
Abstract
Objective:
This study aimed to determine if preoperative impedance testing changed management and if testing was associated with surgical outcome in patients undergoing airway reconstruction.
Methods:
Retrospective review of patients who had impedance testing prior to airway reconstruction at a tertiary pediatric hospital from January 2010 to September 2011. Charts were reviewed for demographics, medical/surgical history, impedance testing, and surgical outcomes.
Results:
Fifty-seven patients were included. Forty-seven (82%) were premature. Forty-seven (82%) had a primary diagnosis of subglottic stenosis. Twenty-six (45%) had prior airway surgery. Thirty-six (63%) had gastroesophageal reflux and 21 (36%) had undergone fundoplication. Patients without fundoplication had a median 46 total reflux, 7 proximal, and 14.5 acidic events compared to a median 5 total reflux, 0 proximal, and 0 acidic events in patients with fundoplication. Impedance testing changed management in 22% (8/36) of nonfundoplication patients and 9.5% (2/21) of fundoplication patients. In unadjusted analysis, fewer fundoplication patients had successful surgery compared to those without (33% vs 67%, P = .01). Prematurity, age at surgery, and previous airway surgery were also important predictors of surgical success.
Conclusion:
Fewer patients than anticipated had a change in management. Impedance testing was unlikely to change management in fundoplication patients. Patients with fundoplication were less likely to have a successful outcome, suggesting that factors other than reflux influence airway reconstruction outcomes.
Introduction
Gastroesophageal reflux disease (GERD) has long been thought to contribute to failures in airway surgery. Evidence suggests a connection between GERD and the development of subglottic stenosis, and studies in animal models have shown that gastric juices negatively affect mucosal healing after subglottic injury.1-5 In a rabbit model of laryngotracheal reconstruction (LTR), simulated GERD led to significant inflammation and subsequent cartilage necrosis. 6 Given the potential negative effect of GERD on operative success, patients undergoing airway reconstruction at our institution are routinely evaluated for GERD prior to surgery. This evaluation can include esophagram, esophagogastroduodenoscopy (EGD) with biopsy, and pH-multichannel intraluminal impedance (pH-MII) testing.
Testing with pH-MII technology combines standard pH monitoring with impedance monitoring, which allows for measurement of gas, liquid, and combined reflux events. 7 The impedance sensors used in pH-MII do not rely on pH, making it possible to evaluate both acid and non-acid reflux events, as opposed to a pH probe, which can evaluate only acidic events. pH-Multichannel intraluminal impedance is particularly useful in the setting of non-acidic or weakly acidic reflux (such as children on anti-reflux medication) and in children with suspected feeding-related reflux.7,8
Although pH-MII testing is part of the preoperative evaluation in many patients prior to airway reconstruction at our institution, we lack data to guide which patients would benefit from such testing. pH-Multichannel intraluminal impedance testing is performed at the discretion of the individual providers without set guidelines to determine which patients should undergo pH-MII testing. This variation in practice was part of the impetus for the study. The goal of this study was to determine if preoperative impedance testing changed patient management and if testing correlated with surgical outcome in patients undergoing open airway reconstruction.
Materials and Methods
After institutional review board approval was obtained, we identified all patients who underwent open airway reconstruction between January 2010 and September 2011 at Cincinnati Children’s Hospital Medical Center. We reviewed the charts of these patients to obtain demographic data, medical and surgical history, comorbidities, pH-MII testing results, and surgical outcomes. Patients without documented pH-MII testing were excluded from the study.
In nearly all patients, the pH-MII probe was placed intraoperatively by a gastroenterology technician at the conclusion of the EGD. A plain radiograph was obtained postoperatively to confirm good position of the probe. Patients were admitted for overnight observation with the caregiver maintaining a log of events and symptoms while the probe was in place. pH-Multichannel intraluminal impedance uses sensors distributed throughout the esophagus to measure the resistance to a flow of current. There are 7 impedance sensors that generate 6 impedance channel waves throughout the esophagus, and based on impedance changes within these channels, it is possible to determine the directionality of the flow (eg, reflux event vs swallow) as well as the height of the refluxate. Because liquid and gas have different impedances (eg, resistance to a current flow), it is possible to differentiate the composition of the refluxed material (liquid, gas, or mixed). There is also a distal pH sensor in the catheter that measures whether the refluxate is acid (pH < 4) or non-acid (pH > 4). A liquid reflux episode was defined as a retrograde decrease in impedance to 50% of the baseline value or below, in at least the 2 distal impedance channels. A proximal event was defined as a reflux episode that reaches 1 of the 2 most proximal channels. Symptom associated probability (SAP) was calculated by automated software based on the temporal relationship between symptoms and all reflux events. Symptom associated probability was considered positive if the probability was greater than or equal to 95%.
We examined the baseline characteristics including demographics, airway diagnosis, history of tracheostomy, history of prior airway surgery, diagnosis of GERD, proton pump inhibitor (PPI) usage, history of gastrostomy tube placement, and history of Nissen fundoplication. A change in management was defined as a change in treatment or diagnosis. Successful surgical outcome was defined as surgical goal obtained following initial surgery. The goal of surgery was classified as decannulation or alleviation of stenosis. If the open airway reconstruction following impedance testing accomplished this goal, the surgery was deemed successful. Descriptive statistics were calculated on all variables. Distributions of continuous variables were evaluated for normality. Non-normally distributed variables are described as medians with ranges or interquartile ranges (IQRs).
Since patients who have a history of fundoplication represent a specific subset of patients who have theoretically received the gold standard treatment for GERD, we examined impedance measures and tested differences between the groups using Wilcoxon rank sum tests. Chi-square tests or Fisher’s exact tests were used to examine relationships between categorical variables. Multivariable logistic regression was used to simultaneously examine several factors including history of fundoplication, age at surgery, prematurity, presence of a syndrome, previous airway surgery, pulmonary comorbidity, and neurologic comorbidity on the outcome of surgical success. Logistic regression models stratified by history of fundoplication were used to examine the role of preoperative impedance measures on changes in management and surgical success. Natural log transformations were used to normalize continuous impedance measures in regression models. All analyses were conducted using SAS (version 9.3; SAS Institute Inc, Cary, North Carolina, USA).
Results
During the study period, 150 patients underwent open airway reconstruction. Of these, 57 (38%) underwent preoperative pH-MII testing and were included in the study. Demographic data and baseline characteristics are presented in Table 1. As shown, the majority of patients had a primary airway diagnosis of subglottic stenosis (n = 47, 82%). Thirty-six (63%) had a pre-existing diagnosis of GERD and 30 (52%) were already taking a PPI at the time of evaluation. The median duration of follow-up was 11 months (range, 1-31 months).
Study Population Characteristics.
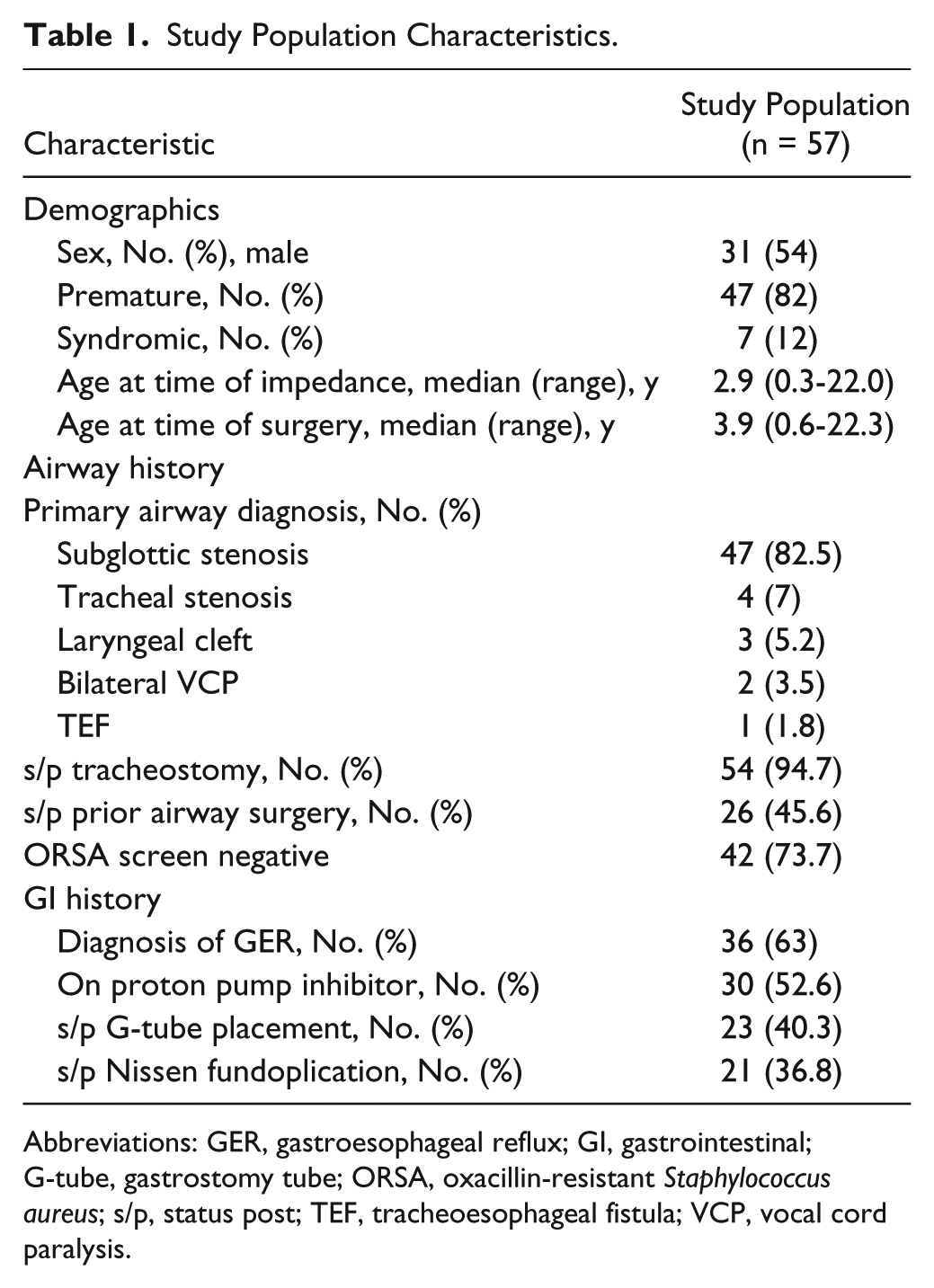
Abbreviations: GER, gastroesophageal reflux; GI, gastrointestinal; G-tube, gastrostomy tube; ORSA, oxacillin-resistant Staphylococcus aureus; s/p, status post; TEF, tracheoesophageal fistula; VCP, vocal cord paralysis.
Twenty-one patients had a history of fundoplication prior to pH-MII testing. Table 2 demonstrates the results of pH-MII testing for patients with a history of fundoplication compared to those without a fundoplication. Patients with a fundoplication had overall fewer reflux events. Eight patients (22%) without a fundoplication experienced a change in management compared to only 2 patients (9.5%) with a fundoplication. In unadjusted analysis, fewer patients with a fundoplication had a successful surgery compared to those without (33% vs 67%, P = .01). The multivariable model examining fundoplication and other factors indicated that prematurity, age at surgery, and previous airway surgery were also important predictors of surgical success.
Effect of Nissen Fundoplication on Impedance Characteristics.
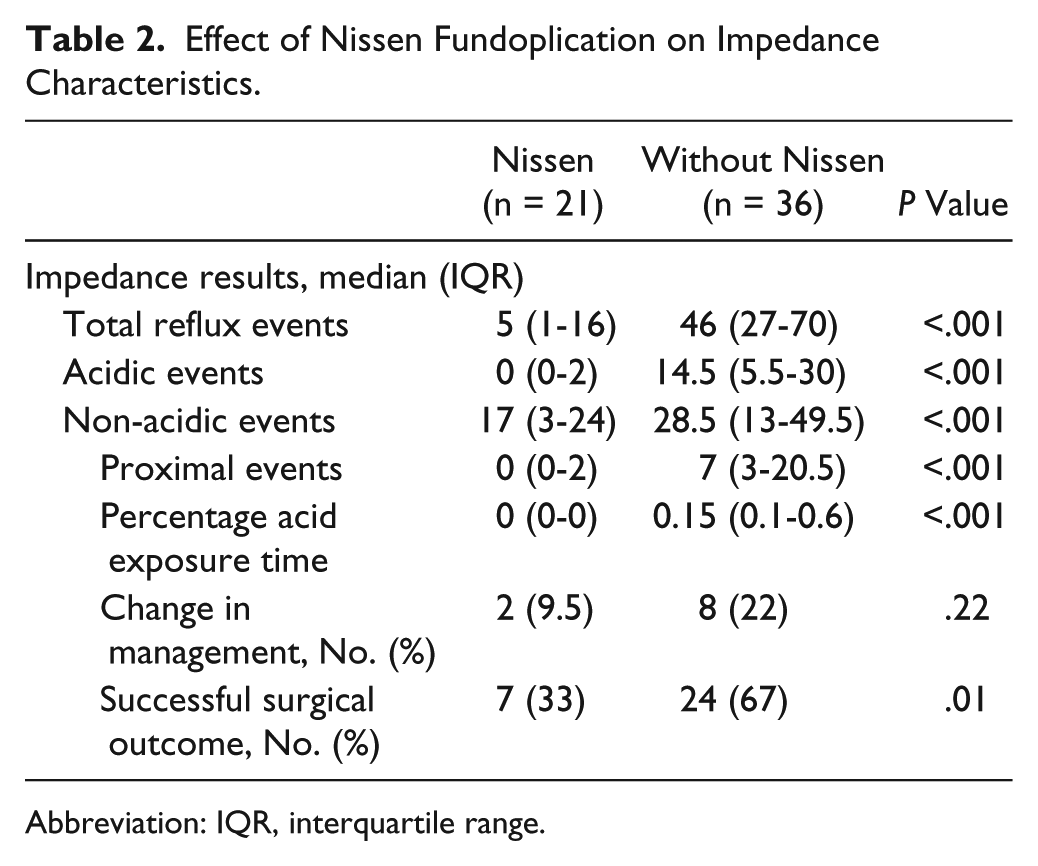
Abbreviation: IQR, interquartile range.
Overall, 10 patients (17.5%) had a change in management. Eight patients had a change in diagnosis, 7 patients had a medication change, and 5 patients had both (see Table 3). Odds ratios (ORs) for impedance measures predicting changes in management for patients without fundoplication are seen in Table 4. Too few patients with a fundoplication had a change in management (n = 2) to perform a regression analysis on these patients independently. When regression analysis was performed on the patients without fundoplication, the number of acidic events (OR = 2.8; 95% confidence interval [CI], 1.0-8.0; P = .05), the number of proximal events (OR = 3.3; 95% CI, 1.2-9.3; P = .02), and a positive SAP (OR = 5.6; 95% CI, 1.0-30.3; P = .05) were predictive of a change in management.
Impedance Measures, EGD, and Biopsy Results in Patients With Change in Management.
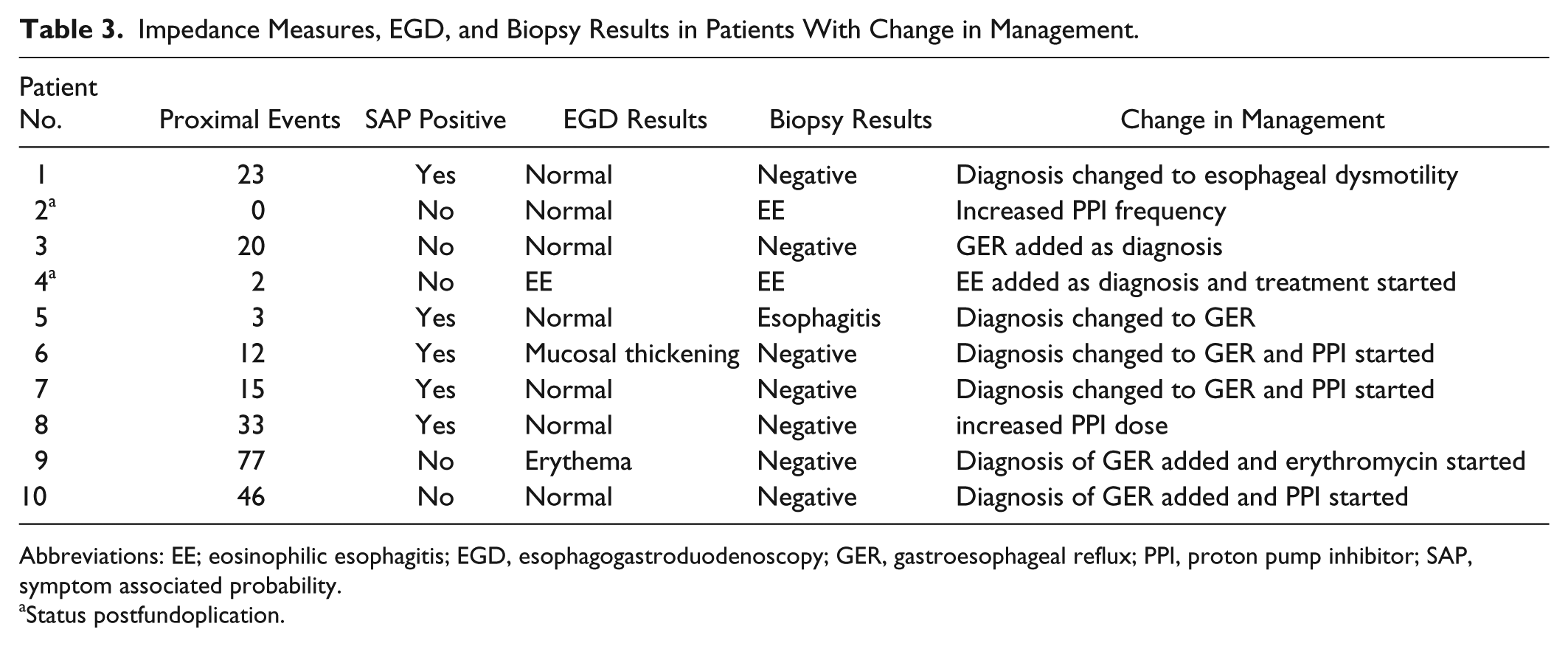
Abbreviations: EE; eosinophilic esophagitis; EGD, esophagogastroduodenoscopy; GER, gastroesophageal reflux; PPI, proton pump inhibitor; SAP, symptom associated probability.
Status postfundoplication.
Logistic Regression Results of Any Change in Management in Patients Without Nissen Fundoplication (N = 36).
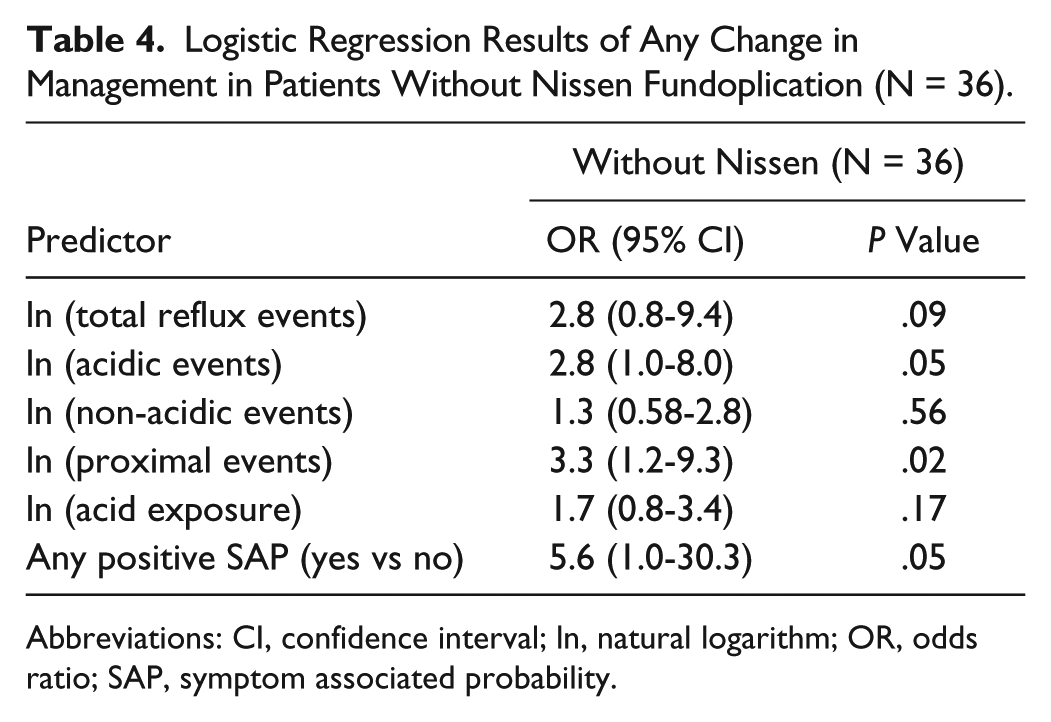
Abbreviations: CI, confidence interval; ln, natural logarithm; OR, odds ratio; SAP, symptom associated probability.
Overall, a successful surgical outcome occurred in 31 patients (54%). Odds ratios for impedance measures on surgical outcome for patients with fundoplication and patients without fundoplication are presented in Table 5. None of the measures considered were predictive of successful outcome in the patients with a fundoplication. For patients without a fundoplication, the absence of postoperative complication was the only factor predictive of successful outcome (OR = 9.6; 95% CI, 2.0-47.3; P = .005).
Logistic Regression Results of Successful Surgical Outcome by Nissen Fundoplication.
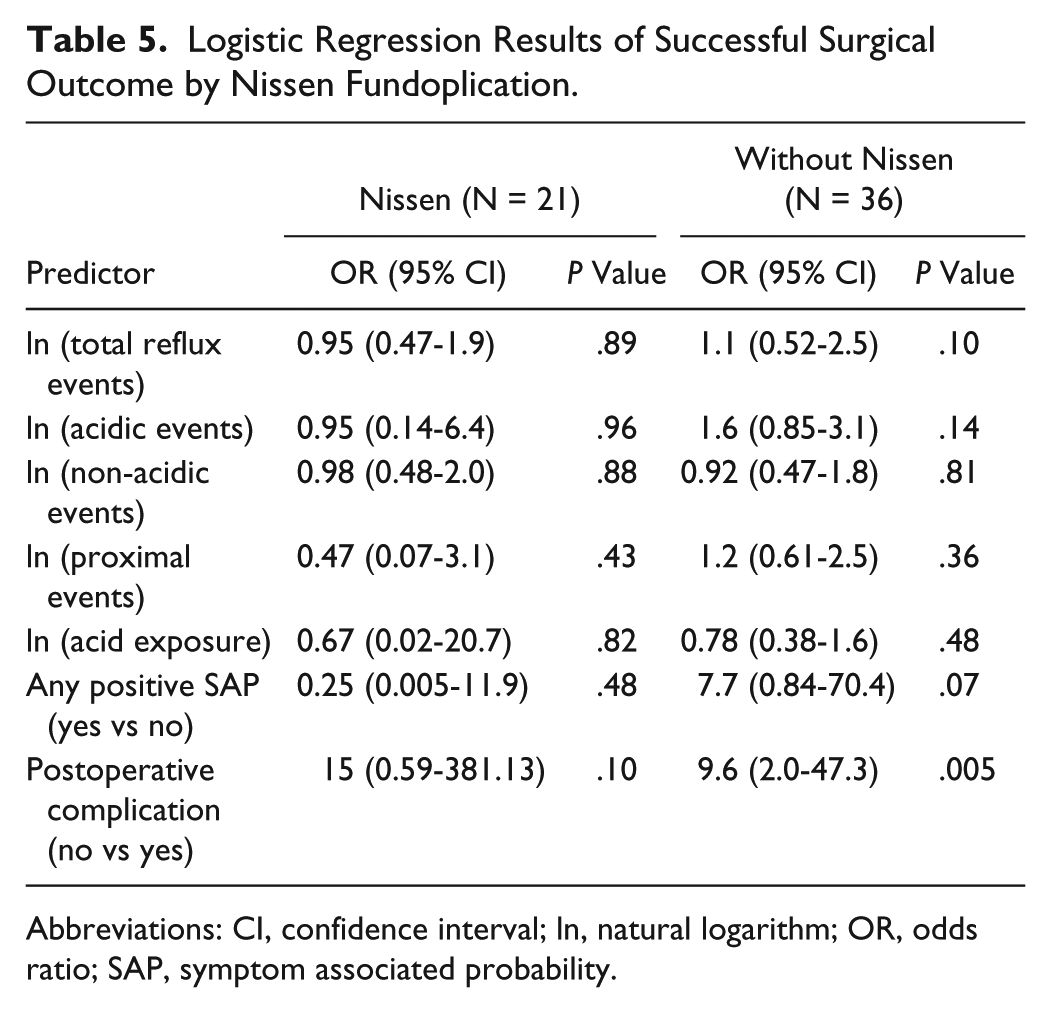
Abbreviations: CI, confidence interval; ln, natural logarithm; OR, odds ratio; SAP, symptom associated probability.
Testing using pH-MII allows for correlation between symptoms and reflux events. The most common symptoms present in the study population and the symptom correlation to all reflux and acid reflux events are listed in Table 6. Cough occurred in the majority of patients (n = 48, 84%). The highest symptom correlation occurred with regurgitation, with 5 patients (20%) having a positive SAP.
Most Common Symptoms.
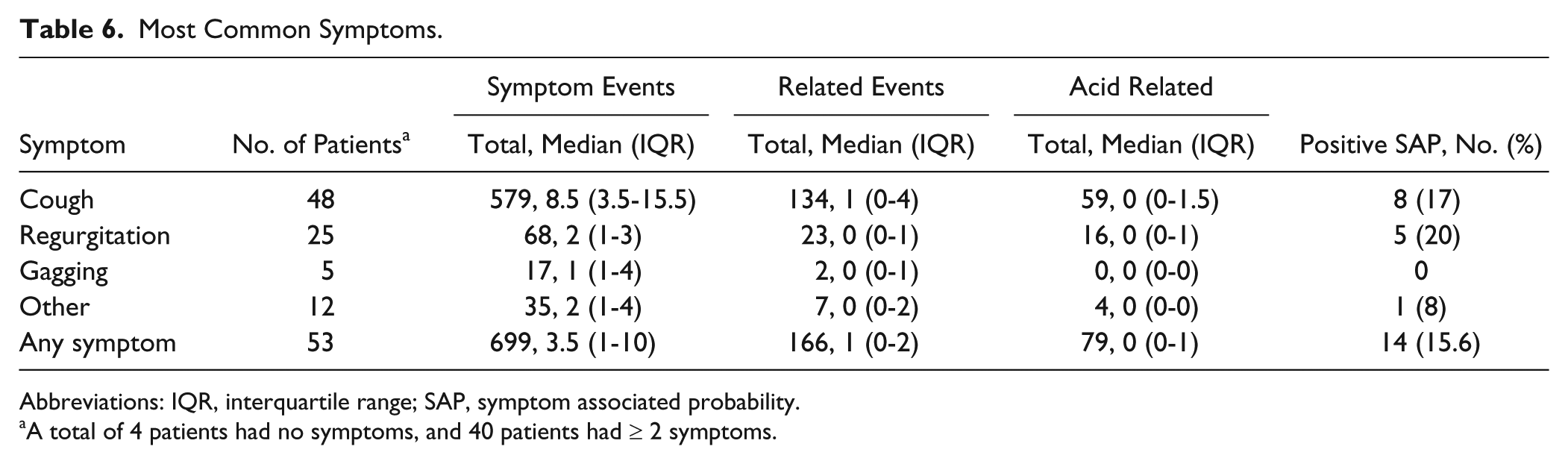
Abbreviations: IQR, interquartile range; SAP, symptom associated probability.
A total of 4 patients had no symptoms, and 40 patients had ≥ 2 symptoms.
Table 3 summarizes the number of proximal events, SAP, EGD results, biopsy results, and changes made for the 10 patients who had a change in management. Two of these patients had abnormalities identified on EGD with normal biopsy results. Two had abnormal biopsies with normal EGD findings and 1 patient had both an abnormal EGD and an abnormal biopsy.
Discussion
The link between GERD, subglottic stenosis, and failed airway reconstruction is well established in the literature.1-6,9 Preoperative optimization is considered critical to successful airway reconstruction.9,10 One element of this is appropriate diagnosis and management of GERD. To our knowledge, this is the first study to examine the role of preoperative pH-MII testing prior to open airway reconstruction.
In our study population, 21 patients (37%) had a history of fundoplication. When considering the results of pH-MII testing, it was logical to compare those patients with a fundoplication to those without. There was a notable difference in the number of reflux events between the patients who had a fundoplication and those who did not. The patients with fundoplication had a range of 0 to 2 proximal episodes, 1 to 16 total reflux episodes, and 0 to 2 acidic events compared to a range of 3 to 20 proximal events, 27 to 70 total reflux events, and 5.5 to 30 acidic events in those without fundoplication. These data suggest that fundoplication was effectively controlling reflux in these patients. Although not statistically significant, a higher percentage of patients without a fundoplication experienced a change in management (22% vs 9.5%, P = .22). It is not surprising that patients without a fundoplication had a higher percentage of reflux events as one would expect fewer reflux events in patients with a fundoplication. Given that the patients without fundoplication also had more acidic events, we were able to initiate therapy with a PPI or increase the dose or frequency in those patients already being treated. It is interesting that, in the unadjusted analysis, a smaller proportion of fundoplication patients had a successful surgical outcome (33% vs 67%, P = .01). Having undergone a fundoplication, these patients were already maximally treated for GERD, so surgical failures were likely not related to reflux and may indicate that these patients had more significant underlying comorbidities. This finding prompted additional analysis in an effort to identify potential confounders that might explain the higher failure rate in patients with fundoplication. In a multivariable analysis, we found that a history of prematurity, fundoplication, and prior airway surgery were all negatively associated with surgical success (Table 7). Although these findings are interesting, the small number of patients with surgical success (n = 31) creates difficulty when constructing a multivariate model including more than 3 variables. To more accurately examine the role of confounding in this patient population, additional study with a larger cohort would be necessary. Overall, pH-MII testing in patients with fundoplication appears to be low-yield.
Multivariable Model of Surgical Success (N = 57).
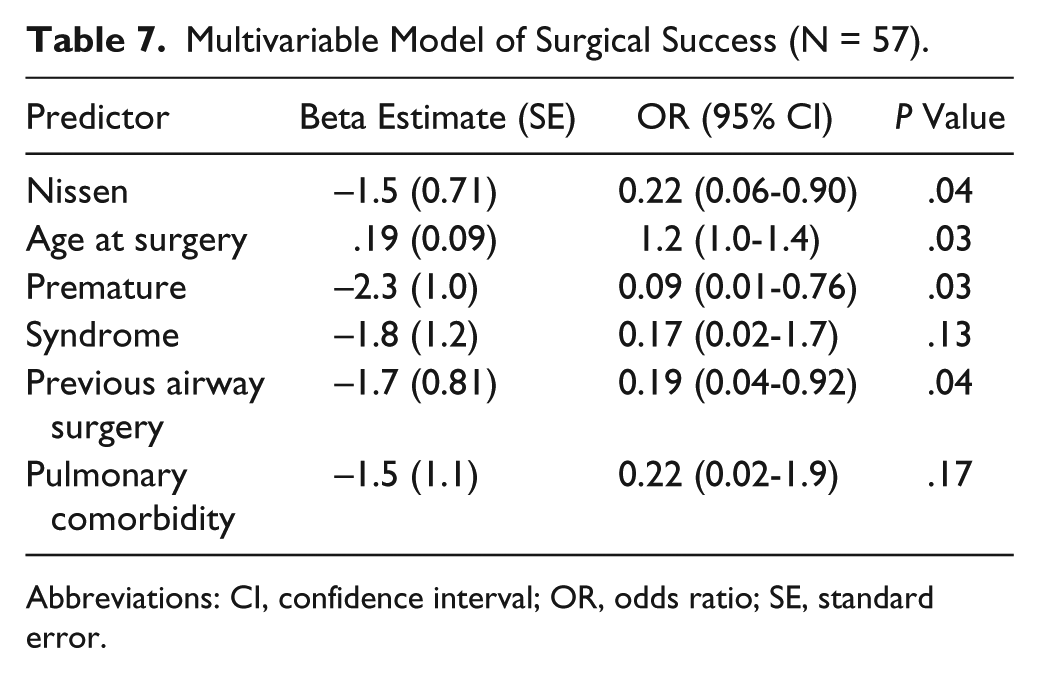
Abbreviations: CI, confidence interval; OR, odds ratio; SE, standard error.
In patients without fundoplication, we found that the increase of certain measures increased the probability of having a change in management. Patients with a 1-unit increase in the number of acidic events had 2.8 greater odds of a change in management (OR = 2.8; 95% CI, 1.0-8.0; P = .05). Likewise, patients had a 3.3 times greater odds of having a change in management for every 1-unit increase in the number of proximal events (OR = 3.3; 95% CI, 1.2-9.3; P = .02). Having a positive SAP increased the probability of having a change in management (OR = 5.6; 95% CI, 1.0-30.3; P = .05). These findings suggest that in patients without a fundoplication, impedance measures may be important factors in guiding management.
Given that changes in the number of non-acidic events alone did not predict a change in management or surgical outcome, one might question the benefit of pH-MII testing compared to standard pH monitoring. pH-Multichannel intraluminal impedance has several advantages. pH-Multichannel intraluminal impedance testing can be performed with patients who are on acid suppression medications at the time of testing. Slightly more than half of the patients in our study population (52%) were on anti-reflux medications at the time of their evaluation. pH-Multichannel intraluminal impedance testing is able to quantify the extent of proximal reflux, which is more likely to be detrimental to surgical outcome. It is also able to detect repeated reflux events that occur without a return to the baseline pH between reflux events. These repeat events would be missed by standard pH monitoring, which may lead to underestimation of the extent of reflux.
Regression analysis of successful surgical outcome by fundoplication demonstrated that surgical failures in the fundoplication group were independent of GERD and also independent of postoperative complications (Table 5). In patients without a fundoplication, having a positive SAP appears to be potentially protective, although the OR did not quite reach statistical significance (OR = 7.7; 95% CI, 0.84-70.4; P = .07). This could indicate that patients who cough with reflux events are able to protect their airways more effectively than those who do not cough during reflux events.
Overall, 17.5% of the patients in our study experienced a change in management based on the results of preoperative gastrointestinal (GI) evaluation including pH-MII and EGD with biopsies, which is a smaller number than we anticipated. However, this is similar to the findings of a recent study that showed that the addition of MII to pH probe testing changed clinical management in 22% of patients. 11 As seen in Table 3, both pH-MII results as well as EGD findings and biopsy results played a role in determining changes in management. Previous studies support the utility of esophageal biopsies to aid in diagnosis of GERD.12,13 In 3 of the 10 patients who had a change in management, the esophageal biopsies were positive despite having minimal to no proximal events. Although our numbers are small, they suggest a role for both EGD with biopsy and pH-MII in the preoperative evaluation.
The lack of correlation between symptoms and reflux events (Table 6) suggests that symptoms alone are not a good indicator of the need for pH-MII testing. This confirms recent studies that demonstrated that non-acidic events were as likely as acidic events to cause symptoms, and in infants, most extraesophageal symptoms were not temporally associated with a reflux event.14,15 This suggests that the lack of symptoms should not preclude pH-MII testing.
Our study was subject to the inherent limitations of a retrospective study. Only 38% of the patients undergoing airway reconstruction during the study period underwent pH-MII testing, and there was no set protocol to determine which patients would undergo testing. This fact certainly introduces bias as these patients likely represent the most complex patients presenting for airway reconstruction. In addition, our sample size is small, which hampers the statistical analysis. Additional study would be useful to further elucidate which patients would benefit most from preoperative pH-MII testing and to determine the role of pH-MII testing in less complex airway reconstruction candidates. Likewise, further study would be helpful to better define the risk factors for surgical failure in fundoplication patients.
Conclusion
We found that fewer patients than anticipated had a change in management based on preoperative GI evaluation. Gastrointestinal evaluation did, however, result in a change in therapy for 17.5% of patients. In addition, our results suggest that performing pH-MII testing on patients with a history of a fundoplication was unlikely to change management. Patients with a history of fundoplication were less likely to have a successful surgical outcome, suggesting that factors other than gastroesophageal reflux also influence the success of airway reconstruction. Further study is warranted to examine the reasons for surgical failure in patients with fundoplication as well as to better define the role of pH-MII testing in children undergoing airway reconstruction.
Footnotes
Authors’ Note
This article was presented as a podium presentation at the American Broncho-Esophagological Association Combined Otolaryngology Spring Meetings in Orlando, Florida, on April 10, 2013.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was supported in part by an Institutional Clinical and Translational Science Award, NIH/NCRR Grant No. 5UL1RR026314-3. Its contents are solely the responsibility of the authors and do not necessarily represent the official views of the National Institutes of Health.