
Abstract
Pulmonary embolism (PE) remains a major cause of cardiovascular mortality, and early identification of high-risk patients is essential. The uric acid-to-albumin ratio (UAR) has emerged as a marker reflecting systemic inflammation. This study aimed to evaluate the prognostic value of UAR for in-hospital mortality in patients with acute PE. This single-center, retrospective study included 1052 consecutive patients diagnosed with acute PE. Clinical characteristics, laboratory parameters, echocardiographic findings, and pulmonary imaging results were obtained from hospital records. Multivariable logistic regression analyses were performed to identify independent predictors of in-hospital mortality. The discriminative performance of UAR was assessed using receiver operating characteristic (ROC) curve analysis. Overall, 70 patients (6.7%) died during hospitalization. Non-survivors had significantly higher UAR values compared with survivors (2.33 vs 1.57, P < .001). In multivariable analysis, UAR C-Reactive Protein, and Pulmonary artery severity index (PESI) score independently predicted in-hospital mortality. UAR demonstrated acceptable discriminative ability (Area under the curve .728; 95% CI: .649-.807; P < .001), with an optimal cut-off of 2.12. The combined use of UAR and PESI demonstrated a modest improvement in predictive performance. UAR is an independent predictor of in-hospital mortality in patients with acute PE. Its combination with the PESI score may provide incremental value for early risk stratification.
Introduction
Pulmonary embolism (PE) is a potentially life-threatening cardiovascular disorder resulting from obstruction of the pulmonary arteries, most commonly by thromboembolic material from the venous system. 1 It represents the third most frequent cardiovascular disease after myocardial infarction and stroke. 2
The clinical presentation of PE ranges widely—from mild dyspnea or chest pain to sudden cardiovascular collapse—making diagnosis often challenging and delayed.3,4 Early diagnosis and accurate risk stratification are crucial to reducing mortality in acute PE. According to the European Society of Cardiology (ESC) guidelines, both the Pulmonary Embolism Severity Index (PESI) and its simplified version (sPESI) are validated prognostic tools for estimating short-term mortality risk.5,6 However, their predictive performance may be enhanced when combined with biochemical or inflammatory biomarkers, leading to growing research interest in identifying novel prognostic markers that improve early risk prediction.6,7
Uric acid is the final product of purine metabolism and serves as a marker of oxidative stress and inflammation, whereas albumin has important antioxidant and anti-inflammatory properties.8-10 The uric acid to albumin ratio (UAR) has recently emerged as a novel index reflecting the balance between systemic inflammation and oxidative stress. 11 Increased oxidative stress contributes to cardiovascular disease through mechanisms involving endothelial injury, inflammation, thrombogenesis, and vascular dysfunction. 11 Recent studies have demonstrated that elevated UAR levels are associated with worse outcomes in various cardiovascular conditions, including acute coronary syndrome, myocardial infarction, atrial fibrillation, and advanced coronary artery disease.11-13
Therefore, the present study aimed to investigate whether the UAR is an independent predictor of in-hospital mortality in patients with acute PE.
Methods
We conducted a single-center, retrospective, observational study including 1052 consecutive patients who were hospitalized with a confirmed diagnosis of acute PE between January 2015 and December 2024 at the University of Health Sciences, Dr. Siyami Ersek Thoracic and Cardiovascular Surgery Training and Research Hospital (Istanbul, Türkiye). The diagnosis of PE was confirmed by computed tomography pulmonary angiography (CTPA) in all patients.
Patients with missing laboratory data, or those with chronic inflammatory or infectious diseases, autoimmune disorders, chronic liver disease, chronic kidney disease, or malignancies that could affect albumin or uric acid levels were excluded from the analysis. The study was conducted in accordance with the Declaration of Helsinki, and the study protocol was approved by the institutional ethics committee.
The patients were divided into 2 groups according to in-hospital mortality. Demographic characteristics, comorbidities, vital signs at admission, laboratory results, electrocardiographic and echocardiographic findings, and CTPA parameters were obtained from the electronic hospital records. Clinical risk stratification was performed using the PESI and sPESI scores at the time of hospital admission. All patients were followed during hospitalization, and in-hospital outcomes were recorded. Treatment strategies for acute PE were determined by experienced physicians in accordance with contemporary guideline recommendations. 14 Patients with high-risk PE or hemodynamic instability received systemic thrombolytic therapy when clinically indicated. Anticoagulation and other medical treatments were initiated based on individual patient characteristics and clinical judgment following guideline-based risk stratification. Detailed data regarding specific anticoagulant agents were not consistently available and were therefore not included in the analysis. Transthoracic echocardiography (Vivid-7, General Electric, Milwaukee, WI, USA) was performed by experienced cardiologists blinded to clinical outcomes. Left ventricular ejection fraction (LVEF), right ventricular (RV) dimensions, tricuspid annular plane systolic excursion (TAPSE), pulmonary artery systolic pressure (PASP), and presence of RV dysfunction or D-shaped septum were recorded. All patients underwent CTPA to confirm diagnosis and evaluate embolism localization (massive, submassive, bilateral, or subsegmental).
Venous blood samples were collected at admission before initiation of specific therapy for PE. Serum uric acid and albumin levels were measured using an automated biochemical analyzer Beckman coulter automated CBC Analyzer (Beckman Coulter, Inc., Fullerton, CA, USA). The UAR was calculated by dividing the serum uric acid (mg/dL) by the serum albumin (g/dL) level. Routine biochemical parameters and complete blood count were analyzed simultaneously. Estimated glomerular filtration rate (eGFR) was calculated using the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) formula. 15
Statistical Analyses
Continuous variables were tested for normality using the Kolmogorov–Smirnov test. Normally distributed data were expressed as mean ± standard deviation (SD) and compared using the independent samples t-test, whereas non-normally distributed variables were presented as median (interquartile range [IQR]) and compared using the Mann–Whitney U test. Categorical variables were expressed as counts and percentages and compared using the Chi-square or Fisher’s exact test, as appropriate.
To identify predictors of in-hospital mortality, univariable logistic regression analysis was first performed for all clinical, laboratory, and echocardiographic parameters. Variables with P < .10 in univariable analysis or deemed clinically relevant were subsequently included in the multivariable logistic regression model. Odds ratios (ORs) with corresponding 95% confidence intervals (CIs) were reported.
Receiver operating characteristic (ROC) curve analysis was conducted to assess the discriminative ability of the UAR for predicting in-hospital mortality. The area under the curve (AUC) and optimal cut-off value were determined using Youden’s index.
To evaluate the incremental prognostic value of the UAR beyond established clinical risk stratification, 2 nested logistic regression models were constructed. The baseline model included the PESI score alone, while the extended model included PESI score plus UAR. Both models were fitted in the same patient cohort with complete data. Incremental predictive value was assessed using the likelihood ratio test.
Clinical utility was further evaluated using decision curve analysis, which was performed to compare the net benefit of the PESI-only model and the PESI + UAR model across a range of clinically relevant threshold probabilities. Risk reclassification was assessed using a category-based net reclassification index (NRI) with predefined risk categories (<5%, 5%-10%, and ≥10%).
Model calibration was evaluated using the Hosmer–Lemeshow goodness-of-fit test and graphical calibration analysis. Calibration plots were generated using bootstrap resampling with 200 repetitions to assess agreement between predicted and observed risks. Assumptions of logistic regression were examined by assessing multicollinearity using variance inflation factors, evaluating model residuals, and identifying influential observations using Cook’s distance.
All statistical analyses were performed using IBM SPSS Statistics version 27 (IBM Corp., Armonk, NY, USA), MedCalc (Version 20.104, Ostend, Belgium), and R statistical software (R Foundation for Statistical Computing, Vienna, Austria). A 2-sided P-value < .05 was considered statistically significant in all analyses.
Results
A total of 1052 patients diagnosed with acute PE were included in the study. Of these, 70 patients (6.7%) died during hospitalization, while 982 patients (93.3%) survived. Baseline demographic, clinical, and laboratory characteristics of the study population according to survival status are presented in Table 1.
Baseline Demographic, Clinical, and Laboratory Characteristics of the Study Population According to In-hospital Mortality.
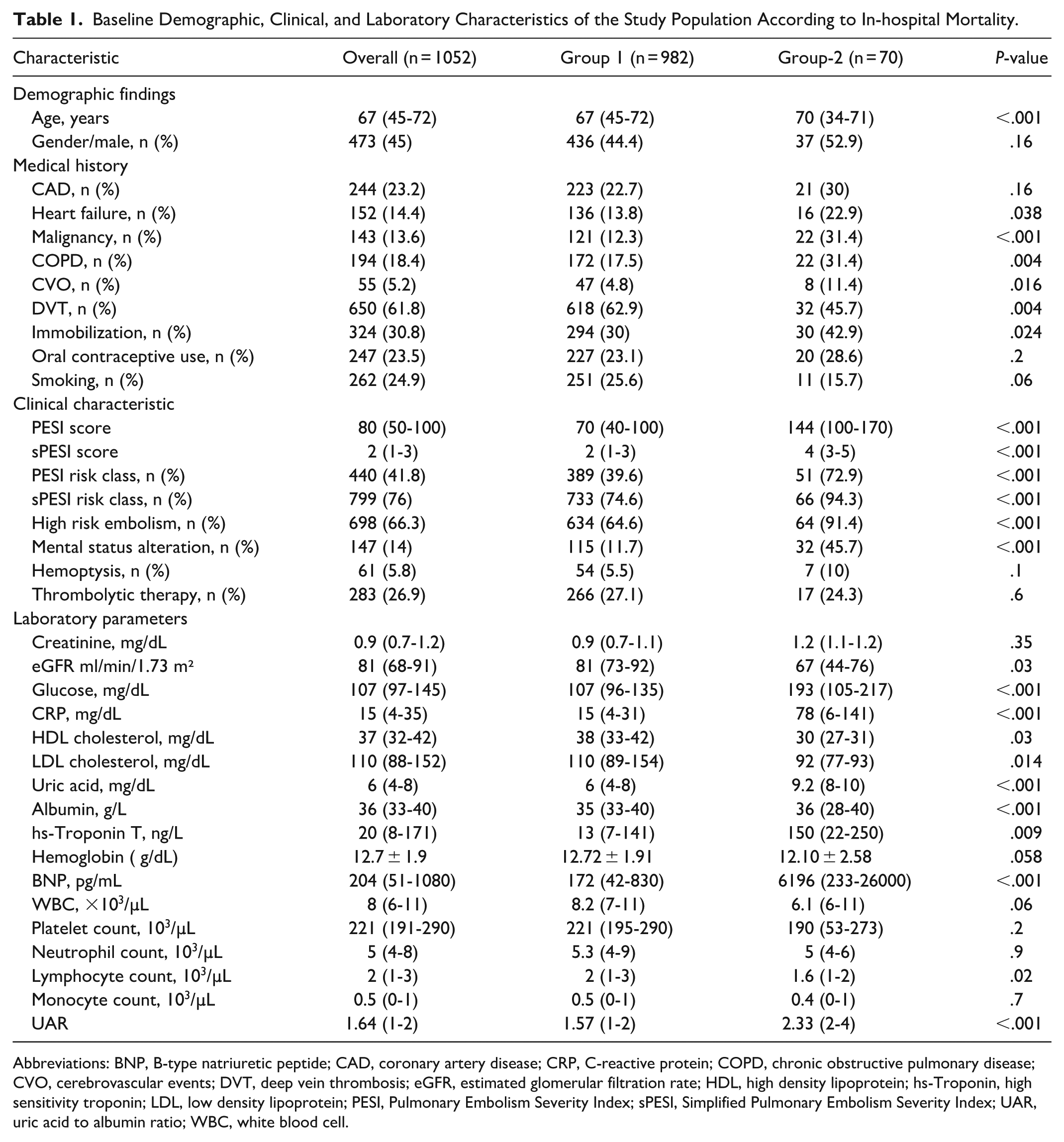
Abbreviations: BNP, B-type natriuretic peptide; CAD, coronary artery disease; CRP, C-reactive protein; COPD, chronic obstructive pulmonary disease; CVO, cerebrovascular events; DVT, deep vein thrombosis; eGFR, estimated glomerular filtration rate; HDL, high density lipoprotein; hs-Troponin, high sensitivity troponin; LDL, low density lipoprotein; PESI, Pulmonary Embolism Severity Index; sPESI, Simplified Pulmonary Embolism Severity Index; UAR, uric acid to albumin ratio; WBC, white blood cell.
Non-survivors were significantly older and more likely to have comorbidities such as heart failure, malignancy, chronic obstructive pulmonary disease (COPD), cerebrovascular events, and immobilization. Conversely, deep vein thrombosis (DVT) was more frequent among survivors compared with non-survivors (62.9% vs 45.7%, P = .004). Clinical severity indices were significantly higher among patients who died during hospitalization. Both the PESI and the sPESI scores were markedly elevated in non-survivors compared with survivors (median PESI: 144 [100-170] vs 70 [40-100]; P < .001; median sPESI: 4 [3-5] vs 2 [1-3]; P < .001). Likewise, high-risk embolism was substantially more common among non-survivors (91.4% vs 64.6%; P < .001). Mental status alteration at presentation was also significantly associated with mortality (45.7% vs 11.7%; P < .001). Hemoptysis and thrombolytic therapy rates did not differ significantly between the groups.
Laboratory analysis revealed that non-survivors had higher levels of C-reactive protein (CRP), glucose, uric acid, troponin, and B-type natriuretic peptide (BNP), whereas eGFR, high-density lipoprotein (HDL), and lymphocyte counts were significantly lower compared with survivors (P < .05 for all). The median UAR was markedly higher in the mortality group compared with survivors (2.33 [2-4] vs 1.57 [1-2]; P < .001).
Imaging and electrocardiographic findings are summarized in Table 2. Non-survivors had a significantly lower LVEF, larger left and right ventricular diameters, higher pulmonary artery systolic pressure (PASP), and more frequent right ventricule (RV) dysfunction and D-shaped septum on echocardiography (all P < .001). Atrial fibrillation and Electrocardiography (ECG) changes were also more prevalent among non-survivors. However, the presence of an S1Q3T3 pattern did not differ significantly between survivors and non-survivors (P = 0.2). Computed tomography findings showed that massive PE was more common in patients who died during hospitalization (P = .03), whereas the prevalence of bilateral embolism was similar between the groups (P = .12).
Imaging Findings of the Study Population According to In-hospital Mortality.
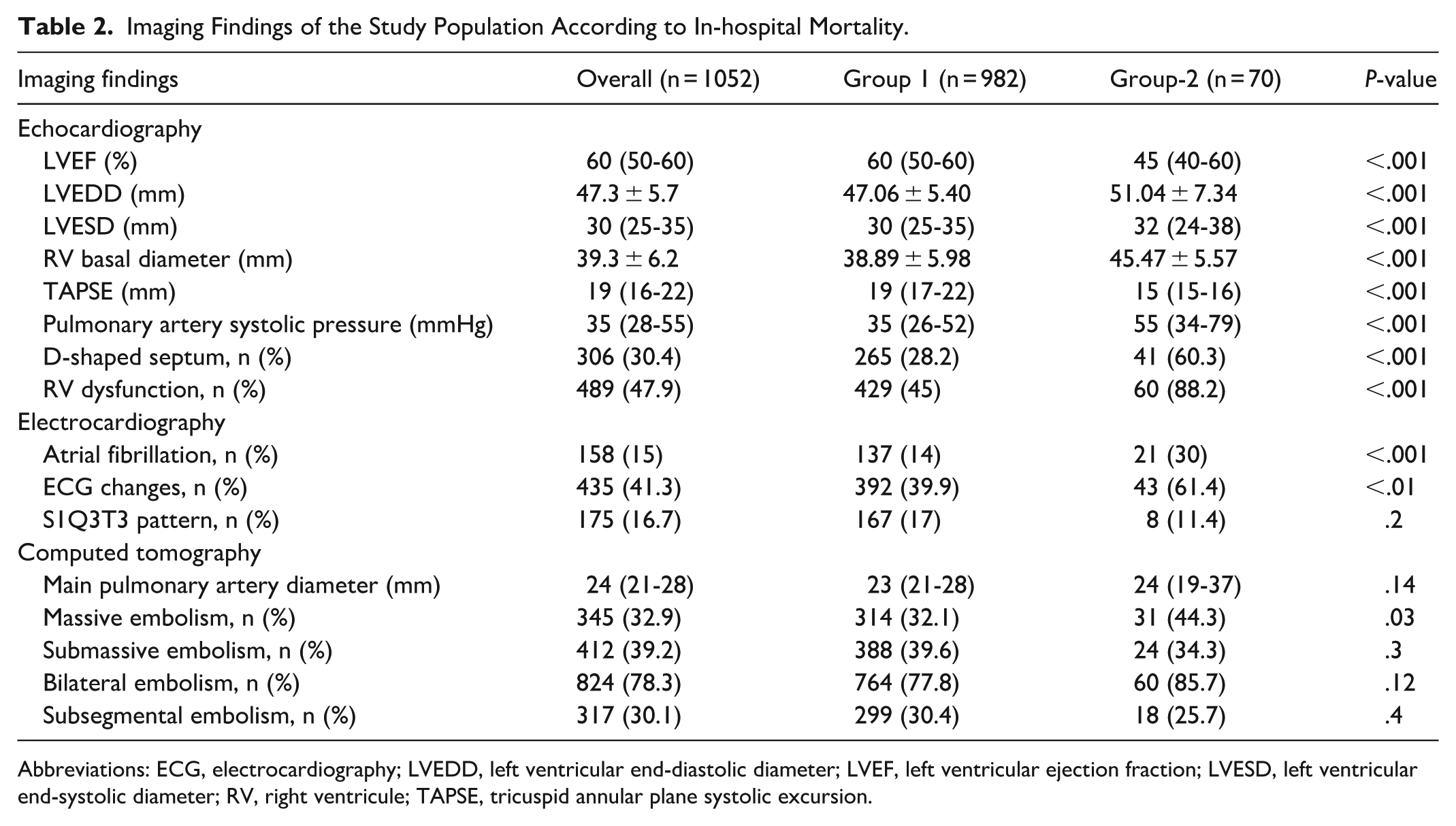
Abbreviations: ECG, electrocardiography; LVEDD, left ventricular end-diastolic diameter; LVEF, left ventricular ejection fraction; LVESD, left ventricular end-systolic diameter; RV, right ventricule; TAPSE, tricuspid annular plane systolic excursion.
In univariable logistic regression analysis (Table 3), Smoking, CRP, ECG changes, PESI score, massive PE, and UAR were significantly associated with in-hospital mortality. In the multivariable logistic regression model, PESI score (OR: 1.02, 95% CI: 1.02-1.03, P < .001), CRP (OR: 1.008, 95% CI: 1.00-1.02, P = .01) and UAR (OR: 1.17, 95% CI: 1.01-1.36, P = .03) remained as independent predictors of in-hospital mortality.
Univariable and Multivariable Logistic Regression Analyses for Predictors of In-hospital Mortality.
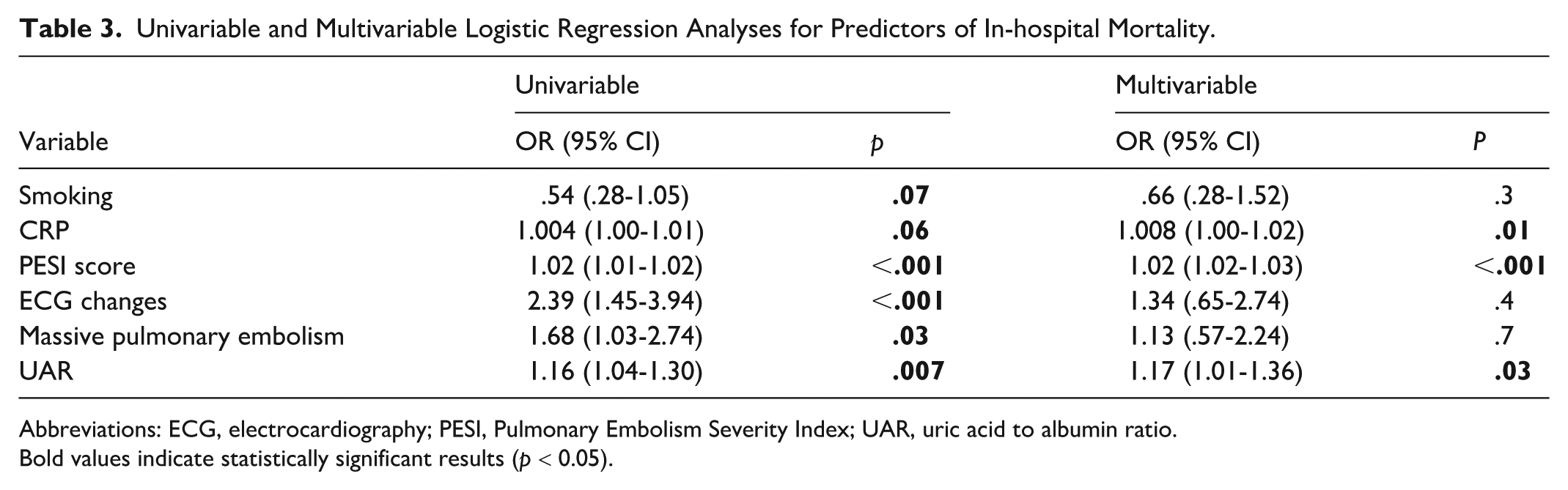
Abbreviations: ECG, electrocardiography; PESI, Pulmonary Embolism Severity Index; UAR, uric acid to albumin ratio.
Bold values indicate statistically significant results (p < 0.05).
The receiver operating characteristic (ROC) curve analysis demonstrated that the UAR had an acceptable discriminative ability for predicting in-hospital mortality, with an area under the curve (AUC) of .728 (95% CI: .649-.807, P < .001). The optimal cut-off value of UAR was 2.12, providing 62.7% sensitivity and 74.9% specificity. The PESI score showed a higher discriminative performance, with an AUC of .822 (95% CI: .757-.886, P < .001). The optimal cut-off value of the PESI score was 129.5, corresponding to a sensitivity of 62.7% and a specificity of 89.1%. When UAR was combined with the PESI score, the predictive performance slightly improved, with an AUC of .829 (95% CI: .763-.895, P < .001; Figure 1).
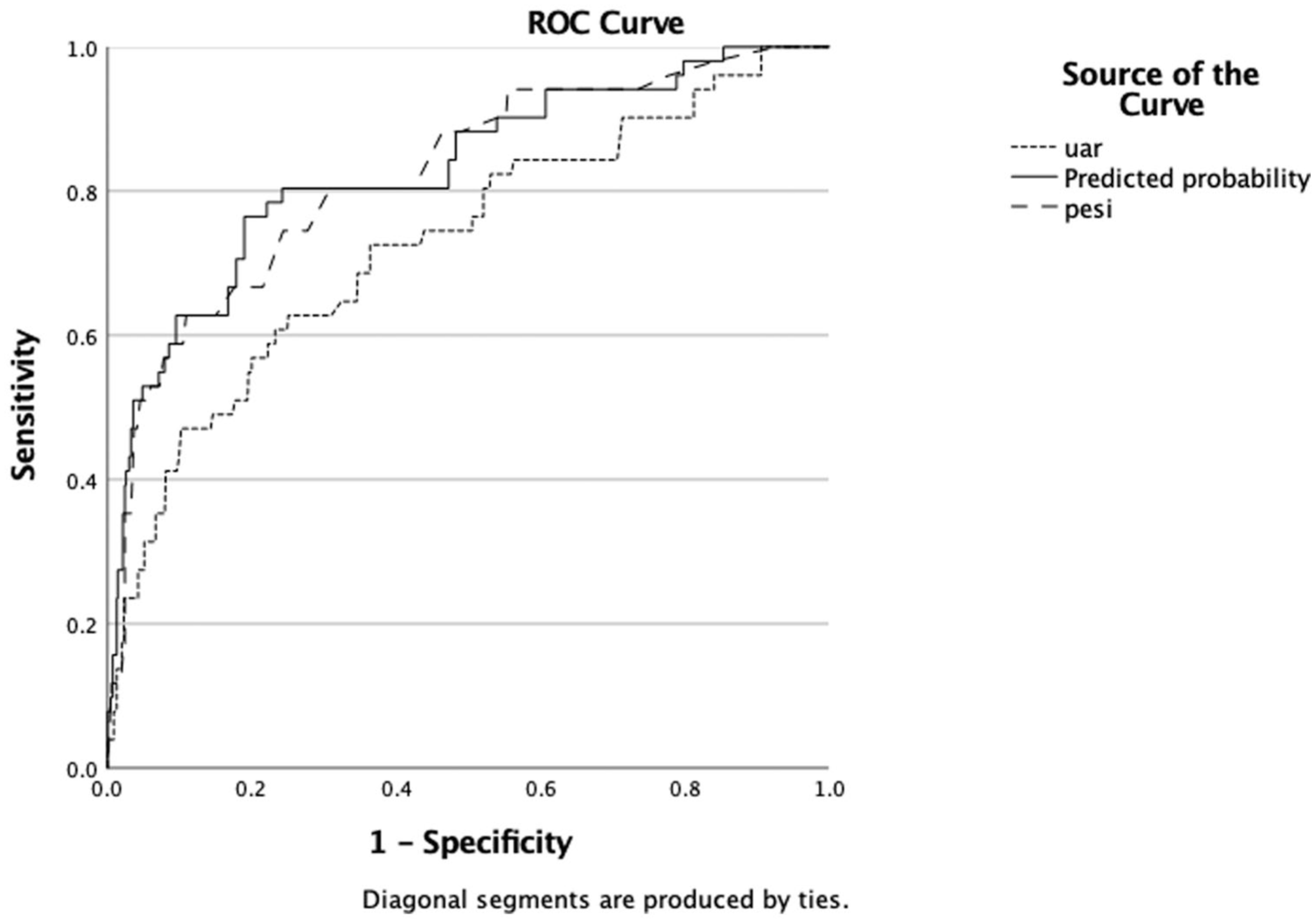
Receiver operating characteristic (ROC) curves comparing the predictive performance of the uric acid to albumin ratio (UAR), PESI score, and their combination for in-hospital mortality. The ROC curve analysis shows the discriminative performance of UAR, PESI score, and their combination for predicting in-hospital mortality. The area under the curve (AUC) was .728 (95% CI: .648-.807) for UAR, .822 (95% CI: .757-.886) for the PESI score, and .829 (95% CI: .763-.895) for the combined model. The addition of UAR to the PESI score resulted in a slight increase in AUC.
In incremental predictive analyses, the addition of the UAR to the PESI significantly improved model performance for predicting in-hospital mortality. In nested logistic regression models fitted in the same patient cohort with complete data, inclusion of UAR resulted in a significant improvement in model fit compared with the PESI-only model, as demonstrated by the likelihood ratio test (χ2 = 10.66, P = .001).
Decision curve analysis demonstrated that the model including PESI and UAR provided a higher net benefit than the PESI-only model across a range of clinically relevant threshold probabilities, indicating improved clinical utility for risk stratification (Supplemental Figure S1).
Risk reclassification analysis further supported the incremental prognostic value of UAR. Category-based NRI analysis showed that patients who experienced in-hospital mortality were more frequently reclassified into higher risk categories, whereas patients without events were more often reclassified into lower risk categories when UAR was added to the PESI-based model.
Model calibration was acceptable for the extended model including UAR. The Hosmer–Lemeshow goodness-of-fit test showed no significant deviation between predicted and observed risks (χ2 = 14.89, df = 8, P = .061), and bootstrap calibration plots demonstrated good agreement between predicted and observed probabilities across most of the risk spectrum (Supplemental Figure S2). Model diagnostic analyses revealed no major violations of logistic regression assumptions, with no evidence of multicollinearity or influential observations (Supplemental Figures S3-S4).
Discussion
According to our findings, a higher UAR was significantly associated with in-hospital mortality in patients with acute PE. To the best of our knowledge, this is the first study to demonstrate a direct relationship between UAR and in-hospital mortality in this clinical setting.
Acute PE remains a major cause of cardiovascular morbidity and mortality worldwide, despite advances in diagnostic imaging and therapeutic strategies.3,16 A considerable proportion of cases are diagnosed late or (remain unrecognized until autopsy), leading to rapid hemodynamic compromise, RV failure, or sudden death.17-19 Most fatalities occur within the first few days of hospitalization, underscoring the importance of early risk stratification and prompt management.20,21 Therefore, the identification of simple, cost-effective, and reliable prognostic biomarkers is of great importance to improve short-term outcomes in this population.
Despite advances in diagnostic imaging and therapeutic strategies, in-hospital mortality remains a major concern in patients with acute PE. 22 Reported short-term mortality rates range from 5% to 15%, depending on clinical severity and the presence of comorbid conditions.13,23,24 In our cohort, the in-hospital mortality rate was 6.7%, which is consistent with previously published data. 16 Several clinical and laboratory factors have been identified as predictors of early mortality in PE, including advanced age, malignancy, heart failure, COPD, hypotension, hypoxemia, elevated cardiac biomarkers, and RV dysfunction.23-26 Our results were largely in line with these findings—non-survivors were significantly older, had higher PESI and sPESI scores, lower LVEF, and a greater prevalence of malignancy, COPD, cerebrovascular disease, and RV dysfunction. We observed that DVT was more common among survivors. This finding, may indicate that patients with concomitant DVT present earlier, receive timely anticoagulation, and are less likely to have massive central embolism.
Inflammation and oxidative stress play a pivotal role in the pathogenesis and progression of acute PE.27,28 The inflammatory response contributes to endothelial dysfunction, thrombus propagation, and vascular remodeling. 27 Uric acid, the final product of purine metabolism, serves as both a marker and mediator of oxidative stress. 10 Elevated uric acid levels can induce endothelial injury, stimulate platelet activation, and reduce nitric oxide bioavailability, all of which may aggravate pulmonary vascular resistance and RV dysfunction.29-31 Several studies have demonstrated that hyperuricemia is associated with unfavorable outcomes in wide range of cardiovascular conditions.29-31
In contrast, albumin exerts antioxidant, anti-inflammatory, and antithrombotic effects. 32 Low serum albumin levels may reflect systemic inflammation, impaired hepatic synthesis, or increased vascular permeability, and have been independently associated with adverse cardiovascular events.13,33,34 Hypoalbuminemia also indicates poor nutritional and metabolic status, which can further amplify oxidative injury and inflammation in patients with PE. 34
The UAR combines these 2 opposing biochemical mechanisms—oxidative stress and antioxidant defense—into a single, easily measurable index. Previous studies have reported that an elevated UAR correlates with worse prognosis in acute coronary syndrome, myocardial infarction, atrial fibrillation, and chronic heart failure.35-37 Consistent with these observations, our study demonstrated that a higher UAR was significantly associated with increased in-hospital mortality in patients with acute PE and remained an independent predictor after multivariable adjustment. In the multivariable regression analysis, PESI score, CRP and UAR emerged as independent predictors of in-hospital mortality, emphasizing the prognostic value of integrating biochemical and clinical parameters. Furthermore, ROC curve analysis confirmed the discriminative ability of UAR in predicting in-hospital mortality, with an AUC of .728, indicating acceptable accuracy. The PESI score showed a higher predictive performance compared to UAR alone. Importantly, when UAR was combined with the PESI score, a slight increase in the discriminative performance was observed. Although this improvement was modest, it suggests that UAR may provide complementary information beyond traditional clinical parameters. These results suggest that UAR may reflect the combined inflammatory and oxidative burden that contributes to early hemodynamic deterioration and adverse outcomes in acute PE.
In the present study, UAR provided incremental prognostic information beyond established clinical risk stratification tools. Although PESI remains the cornerstone for risk assessment in acutePE, our findings demonstrate that incorporation of UAR significantly improves risk prediction. This incremental value was consistently supported by likelihood ratio testing, risk reclassification analysis, and decision curve analysis, suggesting that UAR captures additional pathophysiological information not fully reflected by clinical risk scores alone. Importantly, the added prognostic value of UAR was not limited to statistical improvement but also translated into clinical benefit. Decision curve analysis demonstrated a higher net benefit for the PESI + UAR model across clinically relevant threshold probabilities, indicating that incorporation of UAR may improve clinical decision-making, particularly in identifying patients at higher risk of in-hospital mortality who may benefit from closer monitoring or intensified management strategies. The robustness of these findings is further supported by comprehensive model diagnostics. The extended model demonstrated good calibration, absence of multicollinearity, and no influential observations, indicating that the observed associations are unlikely to be driven by model misspecification or statistical artifacts.
This study has several limitations. First, it was a single-center, retrospective analysis, which may be subject to selection bias and temporal changes in clinical practice. Second, only in-hospital outcomes were assessed; therefore, the long-term prognostic significance of the UAR remains uncertain. Third, detailed nutritional markers beyond serum albumin, lifestyle-related factors (such as dietary habits, alcohol consumption, and physical activity), and comprehensive data on concomitant medications were not systematically available and could not be fully adjusted for, which may have resulted in residual confounding. Hence, large-scale, prospective multicenter studies with serial biomarker assessment are warranted to validate and expand our findings.
Conclusion
The present study demonstrates that the UAR is an independent predictor of in-hospital mortality in patients with acute PE. As an easily obtainable and cost-effective biomarker derived from routine laboratory parameters, UAR may provide incremental prognostic information beyond conventional clinical risk scores. Incorporating UAR into existing risk stratification models could help clinicians identify high risk patients earlier and improve short-term outcomes in acute PE.
Supplemental Material
sj-docx-1-ang-10.1177_00033197261460519 – Supplemental material for Predictive Value of the Uric Acid-to-Albumin Ratio for In-Hospital Mortality in Acute Pulmonary Embolism
Supplemental material, sj-docx-1-ang-10.1177_00033197261460519 for Predictive Value of the Uric Acid-to-Albumin Ratio for In-Hospital Mortality in Acute Pulmonary Embolism by Semih Eren, Murat Gökalp, Özge Çebi Gökalp, Özdemir Gümüşdağ, Semanur Vural, Gönseli Miray Özdemir, Gündüz Durmuş and Mehmet Baran Karataş in Angiology
Footnotes
Author Contributions
All authors contributed to: (1) substantial contributions to conception and design, or acquisition of data, or analysis and interpretation of data, (2) drafting the article or revising it critically for important intellectual content, and (3) final approval of the version to be published.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.