
Abstract
Objective:
This study aimed to examine the authors’ experience with endoscopic management of idiopathic subglottic stenosis (iSGS), and to identify pulmonary function test (PFT) values that can be used to quantify outcomes.
Methods:
Retrospective review.
Results:
Twenty-five patients with a new diagnosis of iSGS were seen between 2006 and 2012. Median age at surgery was 45.3 years (interquartile range [IQR], 38.5-67.0), and median body mass index was 28.7 kg/m2 (IQR, 23.5-32.1). Forty-five procedures were performed. Median preoperative stenosis was 56.8% (Cotton-Myer grade 2). The typical stenosis began 15 mm below the true vocal folds and was 12 mm long. Median follow-up was 21.4 months (IQR, 5.1-43.1). For patients receiving multiple dilations, median time between procedures was 23.7 months. Four PFT parameters demonstrated significant improvement after intervention: (1) PEF (absolute change = 2.54 L/s), (2) PIF (absolute change = 1.57 L/s), (3) FEV1/PEF (absolute change = 0.44), and (4) FIF50% (absolute change = 1.71 L/s). PIF was the only parameter affected by using a larger balloon (P = .047).
Conclusion:
PEF, PIF, FEV1/PEF, and FIF50% improved significantly after endoscopic incision and dilation of iSGS, and this could potentially be used as a metric by which to evaluate outcomes in the endoscopic management of subglottic stenosis.
Introduction
Etiology/Pathophysiology
Idiopathic subglottic stenosis (iSGS) is a nonspecific fibroinflammatory process that results in progressive narrowing of the airway at the level of the cricoid and proximal trachea. Investigators have proposed a multitude of theories as to the etiology of the process since its first description in 1972. 1 The disorder occurs almost exclusively in women, typically presenting in the fourth or fifth decade. 2 This female preponderance led to the hypothesis that estrogen might play a role in the pathogenesis of iSGS, although the evidence for this has not borne out.3,4
Current theories regarding the etiology of iSGS have focused on non-gender-specific causes. Subglottic injury from laryngopharyngeal reflux (LPR) has been implicated as a possible cause. 5 Autoimmune disease, specifically a limited form of seronegative polyangiitis with granulomatosis (GPA), has also been proposed as a mechanism for iSGS. 6 Other theories on the etiology of the disorder include repetitive microtrauma from cough 7 and hereditary factors. 8 Ultimately a disease of the subglottic lamina propria, no single etiologic factor has been identified.
Endoscopic Management of iSGS
Although segmental resection of the diseased portion of the airway is considered the gold standard for obtaining long-term improvement in the airway in iSGS, it is a potentially morbid procedure. 9 Endoscopic surgery provides an attractive alternative that is less invasive, albeit less definitive. As surgeon experience has grown, several variations in technique have been explored. Dedo and Catten 3 described a microflap technique in which a CO2 laser was used to make a mucosal flap followed by resection or ablation of the aberrant soft tissue between the flap and the cricoid. Shapshay et al 10 reported on the use of radial incisions with a CO2 laser, followed by dilation with a rigid bronchoscope. Some surgeons favor a cold technique over the laser for making radial incisions. 11 Balloon dilation was introduced in the management of subglottic stenosis as a theoretically less traumatic alternative to passing rigid dilators. 12
In addition to the different surgical techniques, there have been several investigations evaluating wound-healing modulators as adjunctive therapies. Most notable, inhaled, systemic, and locally injected steroids have been used extensively in an attempt to slow restenosis after dilation. 13 Mitomycin C, an alkylating agent, has been proven to prevent fibroblast proliferation 14 and has been used with varying degrees of success in endoscopic airway surgery. 15 Halofuginone, an inhibitor of collagen 1-α synthesis, 16 and 5-fluorouracil, an antimetabolite that inhibits fibroblast activity, 17 are also being investigated in animal models as potential adjunctive therapies.
Given the variety of options in the endoscopic management of iSGS, it has become obvious that an objective means by which to quantify operative outcomes and to compare the efficacy of different techniques or adjunctive therapies is sorely needed.
Assessing Outcomes in the Endoscopic Management of Subglottic Stenosis
In the late 1960s and early 1970s, there was a great deal of interest in using pulmonary function tests (PFTs) to aid in the diagnosis of upper airway obstruction (UAO). Initial investigations focused on identifying values that could differentiate UAO from lower airway disease.18,19 It was ultimately Hyatt’s 20 description of the flow-volume loop and the different patterns of obstruction (variable intrathoracic, variable extrathoracic, and fixed) that provided clinicians with a powerful tool for diagnosing and classifying UAO. There has been a renewed interest in the past 2 decades in using PFT data not only as a diagnostic tool but also as a means of quantifying the results of interventions in UAO.21,22
This retrospective study is designed to review our experience with using pulmonary function data in the management of patients with iSGS. Specifically, we aim to (1) describe our experience with iSGS, (2) identify which PFT parameters change following endoscopic intervention, (3) quantify the degree of improvement in airflow postoperatively using PFT data, and (4) determine if PFTs change in a predictable manner postoperatively as restenosis invariably occurs.
Methods
Inclusion/Exclusion Criteria
This study was approved by the institutional review board at Oregon Health and Science University. A retrospective chart review was performed, examining a single surgeon’s experience with iSGS. Records for all newly diagnosed adult patients with iSGS referred to the senior author between January 1, 2006, and December 31, 2012, were reviewed. At least 1 standard endoscopic intervention (described below) and 1 pulmonary function test was required for inclusion in the study. Patients with a history of previous airway surgery, airway trauma, tracheotomy, positive serology (c-ANCA or ACE level), or intubation within the previous 12 months were excluded from the analysis.
Management of Stenosis
All patients included in the study were managed endoscopically in a standardized fashion. After confirming that the patient could be mask ventilated, anesthesia was induced and maintained using a total intravenous technique. A plastic tooth guard was used to protect the maxillary dentition. The airway was exposed using an Osshoff-Pilling laryngoscope, and the patient was suspended from the Mustard table. Ventilation was conducted via jet technique. Standard laser precautions were used throughout the procedure, to include placing moist gauze pads over the eyes and wet towels over any exposed skin.
A 4-mm rod lens telescope was used to evaluate and measure the stenosis. If the initial values were obtained by the resident or fellow, the senior author (J.S.) repeated and confirmed the measurements. The stenosis was described by its distance below the true vocal folds and by its total length. Once measurements were complete, 2-mm cup forceps were used to take a biopsy. The stenosis subsequently was infiltrated with 1 mL of triamcinolone suspension (40 mg/mL). A CO2 laser was then used to make 3 to 5 radial incisions in the stenosis. Dilation of the stenosis was performed using a constant radial expansion (CRE) balloon. After confirming hemostasis and obtaining postoperative photo documentation, a small, cuffed endotracheal tube (5.0) was placed through the laryngoscope. The patient was taken out of suspension and the laryngoscope removed. The patient was then remanded to the care of the anesthesia team for recovery. Patients were discharged home from the postanesthesia care unit that same day with a fluticasone inhaler (220 mcg) and instructed to use 2 puffs twice daily until the inhaler was empty.
Data Collection and Statistical Analysis
After obtaining approval from the institutional review board, the senior surgeon’s operative record was reviewed to identify patients with a preoperative diagnosis of subglottic stenosis. Clinical records were then further screened to select patients who met the inclusion criteria. All data points, to include demographic, clinical, operative, laboratory, radiographic, and pulmonary functional data, were entered in a Microsoft Excel spreadsheet. Data were imported into and analyzed via SPSS version 20.0 (SPSS Inc, Chicago, Illinois, USA). A P value < .05 was considered to be significant.
As we could not assume a normal distribution for our small sample size, a Wilcoxon signed rank test was used to look for differences in the pre-dilation and post-dilation differences in pulmonary function data. Subsequently, a Kruskal-Wallis test was performed on those PFT parameters that improved significantly to determine the contribution of dilation size on the change. For those measures that changed significantly, postoperative PFT values were plotted as a function of time to assess the rate of change after intervention.
Results
Clinical Presentation and Evaluation of Stenosis
A total of 25 new patients with iSGS were seen between 2006 and 2011 at our clinic. As anticipated, all patients were female. Ninety-two percent (N = 23) were white and 8% (n = 2) Hispanic. The median age at the time of the first surgical intervention was 45.3 years (interquartile range [IQR], 38.5-67.0), with a median body mass index of 28.7 kg/m2 (IQR, 23.5-32.1) (Table 1).
Clinical Presentation.
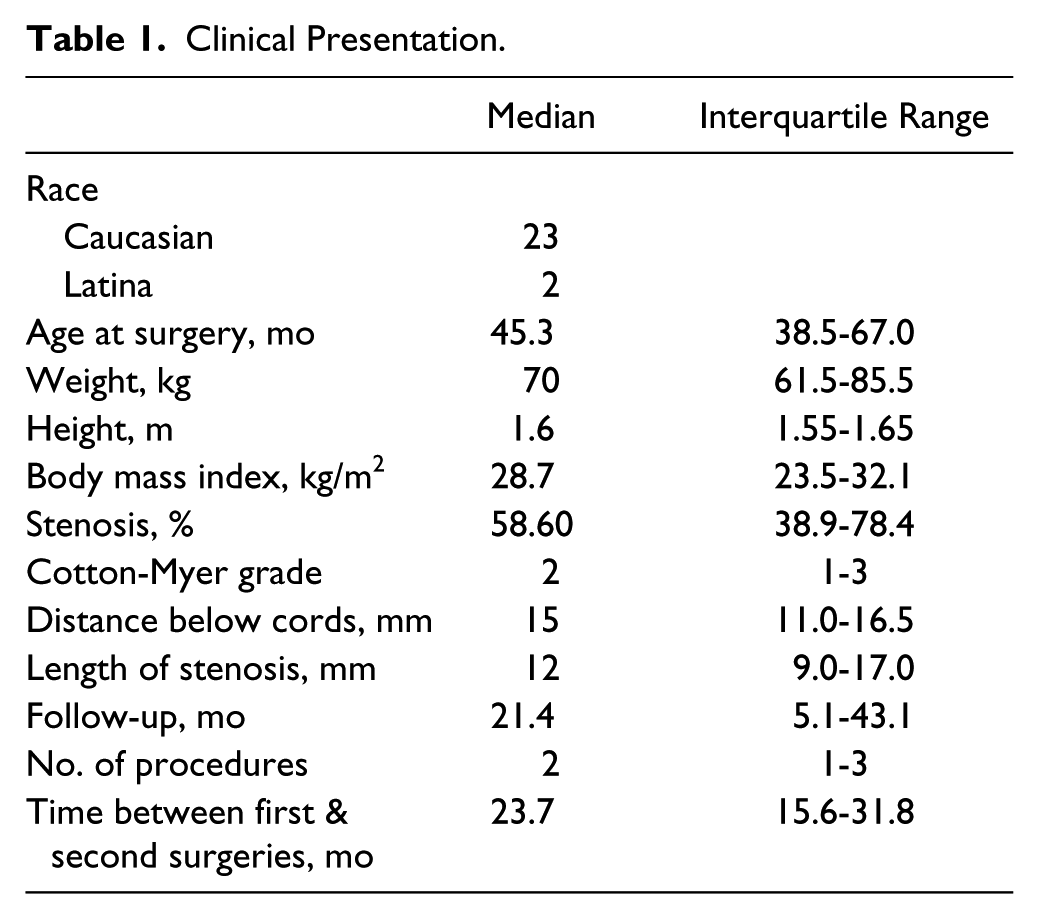
A total of 45 procedures were performed. Twelve patients had 1 procedure, 9 patients had 2 procedures, 2 patients had 3 procedures, 1 patient had 4 procedures, and 1 patient had a total of 7 procedures (median = 2). At the time of initial presentation, the typical stenosis was described as beginning 15 mm below the true vocal folds and measuring 12 mm long. Fifteen patients had preoperative computed tomography (CT) scans. The median degree of stenosis as determined by CT was 56.8% (Cotton-Myer grade 2). Four patients had grade 1 stenosis at presentation and 4 patients had grade 3 stenosis.
Median follow-up after surgery was 21.4 months (IQR, 5.1-43.1). For the 11 patients receiving at least 2 dilations, the median time between the first and second procedures was 23.7 months. Three patients ultimately proceeded to definitive cricotracheal resection.
Preoperative Versus Postoperative PFT Assessment
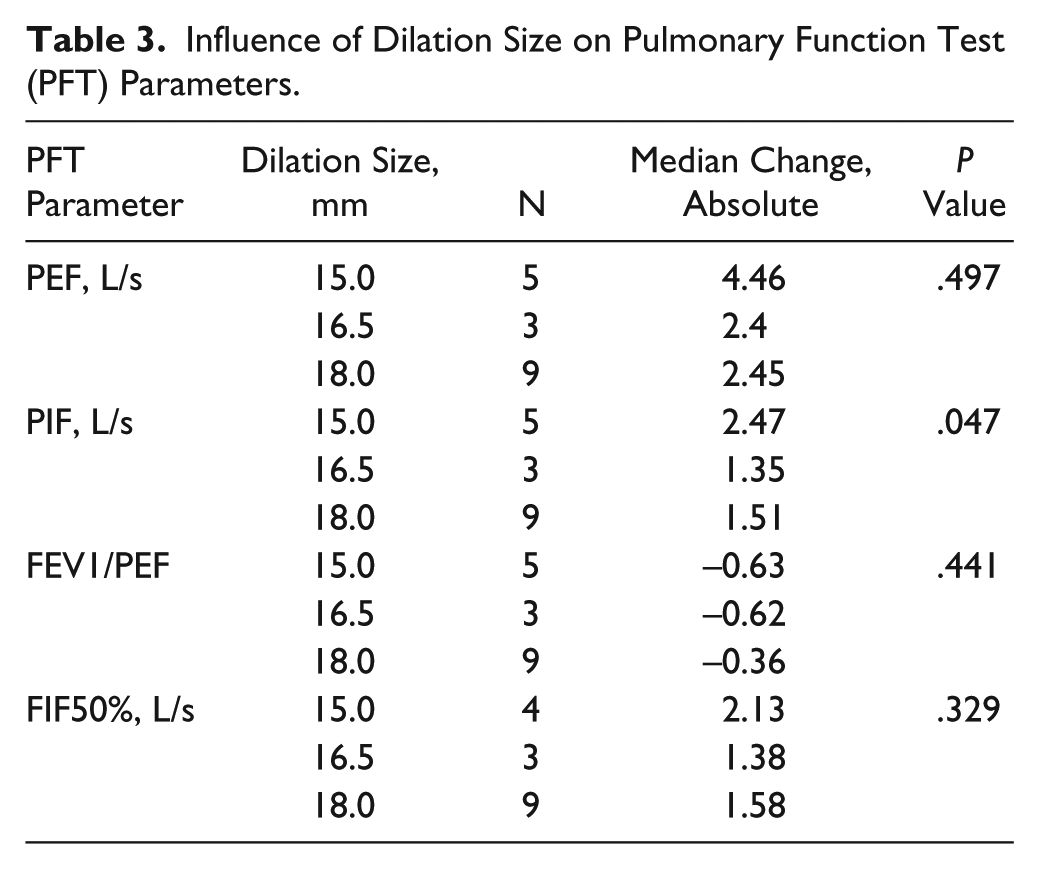
Seventeen of the 25 patients had a preoperative PFT in addition to at least 1 postoperative PFT performed within 8 weeks of surgery. Four parameters demonstrated a statistically significant improvement after intervention: (1) PEF (absolute change = 2.54 L/s), (2) PIF (absolute change = 1.57 L/s), (3) FEV1/PEF (absolute change = 0.44), and (4) FIF50% (absolute change = 1.71 L/s). FEV1, FVC, FEF25%-75%, and PEF/PIF did not change significantly (Table 2). Preoperative and postoperative PFT values were then examined in the context of balloon size. Improvement in the PIF was the only parameter that was affected by the size of dilation, with rank-order testing indicating a greater degree of improvement with use of a larger balloon (P = .047) (Table 3).
Comparison of Pre-dilation and Post-dilation Pulmonary Function Data.
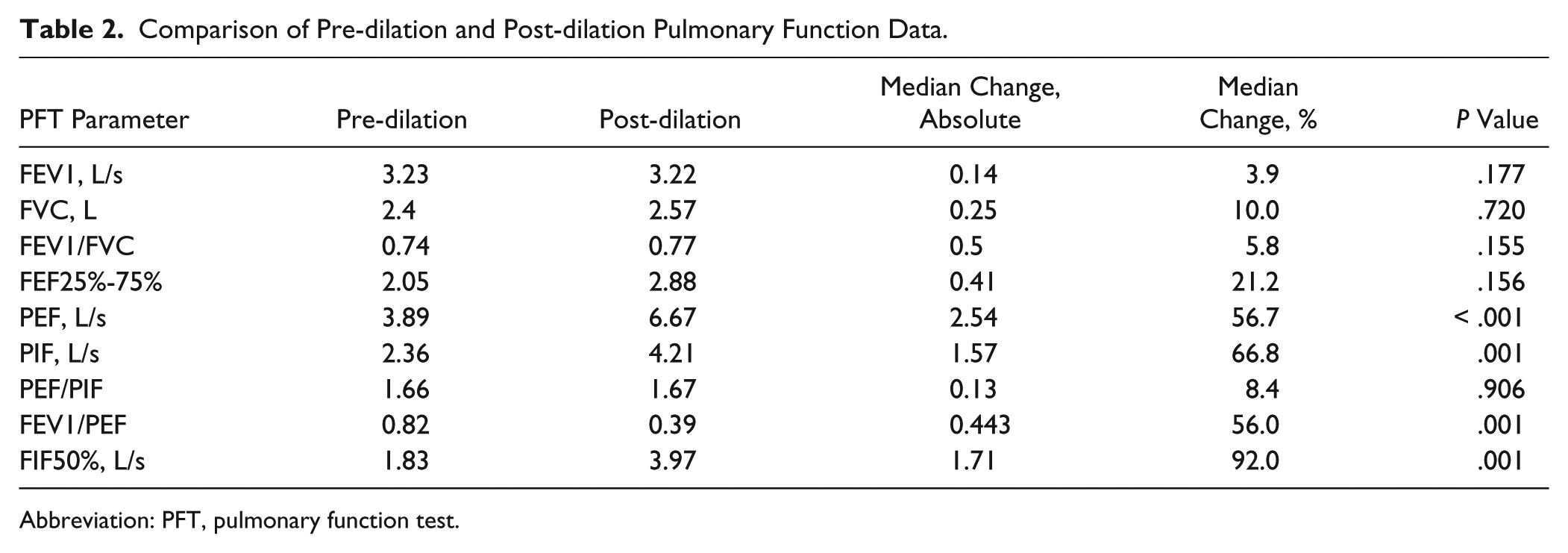
Abbreviation: PFT, pulmonary function test.
Influence of Dilation Size on Pulmonary Function Test (PFT) Parameters.
Changes in PFT Over Time
Seven patients of the 25 in this sample had at least 3 PFTs taken following the initial dilation. PEF, PIF, FEV1/PEF, and FIF50% from these samples were plotted as a function of time. There is a linear relationship between time and both PEF and FEV1/PEF (P = .0307 and P < .001, respectively). The slope of the line was unique to each patient (Figures 1 and 2). PIF and FIF50% generally decrease as the time from surgery increases, but a linear relationship could not be established (data not shown). Five of the 7 patients did have a second procedure but had not accumulated a sufficient number of subsequent PFTs during the study period for analysis. (The patients represented by a star and hexagon had only 1 procedure.)
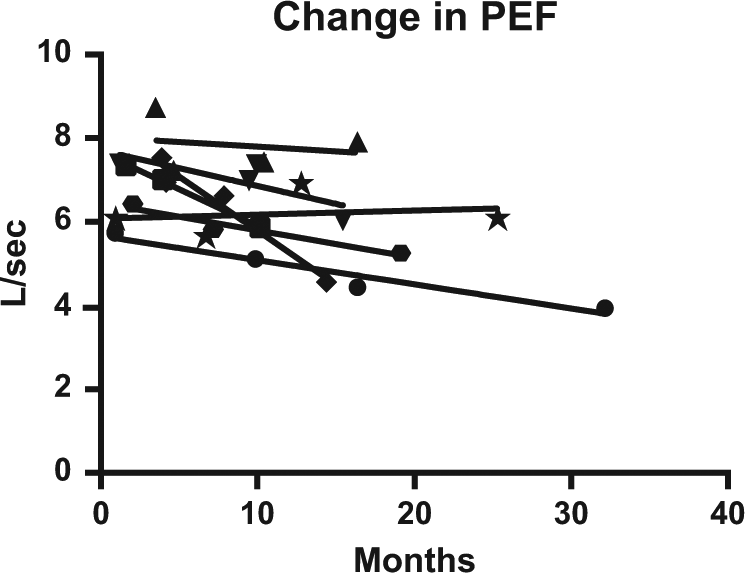
Change in PEF postoperatively. PEF declines in a linear fashion after intervention. The slope of the line is unique to each patient (P = .0307).
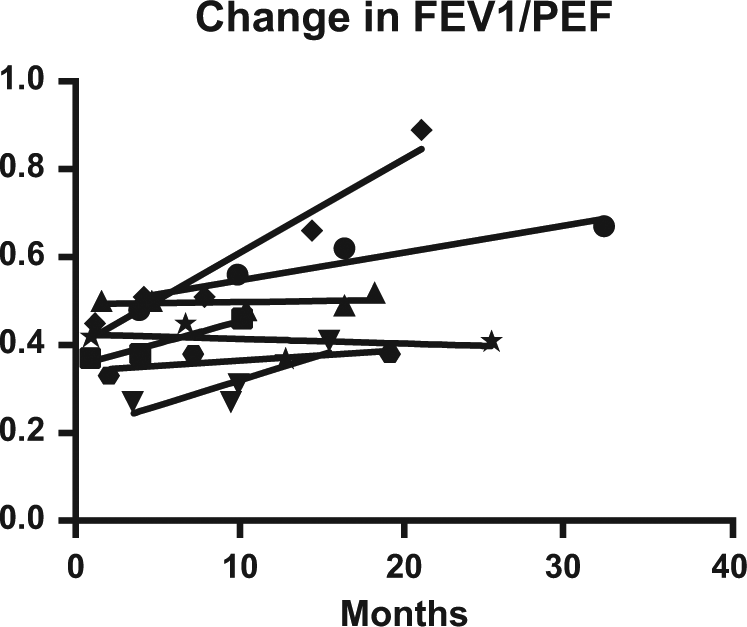
Change in FEV1/PEF postoperatively. FEV1/PEF similarly changes in a unique linear fashion after intervention (P < .0001).
Discussion
Not all patients are ideal candidates for endoscopic management of subglottic stenosis. Historically, previous failed dilations, stenosis length greater than 1 cm, circumferential stenosis, evidence of cartilage loss/damage, a history of severe bacterial infection with tracheotomy, posterior glottic stenosis with arytenoid fixation, and involvement of the inferior margin of the vocal folds were considered poor prognostic indicators. 23 Patients with isolated subglottic disease, however, can successfully be managed endoscopically in approximately 87% of cases. 24 The expectation is that more than 85% of these patients will have recurrence of their stenosis within 5 years, requiring a return to the operating suite. 25
Clinically, the goal is to identify the techniques and adjuvant therapies that provide the greatest improvement in airflow and result in the slowest rate of restenosis. Not surprising, time between surgeries is a commonly reported metric used to demonstrate the efficacy of an intervention.26,27 Although clinically relevant, confounding variables related to the surgical interval raise questions about its reliability for use in research. Surgeon availability certainly affects the time between procedures. Physically active patients are more likely to notice impairment of airflow than sedentary patients and may seek intervention sooner. Financial factors may affect a patient’s decision to seek surgery, as well. It is clear that an objective measure is needed.
Using PFT data to evaluate airway stenosis is not a new concept. In the 1970s, a number of studies tried to identify which values or ratio of values could be used to diagnose UAO. Empey 18 reported on a series of 10 patients (most with bilateral vocal cord paralysis), noting that the FEV1/PEF ratio was greater than 10 in all cases and that the larger the ratio, the greater the degree of obstruction. In comparing UAO with chronic obstructive pulmonary disease, Rotman et al 19 identified 4 measurements that were found to differentiate upper from lower airway disease: (1) FEF50%/FIF50% > 1, (2) FEV1/PEFR > 10, (3) FIF50% < 100 L/min, and (4) FEV1/FEV0.5 > 1.5, with the latter 2 measures being less sensitive.
Pulmonary function tests have been used in a limited fashion to assess postoperative outcomes following tracheal resection 28 and endoscopic dilation, 29 but reports have been generally nonspecific about the degree of improvement and which measures are of greatest utility in quantifying results. To examine this issue, Wasserman et al 21 created a model of fixed obstruction using mouthpieces of decreasing inner diameters (15, 10, 8, and 6 mm) in line with a spirometer. PEF and PIF were found to be the most sensitive measures by which to assess changes in airway resistance. Nouraei et al 22 performed a similar experiment in 2007 in which the resistors were designed to generate a greater resistance to inspiratory flow than expiratory flow. The MEF50/MIF50 and the ratio of the areas under the expiratory/inspiratory curves were the most sensitive and specific parameters.
Both the location of a stenosis and its characteristics (length, radius, boundary conditions) affect airflow, making every stenosis unique. In this study, we elected to specifically look at iSGS as a model of fixed obstruction. We chose to exclude glottic and tracheal stenosis from our analysis, both of which have some component of variability due to the contribution of Bernoulli forces and compression of membranous tracheal wall, respectively. Not surprising, we found that the PFT values that changed after intervention were the same as those reported by Wasserman et al. We suspect that an examination of PFT values affected by intervention for glottic or tracheal stenosis would yield results more closely resembling those recently reported by Nouraei and colleagues for a variable obstructive model.
In our evaluation, we examined the effect of radial incision and dilation on PFT values. Pulmonary function tests are an attractive means of evaluating stenosis patients because the study is inexpensive; widely available; and, unlike current techniques using CT for computational fluid dynamic studies, avoids the need for ionizing radiation. Whereas CT examines the structural component of stenosis, PFTs are a physiologic measure of the effect of stenosis on airflow and the patient’s actual respiratory function. There are limitations to the PFT, the primary issue being that the study is dependent on patient effort. In addition, not all studies are conducted uniformly. Spirometry software is programmed to select the loop with the best expiratory effort for evaluation. Previous studies have demonstrated that the number reported by the computer for PIF and FIF50% did not represent the largest value in 50% and 69% of cases, respectively.30,31 It is necessary to look at all loops or to establish a protocol for maximal inspiratory effort to mitigate this. Finally, some data suggest that the test may not be adequately sensitive for mild stenosis. Miller and Hyatt 32 reported that the trachea would have to be narrowed to 8 mm (~ 80%) prior to creating detectable changes in flow.
The retrospective nature of this study is an inherent limitation. As this is a single surgeon experience, the surgical technique was fairly consistent between patients. However, there was some variability in selecting the initial dilation size. The radius of the fluid conduit being one of the greatest influences on airflow has the potential to affect postoperative PFT values. Our data suggest that PIF may be influenced by dilation size. In addition, pulmonary function data were not collected at consistent time points during follow-up. Our data demonstrate that restenosis occurs in a linear manner that appears to be unique for each patient. It will be important in future studies to standardize the time and manner in which PFTs are administered in order to mitigate these confounding variables.
Conclusion
In the isolated subglottic stenosis model, PEF, PIF, FEV1/PEF, and FIF50% demonstrate a significant change after endoscopic intervention. The postoperative rate of change in the PEF and FEV1/PEF is linear but appears to be unique to each patient. PIF and FIF50% also change as restenosis occurs, but the lack of standardized protocols makes the rate of change more difficult to predict. These pilot data suggest that the change in PEF, FEV1/PEF, PIF, and FIF50% can be used to assess outcomes in the endoscopic management and treatment of iSGS. Furthermore, the rate of change in these values (PEF and FEV1/PEF, in particular) could potentially be used as an objective means of comparing the efficacy of different techniques or adjuvant therapies. Moving forward, prospective studies should focus on establishing uniform time points and protocols for collecting PFT data. Given the low incidence of the entity and the unique characteristics of each stenosis, garnering adequate numbers and long-term follow-up will likely require multi-institutional collaboration.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.