
Abstract
Objective:
The aim of this study was to compare genetic predilection and recurrence tendency between facial palsy in Melkersson-Rosenthal syndrome (MRS) and Bell’s palsy
Methods:
We carried out an investigation on patients with facial palsy in MRS and those with Bell’s palsy who visited the outpatient department in our hospital between February 2009 and February 2013. They were asked about familial history and whether it was the first episode, with the results recorded and compared.
Results:
There were 16 patients with facial palsy in MRS and 860 patients with Bell’s palsy involved in the study. Familial history was positive in 5 of 16 patients (31.3%) with facial palsy in MRS and 56 of 860 patients (6.5%) with Bell’s palsy (P < .01). Twelve of 16 cases (75%) with facial palsy in MRS and 88 of 860 cases (10.2%) with Bell’s palsy had a history of facial palsy in the past (P < .01).
Conclusion:
Compared to Bell’s palsy, facial palsy in MRS has an obvious genetic predilection and recurrence tendency.
Introduction
Melkersson-Rosenthal syndrome (MRS) is characterized by a triad of recurrent orofacial edema, recurrent peripheral facial palsy, and lingua plicata. 1 The complete form, which contains all 3 symptoms, is less common, and the incomplete form, which has only 2 of the symptoms, is more common.2,3 It has sexual predilection and occurs more often in females.4,5
Facial palsy is common in MRS patients.4,6 It seems that facial palsy in MRS has more hereditary predilection and recurrence tendency compared to Bell’s palsy. According to the previous reports,6,7 familial history is positive in 29.4% of the patients (5 of 17 cases who responded to the questionnaire) who had MRS with facial palsy, whereas it is positive in only 4% of the patients with Bell’s palsy. Seventy-five percent of the patients with facial palsy in MRS have a history of facial palsy episodes, 6 whereas only 8.2% of the patients with Bell’s palsy have recurrent facial palsy. 8 However, the data are from different reports, which could not provide a convincing conclusion. Thus, we designed a prospective study that aimed to compare genetic predilection and recurrence tendency of facial palsy in MRS and Bell’s palsy.
Materials and Methods
A prospective investigation was carried out on a consecutive series of patients who had facial palsy in MRS and Bell’s palsy between February 2009 and February 2013 in the outpatient department of otolaryngology. The diagnosis of MRS was made according to the patients’ history and clinical features as well as histopathologic features, where applicable. Bell’s palsy was idiopathic peripheral facial palsy, which was excluded from facial nerve tumors, otitis media, and acoustic neuromas by high-resolution computed tomography of temporal bone and magnetic resonance imaging examination and was identified from Ramsay Hunt syndrome by clinical symptoms.
The patients were asked about whether their first-order or second-order relatives had a history of facial palsy and who had a history of facial palsy. The familial history was confirmed directly by phone contact with the positive relatives. Whether it was the first episode was also inquired about. The percentages of familial history and recurrent facial palsy between facial palsy in MRS and Bell’s palsy were compared by χ2 test, respectively.
Results
A total of 16 patients who had facial palsy in MRS and 860 patients with Bell’s palsy were included in the study. Among MRS patients, there were 5 cases of complete form and 11 of incomplete form. Eleven patients were female and 5 male, with a mean (SD) age of 21.0 (11.9) years. For Bell’s palsy, there were 460 female and 400 male patients, with a mean (SD) age of 39.0 (17.2) years.
Five of 16 patients (31.3%) with MRS reported a history of facial palsy among their first-order or second-order relatives in contrast with 56 of 860 patients (6.5%) with Bell’s palsy (P < .01) (Table 1). Facial palsy was at least the second episode in 12 of 16 cases (75%) with MRS compared to 88 of 860 cases (10.2%) with Bell’s palsy (P < .01) (Table 2). Eight of 12 patients (66.7%) who had recurrent facial palsy in MRS were of homolateral type, and 4 of alternating type. In contrast, 57 of 88 cases (64.8%) with recurrent Bell’s palsy were of homolateral type and 31 of alternating type.
History of Facial Palsy in Melkersson-Rosenthal Syndrome (MRS) and Bell’s Palsy in First-Order and Second-Order Relatives. a
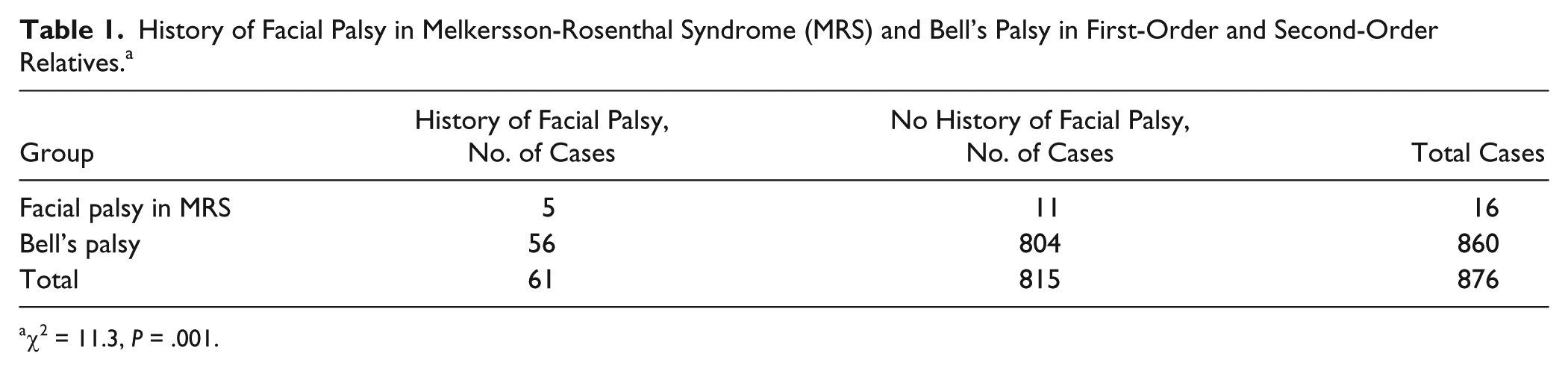
χ2 = 11.3, P = .001.
Recurrent Facial Palsy in Melkersson-Rosenthal Syndrome (MRS) and Bell’s Palsy. a
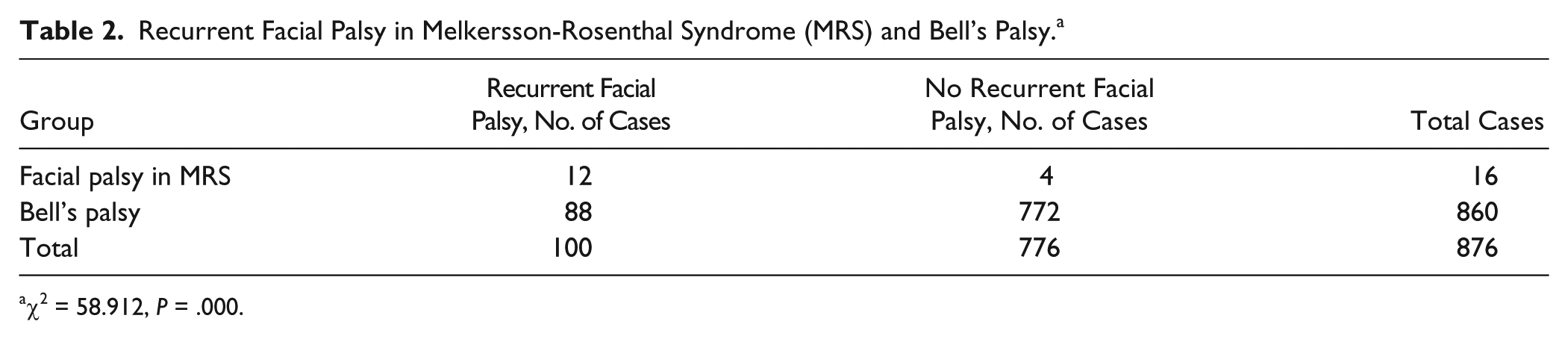
χ2 = 58.912, P = .000.
Discussion
The etiology of MRS is still unknown. Viral infection, allergic factor, or hereditary origin has never been proposed, but there is no convincing evidence available.9-11 Some authors6,12 think that facial palsy in MRS resembles Bell’s palsy, in which viral infection may be the possible etiological factors. But there is no evidence of viral infection in MRS, and furthermore, no viral particles are observed in Bell’s palsy. 13
We notice that familial history is predominant for facial palsy in MRS, whereas it is much less common for Bell’s palsy. In our study, 31.3% of the patients with MRS have a familial history of facial palsy among their first-order or second-order relatives, but only 6.5% of the patients with Bell’s palsy report familial history (P < .01), indicating that a genetic factor is strongly suggested in the etiology of facial palsy in MRS compared to Bell’s palsy. Further investigation into the related genes may cause a breakthrough in revealing the etiology of facial palsy in MRS.
Moreover, familial facial palsy in MRS probably has an alternate inheritance mode from familial Bell’s palsy. The proposed mode of inheritance in familial Bell’s palsy is autosomal dominant inheritance with variable penetrance.7,14-16 However, for typical cases 4, 6, and 8 in Table 3, which combines our cases and the data of Kanerva et al, 5 their brother or sister has facial palsy whereas their parents report no history of facial palsy, suggesting recessive inheritance. There is no sexual predominance among all the patients with facial palsy in Table 3, supporting autosomal inheritance. Genealogic analysis of the data in Table 3 suggests that facial palsy in MRS probably has autosomal recessive inheritance.
Hereditary History of 9 Patients With Facial Palsy in Melkersson-Rosenthal Syndrome (MRS) From Our Study and Kanerva et al Report. a
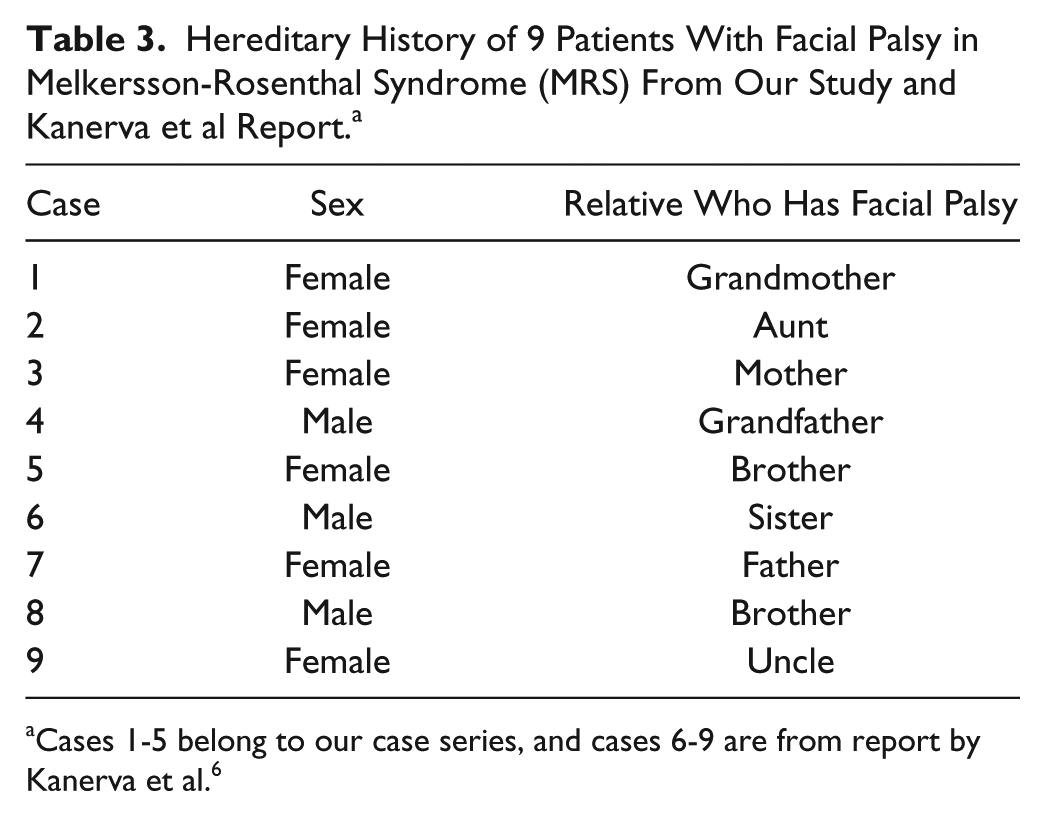
Cases 1-5 belong to our case series, and cases 6-9 are from report by Kanerva et al. 6
Another point of note is that facial palsy in MRS is usually recurrent, whereas Bell’s palsy is rarely recurrent. In the current series, 75% of the patients with facial palsy in MRS had at least a second episode of facial palsy, whereas only 10.2% of the patients with Bell’s palsy had more than 1 episode (P < .01), suggesting that recurrence tendency is dramatically predominant in facial palsy in MRS in contrast to Bell’s palsy. Moreover, further attacks of facial palsy in MRS tend to occur along with orofacial edema rather than by themselves, 17 whereas they are absent in Bell’s palsy.
Facial palsy in MRS and Bell’s palsy may have alternate inflammatory sites. Fisch and Esslen 18 found that the edematous sites of facial nerve were proximal to geniculate ganglion in Bell’s palsy during total facial nerve decompression, consistent with their results of intraoperative electrical stimulation, demonstrating that inflammatory sites of Bell’s palsy were probably located proximally to geniculate ganglion. However, Dai et al 19 decompressed the mastoid segment, tympanic segment, geniculate ganglion, and labyrinthine of the facial nerve in 8 patients who had recurrent facial palsy in MRS and found that the facial nerve was edematous at the mastoid segment in all cases, at the tympanic segment and geniculate ganglion in most cases, and at the labyrinthine segment in only 1 case, suggesting that the geniculate ganglion and its distal segments of the facial nerve were probably the main inflammatory sites of the facial nerve in MRS.
To our knowledge, our study is the first to compare genetic predilection and recurrence tendency between facial palsy in MRS and Bell’s palsy and reveals that facial palsy in MRS is predominant in genetic predilection and recurrence tendency. Furthermore, inflammatory sites of facial palsy in MRS and Bell’s palsy may be different. We hence propose that facial palsy in MRS is not Bell’s palsy and may have its unique clinical and pathogenic features.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. The author(s) alone are responsible for the content and writing of the article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.