
Abstract
Historically, cardiovascular disease (CVD) has often been regarded as a primarily cardiac condition. Nevertheless, recent research data suggests that this disease should be considered a multifactorial and multisystem one. In this narrative review, available evidence related to inflammatory processes, metabolic disorders, neurohormonal signaling, endothelial dysfunction, and communication between organs will be summarized to illustrate the pathophysiology of CVD. A structured search of available literature was performed using the PubMed/MEDLINE, Scopus, Web of Science, and Google Scholar databases. Only articles from 2010 to 2025 were considered to ensure that the latest developments were accounted for. The selected literature includes clinical trials, observational studies, and reviews. The analysis suggests, that all cardiovascular disorders, including heart failure, coronary artery disease, atrial fibrillation, and hypertension, have common systemic mechanisms, namely, chronic inflammation, immunological dysregulation, insulin resistance, and neurohormonal stimulation. Moreover, complex relationships exist between the heart, kidneys, liver, gastrointestinal tract, adipose tissue, and the brain, and they can lead to the aggravation of disease course. Despite promising results obtained within an integrated approach, several difficulties need to be acknowledged, among which, clinical translational issues and lack of systems-level clinical trials are of primary importance.
Keywords
Introduction: Reframing Cardiovascular Disease From a Systems Perspective
Traditional heart-focused views of cardiovascular disease (CVD) are now seen as too limited to explain its complex causes and development. 1 This is especially clear as more people live longer and often have several chronic, concurrent, conditions. 1 CVD is increasingly recognized as involving overlapping disease processes across multiple organ systems such as metabolic tissues, kidneys, liver, immune system, and nervous system.2,3 The way these diseases are connected, like in cardiorenal syndrome and metabolic syndrome, shows why we need to look beyond single-organ approaches.1,4 Shifting to a systems biology perspective is important for understanding CVD, as it helps us see how different organs interact and influence each other. 5 For example, cardiorenal syndrome shows the close relationship between the heart and kidneys, with shared mechanisms like inflammation, oxidative stress, and changes in blood flow. 4 New models, such as multi-organ-on-a-chip platforms, make it possible to study these signals between organs, especially in conditions like cardiovascular-kidney-metabolic syndrome. 6 Recent progress in understanding the molecular causes of chronic inflammation and other factors behind multiple diseases highlights the need to study how organs communicate at different levels. 1
This narrative review brings together current knowledge on inflammation, metabolism, neurohormonal signaling, and organ interactions to provide a broad view of CVD as a disorder involving many systems, mechanisms, and treatment options. Unlike many reviews that emphasize 1 biological pathway, this review considers an integrated systems approach.
Methods
The present narrative review involves data synthesis based on mechanistic, translational, and clinical aspects of multisystem cardiovascular diseases.
To identify relevant literature, a comprehensive and systematic search in PubMed/MEDLINE, Scopus, Web of Science, and Google Scholar was performed from January 2010 to March 2025. The following combinations of keywords were used: “cardiovascular disease,” “inflammation,” “immune dysregulation,” “metabolic dysfunction,” “insulin resistance,” “neurohormonal signaling,” “endothelial dysfunction,” “organ crosstalk,” and “cardiorenal syndrome.”
The included publications covered randomized controlled trials, observational studies, mechanistic studies, guidelines, and systematic narrative reviews. We excluded material not published in English, case reports, and articles unrelated to the pathophysiological aspects of cardiovascular/systemic disorders.
Overall, between 120 and 150 articles were included into the analysis. Considering the narrative nature of the review, no risk of bias assessment was conducted.
Cardiovascular Disease Beyond the Myocardium: A Multisystem Perspective
To better understand CVD, it is important to consider the involvement of several organ systems. Types of CVD, like heart failure (HF), coronary artery disease (CAD), atrial fibrillation (AF), and hypertension, share underlying causes that are not limited to the heart.7,8 These mechanisms frequently include systemic inflammation, metabolic issues, and changes in hormone signals, which work together and affect different organs. As people live longer and treatments improve, more CVD patients have 2 or more ongoing health problems (ie, multimorbidity). 1 This pattern suggests that CVD may involve systemic processes extending beyond the heart and points to the need for care that considers how these conditions interact. A systems-level perspective may improve understanding how CVD develops and supports the design of treatments that address common causes in different organs. 9 Table 1 lists the main factors and organs involved in CVD, and Figure 1 shows how the heart and other organs affect each other.
Multisystem Pathophysiological Drivers of Cardiovascular Disease.
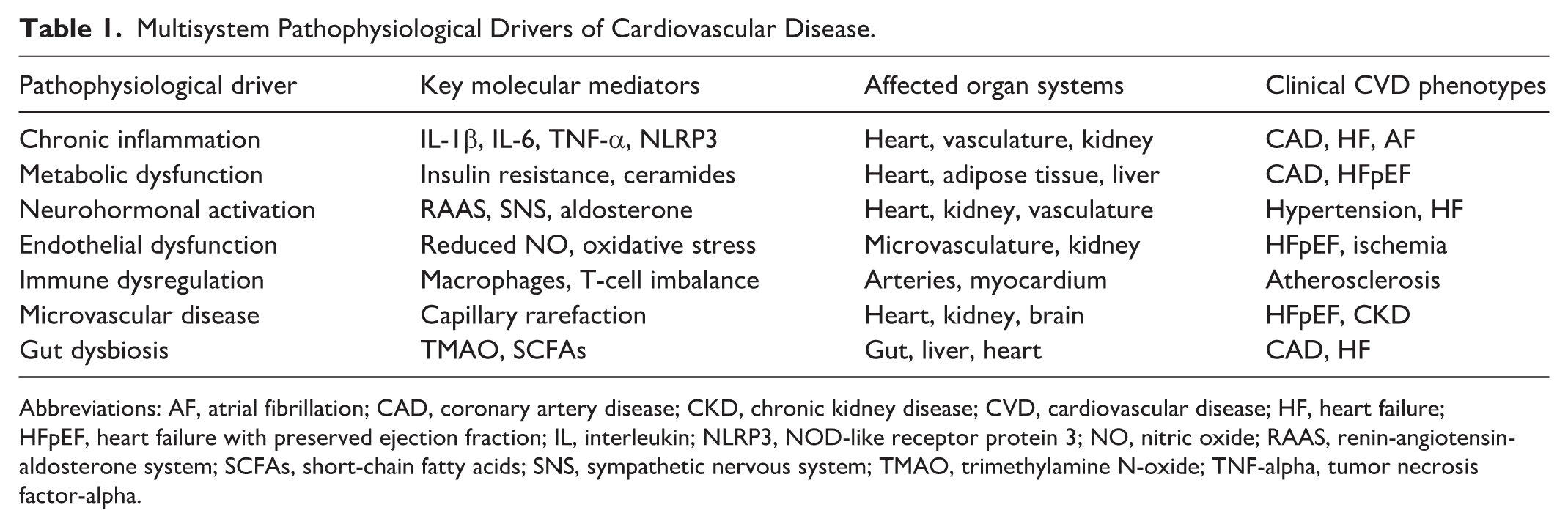
Abbreviations: AF, atrial fibrillation; CAD, coronary artery disease; CKD, chronic kidney disease; CVD, cardiovascular disease; HF, heart failure; HFpEF, heart failure with preserved ejection fraction; IL, interleukin; NLRP3, NOD-like receptor protein 3; NO, nitric oxide; RAAS, renin-angiotensin-aldosterone system; SCFAs, short-chain fatty acids; SNS, sympathetic nervous system; TMAO, trimethylamine N-oxide; TNF-alpha, tumor necrosis factor-alpha.
Cardiovascular disease as a multisystem disorder.
Inflammation and Immune Dysregulation as Core Drivers of CVD
Atherosclerosis, a major cause of CVD, is mainly a chronic inflammatory condition. 10 Both innate and adaptive immune responses play important roles in how it starts and develops. 11 These processes are often affected by chronic low-grade inflammation called “inflamm-aging.” 12 As people age, changes in the immune system make them more likely to develop CVD and have severe viral infections. 13
Important immune cells like macrophages, T cells, and B cells take part in the inflammation that happens in the walls of arteries. Macrophages in atherosclerotic plaques help the plaques grow and become unstable by releasing inflammatory cytokines and changing their behavior.14,15 Pro-inflammatory cytokines such as interleukin-1 (IL-1), IL-6, and tumor necrosis factor (TNF), as well as inflammasome activation like nucleotide-binding oligomerization domain-containing cytoplasmic proteins-like receptor protein 3 (NLRP3), play key roles in ongoing inflammation in CVD.16,17 Higher levels of inflammatory markers, such as high-sensitivity C-reactive protein and different interleukins, can help predict future cardiovascular events.11,18
Toll-like receptors (TLRs), especially those found in endosomes, detect both signals from inside the body and patterns from outside pathogens. This starts processes inside cells that lead to the release of inflammatory cytokines, which add to overall inflammation and atherosclerosis.19,20 Also, when there is an imbalance between types of T cells, like regulatory T cells and T-helper 17 cells, it creates a long-lasting pro-inflammatory state that raises the risk of CVD, particularly as people get older. 21
Although inflammation plays an essential role in the development of CVDs, studies evaluating the effects of treatments that inhibit inflammatory pathways have produced conflicting results. Indeed, while some patients may respond positively to such treatments, others will not exhibit any changes. 22 Therefore, it is evident that the mechanisms underlying inflammation are very complicated, and a treatment that targets only 1 pathway might prove ineffective.
Metabolic Dysfunction and Its Role in Cardiovascular Remodeling
Metabolic dysfunction is strongly linked to CVD through several related processes. Insulin resistance is a main factor connecting metabolic disorders to heart problems. It leads to chronic inflammation, disrupts how the body handles glucose, and increases oxidative stress, all of which help cause atherosclerotic plaques and high blood pressure.22,23 When the body becomes less sensitive to insulin, insulin levels rise and glucose metabolism gets worse. This triggers inflammation, raises pro-inflammatory cytokines, and produces more reactive oxygen species. These molecules make insulin resistance worse and add to plaque buildup in arteries and thickening of blood vessel walls, which is important in hypertension. 23
Dysfunctional fat tissue, especially around the organs and heart, is not just passive. It acts as an active endocrine organ.24,25 This tissue releases pro-inflammatory adipokines, interleukins, and tumor necrosis factor alpha, which lead to inflammation throughout the body, fat buildup in the heart and other organs, and changes in heart structure.22,25 More fat around the organs is linked to worse insulin sensitivity, more inflammation, and a higher risk of atherosclerosis.24,25
Mitochondrial dysfunction is common in heart failure and involves a steady loss of energy reserves and a shift from using fatty acids to using glucose for energy in heart cells.26,27 Although this change is meant to help, it does not restore balance and instead makes the disease worse over time. 26 This dysfunction increases oxidative stress, which leads to heart cell death, problems with calcium balance, damage to proteins and fats, and DNA leakage. These effects activate signaling pathways that cause harmful changes in the heart’s structure and lead to heart failure. 26 In addition, ketone bodies, which are important energy sources for the heart, also play roles in metabolism, inflammation, and communication between organs. Using more ketone bodies is being studied as a possible treatment for the metabolic problems that drive heart failure. 27
Changes in how the body handles fats, such as dyslipidemia and the buildup of bioactive lipids like ceramides, play a major role in the development of atherosclerosis by causing problems in blood vessel lining, inflammation, and insulin resistance.28,29 Ceramides are active sphingolipids made by a complex set of enzymes, and higher levels are linked to heart problems, obesity, and diabetes. 28 More generally, issues with fat metabolism, including changes in how fat is made and broken down, contribute to obesity, type 2 diabetes, and non-alcoholic fatty liver disease, all of which are connected to CVD. 29 Targeting fat metabolism pathways, such as those controlled by peroxisome proliferator-activated receptors (PPARs), may help improve metabolic health and lower inflammation in atherosclerosis. 30 Table 2 summarizes the main metabolic and inflammatory factors that link cardiometabolic dysfunction with changes in the heart and blood vessels.
Metabolic and Inflammatory Mediators Linking CVD and Multimorbidity.
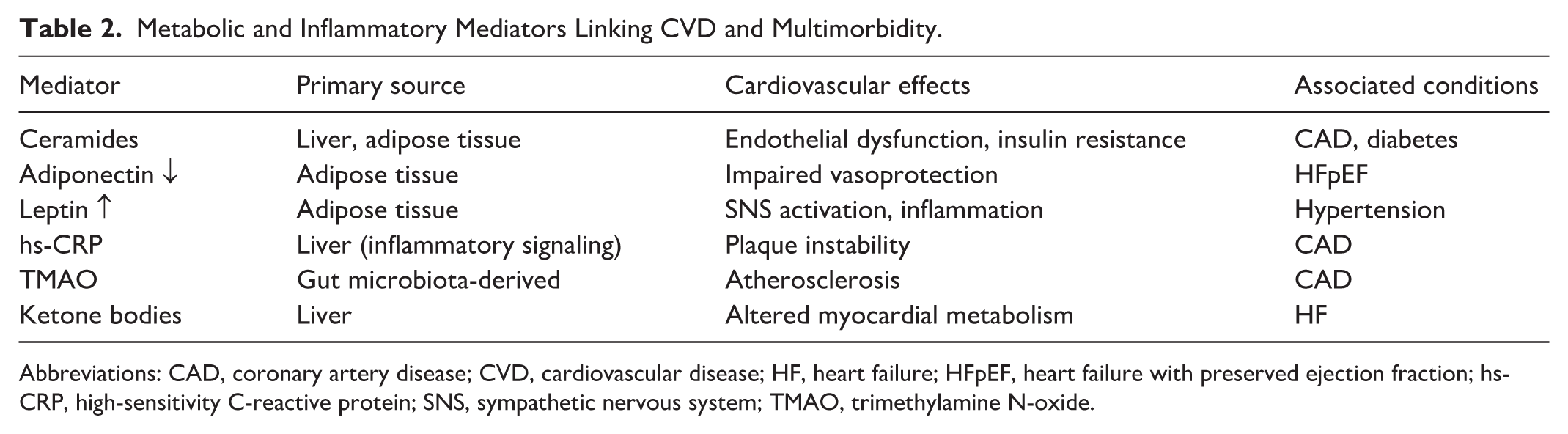
Abbreviations: CAD, coronary artery disease; CVD, cardiovascular disease; HF, heart failure; HFpEF, heart failure with preserved ejection fraction; hs-CRP, high-sensitivity C-reactive protein; SNS, sympathetic nervous system; TMAO, trimethylamine N-oxide.
Neurohormonal and Autonomic Pathways in CVD Pathogenesis
The renin-angiotensin-aldosterone system (RAAS) and sympathetic nervous system (SNS) play key roles in the development and progression of hypertension and heart failure.2,31 When the sympathetic nervous system is overactive, higher catecholamine levels can lead to endothelial dysfunction, stiffer arteries, and left ventricular hypertrophy, which push CVD from early risk factors to established illness. 31 This overactivity also raises cardiovascular risk in people with obesity, metabolic syndrome, and chronic kidney disease. 31 In addition, adrenomedullin (ADM), a natural peptide, has shown protective effects on heart structure and function in obese rats with hypertension by lowering body weight and blood pressure, and by improving inflammation and oxidative stress. 32
Harmful neurohormonal signaling can also cause changes in blood vessels and damage organs. High levels of purine metabolites in the extracellular space, along with disrupted purinergic signaling, are linked to metabolic and heart diseases. 33 Normally, estrogen signaling helps reduce inflammation and protect blood vessels, but these benefits can be lost after menopause or gender reassignment. This loss can lead to more inflammation, oxidative stress, heart muscle scarring, and problems with heart relaxation. 33 Learning more about how purinergic and estrogen signaling interact may help develop new treatments to improve heart health in older women. 33
Treatments that target neurohormonal activation have been shown to lower illness and death rates from different heart diseases. Key therapies include RAAS inhibitors, which are still vital for managing cardiovascular-kidney-metabolic (CKM) syndrome. 2 New drugs like finerenone, a non-steroidal mineralocorticoid receptor blocker, have shown potential by reversing kidney disease caused by a Western diet. They do this by improving mitochondrial metabolism, lowering fat buildup, and reducing inflammation. 34 Finerenone helps by changing how mitochondria work through estrogen-related receptor (ERR) and by reducing fat buildup, which helps prevent inflammation. 34 These treatments aim to reduce inflammation, improve metabolism, and protect organs, especially in CKM syndrome, where problems in one system can speed up decline in others.2 Figure 2 shows how inflammation, metabolism, and neurohormonal factors all play a role in changes to the heart and blood vessels.
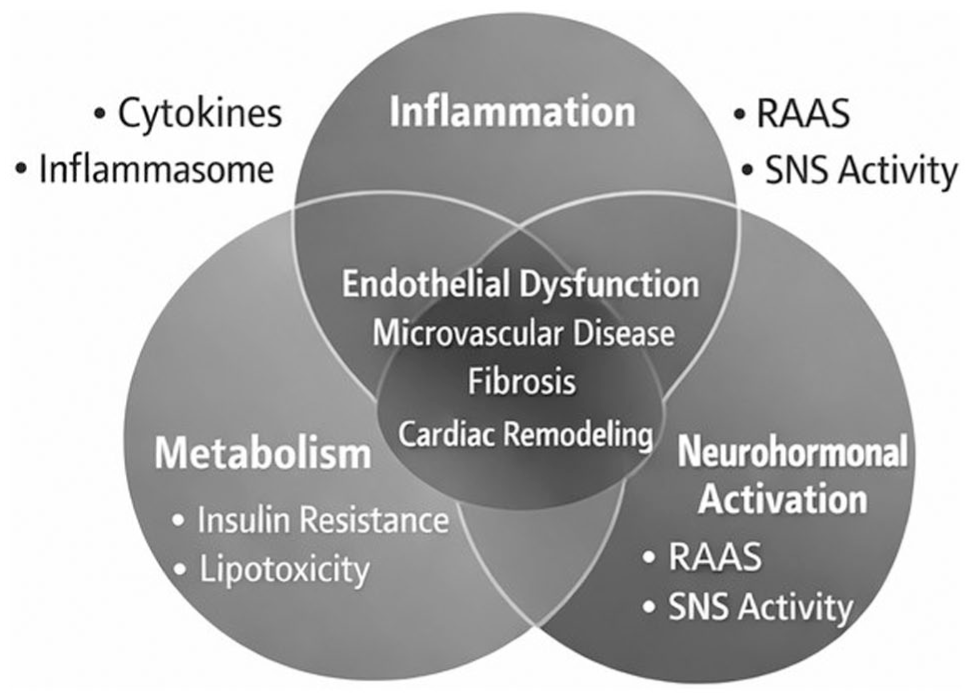
Converging pathways in cardiovascular remodeling.
Endothelial Dysfunction and the Critical Role of the Microvasculature
Endothelial dysfunction, which involves reduced nitric oxide availability and higher endothelial permeability, is an early and important step in the development of atherosclerosis and other CVDs.35 This dysfunction suggests a loss of vascular balance, as both mechanical and biochemical factors interfere with the normal control of vascular tone and permeability. 35 Inflammation in blood vessels makes this dysfunction worse by increasing reactive oxygen species, releasing chemokines and cytokines, and leading to plaque formation and instability. 36 These inflammatory responses also activate immune cells and may be related to sterile inflammation caused by Toll-like receptor 9. 20
Microvascular disease impacts several organs, such as the heart and kidneys, causing cellular problems and eventually leading to organ failure. Poor microvascular function is seen in different heart conditions, especially in heart failure with preserved ejection fraction (HFpEF), where widespread endothelial cell dysfunction is thought to be a key cause. 37
Endothelial and microvascular dysfunction can lead to many problems, including high blood pressure, reduced blood flow, and a higher risk of other heart issues. Research into cardiometabolic stress has found metabolites that highlight the shared causes of metabolic dysfunction and CVD, pointing to possible ways to improve outcomes for these related conditions. 38
Organ Crosstalk: Interconnected Systems in Cardiovascular Disease
The heart and kidneys are closely connected. Chronic kidney disease (CKD) increases the risk of CVD because both organs are affected by inflammation, oxidative stress, neurohormonal changes, and uremic toxins.4,39,40 This connection can cause cardiorenal syndrome, where a problem in one organ directly impacts the other. 41 The heart and liver also influence each other in cardiohepatic syndromes. Conditions like metabolic dysfunction-associated steatotic liver disease (MASLD) and its more severe form, metabolic dysfunction-associated steatohepatitis (MASH), increase cardiovascular risk by causing systemic inflammation, lipotoxicity, and changes in metabolic signals that affect both the heart and kidneys.42-44
The gut-heart axis highlights how gut bacteria can strongly influence heart health. When the gut microbiota is unbalanced, the gut wall may become more permeable, letting bacterial products and metabolites like trimethylamine N-oxide (TMAO) enter the bloodstream. This can cause chronic inflammation, damage to blood vessel linings, and atherosclerosis.45-47 Changes in how gut bacteria make short-chain fatty acids also affect inflammation and metabolic balance. 48 New models, such as the cardiovascular-renal-hepatic-metabolic (CRHM) syndrome, build on the CKM model by adding the liver’s important role in this network. 49 Other organ links, like the brain-heart axis, show that neurological events can affect the heart, and the heart can affect the brain through shared inflammatory and nervous system pathways.50,51 Table 3 lists the main ways organs communicate to drive CVD, and Figure 3 shows the main pathways involved in disease progression.
Organ Crosstalk Axes in Multisystem Cardiovascular Disease.
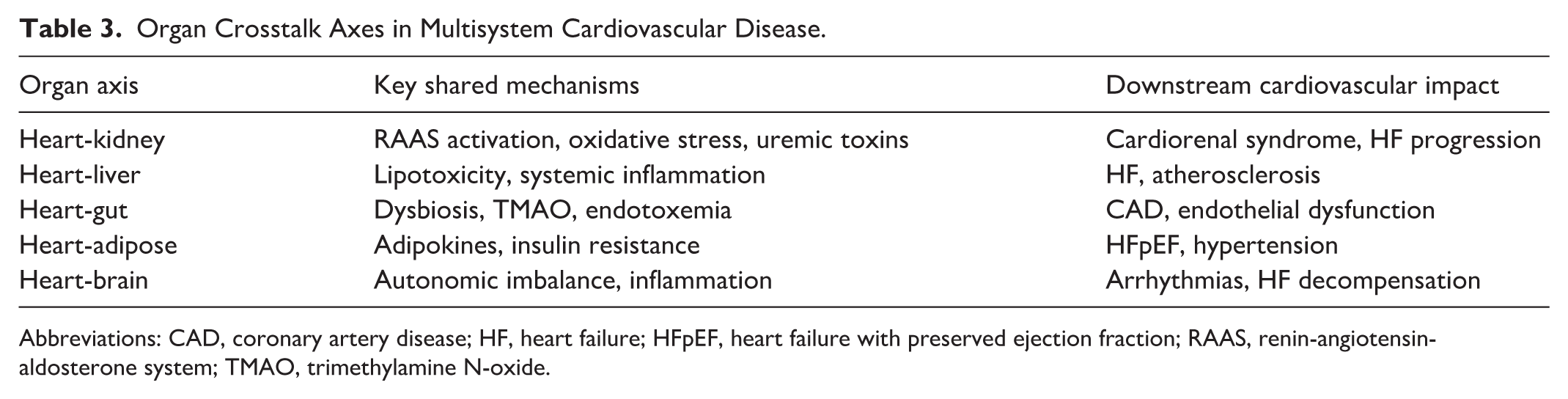
Abbreviations: CAD, coronary artery disease; HF, heart failure; HFpEF, heart failure with preserved ejection fraction; RAAS, renin-angiotensin-aldosterone system; TMAO, trimethylamine N-oxide.
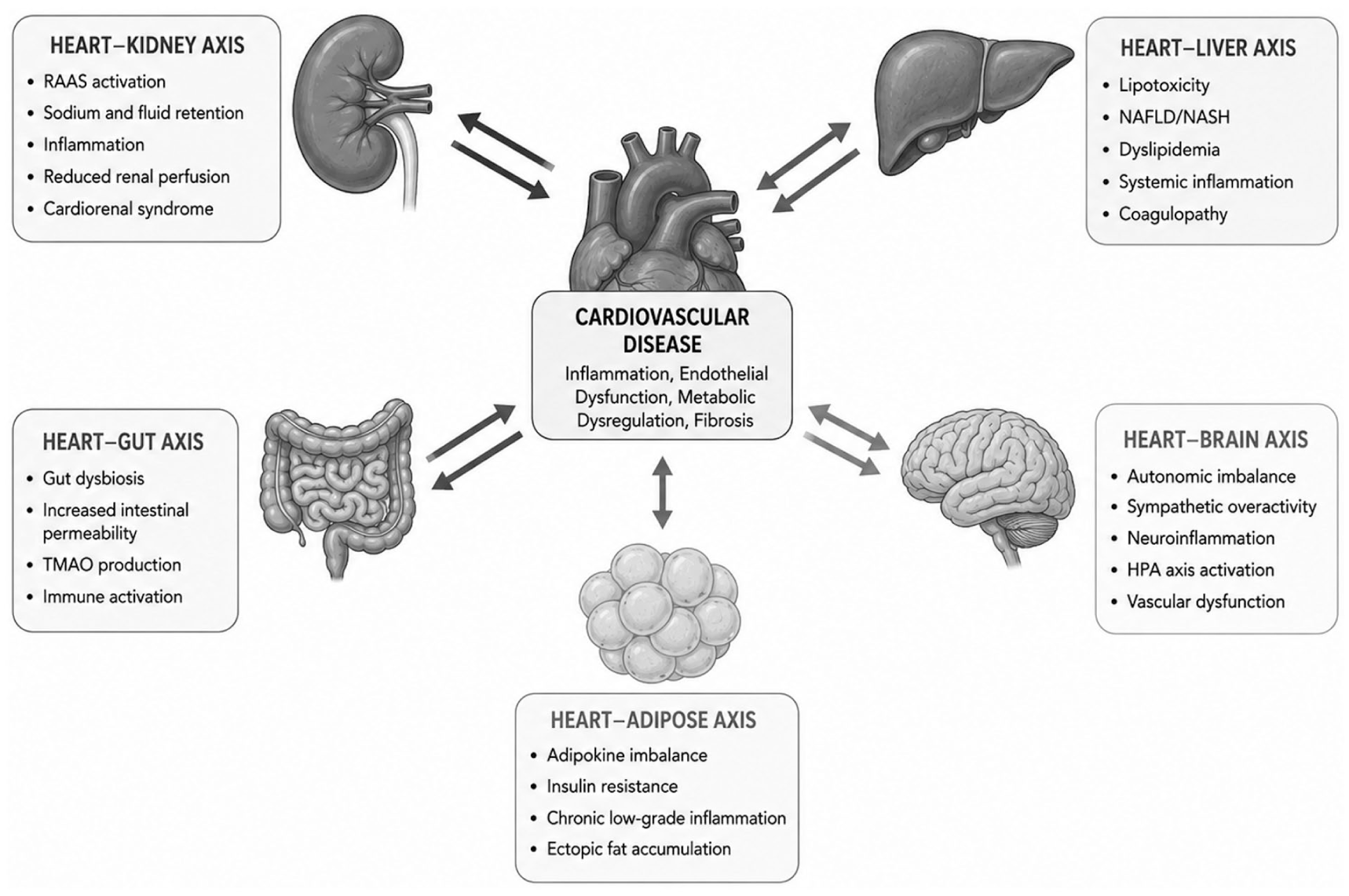
Organ crosstalk in cardiovascular disease.
Aging, Frailty, and Multimorbidity in the Context of CVD
Cardiovascular aging is a complex process that differs from simply getting older and leads to a higher risk of CVD in older adults. As people age, changes like immune system dysregulation and ongoing low-level inflammation, known as “inflammaging,” make them more likely to develop CVD and have weaker anti-viral defenses.12,13 This ongoing inflammation, along with reduced immune function, weakens the body’s ability to fight infections and increases inflammation in the cardiovascular system. 13 In addition, the changes that drive cardiovascular remodeling in conditions such as hypertension, atrial fibrillation, atherosclerosis, and heart failure are fueled by cellular aging, mitochondrial problems, and changes in the structure of heart tissue. 52
Frailty means having less physical reserve and being more vulnerable to stress, and it is an important factor that increases the risk of heart problems. It is linked to worse outcomes and less effective treatments in older adults with CVD. For example, heart transplant patients with several cardiovascular, kidney, and metabolic conditions – which often come with aging and multiple health issues – face a higher risk of death. 53
Biomarkers, Imaging, and Systems-Level Phenotyping for Multisystem CVD
Researchers are finding that using only single biomarkers does not fully capture the complex and multisystem nature of CVD. 54 By combining different types of biomarkers, comprehensive panels can provide a broader view of disease status, progression, and how organs interact. For example, genomic biomarkers like microRNA-21 (miR-21) and proteomic markers such as C-reactive protein and N-terminal pro-B-type natriuretic peptide have shown potential for predicting and diagnosing cardiorenal diseases. 54 Machine learning methods, including XGBoost, can make these biomarker panels even more effective for predicting clinical outcomes. 54
New “omics” technologies, such as proteomics, genomics, and metabolomics, are helping scientists find new biomarkers and molecular patterns that show how different body systems interact.54,55 Studies using machine learning have found genes and immune subtypes shared by heart failure and chronic kidney disease, with genes like pleckstrin homology-like domain family A member 1 (PHLDA1), ATPase Na+/K+ transporting subunit alpha 1 (ATP1A1), interferon-induced protein with tetratricopeptide repeats 2 (IFIT2), helicase-like transcription factor (HLTF), and membrane palmitoylated protein 3 (MPP3) standing out as possible diagnostic markers. 55 In addition, molecular signatures from cardiometabolic stress have identified metabolites linked to both known and new disease pathways, pointing to possible targets for improving outcomes in related conditions. 38
Imaging tools like magnetic resonance imaging (MRI), positron emission tomography (PET), computed tomography (CT), and single photon emission computed tomography (SPECT) provide valuable information about changes in structure and function across different organs, helping doctors assess overall disease burden and how organs interact.39,56 These advanced imaging methods can show important connections, such as those between the brain and heart, heart and liver, and the relationship among fat, muscle, and heart, which helps us better understand cardiometabolic diseases. 56 Molecular imaging, especially for the heart-kidney connection, can look at key processes like pro-fibrotic signaling, inflammation, and nerve health. Table 4 lists biomarkers and imaging methods that can capture multisystem CVD.
Biomarkers and Imaging Approaches for Systems-Level CVD Phenotyping.

Abbreviations: CMR, cardiac magnetic resonance; CVD, cardiovascular disease; HF, heart failure; hs-CRP, high-sensitivity C-reactive protein; IL, interleukin; NT-proBNP, N-terminal pro-B-type natriuretic peptide; PET, positron emission tomography.
Therapeutic and Clinical Implications: Multi-Target and Precision Approaches
Because CVD affects multiple systems, treating just 1 pathway often leaves other related problems unresolved, which can result in less effective outcomes. 57 This has led to the development of treatments that target several pathways at once. For example, drugs like sodium-glucose cotransporter 2 (SGLT2) inhibitors and glucagon-like peptide-1 (GLP-1) receptor agonists have broad effects that help the heart, kidneys, and metabolism at the same time.2,58
Precision medicine uses patient phenotyping and detailed “-omics” data to match treatments to each person’s unique needs, aiming for personalized care that addresses each patient’s specific problems.9,55 For example, immunophenotyping in clinical trials can identify immune patterns and help choose patients who are most likely to benefit from certain immunotherapies. 57 While anti-inflammatory treatments show promise for diseases like atherosclerosis, they must be used carefully to avoid the risks of suppressing the immune system too much. 57 One of the main challenges is to develop ways to target specific inflammatory pathways without affecting the whole immune system.57,59 Table 5 summarizes current treatments that have effects on multiple systems, highlighting the move toward more integrated care.
Therapeutic Strategies Targeting Multisystem Pathways in CVD.
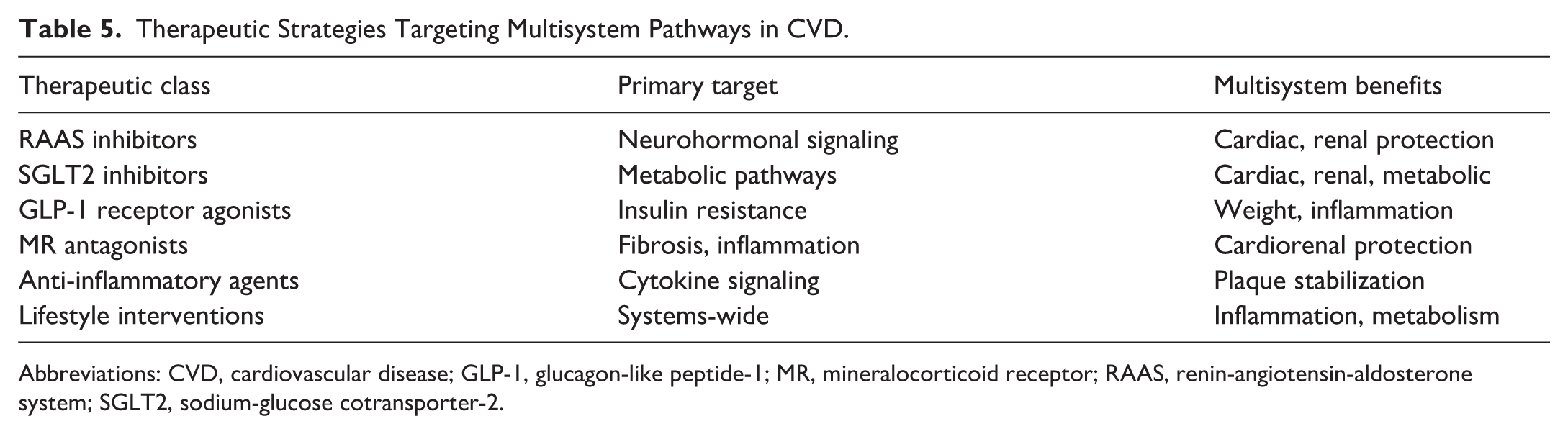
Abbreviations: CVD, cardiovascular disease; GLP-1, glucagon-like peptide-1; MR, mineralocorticoid receptor; RAAS, renin-angiotensin-aldosterone system; SGLT2, sodium-glucose cotransporter-2.
Future Directions and Knowledge Gaps in Multisystem CVD Research
Although there has been progress, much about multisystem CVD is still unclear. More research is needed to understand the complex molecular mechanisms behind organ crosstalk and to find new treatment targets where inflammation, metabolism, and neurohormonal signaling meet. New tools like computational models and multi-organ-on-a-chip platforms can help investigate these interactions and speed up the search for better ways to diagnose and treat multisystem CVD.
Key research areas include how the gut microbiome interacts with the body in different types of CVD, looking at how disease develops and responds to treatment in men and women, and examining how environmental and lifestyle factors affect CVD beyond the usual risk factors.45,60,61 These trials should use broad biomarker panels and advanced imaging to show how treatments affect all related organs.
Limitations and Controversies
In spite of the increasing awareness regarding the nature of CVD as a multisystem condition, there are still several limitations and controversies. The present review has obvious limitations inherent to narrative reviews, such as the presence of selection bias and inability to provide an objective assessment of available literature comparable to systematic reviews and meta-analyses. Moreover, while many of the findings connecting multiple system pathways and CVD are supported by experimental evidence, few of them have been clinically verified on a wide scale.
Even though biomarker analysis and the use of “omics” techniques allow for gaining deeper understanding of CVD’s multisystem character, their usefulness for clinical purposes is questionable due to lack of reproducibility, standardization, and high costs of the analyses. Additionally, there is controversial evidence about the impact of targeting single mechanisms, such as inflammation and metabolic dysfunction, on patients’ outcomes.
Conclusion
Cardiovascular disease is a multisystem disorder driven by interconnected pathways involving inflammation, metabolic dysfunction, neurohormonal activation, endothelial injury, and organ crosstalk. A systems-based framework may improve phenotyping, risk stratification, and therapeutic targeting beyond traditional organ-centered models. Future studies should validate integrated biomarkers and multimodal treatment strategies in prospective clinical trials.
Footnotes
Abbreviations
ADM – Adrenomedullin
AF – Atrial fibrillation
ATP1A1 – ATPase Na+/K+ transporting subunit alpha 1
CAD – Coronary artery disease
CKD – Chronic kidney disease
CKM – Cardiovascular-kidney-metabolic
CRHM – Cardiovascular-renal-hepatic-metabolic
CRP – C-reactive protein
CT – Computed tomography
CVD – Cardiovascular disease
DNA – Deoxyribonucleic acid
ERR – Estrogen-related receptor
GLP-1 – Glucagon-like peptide-1
HF – Heart failure
HFpEF – Heart failure with preserved ejection fraction
HLTF – Helicase-like transcription factor
IFIT2 – Interferon-induced protein with tetratricopeptide repeats 2
IL – Interleukin
IL-1 – Interleukin-1
IL-6 – Interleukin-6
MASLD – Metabolic dysfunction-associated steatotic liver disease
MASH – Metabolic dysfunction-associated steatohepatitis
MAFLD – Metabolic-associated fatty liver disease
miR-21 – MicroRNA-21
MRI – Magnetic resonance imaging
NLRP3 – NOD-, LRR-, and pyrin domain-containing protein 3
NOD – Nucleotide-binding oligomerization domain
NT-proBNP – N-terminal pro-B-type natriuretic peptide
PET – Positron emission tomography
PHLDA1 – Pleckstrin homology-like domain family A member 1
PPAR – Peroxisome proliferator-activated receptor
RAAS – Renin-angiotensin-aldosterone system
ROS – Reactive oxygen species
SGLT2 – Sodium-glucose cotransporter 2
SGLT2i – Sodium-glucose cotransporter 2 inhibitors
SNS – Sympathetic nervous system
SPECT – Single photon emission computed tomography
TLR – Toll-like receptor
TLR9 – Toll-like receptor 9
TMAO – Trimethylamine N-oxide
TNF – Tumor necrosis factor
TNF-α – Tumor necrosis factor alpha
Author Contributions
All authors contributed to: (1) substantial contributions to conception and design, or acquisition of data, or analysis and interpretation of data, (2) drafting the article or revising it critically for important intellectual content, and (3) final approval of the version to be published.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was not supported by any specific grant from public, commercial, or non-profit funding agencies.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.