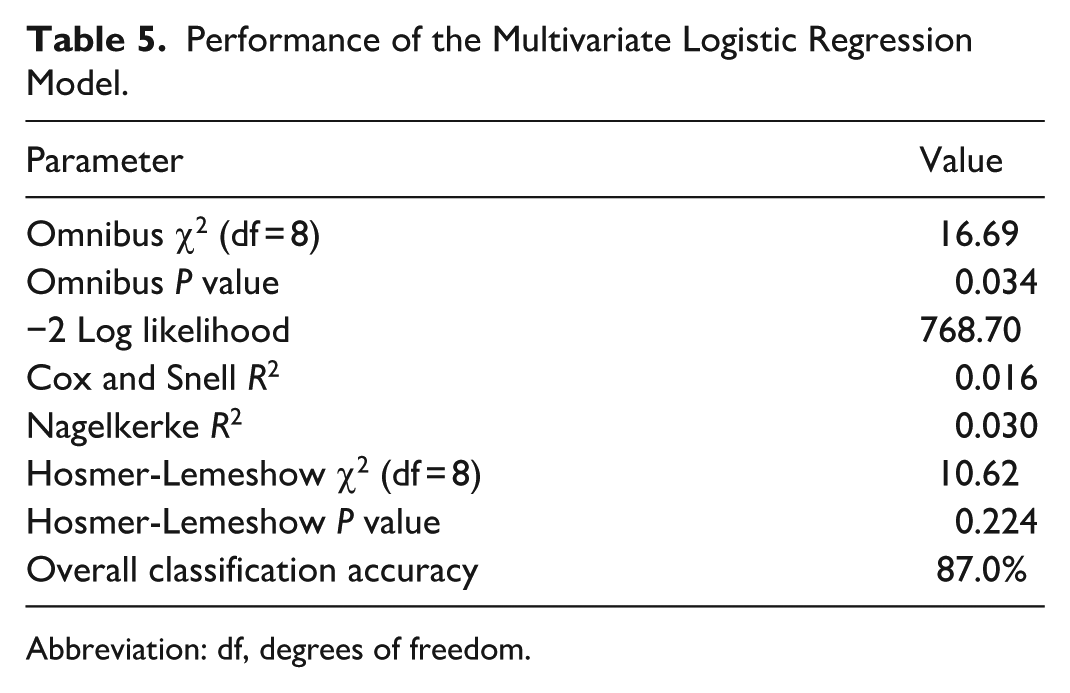
Abbreviation: df, degrees of freedom.
Discussion
We found that higher admission SIPS categories were associated with more no-reflow in 1018 STEMI patients receiving PPCI. Patients in the moderate- and high-risk SIPS groups exhibited progressively higher rates of no-reflow (15.9% and 16.5%, respectively) compared to the low-risk group (10.2%; P = .022). The SIPS score demonstrated modest but statistically significant discriminative performance (AUC 0.563; P = .019), comparable to that of neutrophil count alone. However, in multivariate analysis, SIPS did not emerge as an independent predictor of no-reflow, whereas diabetes mellitus did (OR 1.30; P = .032).
Systemic inflammation plays a pivotal role in the pathogenesis of no-reflow through mechanisms including neutrophil-mediated microvascular obstruction, endothelial dysfunction, and reperfusion injury. 13 Numerous inflammation-based indices have recently been evaluated as predictors of no-reflow in STEMI. For instance, the systemic immune-inflammation index (SII) has been shown to independently predict no-reflow, with superior discriminative ability in some cohorts.14,15 Similarly, the derived neutrophil-to-lymphocyte ratio (dNLR), inflammatory prognostic index (IPI), and haemoglobin-albumin-lymphocyte-platelet (HALP) score have demonstrated independent associations with no-reflow and related adverse outcomes in contemporary studies.16 -18
The neutrophil percentage-to-albumin ratio (NPAR) has also emerged as a robust independent predictor of no-reflow in patients undergoing PPCI. 19 These findings align with a growing body of evidence from meta-analyses confirming that heightened inflammatory responses, reflected by elevated neutrophil-based markers and hypoalbuminemia, contribute significantly to microvascular dysfunction and impaired reperfusion. 20
The graded association between SIPS and no-reflow observed in this study is biologically plausible. Elevated neutrophil counts indicate neutrophilic infiltration, degranulation, and the release of reactive oxygen species that directly hinder microvascular patency after PPCI.6,7 Hypoalbuminaemia, as a negative acute-phase reactant, worsens this effect by promoting endothelial dysfunction, increasing oxidative stress, and decreasing antioxidant capacity. 8 The SIPS combines these 2 related pathophysiological signals into a straightforward categorical score that can be easily obtained from routine admission blood tests. The observed increase in the incidence of no-reflow across SIPS categories suggests that this combined index reflects an additive inflammatory and nutritional risk burden associated with microvascular injury.
The SIPS, which integrates neutrophil count and serum albumin, 2 readily available and inexpensive parameters, offers a simple categorical approach to assessing inflammatory burden. Although SIPS showed a graded association with no-reflow in unadjusted analyses and a comparable AUC to neutrophil count, its lack of independent predictive value in multivariate modelling most likely reflects collinearity with its constituent components, both of which (neutrophil count and albumin) were entered separately as continuous variables in the regression model, effectively partitioning the SIPS signal across individual predictors. Confounding by established risk factors, particularly diabetes mellitus, thrombus burden, and stent length, may have additionally diluted the independent contribution of SIPS.
The modest discriminative performance of SIPS (AUC ~0.56) is consistent with the established pattern for single inflammatory biomarkers in this clinical context. It should be acknowledged that an AUC of 0.563, while statistically significant, falls well below the conventionally accepted threshold for clinically meaningful discrimination (AUC ≥0.70), indicating that SIPS alone is insufficient to guide clinical decision-making and should not be used as a standalone triage tool. For comparison, SII-based models have reported AUC values of 0.59 to 0.68 for no-reflow prediction, and HALP scores have demonstrated similar ranges.14,15,18 The convergence of AUC values across these indices underscores that while systemic inflammation is mechanistically central to no-reflow, no single biomarker fully captures the multifactorial aetiology of this phenomenon, which includes distal atherothrombotic embolisation, microvascular spasm, ischaemia-reperfusion injury, and patient-specific vascular biology. The categorical structure of SIPS mirrors other simple composite scoring systems recently validated for peri-procedural risk stratification in interventional cardiology. Notably, the Osaka prognostic score, a categorical composite index, has demonstrated predictive value for contrast-induced nephropathy after coronary intervention, supporting the broader utility of such readily calculable scoring tools in the catheterisation labouratory. 21
Diabetes mellitus emerged as the sole independent predictor of no-reflow in our multivariate model (OR: 1.30; P = .032). This finding is consistent with the well-recognised role of diabetes in promoting endothelial dysfunction, accelerated atherosclerosis, platelet hyperreactivity, and a prothrombotic milieu, all of which exacerbate microvascular injury during STEMI reperfusion. 22 Diabetic patients also tend to have greater thrombus burden and longer occlusion times, contributing to a higher risk of impaired myocardial perfusion after PPCI. The independent predictive value of diabetes in our adjusted model, in the absence of SIPS independence, reinforces that metabolic comorbidity status may be a more robust discriminator of no-reflow risk than admission inflammatory indices alone.
Regarding the reversal of the female sex association after multivariable adjustment, from a univariate OR of 1.65 (higher risk) to an adjusted OR of 0.62 (lower risk, P = .053), this likely reflects confounding by the differential distribution of comorbidities and angiographic characteristics across sexes in our cohort. Women in STEMI registries typically present with higher thrombus burden, smaller vessel calibre, and more complex lesion morphology, which may explain the crude univariate association; however, after adjusting for these factors, the direction of the effect reverses. This observation warrants further investigation in larger, sex-stratified cohorts.
To our knowledge, this is the first study to investigate SIPS in the context of acute coronary syndromes and specifically the no-reflow phenomenon. Prior evaluation of SIPS has been limited to oncology and, more recently, acute heart failure, where it predicted in-hospital mortality. 12 Our findings extend the potential utility of SIPS to STEMI, suggesting it may serve as a pragmatic tool for early identification of patients at elevated risk of reperfusion complications, even if not superior to more complex indices.
Several limitations warrant consideration. The retrospective design introduces potential selection bias, and the study was conducted at a single centre, limiting generalizability. Angiographic no-reflow was defined using TIMI flow grade, which, while standard, may underestimate microvascular dysfunction detectable by advanced imaging modalities. We did not assess long-term clinical outcomes or incorporate intracoronary imaging to evaluate thrombus composition or distal embolisation in detail. Furthermore, door-to-balloon time and the use of glycoprotein IIb/IIIa inhibitors, both of which may influence no-reflow rates, were not consistently available in our electronic records and could therefore not be incorporated into the regression model; these represent potentially important unmeasured confounders that may have influenced the multivariate estimates.
Conclusion
In conclusion, higher admission SIPS was associated with an increased incidence of the no-reflow phenomenon in STEMI patients undergoing PPCI, and this association followed a graded pattern across SIPS risk categories. However, SIPS did not emerge as an independent predictor of no-reflow after adjustment for established clinical risk factors; diabetes mellitus was the sole independent predictor identified in the multivariate model. These findings suggest that SIPS, while reflecting the inflammatory and nutritional burden relevant to microvascular dysfunction, does not provide incremental predictive value beyond conventional risk factors in this setting. Prospective validation in larger, multicentre cohorts is warranted before clinical implementation can be recommended.
Supplemental Material
sj-docx-1-ang-10.1177_00033197261448371 – Supplemental material for Association of the Scottish Inflammatory Prognostic Score With the No-Reflow Phenomenon in Patients With ST-Segment Elevation Myocardial Infarction
Supplemental material, sj-docx-1-ang-10.1177_00033197261448371 for Association of the Scottish Inflammatory Prognostic Score With the No-Reflow Phenomenon in Patients With ST-Segment Elevation Myocardial Infarction by Fatih Aydın, Bektas Murat and Selda Murat in Angiology
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.