
Abstract
Objectives:
The objective was to identify whether the experience of the operating surgeon was relevant to the frequency of the laryngeal mask airway (LMA) airway obstruction or change to an endotracheal tube during ear, nose, and throat surgery.
Methods:
Data were prospectively collected for 186 patients undergoing a procedure with the use of a Boyle–Davis gag and LMA over 12 months in a district-general hospital in the United Kingdom. patient demographics (age, mallampati grade), grade of surgeon, grade of anesthetist, LMA size inserted, and any intraoperative adjustments needed were recorded.
Results:
There was an overall intraoperative airway intervention rate of 21%. The experience of the surgeon affected the rate of intraoperative airway interventions encountered, reflected by the significantly lower rate of airway complications (ie, 10%) seen when associate specialists perform these types of procedures compared to other grades of surgeon (Fisher’s exact test 2-tailed P value = .04). A significant complication rate of 50% was seen with core surgical trainees compared to other grades of surgeon (Fisher’s exact test 2-tailed P value = .002).
Conclusions:
The results of this study suggest there may be a learning curve for otolaryngology trainees when using a LMA. However, larger studies and further subanalyses are essential before further conclusions can be made.
A reinforced laryngeal mask airway (LMA) has been presented as an efficient alternative to endotracheal tube (ET tube) insertion during ENT surgery. However, upon opening of the Boyle–Davis gag (B-D gag), obstruction of the tube and leakage from the airway circuit have been acknowledged as problems. 1 Rates of intraoperative airway complications of the LMA vary between studies (18.2% 1 to 25% 2 ), and the changeover rate to an ET tube during the procedure can range from 1% 3 to 11.4%. 4
There is little published evidence stating whether the experience of the operating surgeon controlling the mouth-gag opening and/or the grade of anesthetist inserting the LMA had any impact on subsequent airway obstruction or circuit leakage and the eventual necessity to adjust the LMA or intubate. Our study was designed to identify if such a learning curve existed, and which factors significantly influenced the intraoperative airway intervention rate when using a B-D gag with a LMA.
Methods
Data were prospectively collected for all patients undergoing an ENT surgical procedure with the use of a B-D gag under a general anesthetic. All work was performed with local research and ethics committee approval. This study was undertaken from June 2011 until June 2012 (12 months). Patients were excluded from the study if they had any previous craniofacial or syndromic abnormalities, if they were younger than 18 months old, or if they had undergone previous surgery to the upper aerodigestive tract. The number of procedures identified was 233.
In 45 patients it was deemed necessary to replace the LMA with an ET tube prior to the surgeon commencing operating. 2 further patients were excluded due to lack of identifiable data. These procedures were therefore excluded from the overall analysis, which left 186 patients (N = 186) who started an ENT procedure with a B-D gag and an airway secured via a LMA. Of these 186 procedures, 33 were adenoidectomies, 117 were tonsillectomies, 29 were adenotonsillectomies, and 7 were other “miscellaneous” procedures (see Table 1).
Breakdown of the 186 ENT Operations Identified Using an LMA and a B-D Gag Over the 12-month Period.
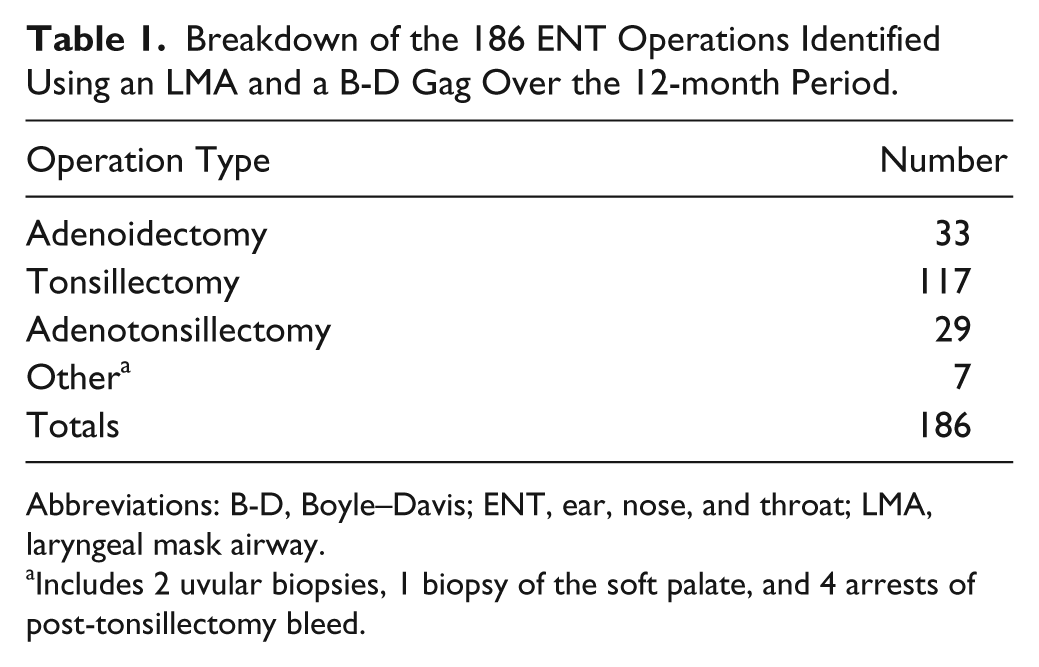
Abbreviations: B-D, Boyle–Davis; ENT, ear, nose, and throat; LMA, laryngeal mask airway.
Includes 2 uvular biopsies, 1 biopsy of the soft palate, and 4 arrests of post-tonsillectomy bleed.
Information was gathered by the authors (the operating surgeons with assistance from operating-department assistants) regarding patients’ demographics (age, Mallampati grade), grade of surgeon, grade of anesthetist securing the airway, LMA size inserted, and any adjustments to the airway needed during the operation.
The criteria for “obstructive” events were designated by the authors as follows: inability to ventilate, decreased tidal volumes, increased airway pressures, or any concerns from the anesthetist. A “circuit leak” was any scenario in which anesthetic gases or oxygen may have escaped the closed anesthetic circuit, which may have resulted in patient hypoxia or patient awareness.
This information was successfully prospectively gathered in 92% of cases, and for the remaining 8%, a retrospective case note review was undertaken to determine whether any further airway interventions had been documented. Operator experience was implied by recording the total number of operations involving B-D gag use performed by that particular surgeon over the previous 12 months (see Table 2).
Grade of Surgeon Against Number of Procedures Involving a B-D Gag and an LMA Over the 12 Months Studied. a
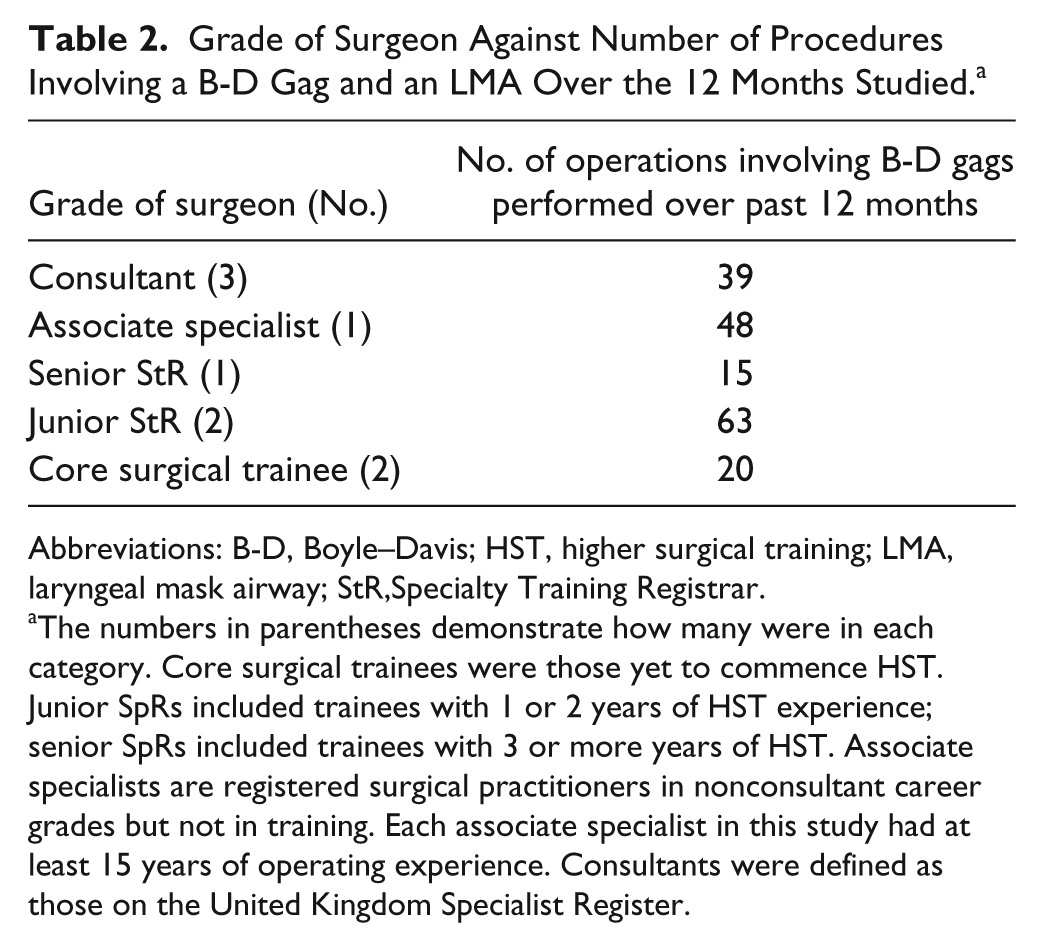
Abbreviations: B-D, Boyle–Davis; HST, higher surgical training; LMA, laryngeal mask airway; StR,Specialty Training Registrar.
The numbers in parentheses demonstrate how many were in each category. Core surgical trainees were those yet to commence HST. Junior SpRs included trainees with 1 or 2 years of HST experience; senior SpRs included trainees with 3 or more years of HST. Associate specialists are registered surgical practitioners in nonconsultant career grades but not in training. Each associate specialist in this study had at least 15 years of operating experience. Consultants were defined as those on the United Kingdom Specialist Register.
The parametric patient demographic data were analyzed using paired t tests. The nonparametric demographic data were analyzed using Mann–Whitney U tests. The intraoperative airway intervention rates were analyzed using Fisher’s exact test (2-tailed test), and a significant P value was deemed to be < .05. These analyses were carried out using SPSS statistical software.
Results
In all, 186 ENT operations were recorded involving the use of a LMA with a B-D gag. Table 1 shows the breakdown of these operations. Out of the 186 procedures, 39 resulted in airway obstruction or leak and warranted further management by way of adjustment of the B-D gag, adjustment or replacement of the LMA, or ET tube insertion. This gave an intraoperative airway intervention rate of 21% overall.
The patient demographic data can be seen in Table 3. The patient demographics (age, American Society of Anesthesiologists [ASA] Classification, and Mallampati scores), made no significant difference to the intraoperative airway intervention rates (P values of .95, .78, and .18, respectively, paired t test and Mann–Whitney U tests). The size of LMA inserted also proved not to be a significant factor between the group of patients requiring intraoperative interventions to their airway and those that did not (P = .96, Mann–Whitney U test).
Patient Demographic Data.
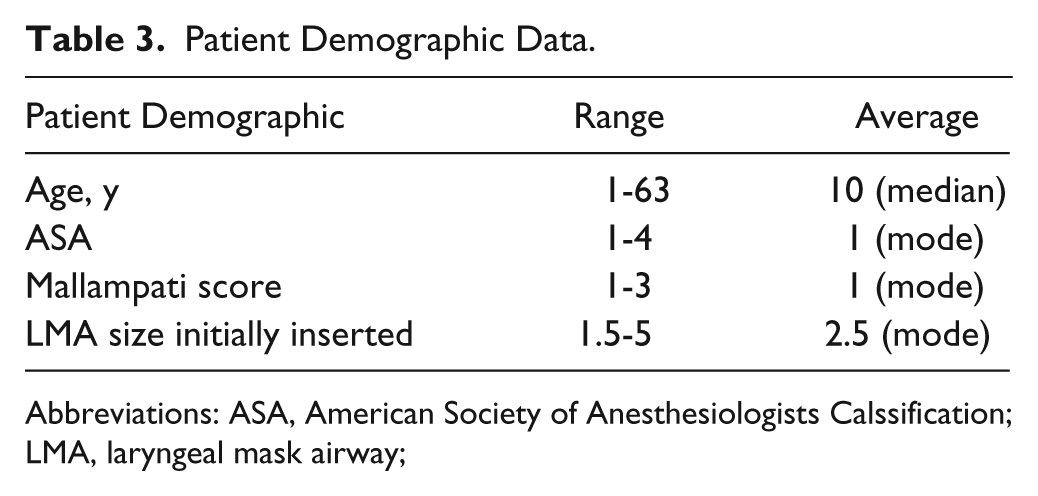
Abbreviations: ASA, American Society of Anesthesiologists Calssification; LMA, laryngeal mask airway;
Table 4 demonstrates the breakdown of surgical grade performing the operations and shows the rates of further airway intervention encountered with each surgical grade. The most junior of trainees (core surgical trainees) recorded significantly higher intraoperative intervention rates than did other surgical grades. The associate specialist recorded significantly lower intraoperative intervention rates than did other surgical grades.
The Grade of Surgeon and the Rates of Further Airway Intervention Encountered. a

Abbreviation: StR, Specialty Training Registrar.
The numbers in parentheses demonstrate how many surgeons were in each category.
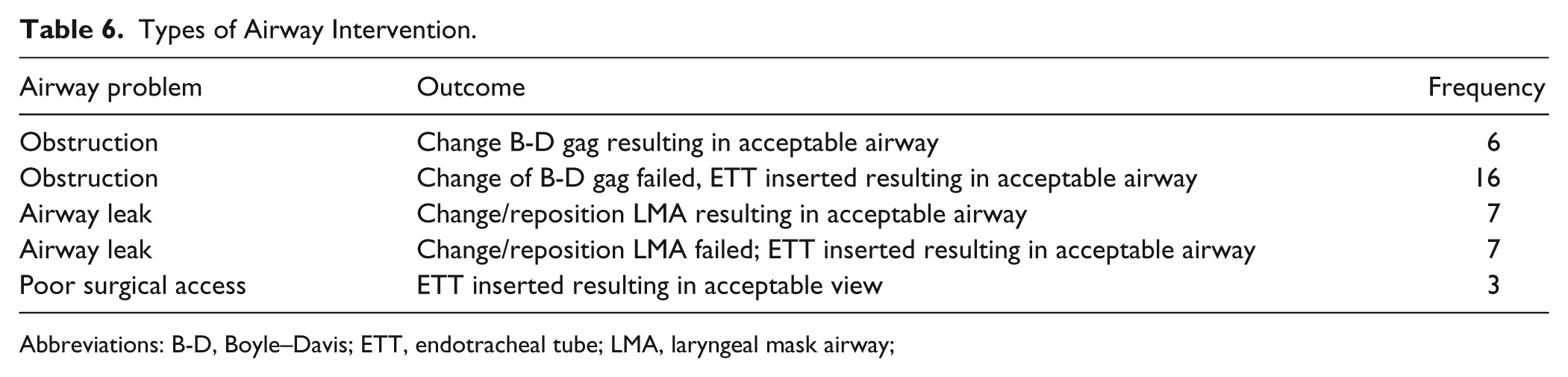
Table 5 demonstrates the breakdown of anesthetic grade performing the LMA insertions and the rates of further airway intervention encountered with each anesthetic grade. The grade of anesthetist did not make a significant difference to the rate of intraoperative airway interventions encountered. The 39 airway interventions gave an overall intraoperative intervention rate of 21%. The rate of change from an LMA to an ET tube overall was 14%. These interventions are summarized in Table 6.
The Anesthetic Grade Performing the LMA Insertions and the Rates of Further Airway Intervention Encountered With Each. a
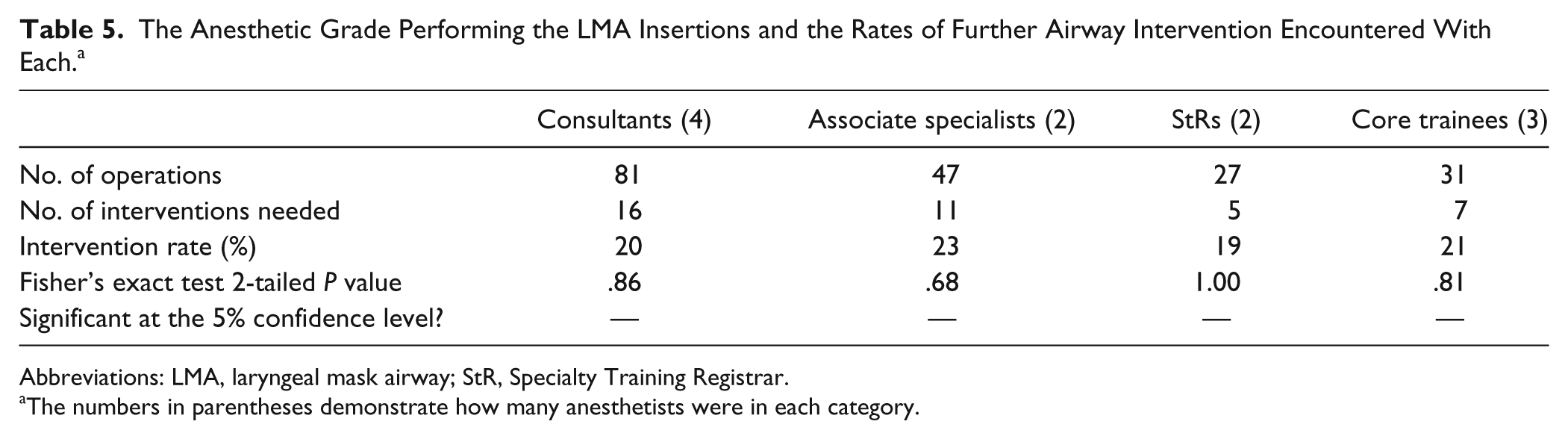
Abbreviations: LMA, laryngeal mask airway; StR, Specialty Training Registrar.
The numbers in parentheses demonstrate how many anesthetists were in each category.
Types of Airway Intervention.
Abbreviations: B-D, Boyle–Davis; ETT, endotracheal tube; LMA, laryngeal mask airway;
Discussion
The concept of a “shared airway” in ENT surgery is not new to otolaryngologists and their anesthetic colleagues. The impact of airway management on the surgical field and perioperative conditions requires the surgeon to be aware of contemporary tools and techniques available. A reinforced LMA has been presented as an efficient alternative to ET tube insertion during ENT surgery. The literature suggests various advantages of LMA use: ease of insertion, lower frequencies of postoperative airway irritation; that is, cough, 5 stridor, 6 and laryngospasm 2 ; significantly shorter time to extubation, 2 fewer hemodynamic changes, 6 less time in the operating room after surgery, 7 and less blood in and around the larynx. 1 No significant differences in postoperative pain, nausea or vomiting have been reported when compared to ET tubes. 7 LMAs have even been used to secure the airway for hemostasis for post-tonsillectomy hemorrhage when intubation was not possible. 8
However, upon opening of the B-D gag, kinking of the tube causing airway obstruction or circuit leakage has been acknowledged as a problem. 1 Rates of airway obstruction of the LMA vary between studies (18.2% 1 to 25% 2 ) and the changeover to an ET tube during the procedure can range from 1% 3 to 11.4%. 4
In our study, the rate of airway problems encountered intraoperatively was 21% which is comparable to the literature, although we have included circuit leakage rates as well as airway obstruction, unlike most studies which only measure the latter. The “circuit leakage” events were included in the overall analysis of the intraoperative airway complication rates (see Table 6), as the authors felt that upon insertion and opening of the B-D gag, the LMA can advance and become twisted or “kinked.” This can reduce the effective seal around the supraglottis, causing a leak, but is usually avoidable if the operating surgeon is careful. On occasion, however, no matter how cautious the surgeon attempts to be, a leak may occur as a function of the LMA, and the authors acknowledge an element of error may be introduced into the analysis.
The rate of changeover to an ET tube in our study was around 14%, which was slightly higher than of other literature estimates. One might infer, from the intraoperative airway complication rate of around 1 in 5, that there may be an argument to intubate all patients undergoing surgery with a B-D gag for patient safety reasons. Despite this, the advantages of LMAs (as previously listed) to secure the airway during certain ENT operations make them the technique of choice in the authors’ institution, unless specified otherwise, preoperatively.
Surgical access and adequate visualization is controversial with some studies indicating little difference between LMA and ET tube use,1,6 and others suggesting inferior surgical access and even stating the weight of tonsillar tissue excised is less when using an LMA. 4 The B-D gag was originally designed for use with ET tubes which have a smaller diameter external tube. The LMA tubes are of a larger caliber, which may be an explanation for the decreased exposure of the oropharynx. If the B-D gags were suitably modified to accommodate the LMA, then the airway complication rate may be reduced further. There were no recorded cases in which the LMA was dislodged with removal of the B-D gag in our study, but the authors acknowledge that this can be a problem which could potentially further increase intraoperative airway complication rates.
Little analysis has been done regarding the experience of the operating surgeon to see whether this factor had any impact on subsequent airway obstruction or circuit leakage, and the eventual necessity to adjust the LMA or intubate. Our investigation was designed to identify whether the grade and experience of the operating surgeon was relevant to the rate of airway interventions required intraoperatively, and thus investigate the existence of a learning curve when undertaking this type of surgical procedure.
Core surgical trainees were involved in around 10% of the operations. According to our analysis, the most junior trainees experienced higher rates of intraoperative problems with LMAs. A significant complication rate of 50% was seen with core surgical trainees compared to other grades of surgeon (Fisher’s exact test 2-tailed P value = .002).
Although the juniors were always supervised by a senior trainee or consultant, the skill of selecting the correct sized gag and tongue-blade for the B-D gag, subsequent placement of the gag and its opening without causing obstruction is something that may be perfected with experience. 9 This experience may be reflected by the statistically, significantly lower rate of intraoperative airway complications (ie, 10%) seen when associate specialists perform these types of procedures compared to other grades of surgeon (Fisher’s exact test 2-tailed P value = .04). However, the more complicated cases with an anticipated higher risk of intraoperative airway complications will have been placed on consultant-led lists. This may, in part, be responsible for the higher rates of airway interventions experienced during consultant and specialty registrar operations (who mostly operated under consultant supervision), compared to the routine cases listed for the associate specialists.
The experience of the user should not affect the ability of the supervisors’ ability to modify the position of the gag. However, anecdotal experience may tell us that clear communication with the anesthetist at the time of B-D gag opening and the use of a longer blade are associated with improved surgical access and decreased rates of obstruction. These are skills that may be improved by experience and regular practice of a certain procedure. Interestingly, the rate of intraoperative airway complications encountered in this study seems to reflect the experience in these types of operations, rather than the grade of the surgeon alone.
The size of the LMA tube chosen by the anesthetist is likely to have an effect on airway obstruction rates, 10 although little variation in complication rates were noted in our study between the grades of anesthetists inserting the LMA (see Table 5). Once an airway complication had been encountered intraoperatively, one-third of problematic airways were solved with adjustment of the B-D gag or the LMA (see Table 6), and therefore these are appropriate to trial as a first-line method of airway control. However, in two-thirds of cases, conservative efforts by the surgeon or anesthetist failed to improve ventilation of the patient and therefore the prompt assessment and decision to provide a definitive airway via an ET tube was essential. In these cases it is not clear why adjustment of the LMA or B-D gag failed to resolve the problem in this subset of patients that required eventual intubation. Further analysis of the cofactors in greater numbers of patients may be required before useful conclusions can be drawn regarding this subset.
Our analysis did not reveal that patient factors were influential in determining the intraoperative airway intervention rate. However, with a P value of .18, one could argue that the Mallampati scores were closer to being significant between the 2 cohorts than the other patient factors. Type 2 error may be responsible for the lack of significance in this analysis, and could be an interesting focus for further large scale studies. Anecdotally, there is little doubt that an experienced anesthetic assessment of the airway to select potential patients that are not suitable for a LMA (and thus require intubation prior to surgery) reduces the need for intraoperative airway interventions. The analysis also did not reveal a relationship between type of procedure being performed and the airway intervention rate, but again the numbers were small and therefore prone to type 2 error.
Caution should be exercised before drawing any firm conclusions from this study. This study did not identify the reasons why a cohort of patients started their operation with an ET tube rather than a LMA. The experience in prior airway assessment or surgical preference may have had an effect on masking the true intraoperative intervention rate or conceal the effect that patient factors such as Mallampati scores had. Indeed, this may be reflected in a separate analysis of the 45 excluded patients intubated prior to the start of any operation with a B-D gag, as 70% of these patients had an anesthetic consultant, or ENT consultant, or both, involved in the decision to intubate preoperatively.
The pairings between surgeons and anesthetists were not analyzed in this study and this could be a major source of bias. It is not uncommon for a regular anesthetist to work with a surgeon, particularly in the case of associate specialists or consultants. A familiar team is less likely to run into airway trouble and this may be the more powerful factor when trying to determine the cause for a difference in complication rates. Also, a familiar team might employ effective communicative strategies to improve perioperative conditions and display a higher threshold prior to the request to replace the LMA.
This study was carried out in a typical district-general hospital in the United Kingdom, and these figures may not necessarily be transferable to larger tertiary centers that have a different case mix or carry out similar otolaryngology procedures, but on patients with more complex airway abnormalities.
Conclusions
The results of this study suggest there may be a learning curve for otolaryngology trainees when opening the B-D gag in a patient with an airway secured with an LMA. The intraoperative airway intervention rate is not linearly related to grade of surgeon but appears more likely related to experience in this type of operation. However, further multicenter studies incorporating a larger sample of patients, analyses of the surgical-anesthetic perioperative relationship, and identification of those factors predictive of intraoperative complications are essential before further definitive conclusions can be made. The authors of this study recommend that targeted teaching and training in theater for junior surgical trainees incorporate not only the necessary techniques needed to perform the operation but also the perioperative skills needed to safely and successfully manage a “shared airway.”
Footnotes
Acknowledgements
The authors would like to thank the staff in the operating department at Milton Keynes General Hospital for their support during the duration of this study. This study was presented previously to the 14th British Academic Conference in Otolaryngology (BACO) in Glasgow, July 6, 2012.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.