
Abstract
Objective:
This study aimed to determine the success of oral alimentation and patient retention rate 1 to 5 days after passing the Yale Swallow Protocol.
Methods:
Participants were 200 consecutive acute care inpatients referred for swallow assessment. Inclusion criteria were adequate cognitive abilities to participate safely, completing an oral mechanism examination, and passing the 3-ounce water swallow challenge. Exclusion criteria were altered mental status, failing the 3-ounce challenge, preadmission dysphagia, head-of-bed restrictions < 30°, and a tracheotomy tube. Electronic medical record monitoring post-protocol passing for 1 to 5 consecutive days determined success of oral alimentation and retention rate.
Results:
All patients who remained medically and neurologically stable drank thin liquids and ate successfully 1 to 5 days after passing the protocol. Mean (SD) volume of liquid ingested per day was 474.2 (435.5) cc. Patient retention declined steadily from day of testing (n = 200) through post-testing day 5 (n = 95).
Conclusion:
Passing the Yale Swallow Protocol allowed for initial determination of aspiration risk followed by successful oral alimentation for 1 to 5 days in medically and neurologically stable acute care hospitalized patients and without the need for instrumental dysphagia testing. The decline in patient retention was expected because of increasingly rapid transit through the acute care setting, which often renders longer follow-up problematic.
Introduction
In today’s health care environment, optimal patient care, as demonstrated by successful evidence-based interventions, is demanded by both insurers and providers. The 2004-2005 National Hospital Discharge Survey reported that comorbid dysphagia in patients ≥ 75 years of age resulted in a 40% increase in length of stay (2.4 vs 4.0 days), an additional 223 027 hospitalization days per year, and a staggering cost of $547 307 964. 1 Therefore, avoidance of prandial pulmonary aspiration as a cause of nosocomial infection is an important goal for all acute care hospitalized patients deemed at risk for aspiration.
Referral for a swallow evaluation must result in use of a validated tool with the dual capabilities to reliably determine aspiration risk and appropriately recommend oral alimentation. It is surprising that no studies, to date, reported > 24 hours of follow-up for oral feeding status based upon passing either a swallow screen or an instrumental dysphagia evaluation. It is not surprising that the realities of the acute care setting have limited the ability to track and collect longitudinal data due to acute medical or neurological status changes, rapid discharge from inpatient to home or extended care facilities, and billing regulations that preclude follow-up after a negative test result.
Three studies from the acute care setting reported on ≤ 24 hours of success for oral alimentation recommendations. Twenty-four hours after passing the Yale Swallow Protocol 2 and remaining medically and neurologically stable, all intensive care unit, 3 stroke, 4 and general hospital 5 patients were both eating and drinking successfully. Although supportive of short-term benefits, a longer follow-up period is needed to demonstrate either continued success of oral alimentation or record potential overt aspiration events later in the patient’s clinical course. It is important to note that the focus of the present investigation was not to determine adequacy of oral nutrition and hydration in hospitalized patients. The purposes of the present study were to investigate longer term success of oral alimentation recommendations and hospital retention rate for up to 5 days after passing the Yale Swallow Protocol. 2
Methods
Subjects
This study was approved by the Human Investigation Committee, Yale School of Medicine. Each patient was referred for a swallow assessment and administered the Yale Swallow Protocol 2 by an experienced speech-language pathologist. Inclusion criteria were adequate cognitive abilities to participate safely in the protocol, 6 completion of an oral mechanism examination, 7 and passing the 3-ounce water swallow challenge. 8 Exclusion criteria were severely altered mental status precluding safe participation in the protocol, failing the 3-ounce water swallow challenge, a current modified consistency diet due to a pre-existing dysphagia, head-of-bed restrictions < 30°, and presence of a tracheotomy tube.3-5 Referred patients who failed the protocol were not included.
Procedures
Yale Swallow Protocol
The Yale Swallow Protocol 2 incorporated, validated, and generalized use of the 3-ounce water swallow challenge component, originally used in isolation with a small (n = 44) cohort of stroke patients in the rehabilitation setting, 9 to a large (n = 3000) and heterogeneous (14 diagnostic categories) sample of hospitalized individuals. 8 Subsequent double-blinded objective testing with fiberoptic endoscopic evaluation of swallowing (FEES)7,10 and videofluoroscopic swallow studies (VFSS) 11 confirmed that all participants who passed the protocol also did not aspirate, that is, sensitivity of 100% and negative predictive value of 100%.
The Yale Swallow Protocol 2 has 3 components: (1) a 3-ounce water swallow challenge 8 ; (2) a brief cognitive screen composed of 3 orientation questions (What is your name? Where are you right now? What year is it?) and 3 single-step directions (Open your mouth. Stick out your tongue. Smile.) 6 ; and (3) an oral mechanism examination that assessed labial closure, lingual range of motion, and facial symmetry (smile/pucker), 7 with the latter 2 again using a large and heterogeneous sample of hospitalized individuals (n = 4102). It is important to note that results of the brief cognitive screen 6 and oral mechanism examination 7 provide the clinician information only on odds of aspiration risk with the 3-ounce water swallow challenge and should not necessarily be used as exclusionary criteria for screening. The reason is that some patients will pass the 3-ounce challenge component despite altered mental status and impaired oral mechanism functioning.
Each participant was administered the Yale Swallow Protocol 2 by experienced speech-language pathologists with more than 10 years of protocol administration. Passing required uninterrupted drinking (assisted or independent) of 3 ounces of water from a cup or with a straw and with no overt signs of aspiration risk (ie, cough). Failure was inability to drink the entire amount, interrupted drinking, or coughing during or immediately after drinking. When passed, an oral diet was recommended based on combined results of the cognitive screen, oral mechanism examination, and dentition status. For example, edentulous patients were usually recommended a liquid and puree consistency diet whereas dentate patients a soft or regular diet. When failed, either continued nil per os status with repeat screening in 24 hours or FEES was done immediately. When failed, the options are continued nil per os status with repeat screening in 24 hours, FEES done immediately at bedside, or VFSS performed within 24 hours.
Data collection
Standard oral intake as routinely entered by nursing in each patient’s electronic medical record allowed for retrieval of the total volume of liquid ingested for days 1 to 5. Nurses were blinded to the oral intake purpose of the study. A pre-existing protocol directed nursing to discontinue the oral diet and reconsult speech-language pathology if overt signs of prandial aspiration occurred (eg, coughing or choking). Patient retention rate required passing the protocol and then with no overt signs of aspiration risk at meal times, stable medical and neurological status, and not discharged from the hospital between day of testing and day 5.
Results
A consecutively referred sample (August 15, 2011–December 1, 2011) of 200 inpatients from a large, urban, acute care, teaching hospital participated. All patients were referred for a swallow assessment by a physician, physician assistant, or licensed independent provider.
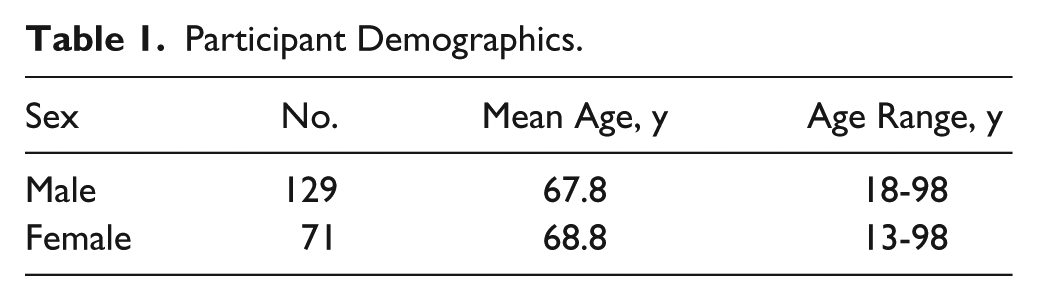
Table 1 shows participant demographics including age and sex. Table 2 shows admitting diagnostic categories.
Participant Demographics.
Participant Diagnostic Categories.
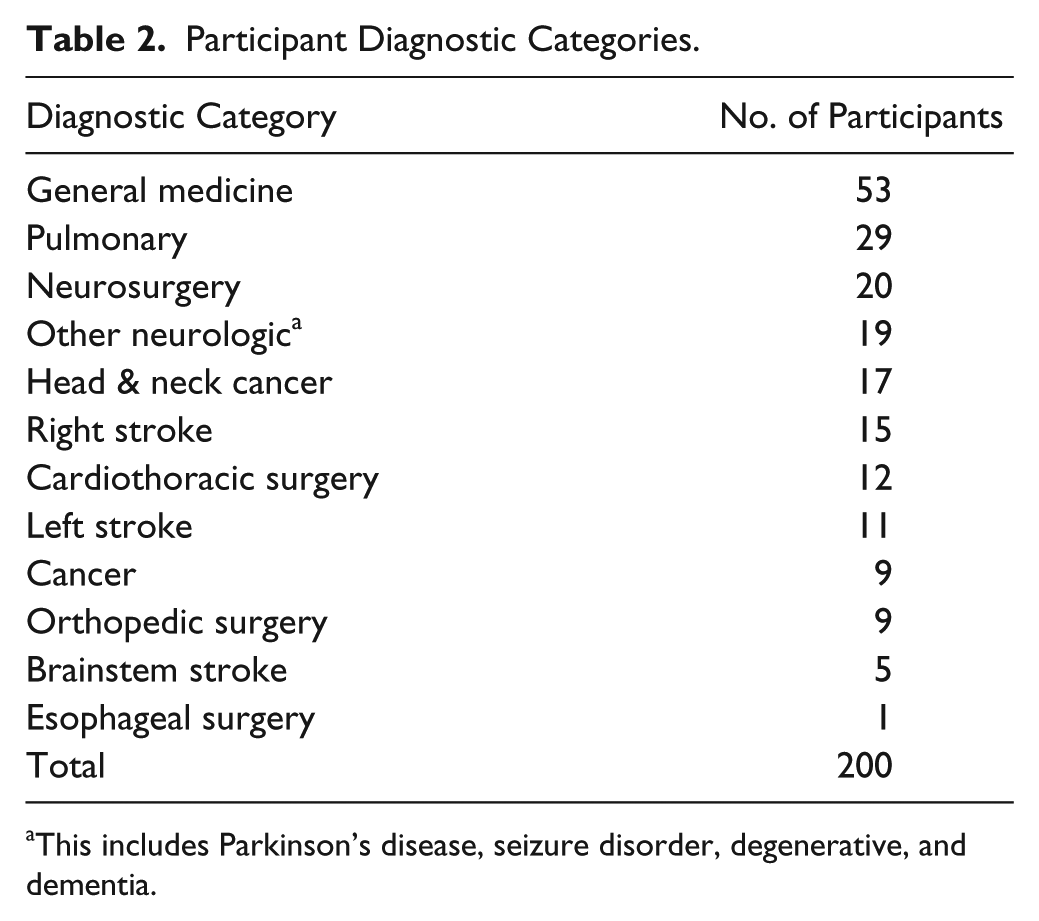
This includes Parkinson’s disease, seizure disorder, degenerative, and dementia.
Table 3 shows results of oral intake data as entered by nursing into the electronic medical record. Neither the speech-language pathology nor nursing services identified any patient as exhibiting overt signs of aspiration risk at meal times. All patients who passed the protocol and maintained a stable medical and neurological status while hospitalized drank and ate successfully without overt signs of aspiration risk up to and including post-testing day 5. Mean (SD) volume of liquid ingested per day for the entire sample was 474.2 (435.5) cc. The recommended diets spanned thin liquids with puree, soft solid, or regular solid consistency foods dependent upon cognition and dentition status.
Volume of Liquid Ingested Per Day After Passing the Yale Swallow Protocol.
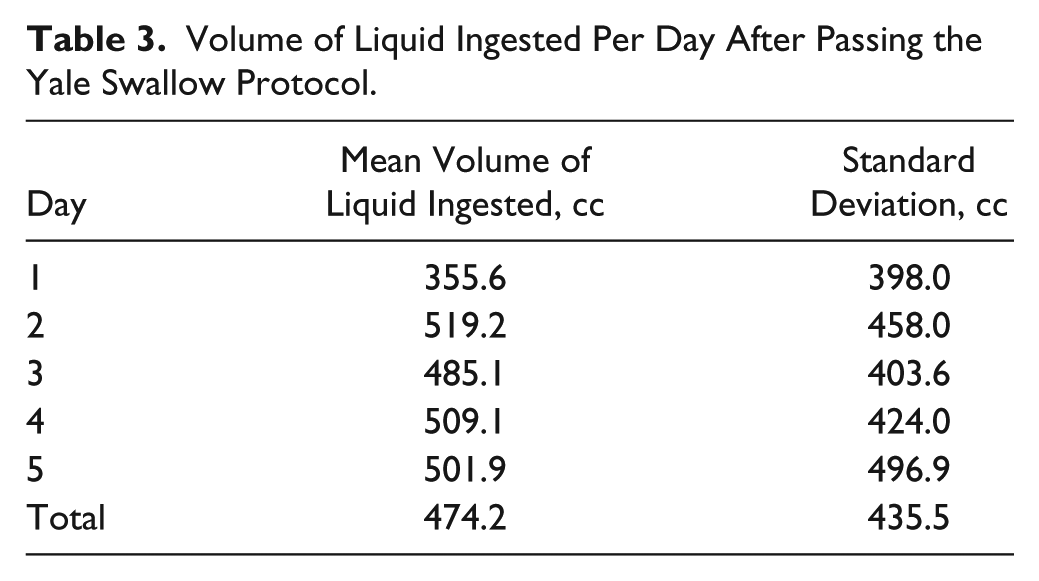
Table 4 shows nutrition and hydration delivery routes. A total of 181 (90.5%) patients had an appropriate nil per os order and were receiving enteral or parenteral nutrition concomitant with referral for a swallowing evaluation. Nineteen (9.5%) patients were ordered an oral diet in addition to being referred for a swallow evaluation.
Nutrition and Hydration Delivery Routes.
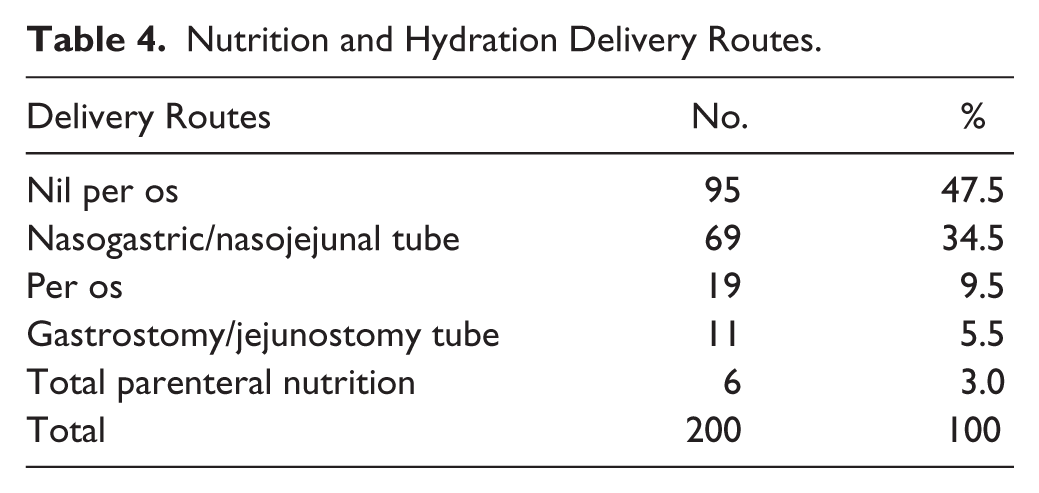
Figure 1 shows that patient retention decreased steadily from day of testing (n = 200; 100%) through post-testing day 5 (n = 95; 48%). The majority of patients (n = 60) were discharged on post-testing days 3 (n = 29) and 4 (n = 31). Sixteen (8%) patients were discharged from the hospital either on day of testing or post-testing day 1. Eight (4%) patients were made nil per os due to inability to maintain inclusion criteria, such as worsening medical or neurological conditions. Four (2%) patients did not eat anything and took only sips of liquid despite passing the protocol, during the 5-day follow-up period, but rather relied totally on a nasogastric or nasojejunal (n = 3) or gastrostomy (n = 1) feeding tube for delivery of nutrition and hydration.
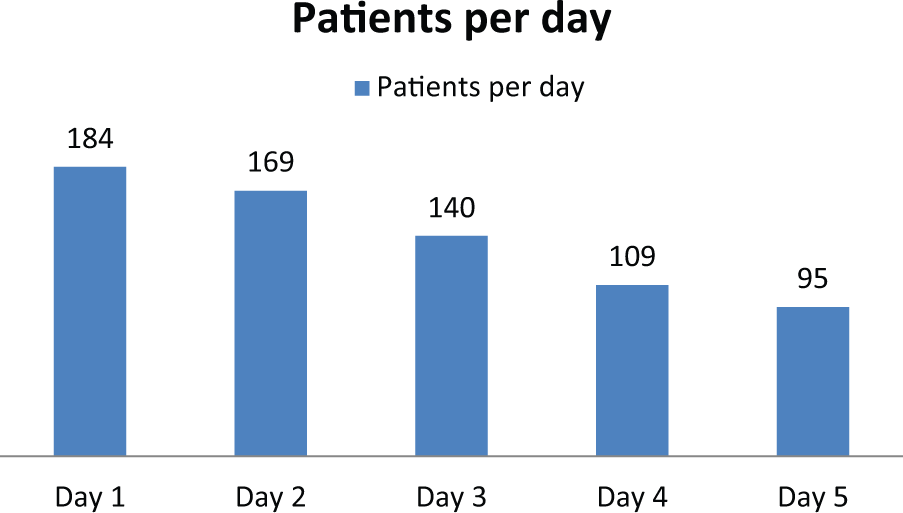
Patient retention rate per day of hospitalization.
Discussion
For the first time, long-term success of oral alimentation after swallowing testing has been documented. Passing the Yale Swallow Protocol 2 allowed for initial determination of aspiration risk followed by up to 5 days of successful oral alimentation in hospitalized patients.
These long-term results corroborated short-term (< 24 hour) eating and drinking success with intensive care unit, 3 stroke, 4 and general hospital 5 patients. The Yale Swallow Protocol meets all criteria necessary for a successful screening tool, that is, simple and inexpensive to administer 12 ; quick to perform and interpret 13 ; reliable, accurate, and timely 14 ; validated for use with other health care professionals, for example, registered nurses 15 ; applicable to virtually all patients regardless of diagnosis 8 ; and spanning the age spectrum from pediatric 16 to geriatric. 17
The protocol is strengthened by its key operating criteria and a unique factor not found in any other instrument. The key criteria include determination of aspiration risk with a high sensitivity of 96.5% and a high negative predictive value of 97.9% 8 and, since silent aspiration is volume dependent, a low false negative rate < 2.0%. 18 The unique factor is a priori knowledge of successful swallowing with thin liquid, puree, and solid food consistencies because the 3-ounce challenge 8 was performed in conjunction with and corroborated by double-blinded testing with both FEES7,10 and VFSS. 11 This allows for specific diet recommendations to be made safely, confidently, and in a timely fashion without the need for objective (instrumental) dysphagia diagnostic testing 8 in virtually all hospitalized patients who are deemed potential candidates for oral alimentation.3-5,8
The findings of the present study are corroborated by previous research. Specifically, the mean amount of liquid ingested orally per day during this study (474.2 cc) was in agreement with short-term (< 24 hours) amount of liquid ingested by studies which focused on intensive care unit (360 cc), 3 stroke (385 cc), 4 and general hospital (340 cc) 5 patients. The approximate 120-cc increase can be attributed to the benefits afforded by longer term follow-up, which allowed for health improvement leading to enhanced oral alimentation. It is important that the present study’s population sample (Tables 1 and 2) with respect to age ranges, sex differences of more males than females, and admitting diagnostic categories was consistent with a much larger (n = 4038) epidemiologic study on aging and dysphagia in the acute care hospitalized population, 17 thereby increasing reliability and generalizability of results.
A total of 69 (34.5%) patients successfully supplemented oral nutrition and hydration with enteral alimentation via nasogastric or nasojejunal tubes (Table 4). Previous research demonstrated that the presence of a nasal feeding tube, regardless of age, diagnostic category, or tube diameter, did not increase incidence of aspiration for either liquid or puree food consistencies.19,20 Therefore, a swallowing evaluation can be performed with a nasal feeding tube in place and there is no contraindication, as the present study has demonstrated, to continuing supplemental enteral nasal tube feeding until prandial nutrition and hydration are adequate.
Despite passing the Yale Swallow Protocol, a total of 4 (2%) patients relied on enteral tube feedings, thereby choosing not to eat and taking only sips of liquid. This is not unexpected in the acute care setting. It is important to note that passing the protocol permits safe oral alimentation but cannot mandate compliance. A lack of appetite and subsequent desire to eat per os occurs due to feeling unwell or satiety from tube feedings. These patients should be referred to a registered dietitian in order to adjust tube feedings, for example, reducing flow rate or cycling to night, with the goal of maintaining adequate nutrition and hydration concomitant with increasing oral alimentation.
Although the present study documented success of long-term oral alimentation, it must be emphasized that swallowing assessment provides only a snapshot-in-time of a patient’s swallowing abilities and neither subjective nor objective testing can guarantee continued successful swallowing behavior. The clinician must be aware that a negative test allows for safe eating and drinking only as long as the patient remains stable. Therefore, caregivers must remain vigilant to signs of aspiration risk, for example, coughing at meal times, altered mental status, or symptoms of upper respiratory infection, and recommend timely re-evaluation.
Strengths, Limitations, and Future Research
Strengths of this study were prospective and consecutive participant accrual, reliability and generalizability of results due to use of a representative population sample of acute care hospitalized patients with respect to age, sex, and admitting diagnostic categories, and blinded data entry by nursing. A limitation was a 5-day follow-up period, which, although longer than any other study in the literature to date, remains a relatively short time frame. However, an even longer follow-up period than 5 days in the acute care setting appears to be unrealistic in the present health care environment. Future research replicating this study’s methodology in the rehabilitation setting with > 5 days’ follow-up would be beneficial.
Conclusion
All patients who maintained the inclusion criteria were successfully drinking thin liquids and eating 1 to 5 days after passing the Yale Swallow Protocol. 2 Mean (SD) volume of liquid ingested per day for the entire sample was 474.2 (435.5) cc. Patient retention decreased steadily from day of testing (n = 200) through post-testing day 5 (n = 95). This was expected due to increasingly rapid transit through the acute care setting, which often renders longer follow-up problematic. For the first time, longer term success of oral alimentation after swallowing testing has been documented. Passing the Yale Swallow Protocol 2 allowed for initial determination of aspiration risk followed by longer term success of oral alimentation in acute care hospitalized patients and without the need for instrumental dysphagia testing.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.