
Abstract
Objectives:
The objectives were to determine the prevalence of laryngeal dysplasia and associated human papilloma virus (HPV) subtypes in adult patients, 18 years or older, suffering from laryngeal papillomatosis at a tertiary care institution.
Study Design:
Retrospective cohort study.
Methods:
Patients with biopsy proven laryngeal papillomatosis were identified via chart review. All available pathology specimens were reviewed by a dedicated head and neck pathologist to confirm/refute the diagnosis of laryngeal dysplasia, and grade the level of dysplasia. Interrater agreement was compared using cross-tabulation methods. Specimens identified to be positive for dysplasia underwent further testing via in situ hybridization for low-risk (6/11) or high-risk (16/18) HPV subtypes.
Results:
Of the 85 subjects identified to have laryngeal papillomatosis, 24(28%) demonstrated laryngeal dysplasia. There was good interrater agreement on the presence of dysplasia; however, there was only fair agreement on the grade of dysplasia. Of the pathology specimens tested for HPV subtype, the majority of patients (62%) were positive for HPV 6/11, including all high-grade dysplasia patients. Three (12%) dysplasia specimens were negative for both high- and low-risk HPV subtypes.
Conclusions:
We found a 28% prevalence of dysplasia in our patient population with the majority of patients positive for low-risk HPV subtypes indicating that high-risk HPV subtypes do not predispose laryngeal papilloma patients to dysplasia.
Keywords
Laryngeal papillomatosis is a relapsing remitting growth of the upper airway that impairs voice and risks airway obstruction in children and adults if left untreated. Laryngeal papillomatosis is a benign manifestation of the human papilloma virus (HPV), and is typically associated with HPV subtypes 6, 11, as well as HPV 16, 18, 31, 33, 51. 1 Laryngeal dysplasia is a potentially premalignant lesion of the larynx that carries up to a 14% chance of progression to malignancy in the absence of laryngeal papillomatosis. 2 Existing studies have failed to implicate HPV infection as a cause for laryngeal dysplasia in the absence of laryngeal papillomatosis3,4; however; recent studies have documented a particularly high prevalence (22-50%) of laryngeal dysplasia in association with laryngeal papillomatosis.5,6 It is therefore important to further establish the incidence of dysplasia in laryngeal papillomatosis to better educate papilloma patients on the natural history of the disease and the potential chance for malignant transformation.
The role of “high-risk” HPV subtypes (16 and 18) has become increasingly apparent in the development of oropharyngeal carcinoma; however, high-risk subtypes have yet to be proven to increase the risk of progression of laryngeal papillomatosis to malignancy. 6 The role of HPV subtypes and dysplasia in the laryngeal papillomatosis literature has yet to be fully explored. The purpose of this study is to determine the prevalence of laryngeal dysplasia and associated HPV subtypes in adult patients, 18 years or older, suffering from laryngeal papillomatosis at a tertiary care institution.
Materials and Methods
Following approval from Emory University Institutional Review Board, potential study subjects were identified using billing codes for “benign laryngeal disease” and “microlaryngoscopy.”
Chart Review
Retrospective chart review was performed on all patients over the age of 18, who had undergone at least 1 surgical procedure under anesthesia with pathologic confirmation of laryngeal papillomatosis over a 7-year period at the Emory Voice Center. Detailed chart review of otolaryngology clinic reports and existing pathology reports was performed to document age, sex, duration of disease, number of laryngeal papilloma related surgical procedures, presence of dysplasia, degree of dysplasia, HPV subtyping (if available), and history of dysplasia risk factors including smoking history (current or previous), gastroesophageal reflux (treated or untreated), head and neck irradiation, carcinogen exposure, and immunosuppression.
Pathology
All available pathology specimens for all subjects enrolled in the study were pulled from the files in the Department of Pathology and Laboratory Medicine, Emory University Hospital. All cases were reviewed by a single, dedicated, head and neck pathologist (S.M.) to confirm or, refute the diagnosis, and grade of dysplasia.
Dysplasia was defined by the WHO classification of tumors 7 as an absence of maturation above the basal cell layer. Mild dysplasia (Figure 1a) was defined as cells above the basal cell layer with a lack of nuclear polarization or mitoses and a high nuclear-cytoplasmic ratio. Laryngeal papillomatosis generally has minimal keratinization and can show mild dysplastic changes and some studies suggest this corresponds to positive HPV 6/11 (active clinical course). Moderate or high-grade dysplasia (Figures 1b, 1c) was defined by atypia involving greater than 50% of the epithelium.
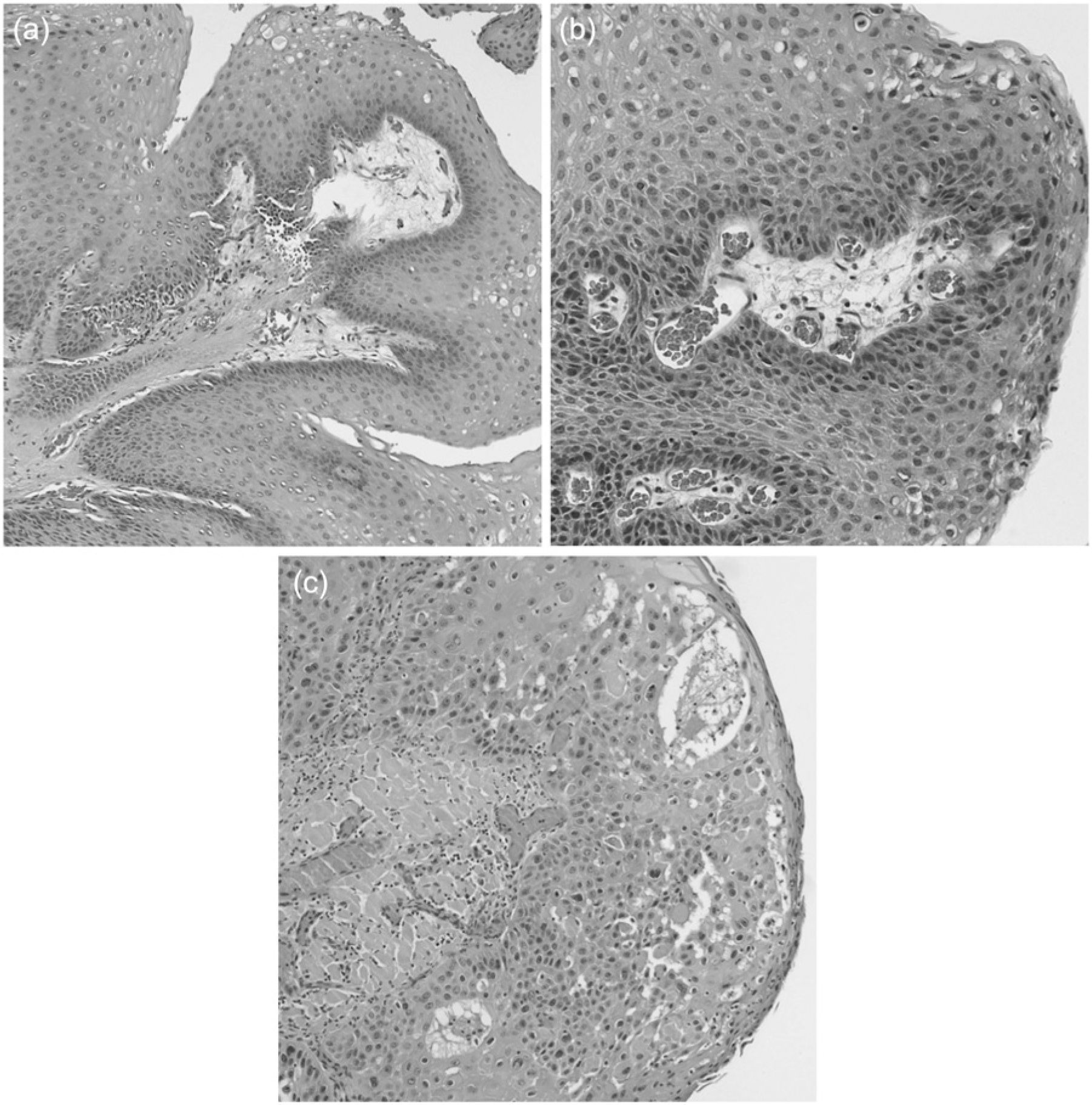
(a) Laryngeal papilloma without dysplasia showing a papillary epithelial frond supported by a fibrovascular core. (b) Mild (low) dysplasia in laryngeal papilloma showing budding of the basal cells with increased hyperchromasia in the basal and parabasal cells but with an otherwise normal maturation. (c) Severe (high) grade dysplasia in laryngeal papilloma showing abnormal maturation with numerous dyskeratotic cells and mitoses involving at least two-thirds of the epithelium.
In situ hybridization (ISH) was carried out on cases of laryngeal papillomatosis with dysplasia where formalin fixed paraffin embedded (FFPE) tissue was available. For HPV testing, hybridization was demonstrated using a biotinylated HPV 6/11 or 16/18 DNA probe (DAKO, Carpinteria, California, USA) and GenPoint Catalyzed Signal Amplification System (DAKO) according to the supplier’s instructions using 3, 3’-diamino benzidine (DAB). Both punctate (consistent with episomal DNA) and diffuse (consistent with HPV integration) staining was evaluated in HPV 6/11 ISH (Figure 2). Positive control was a known HPV 6/11+ condyloma acuminatum. Cases that were HPV 6/11 ISH negative were further examined for HPV 16/18 ISH positivity. Punctate staining in the nuclei (distinct dot-like intranuclear signal) was considered positive for HPV 16/18. Positive control was a known HPV 16/18 + oropharyngeal squamous cell carcinoma, and both a positive DNA and a negative control were run for each specimen.
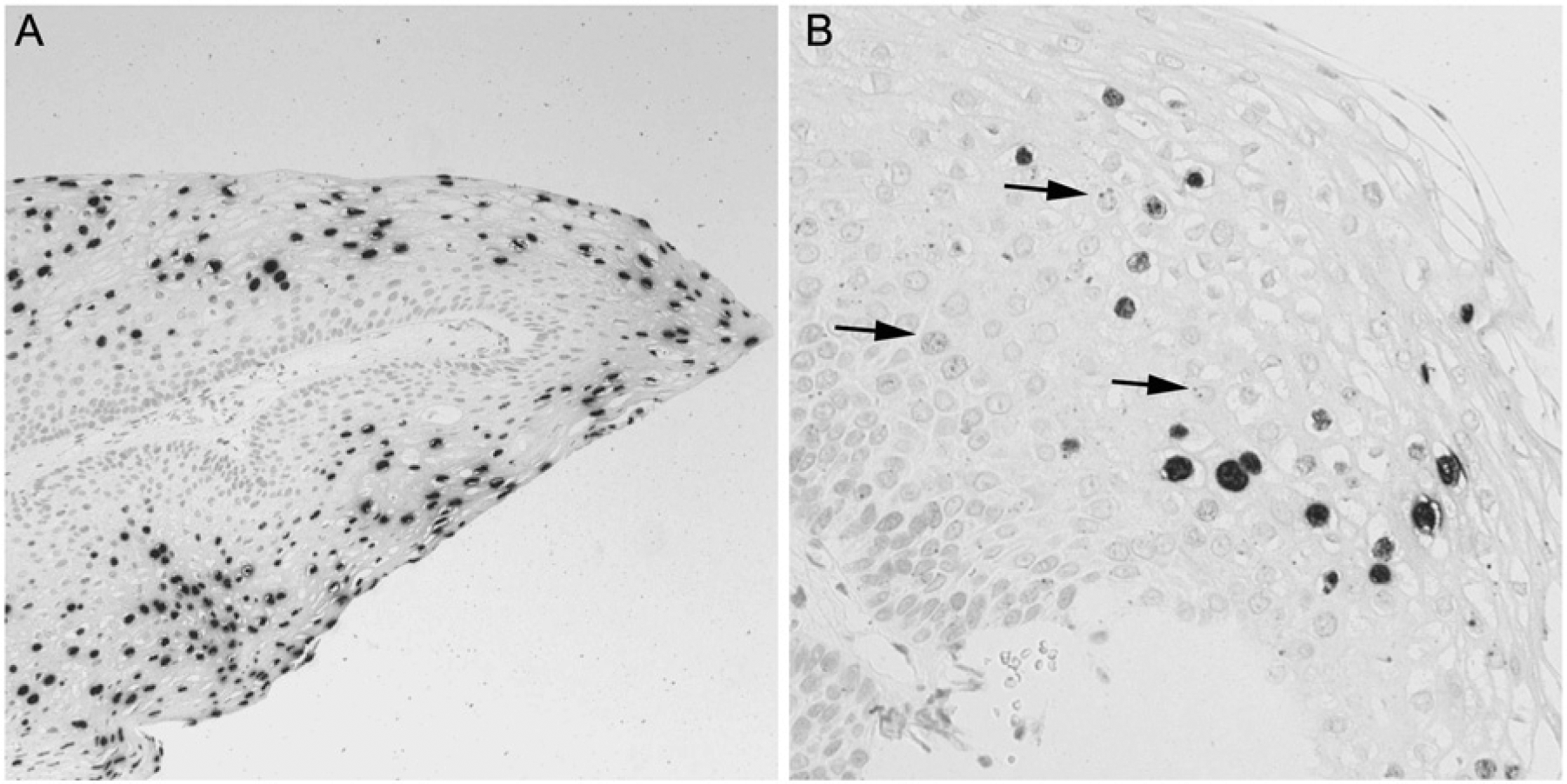
(A) High power image of a papillary frond of laryngeal papilloma showing diffuse in situ hybridization signals of low-risk HPV 6/11 within the nuclei indicating episomal virus. (B) High power image of laryngeal papilloma showing punctuate intranuclear in situ hybridization of HPV 6/11 signal indicating viral integration (arrows). Episomal HPV 6/11 signal is also present.
Data Analysis
Demographic data were codified, scrubbed of identifying information, and analyzed using the SPSS statistical program. Prevalence of dysplasia in initial and revised pathologic specimens was assessed using descriptive statistics. Cohen’s kappa was calculated to determine agreement of presence/absence of dysplasia and grade of dysplasia between the initial pathologic diagnosis and the revised diagnosis on the full patient cohort. Cohen’s kappa is considered to be a superior measure of agreement over other methods (eg, correlation or percentage agreement) because it takes into account chance agreement. Fisher’s exact tests were performed to assess whether the presence of dysplasia differed proportionately between HPV subtypes and whether staining patterns differed between HPV subtypes. Logistic regression analysis was conducted to determine which known risk factors were significant predictors of the presence of dysplasia. For all statistical analyses a P value < .05 was considered statistically significant.
Results
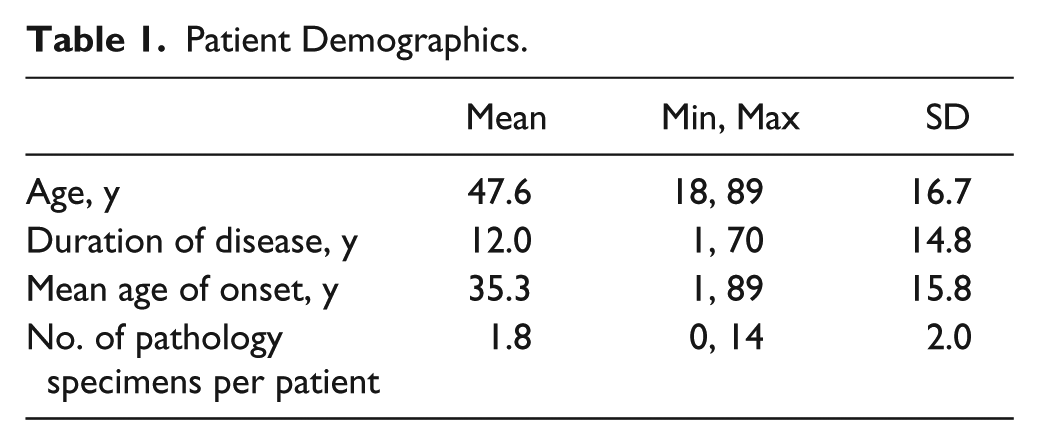
A total of 85 patients (26 females, 59 males) treated for laryngeal papillomatosis at the Emory Voice Center from 2004 to 2010 were identified. Mean patient demographics are listed in Table 1. Of the 85 patients, 17 patients were diagnosed with laryngeal papillomatosis in childhood (juvenile onset recurrent respiratory papillomatosis), while the remaining patients were diagnosed in adulthood. A total of 154 specimens were reviewed, with an average of 1.8 specimens per patient (min 1, max 14). Specimens were obtained for all patients at their first procedure at the Emory Voice Center and at further procedures (direct laryngoscopy under general anesthesia) throughout the disease course for 34 patients. Multiple biopsies at different stages were included in the analysis, but no disease progression was noted.
Patient Demographics.
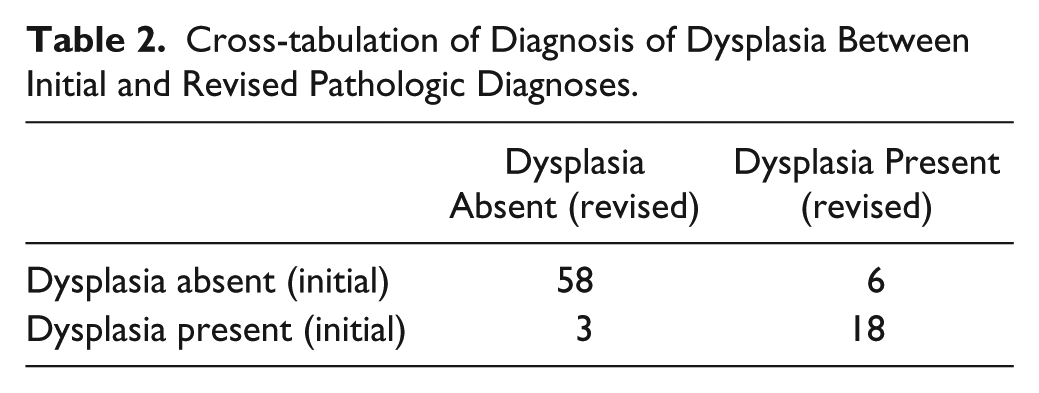
On initial chart review of the patient cohort, 21 patients were identified to have dysplasia. Following pathologic review 24 patients (28%) were identified to have dysplasia. A cross-tabulation of the full sample of patients (85) identified with laryngeal papillomatosis for the presence or absence of dysplasia between the initial diagnosis and the revised diagnosis is presented in Table 2. A Cohen’s kappa of .73 implies very good agreement between the 2 diagnoses assessed agreement between the 2 raters.
Cross-tabulation of Diagnosis of Dysplasia Between Initial and Revised Pathologic Diagnoses.
In addition to presence or absence of dysplasia, agreement between the initial diagnosis and the revised diagnoses was assessed with respect to degree of dysplasia (see Table 3) for the full papilloma cohort. The computed Cohen’s kappa did not reach the level of .70 (kappa = .63) and indicates that the agreement of grade of dysplasia between diagnoses was fair.
Cross-tabulation of Grade of Dysplasia Between Initial and Revised Pathologic Diagnosis.
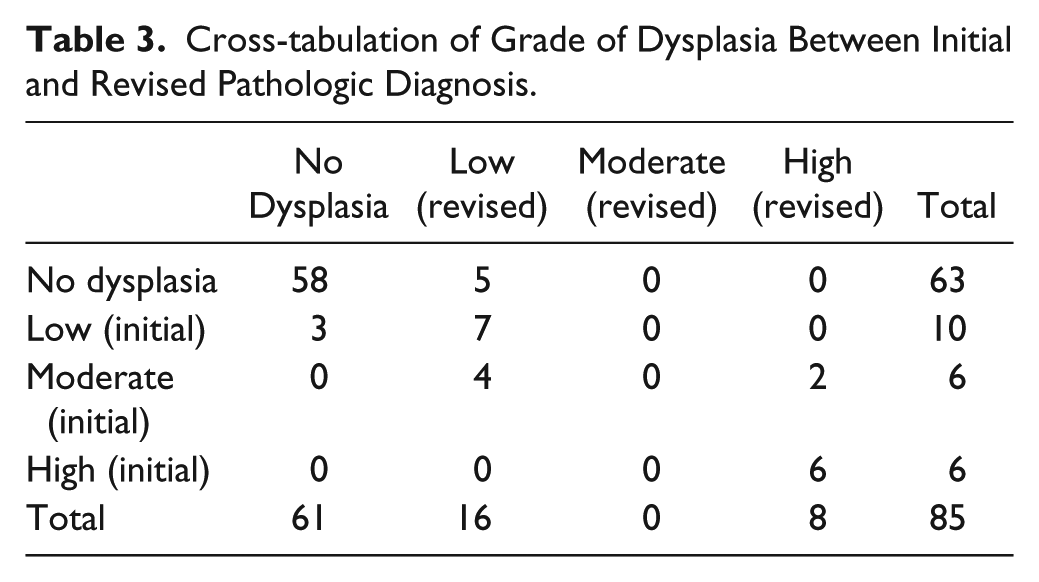
Of the revised subset of 24 patients diagnosed with dysplasia, 5 were identified to have low–grade dysplasia that was initially read “negative for dysplasia.” Three patients initially diagnosed to have mild dysplasia were found to be negative for dysplasia on review. Only specimens classified as high-grade dysplasia were consistent among pathologists.
Of the 24 patients diagnosed with dysplasia, 18 patients had available tissue for HPV subtyping using ISH primers (Table 4). Three of the 18 patients already had HPV subtype documented, thus only a further 15 cases underwent formal ISH testing. Of the 8 patients with high grade dysplasia, 7 had HPV testing (1 had inadequate tissue available for subtyping). All 7 patients were positive for low grade HPV 6/11. Four of 8 had a smoking history, and 4/8 had a history of reflux. No patients with high grade dysplasia had a history of cidofovir exposure.
HPV Subtyping for Dysplasia Patients.
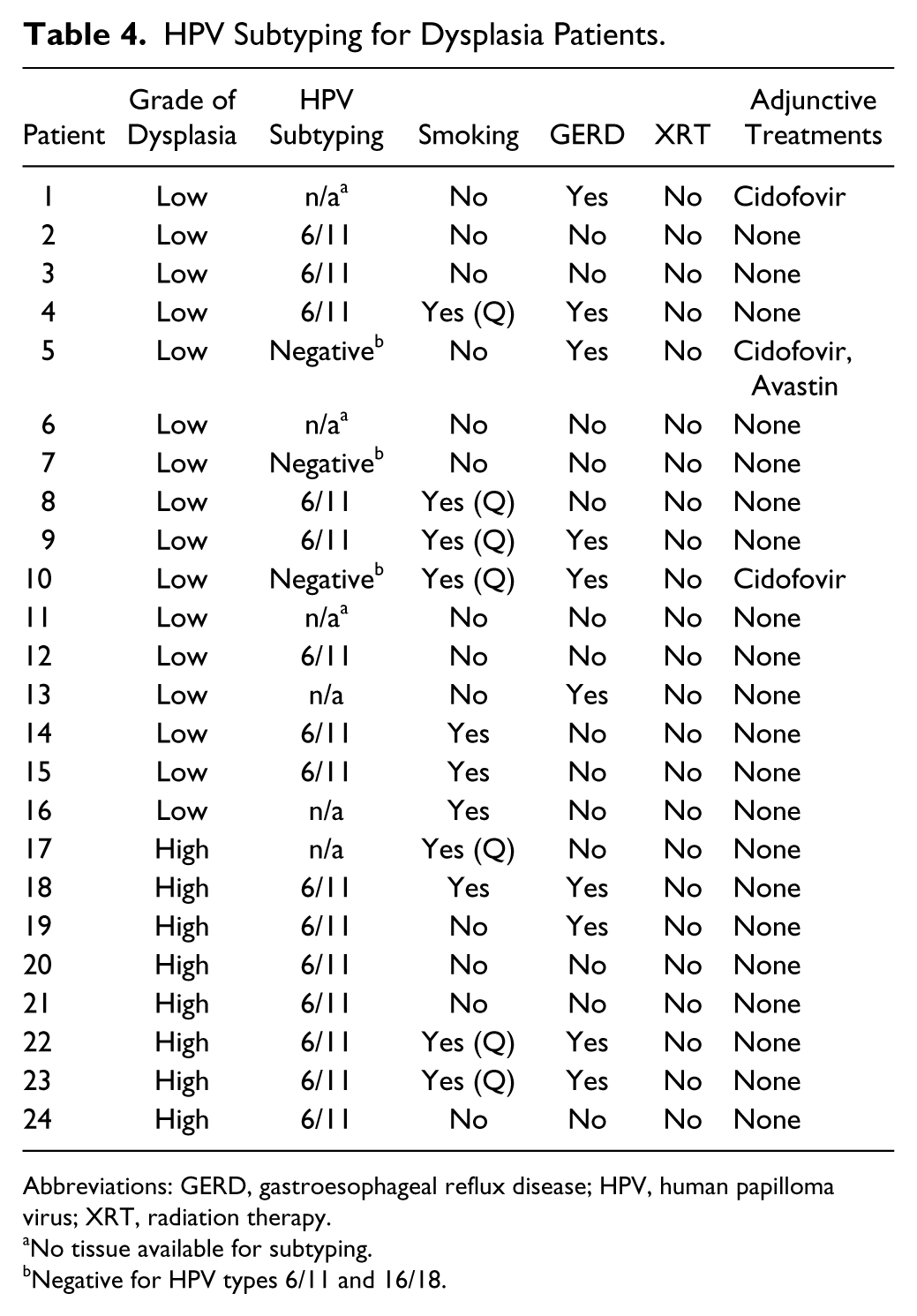
Abbreviations: GERD, gastroesophageal reflux disease; HPV, human papilloma virus; XRT, radiation therapy.
No tissue available for subtyping.
Negative for HPV types 6/11 and 16/18.
Of the remaining 16 patients with low-grade dysplasia, 11 had tissue available for HPV testing with high- and low-risk HPV primers. Eight patients were positive for HPV 6/11 and 3 patients negative for HPV 6/11 and 16/18. Seven patients had a history of smoking, 4 a history of reflux, and 3 had a history cidofovir exposure.
Six patients without dysplasia (confirmed negative for dysplasia on pathologic review) had available HPV subtyping on retrospective chart analysis. All 6 patients were negative for HPV subtypes 16/18, 3 were negative for 6/11 (3 untested for 6/11), and 1 was positive for HPV 6/11.
HPV staining patterns that is, punctate versus diffuse staining (Figure 2) were also assessed for patients with and without dysplasia. Punctate staining patterns were observed in 1 specimen without dysplasia and 7 specimens with dysplasia. Diffuse staining patterns were noted in 7 specimens without and 7 specimens with dysplasia. A Fisher’s exact test indicated that here was no statistical significance (P > .05) observed in the staining patterns associated with dysplasia.
Finally, a logistic regression analysis was conducted on the entire sample (N = 85) to determine which of the known dysplasia risk factors were significant predictors of dysplasia in laryngeal papillomatosis. Due to small sample numbers of patients with adjuvant therapy or immunosuppression, only smoking and a history of acid reflux could be included in the analysis. The analysis did not show that smoking or reflux was a significant predictor of dysplasia. Of note, there were 6 patients who had a history of cidofovir exposure, 3 patients with low grade dysplasia, and 3 patients with no evidence of dysplasia.
Discussion
The primary outcome of this article is to add to the current data regarding the prevalence of dysplasia in the laryngeal papilloma patient population. Two studies5,6 have recently been published citing the incidence of dysplasia in laryngeal papilloma to range from 22% to 50%. We found a dysplasia prevalence of 28% in patients with laryngeal papilloma in our patient population. This is closer to the prevalence cited by Blumin et al 5 who performed a retrospective chart review of 73 adult patients with biopsy proven laryngeal papillomatosis for the presence of laryngeal dysplasia (as determined from existing pathology reports) and potential risk factors associated with dysplasia (as per health record data). Of laryngeal papilloma patients, 22% demonstrated some element of dysplasia, with no difference in associated risk factors in each group. Grade of dysplasia was not defined, nor were HPV subtyping data available.
A similar retrospective cohort was performed by Hall et al. 6 In this study not only were the prevalence (50%) and association of potential risk factors (no statistically significant associations) assessed, but also the grade of dysplasia and HPV subtype (where available). As was seen with our study, low-grade dysplasia was most common (52%), followed by moderate (30%), and then high-grade dysplasia (9%). Interestingly, in our study population, following review of the pathology, patients were primarily diagnosed with low-grade (66%) or high-grade (33%) dysplasia, with few or no patients being classified as moderate grade dysplasia.
There is known interobserver variability in the pathologic classification of laryngeal dysplasia,8-10 particularly in the moderate grades, with higher consistency observed for the low or high grades of dysplasia. While the overall kappa value was low for agreement of dysplasia grade, the primary disagreements occurred in the “moderate grade” category. This is consistent with the known literature.
Hall et al 6 went on to determine the risk of progression to malignancy based on grade of dysplasia. While this was not a primary outcome measure of our article, we had only 2 patients in the severe dysplasia group that progressed to carcinoma (both patients were positive for HPV6/11). No patients in our study cohort with mild dysplasia progressed to carcinoma.
The secondary outcome measure of this study was to determine if high-risk HPV subtypes were associated with laryngeal papillomatosis-associated dysplasia. Both high-risk (HPV 16/18) and low-risk (HPV 6/11) HPV primers were used to assess the presence of HPV in dysplasia specimens. Of the patients tested for HPV subtype the majority of patients (62%) were positive for HPV 6/11 including all of the high-grade dysplasia patients. Three (12%) of the dysplasia patients were negative for both high- and low-risk HPV subtypes. This was similar to the data found in the study by Hall et al 6 who also found HPV 6 to be the most common subtype found in this cohort, however, no conclusive statements regarding HPV status and dysplasia or HPV status and progression of dysplasia could be made due to the limited numbers of patients with documented HPV subtypes. An obvious limitation of our study as well as previous studies cited includes the wide number of potential HPV subtypes, and the inability to specifically subtype each individual case of dysplasia due to expense.
Similar to the previous studies quoted above, our study cohort did not identify an association of known dysplasia risk factors (smoking, reflux) with the presence of dysplasia. It is possible that presence of dysplasia rests purely on the disease itself as opposed to potential underlying risk factors including HPV subtype. This is corroborated by the lack of evidence for HPV association in laryngeal dysplasia in the absence of laryngeal papilloma.
Waters et al 4 evaluated the presence of HPV in dysplasia not associated with laryngeal papilloma. A cohort of patients with high-grade laryngeal dysplasia or carcinoma in situ was tested for HPV by ISH. Of the 15 patients tested, only 1 specimen was positive for HPV (high-risk HPV subtype). Eleven of the 15 patients had a smoking history. This very small cohort demonstrated that HPV is rarely associated with laryngeal dysplasia in the absence of laryngeal papillomatosis.
Limitations of the Study
While laryngeal papillomatosis is relatively easily diagnosed via pathologic evaluation, dysplasia diagnosis has greater variability and discordance between pathologists particularly in grading the degree of dysplasia.8-10 Dysplasia can be categorized as low, moderate, and high grade. While there are guidelines for grading dysplasia, this is subjectively interpreted by the pathologist reading the slides; therefore, cases that are misread as nondysplasia may actually have mild dysplasia and be excluded from the cases but be selected in the control group. We aimed to reduce interrater variability by having a single dedicated pathologist review the initial diagnosis.
An additional limitation of the study design is the reliance on previously recorded information for data collection. This is particularly important for the collection of confounding variables/risk factors including smoking and reflux. Another potential limitation of this study is that is was performed at a single institution resulting in a convenience sample that could potentially under-represent all socioeconomic groups, races, and ethnicities, with a possible overrepresentation of complicated cases being referred for tertiary care management. This limitation, however, is overcome by the fact that the incidence of laryngeal papillomatosis is low, and the majority of cases in the region are referred to this tertiary care institution for specialized management of the condition regardless of location, race, and socioeconomic status.
Conclusions
We identified a 24% prevalence of dysplasia in laryngeal papillomatosis in our patient population. We do not identify any association of high-risk HPV subtype with laryngeal papillomatosis. By adding to the emerging data on dysplasia prevalence in laryngeal papillomatosis, we hope to aid clinicians in their education of patients diagnosed with laryngeal papillomatosis, including their associated risk of progression to dysplasia and potential malignancy. In addition, by establishing important subtypes in the progression of laryngeal papillomatosis to dysplasia, we can advocate the need for specific HPV subtypes to be represented in HPV vaccines and potentially prevent HPV related laryngeal papilloma and dysplasia by promoting HPV vaccination.
Footnotes
Authors’ Note
All work was undertaken at the Emory Voice Center, Emory University, Atlanta, Georgia. This work was presented in poster format at the Triological Society at the Combined Otolaryngological Spring Meetings in 2013.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.