
Abstract
Objective:
Deconditioning and frailty may contribute to dysphagia and aspiration. Early identification of patients at risk of aspiration is important. Aspiration prevention would lead to reduced morbidity and health care costs. We therefore wondered whether objective measurements of frailty could help identify patients at risk for dysphagia and aspiration.
Methods:
Consecutive patients (n = 183) were enrolled. Patient characteristics and objective measures of frailty were recorded prospectively. Variables tested included age, body mass index, grip strength, and 5 meter walk pace. Statistical analysis tested for association between these parameters and dysphagia or aspiration, diagnosed by instrumental swallowing examination.
Results:
Of variables tested for association with grip strength, only age category (P = .003) and ambulatory status (P < .001) were significantly associated with grip strength in linear regression models. Whereas walk speed was not associated with dysphagia or aspiration, ambulatory status was significantly associated with dysphagia and aspiration in multivariable model building.
Conclusion:
Nonambulatory status is a predictor of aspiration and should be included in risk assessments for dysphagia. The relationship between frailty and dysphagia deserves further investigation. Frailty assessments may help identify those at risk for complications of dysphagia.
Frailty is increasingly recognized as an important predictor of prognosis. Frailty has been defined by Fried and colleagues 1 as “a clinical state of increased vulnerability and decreased ability to maintain homeostasis that is age-related and centrally characterized by declines in functional reserves across multiple physiologic systems.” The relationship between frailty and dysphagia is synergistic. The sequelae of dysphagia including malnutrition and pneumonia certainly contribute to the development of frailty. On the other hand, deconditioning and frailty may contribute to dysphagia and aspiration. Decline in tongue strength is associated with age and has clinical relevance with respect to the development of dysphagia. The correlation between tongue strength and grip strength 2 as well as other measures of physical strength including jump height and power has been established. 3 Measures of frailty including grip strength and walking speed have also been associated with increased morbidity 4 and mortality5,6 in a variety of populations.
Early identification of patients at risk of aspiration is important as aspiration pneumonia often leads to increased length of stay and health care costs.7,8 Effective aspiration prevention may lead to reduced morbidity and health care costs. We therefore wondered whether objective measurements of frailty could help identify patients at risk for dysphagia and aspiration. Tongue strength and hand grip strength have been established as objective parameters for assessment in multiple studies of swallowing function. 9 Whereas tongue strength requires specialized equipment for accurate assessment, hand grip strength can easily be measured with a dynamometer. Gait speed is another validated measure of performance and has been linked to survival in older adults. 10
Materials and Methods
Consecutive patients referred to the outpatient swallowing clinic were enrolled. Patient characteristics and objective measures of frailty were recorded prospectively. Demographic information including age and sex were recorded. Grip strength was measured with a hand-held hydraulic dynamometer set at level 2 (Jamar Inc, Bolingbrook, Illinois, USA) and reported in units of kilograms-force (kgf). The dominant hand was used unless there was a limitation (trauma, paralysis). Three attempts were recorded and the maximum value was recorded as grip strength. Walking speed was measured by asking patients to walk 5 meters at their normal pace. Assistive devices such as canes and walkers were allowed. Patients in wheelchairs were designated nonambulatory. Comorbid conditions contributing to dysphagia were also recorded. The presence or absence of dysphagia was recorded as well as the type of dysphagia (oral, oropharyngeal, pharyngeal, esophageal).
We categorized grip strength using 2 different methods. For each of the 2 methods, grip strength categories were defined separately for men and women. For the first categorization methods, we identified patients with the lowest quartile of grip strength for their sex and defined these patients as the weakest Q1 and patients in the upper 3 quartiles as the stronger Q2 to Q4. For the second categorization methods, we defined the stronger versus weaker grip strength based on median value of the strongest patients, analyzing men and women separately. Age category (defined by the median), ambulatory status, pneumonia diagnosis within 3 months of study enrollment, hospitalization for at least 3 days within 1 month of study enrollment, and presence/absence of neurological disorder were tested for significant association with grip strength using linear regression models. A description of the frequency of these characteristics in the study population is provided in Table 1. Of variables found to be significantly associated with grip strength, the category or combination of categories with the stronger grip strength was used to define grip strength (stronger/weaker) based on the median value. Two walk speed categories were defined based on the distribution of walk speed in the unassisted ambulatory study population.
Summary of Patient Characteristics.
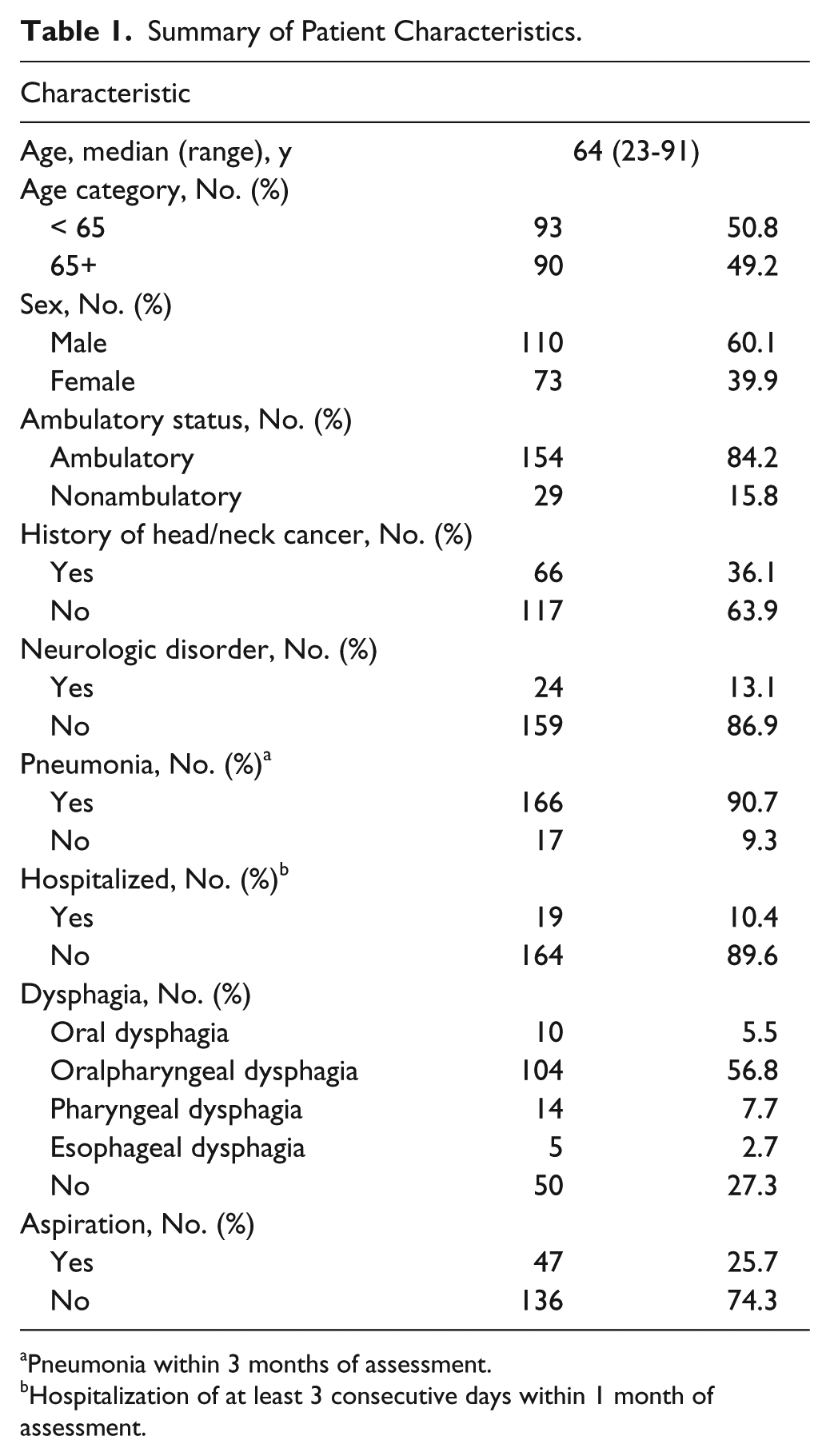
Pneumonia within 3 months of assessment.
Hospitalization of at least 3 consecutive days within 1 month of assessment.
The following variables were tested for significant association with (1) dysphagia and (2) aspiration separately using univariate logistic regression analyses: age, sex, ambulatory status, history of head and neck cancer, diagnosis of neurological condition, diagnosis of pneumonia within 3 months of study enrollment, and hospitalization of at least 3 consecutive days within 1 month of study enrollment. Variables found to be statistically significantly associated (Wald P < .05) with dysphasia and/or aspiration were tested for association in multivariable logistic regression models and retained in the main effects model if the associated Wald P < .05. Grip strength category and walk speed category, the primary variables of interest, were tested for association with dysphagia and aspiration in univariate models and after adjusting for variables in the main effects model. Models were developed for all patients and for patients without a history of head and neck cancer separately.
Results
Complete data were obtained for 183 patients. Characteristics of the cohort are described in Table 1.
Women with the lowest 25th percentile of grip strength were defined as those having grip strength of 15.9 kgf or less; men with the lowest 25th percentile of grip strength were defined as those having grip strength of 27.2 kgf or less. Thirty-four of 110 men (31%) and 24 of 73 women (33%) had grip strengths in the lowest 25th percentile. Due to similar grip strengths of patients, the actual number of patients assigned to the weakest quartile was greater than 25% of patients. Of variables tested for association with grip strength, only age category (P = .003) and ambulatory status (P < .001) were significantly associated with grip strength in linear regression models. Grip strength was significantly higher for patients younger than 65 years of age and for patients who were ambulatory. The general diminishment of grip strength with increasing age for both men and women is apparent in Figures 1A and 1B. We, therefore, defined stronger and weaker grip strength separately for men and women based on the median grip strength for patients who were younger than 65 years and who were ambulatory. For men, grip strength of less than 40.9 kgf was defined as weaker and 40.9 kgf or more was stronger. For women, grip strength of less than 24.9 kgf was defined as weaker and 24.9 kgf or more was defined as stronger. Seventy-four of 110 men (67%) and 50 of 73 women (68%) were defined as having weaker grip strength.
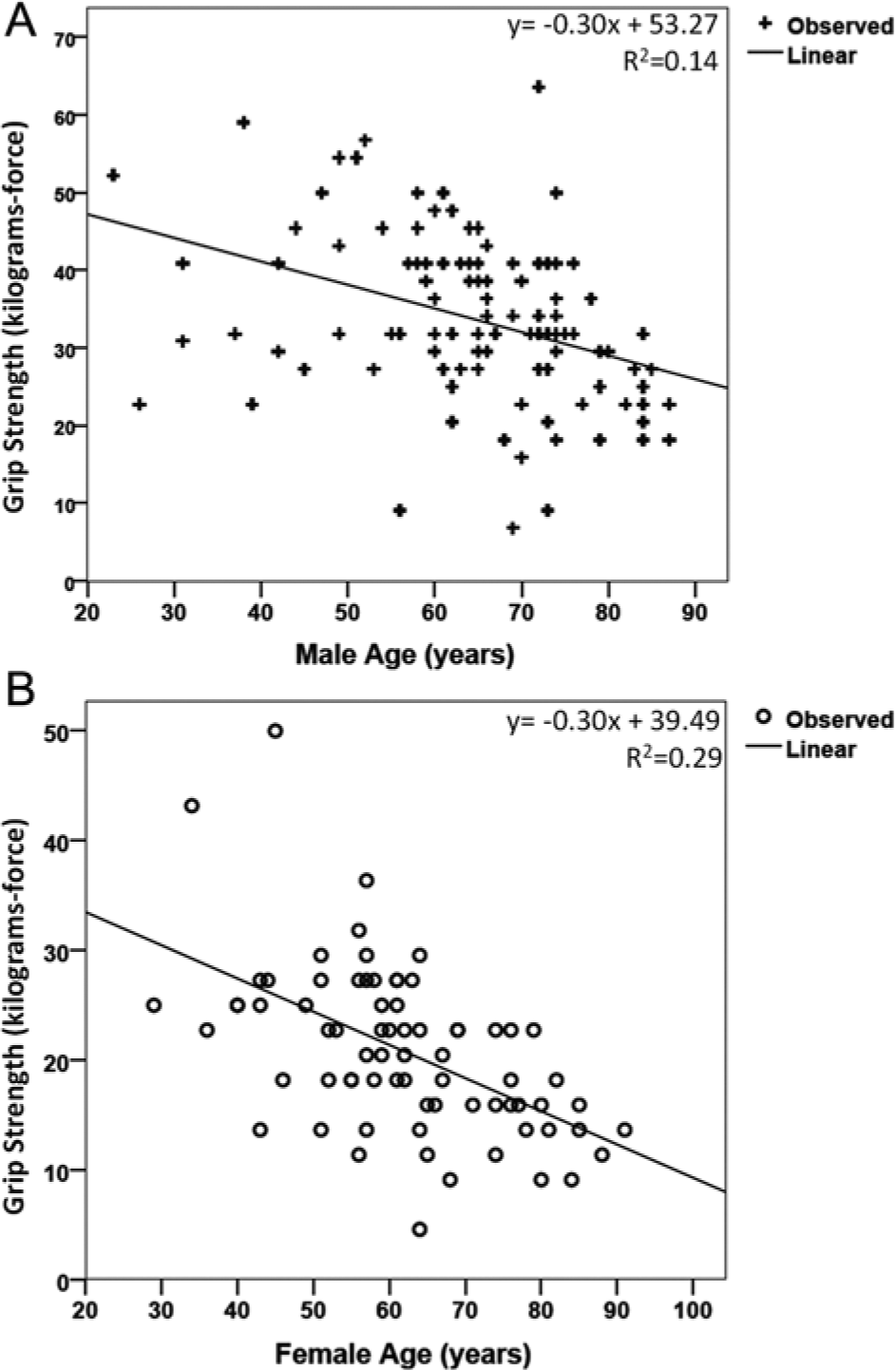
Plots of grip strength by age for men (A) and women (B). Linear regression curve estimation equation and R2 values provided.
The time required by each patient to traverse 5 meters was determined. Meters per second (m/s) walk speeds were calculated and were determined to be independent of age. Plots of walk speed by age for men and women are provided in Figures 2A and 2B, respectively. The distribution of walk speeds was graphed for those patients who were ambulatory and able to walk unassisted by a cane (Figure 2C). Three ambulatory patients required the use of a cane, and their walk speeds, which are not included in Figure 2C, were 0.4, 0.6, and 0.8 m/s. The majority of patients had walk speeds between 1.0 and 1.7 m/s. Patients whose walk speeds were 0.8 m/s or slower were defined as slower, whereas patients with walk speeds of 1.0 m/s or faster were defined as quicker, as illustrated in Figure 2C.
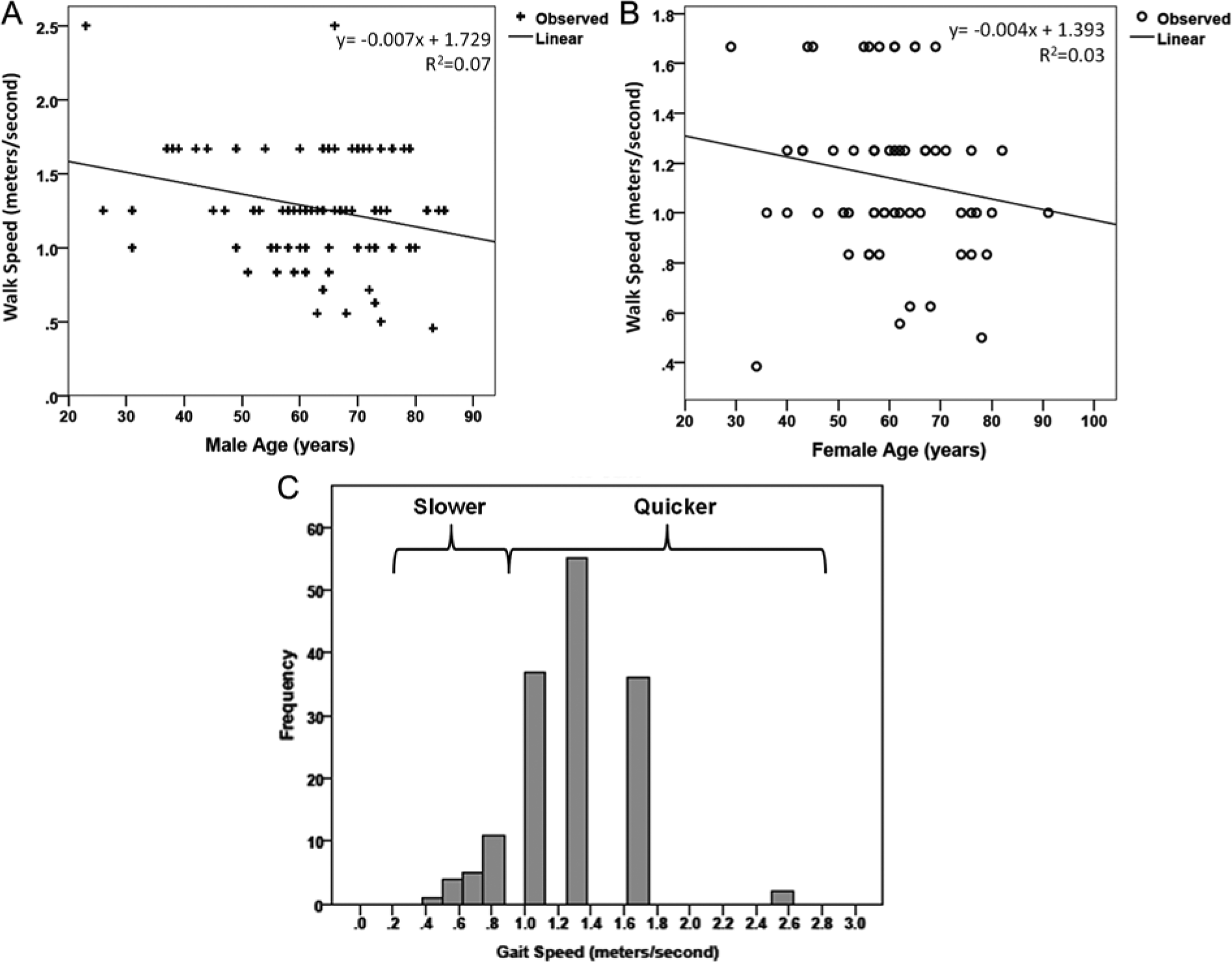
Plots of walk speed by age for men (A) and women (B). Linear regression curve estimation equation and R2 values provided. (C) Distribution of walk speeds among ambulatory patients who did not require use of a cane. Patients whose walk speeds were 0.8 m/s or slower were defined as slower for regression analysis, and patients whose walk speeds were 1.0 m/s or faster were defined as quicker.
In univariate models, age 65 years or older, male sex, nonambulatory status, positive history of head and neck cancer, and weaker grip strength were all significantly associated with dysphagia among all patients (Table 2). The strongest association with dysphagia was a positive history of head and neck cancer, as patients with a history of head and neck cancer were more than 20 times more likely to have dysphagia (P < .001). Patients 65+ years of age or nonambulatory were almost 4 times more likely to have dysphagia. Patients with weaker grip strength were more than twice as likely to have dysphagia compared to patients with stronger grip strength. Walk speed was not associated with dysphagia and neither was having grip strength within the lowest quartile (weakest Q1). Age, ambulatory status, and history of head and neck cancer were all significantly associated with dysphagia in a multivariable model containing all 3 variables. Weakened grip strength, defined using either method, and walk speed were not significantly associated with dysphagia after controlling for age, ambulatory status, and history of head and neck cancer.
Test of Characteristics for Association With Dysphagia. a
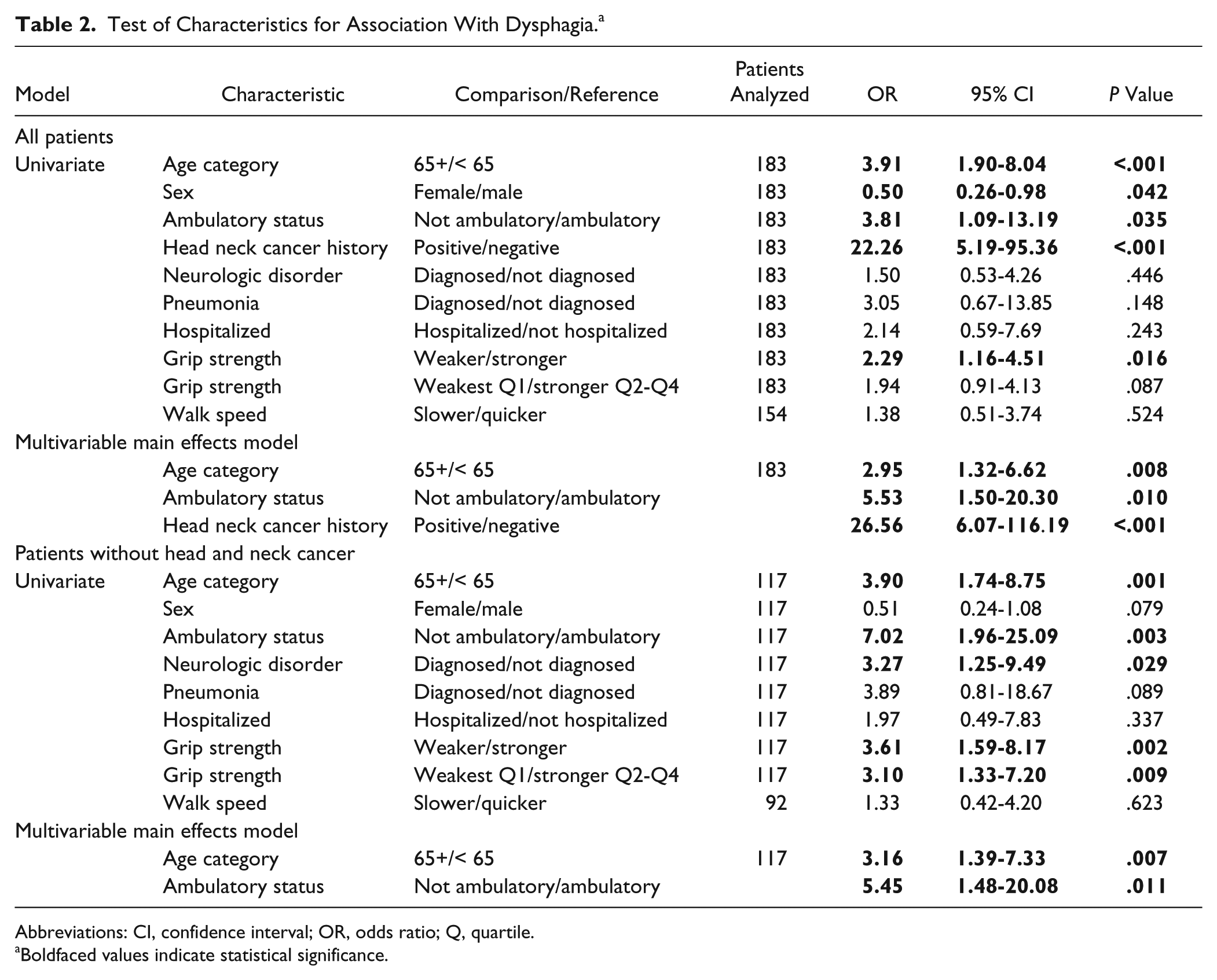
Abbreviations: CI, confidence interval; OR, odds ratio; Q, quartile.
Boldfaced values indicate statistical significance.
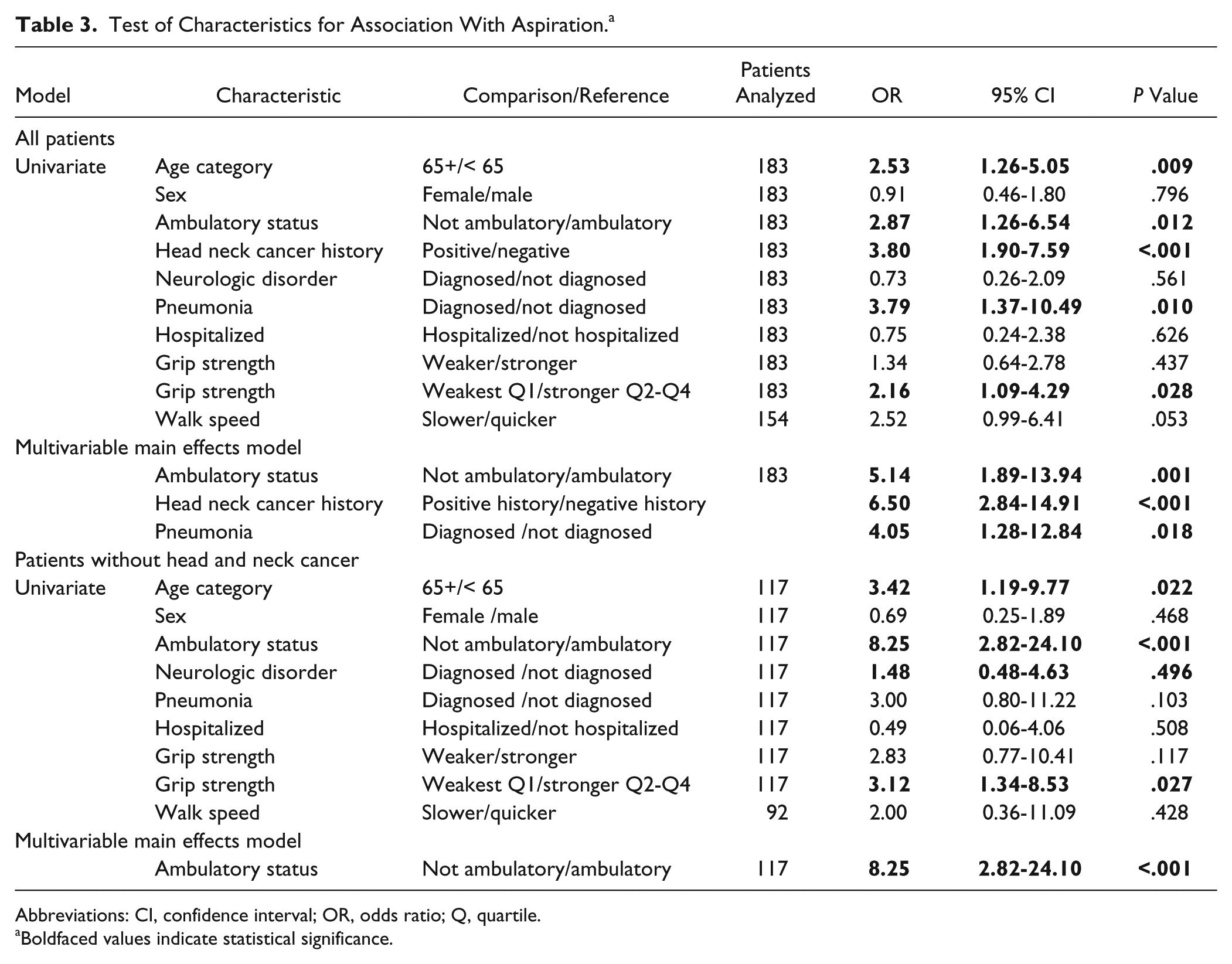
We found similar associations with aspiration for all patients (Table 3). As with dysphagia, age 65 years or older, nonambulatory status, and a positive history of head and neck cancer were also associated with increased likelihood of aspiration. Walk speed was also not associated with aspiration. In contrast to dysphagia, a recent diagnosis of pneumonia or having grip strength in the weakest Q1 was associated with greater likelihood of aspiration. Patient sex and weaker grip strength defined by method 2 were not significant contributors. Positive history of head and neck cancer and recent diagnosis of pneumonia were both associated with almost 4 times the likelihood of aspiration compared to patients without these characteristics. In the multivariable model, ambulatory status, history of head and neck cancer, and recent diagnosis of pneumonia were associated with aspiration in a model containing all 3 variables. Neither weakened grip strength as defined using either method nor walk speed was significantly associated with aspiration after controlling for the effects of ambulatory status, history of head and neck cancer, and recent history of pneumonia.
Test of Characteristics for Association With Aspiration. a
Abbreviations: CI, confidence interval; OR, odds ratio; Q, quartile.
Boldfaced values indicate statistical significance.
Among patients without a history of head and neck cancer, age 65+ years, nonambulatory status, diagnosis of neurological disorder, and weakened grip strength, defined using either method, were significantly associated with dysphagia in independent univariate models (Table 2). In these patients, nonambulatory status was associated with a 7-fold increased likelihood of dysphagia. Age 65+ and nonambulatory status remained significantly associated with increased likelihood of dysphagia in the multivariable model containing both. Neither weakened grip strength, as defined using either method, nor walk speed was associated with dysphagia after controlling for age and ambulatory status. We found similar associations with aspiration among patients without a history of head and neck cancer (Table 3). Nonambulatory status was associated with a greater than 8-fold increase in likelihood of aspiration among these patients. Age 65+, diagnosis of neurological disorder, and grip strength in the weakest Q1 were significantly associated in independent models with aspiration among patients without a history of head and neck cancer. In a model containing ambulatory status, neither age nor diagnosis of neurological disorder remained significantly associated with aspiration after controlling for ambulatory status. Therefore, ambulatory status was the only variable remaining significantly associated in multivariable model building. Weakened grip strength defined by either method was not significantly associated with aspiration after controlling for the effects of ambulatory status. We were unable to test the effects of walk speed after controlling for the effects of ambulatory status because of the absolute covariance of these variables; patients who were nonambulatory lacked a 5 meter walk speed assessment.
Discussion
Frailty has been linked to adverse outcomes in multiple studies. Hand grip strength and gait speed have been established as reliable measures of frailty.4,11,12 Butler et al 2 did not observe a significant difference in grip strength between healthy, community-dwelling adult aspirators and nonaspirators, but they did notice a correlation between grip strength and posterior tongue strength. Similarly, Buehring and colleagues 3 observed a positive correlation between anterior tongue pressures and grip strength as well as jump height and power. Although the data presented here do indicate a relationship between hand grip strength and dysphagia in the univariate analysis, multivariate analysis did not substantiate this relationship. However, further investigation is necessary to determine if grip strength may be associated with dysphagia and aspiration in other settings including acute care, rehabilitation, and skilled nursing facilities.
We did identify nonambulatory status as a strong predictor for dysphagia and aspiration. We observed a more than 8-fold increase in aspiration risk in nonambulatory patients. Inability to complete a 5 meter walking task denotes a severe form of gait impairment. Although we were unable to identify a specific 5 meter walk pace limit that would signify a higher risk of dysphagia or aspiration, there were relatively few patients with prolonged 5 meter walk speeds. The fact that such a high rate of aspiration occurred in nonambulatory patients suggests that decline in walk speed may be a predictor of dysphagia.
The results presented here may be confounded by the fact that the study was performed in an outpatient setting dedicated to the treatment of swallowing disorders. A high proportion of the patients in this setting have dysphagia related to a wide variety of causes other than frailty. Approximately 36% of the patients in this study were being treated for head and neck cancer or had a history of treatment for head and neck cancer. Severity of dysphagia for these head and neck cancer patients is likely disproportionate to their overall conditioning. Analysis performed excluding those with head and neck cancer revealed stronger associations between the frailty markers (grip strength and nonambulatory status) and dysphagia and aspiration. The remainder of patients with dysphagia had a variety of diagnoses, with the most frequently encountered being stroke, Parkinson’s disease, history of cervical spine surgery, and Zenker’s diverticulum. These varied comorbid conditions likely affected grip strength and walk speed in different ways not accounted for in this study. Examining a more homogeneous population may reveal different associations between grip strength, walk speed, and dysphagia. However, the purpose of this exploratory study was to determine whether grip strength and walk speed might be indicators of dysphagia in a broader population.
Those most severely affected by frailty are often in acute care or nursing facilities or may be homebound. Frailty associated dysphagia is likely encountered much more frequently in these settings. Future studies should address frailty as a risk factor for dysphagia in hospitals and nursing homes.
Conclusion
The relationship between frailty and dysphagia deserves further investigation. Identification of those at risk for dysphagia would allow clinicians to direct screening resources more efficiently with the ultimate goal of decreasing the morbidity, mortality, and costs associated with complications of dysphagia. Nonambulatory status is a predictor of aspiration and should be included in risk assessments for dysphagia. Frailty assessments may provide a means of screening patients who may benefit from formal dysphagia assessment with a speech-language pathologist or other dysphagia specialist.
Footnotes
Authors’ Note
This was a podium presentation given at the ABEA meeting in Orlando, Florida, on April 10, 2013.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Support was provided by the Department of Otolaryngology, University of Pittsburgh School of Medicine.