
Abstract
Objective:
This study aimed to evaluate the relationship between nasopharyngeal pH and Eustachian tube dysfunction (ETD) in adults.
Study Design:
Unmatched case-control study.
Methods:
Forty-one subjects, 20 adults with a diagnosis of ETD and 21 healthy adults as controls, were enrolled from an outpatient clinic. All subjects had a Dx–pH probe placed near the torus tubarius in the posterior nasopharynx for 24 hours. The pH values were recorded every 0.5 second. Decreases in pH were considered as reflux events if the pH dropped below 5.5.
Results:
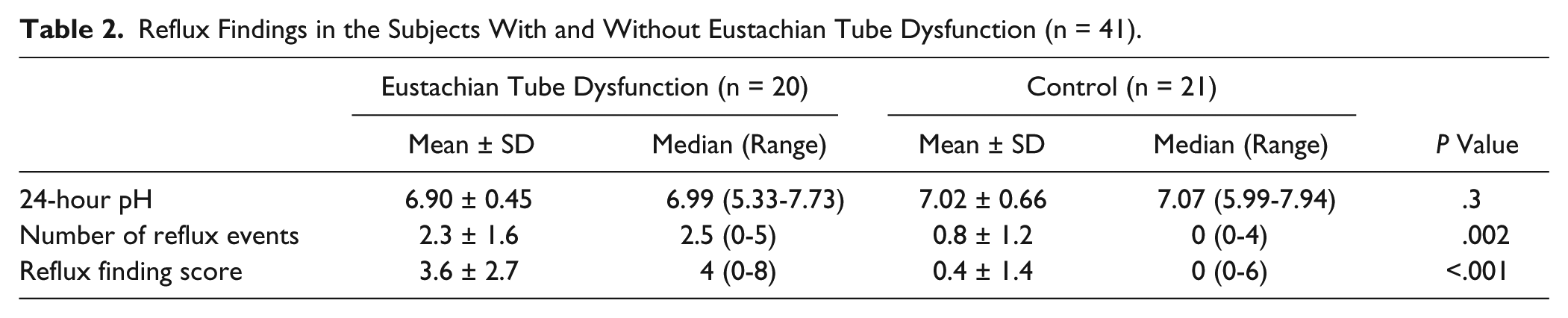
The average nasopharyngeal pH value was 6.90 (range, 5.33-7.73) in the subjects with ETD and 7.07 (range, 5.99-7.94) in the controls. The difference between the 2 groups was not statistically significant (P = .30). The ETD group, on average, had a higher number of nasopharyngeal reflux events (2.3 ± 1.6 vs 0.8 ± 1.2, respectively; P = .002) and higher reflux finding score (3.6 ± 2.7 vs 0.4 ± 1.4, respectively; P < .001) than the control group.
Conclusion:
By using a novel pH probe that allows detection of acidity in a nonliquid environment, a comparison of nasopharyngeal pH between control patients and those with ETD was performed. Eustachian tube dysfunction was more likely to be associated with a higher number of nasopharyngeal reflux events and higher reflux finding score. Nasopharyngeal reflux may have a role in the pathogenesis of ETD.
Introduction
Reflux of gastric contents into the larynx, pharynx, and upper aerodigestive tract is known to cause a multitude of otolaryngologic manifestations. 1 Despite the relationship between laryngopharyngeal reflux and laryngeal diseases demonstrated by many studies,2-4 the relationship between nasopharyngeal reflux and middle ear abnormalities is not clear.
It remains controversial whether nasopharyngeal reflux can lead to an increased risk of Eustachian tube dysfunction (ETD) in adults. Previous studies in children have shown that reflux affects the Eustachian tubes and can lead to an increased risk of otitis media.5-8 Bench research has found histological differences in the mucosa of animal Eustachian tubes after contact with gastric acids.9-11 Antireflux therapy has also been found to relieve the chronic refractory feeling of pressure in the ears. 12 No study, however, has directly investigated the relation between nasopharyngeal reflux and ETD.
The study of nasopharyngeal reflux in the past has been limited due to the pH probe technology. Earlier pH probes were designed for testing in the esophagus and were capable of measuring pH only in moist environments. The placement of conventional pH probes above the larynx would have led to errors due to the dry environment. 13 Recent advances in pH probe technology have allowed for pH monitoring in nonliquid environments. This development enables researchers and clinicians to determine whether gastric acid has reached nonmoist environments such as the nasopharynx. 14 In the current study, we used 1 of the new pH probe systems to investigate the relationship between ETD and nasopharyngeal reflux. The aims of this study were (1) to determine the average pH values and number of reflux events near the Eustachian tube orifice of adult patients who suffer from Eustachian tube dysfunction and (2) to compare the results with those of control subjects without ETD. To achieve these goals, a pH probe designed for a moist but nonliquid environment was placed at the Eustachian tube orifice of adults with ETD as well as other healthy controls.
Methods
Institutional Review Board approval was obtained from the office of research administration at our institution. Twenty adult patients who were diagnosed with ETD were enrolled in the study through the otolaryngology clinic of our tertiary care medical center between December 2009 and March 2011. Eustachian tube dysfunction was defined to be present when both of the following conditions were met: (a) subjective report of difficulty with equalizing middle ear pressure, and (b) retraction of tympanic membrane under microscope, or tympanogram peak at less than −100 dPa. Subjects were excluded if any of the following was present: symptoms of allergic or nonallergic rhinitis, history of previous head and neck surgery or radiation, history of ear disease, history of smoking tobacco, or the usage of over-the-counter sinus relief medications (eg, intranasal steroids, decongestants, or antihistamines) due to their potential alterations in the physiology of the nasopharynx and probe readings.
We previously studied the nasopharyngeal pH of a group of 20 healthy subjects who did not suffer from ETD. 14 The subjects in the previous study were recruited from the adults who visited the same clinic and, in addition to 1 new healthy subject, served as the control group for the current study. The control group had the same exclusion criteria as the ETD group. If the study subjects had a history of acid reflux, they were asked to stop their medications 2 weeks prior to the study.
After obtaining written informed consent, a small questionnaire was completed that included questions on age, sex, duration of ETD, and history and frequency of “heartburn.” All subjects had a Dx–pH Measurement System Probe (Restech Corporation, San Diego, California, USA) placed at the torus tubarius in the posterior nasopharynx, and then it was secured to the subjects’ face (Figure 1). Proper placement of the probe was confirmed in all subjects using fiberoptic nasopharyngoscopy. Each subject’s reflux finding score was determined by the senior author and confirmed by another author according to the method described by Belafsky et al. 15 Once in place, the single-channel Dx–pH probe performed a pH reading every 0.5 second and sent the data wirelessly from the attached Dx–Transmitter to the Dx–Recorder. The Dx–Recorder was worn around the neck or on the belt for 24 hours. During the 24-hour period, subjects were instructed to eat and perform their daily activities as usual and to record relevant information such as meals, sleeping, and reflux symptoms (heartburn) with the push of a button as well as manually into a written diary. Any reading during the ingestion period was disregarded. Upon completion of the study, the pH data and patient information were downloaded from a memory card into Dx–pH DataView software to be assessed, graphed, and analyzed. Decreases in pH were considered as reflux events if the pH dropped below 5.5. This threshold was provided by the manufacturer’s guideline for pharyngeal reflux and adapted from the study by Ayazi et al.14,16

Dx–pH Measurement System Probe was secured to face using an adhesive tape. This was done once the placement of the probe tip near the torus tubarius was confirmed using flexible fiberoptic laryngoscopy.
The mean (standard deviation), median, and range of values were reported wherever appropriate. Nonparametric tests were used to evaluate the difference in average pH, number of reflux events, and average reflux score between subjects with and without ETD. Chi-square was used to compare the presence of at least 1 reflux event between the 2 groups. A P value of less than .05 was considered as statistically significant. All statistical tests were performed using PASW 18.0 (SPSS Inc, Chicago, Illinois, USA).
Results
All subjects were able to complete the single-channel pH probe study. The male/female ratio was 10/10 in the ETD group and 12/9 in the control group (P = .70). The age of participants ranged from 19 to 77 years. The mean (SD) age was 51.1 (17.6) years in the ETD group and 35.3 (17.0) years in the control group (P = .01). Table 1 presents the demographics and characteristics of the ETD group. Among the subjects with ETD, 1 was recently diagnosed, 6 had ETD for 1 to 6 months, and 13 had ETD for more than 6 months. Of the subjects with ETD, 9 out of 20 (45%) had a history of at least 1 symptomatic episode of heartburn per week (4 had “once a week” and 5 had “2 to 4 episodes a week”).
Demographics and Characteristics of the Subjects With Eustachian Tube Dysfunction.
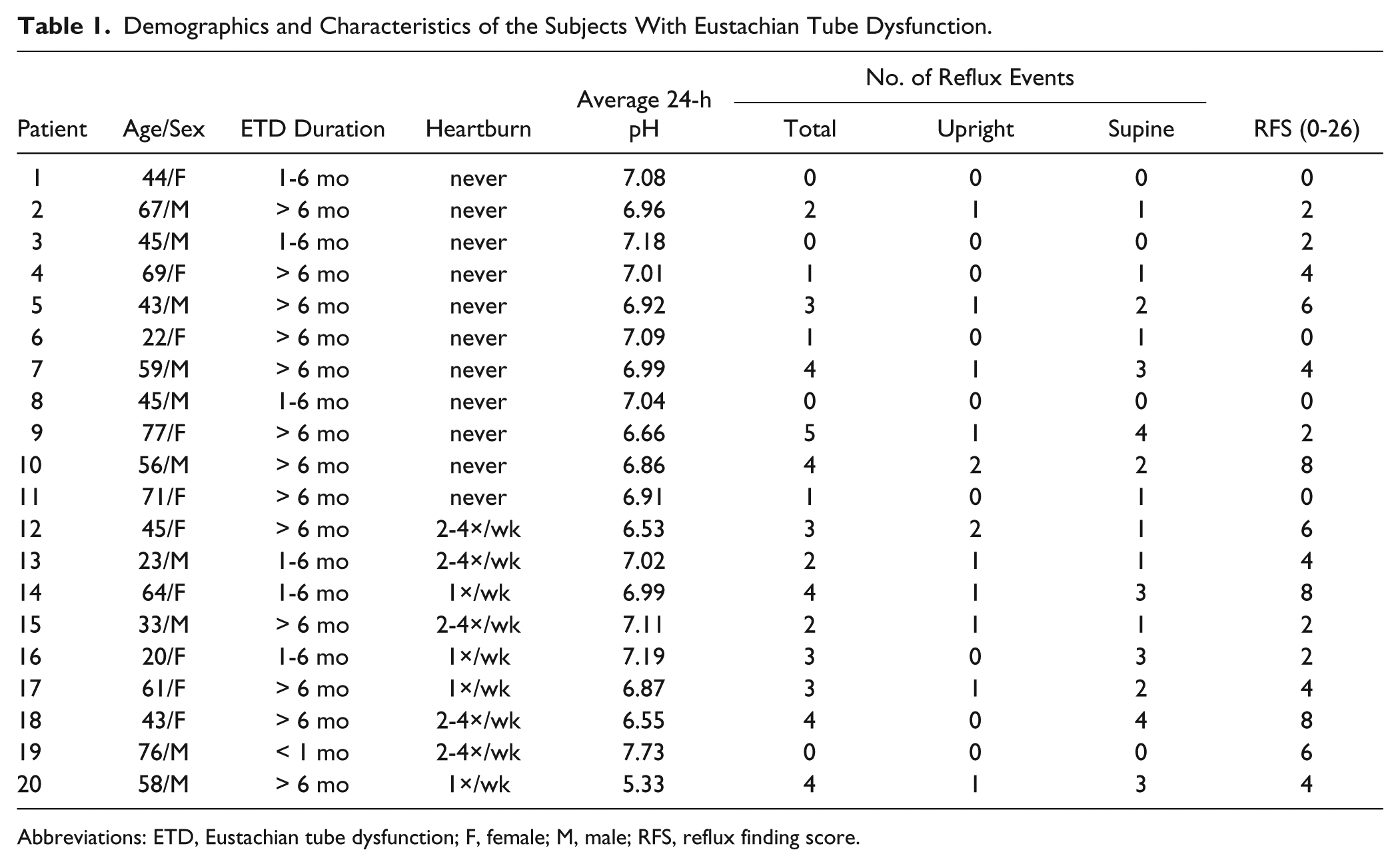
Abbreviations: ETD, Eustachian tube dysfunction; F, female; M, male; RFS, reflux finding score.
Table 2 summarizes the findings of the 24-hour pH recording in the ETD and control groups. Although the mean nasopharyngeal pH was lower in the ETD group, the difference between the 2 groups was not statistically significant. Sixteen subjects in the ETD group (80%) and 8 subjects in the control group (38%) were found to have at least 1 reflux event during the 24-hour pH recording (P = .01). The average number of reflux events and the average reflux finding score were both greater in subjects with ETD. Both differences were statistically significant (Table 2).
Reflux Findings in the Subjects With and Without Eustachian Tube Dysfunction (n = 41).
Discussion
In this study, we found that participants with ETD were more likely to have at least 1 nasopharyngeal reflux event during the study period compared to subjects without ETD. In addition, the average number of reflux events and average reflux finding score were both found to be significantly greater in the ETD group. There was a trend showing lower average pH values in patients with ETD compared to the control subjects. However, the observed difference was not statistically significant.
Previous studies in adults have established the presence of laryngopharyngeal reflux disease (LPR) in ETD patients subjectively using questionnaires,17-19 and a potential mechanism has been proposed to explain this relationship. Edema of the mucosa in the area of the Eustachian tube as a direct effect of LPR might cause a difference in pressure between the middle-ear cavity and the nasopharynx. This pressure difference could result in the development of ETD symptoms. 20
There is a paucity of data on the role of LPR in ETD—whether treating ETD patients with antireflux medications could help mitigate their otologic symptoms.8,21 With the advent of novel pH probes that allow measuring acidity in a dry environment, it is feasible to determine the pH values found at the Eustachian tube orifice of patients and analyze the association between ETD and LPR. As demonstrated in the current study, it would be more accurate if the presence of LPR were verified by direct pH monitoring at the Eustachian tube orifice than by the use of subjective questionnaires. Nearly 45% of the patients with ETD in our study reported having heartburn and/or acid regurgitation compared to 20% to 40% of the general population, as found by Locke et al. 22
Eight out of the 21 control patients who denied symptoms of reflux or Eustachian tube dysfunction had significant reflux events (pH less than 5.5) during the 24-hour pH probe study. These “silent reflux” patients lowered the average pH of control subjects and contributed to the lack of statistical significance when comparing the average nasopharyngeal pH of patients with ETD to the control population. Further investigation of our data revealed that ETD was more likely to be associated with the presence of reflux events rather than having heartburn as a symptom of gastroesophageal reflux disease (GERD).
As any other study, ours was not without limitations. First, our method did not include proximal/distal esophageal probes to assess the role of GERD. Second, our data were collected during a 24-hour period on a relatively small sample of subjects due to the difficulty associated with having probes attached for a long period. The major limitation to previously available pH probes was the inability to properly calculate pH in nonliquid environments. The future application of measuring pH to detect nasopharyngeal reflux and its relevance to otologic and sinonasal disease processes has yet to be determined. With the introduction of the currently described pH probe, we were able to delineate a trend of increased reflux events in patients with Eustachian tube dysfunction. Although findings of the current study remain to be confirmed in future larger studies, an empirical treatment trial including a reflux diet may be beneficial for patients with symptoms of both GERD and ETD or those who do not respond to allergic rhinitis treatment. Anecdotally, we have seen significant improvement in the majority of our nonallergic ETD patients with antireflux treatment using H2 blockers. Further studies will need to concentrate on the response to treatment with antireflux medications and long-term follow-up of these patients.
Conclusion
Patients with ETD, on average, have a higher prevalence of nasopharyngeal reflux (detected by a pH probe), a greater number of reflux events, and a greater reflux finding score than those without ETD. Those who deny having reflux symptoms are found to have occasional reflux events into nasopharynx. Therefore, nasopharyngeal pH measured by a pH probe might be a better predictor of having ETD rather than having reflux symptoms. An empiric trial of antireflux medication may help in determining the underlying cause of ETD.
Footnotes
Authors’ Note
This study was preliminarily presented at the American Academy of Otolaryngology–Head and Neck Surgery meeting in San Francisco, California, USA, September 2011. At the principal investigator’s request, Restech Corporation provided the probes for the study but had no influence on the concept, design, analysis, or manuscript that resulted from the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.