
Abstract
Objective:
The aim was to study the prevalence of otolaryngologic surgeries in pediatric patients with eosinophilic esophagitis (EoE).
Methods:
Retrospective cohort study at a tertiary care center. The type of otolaryngologic surgeries performed in patients with diagnosis of EoE was recorded during a 5-year period.
Results:
Seventy-five percent of patients were male, with average age of EoE diagnosis at 7.5 years with an 83% incidence of atopy. Cohort analysis revealed that 33% (119/362) had a total of 275 otolaryngologic surgeries. Surgeries performed on 119 patients are as follows: 20% bilateral myringotomy with tubes, 14% tonsillectomy, 18.5% adenoidectomy, 1.4% sinus irrigation, 3.3% bronchoscopy, and 1.4% laryngotracheoplasty (LTP); 63% of patients underwent multiple procedures. Thirty percent of patients undergoing bilateral myringotomy with tube placement (BMT) needed additional tubes. Four of 5 LTP patients had successful operations. Twelve percent of patients had EoE diagnosis prior to an otolaryngologic surgery.
Conclusion:
Thirty-three percent of children with EoE required otolaryngologic surgical intervention and nearly one-third who underwent BMT required additional ear tubes. A large fraction of children with EoE will undergo an otolaryngologic surgery, only a minority with a preoperative EoE diagnosis. Until the nature of this relationship is clarified, the high coincidence with otolaryngologic surgeries dictates that otolaryngologists should be familiar with diagnosis of EoE in patients.
Keywords
Introduction
Eosinophilic esophagitis (EoE) is an inflammatory disease of the aerodigestive tract manifesting in the pediatric population with symptoms that include failure to gain weight, feeding disorder, and vomiting often in younger patients and abdominal pain, dysphagia, and food impaction in older patients.1-3 Eosinophilic esophagitis is a clinicopathologic diagnosis dependent on clinical symptomatology, histologic criteria, and exclusion of other conditions that can produce esophageal eosinophilia, especially gastroesophageal reflux disease.4,5 Although the contribution of detection bias cannot be excluded, the calculated incidence of EoE of 1 case per 10 000 pediatric population per year appears to be increasing.3,6 Eosinophilic esophagitis is also strongly associated with atopic disease, with an estimated coincidence of 50% to 80%, leading some to consider EoE a manifestation of allergic response.2,7,8
Despite mucosal inflammation that is limited to the esophagus, EoE should be viewed as an immune-mediated aerodigestive tract disorder that also can be associated with otolaryngologic symptoms. A prior study indicated that 10% to 15% of pediatric patients presented to an otolaryngologist prior to a referral to a gastroenterologist. 9 In addition, EoE may produce sequelae in other regions of the aerodigestive tract, as has been seen with gastroesophageal reflux (GER).5,10-13 The chronic inflammatory response and eosinophilic infiltration in EoE has findings comparable with that seen in the airway mucosa in chronic rhinosinusitis and asthma. 10 Given that EoE does not typically result in pharyngeal mucosal eosinophilia, 14 how esophageal inflammation and airway symptoms are associated remains unclear but may require cytokines and other inflammatory messenger molecules.
Notwithstanding the high prevalence of EoE in otolaryngology patients, there is a paucity of literature on the subject. Whereas data on frequency and type of otolaryngology diagnoses in EoE patients have been reported, 9 the frequency of otolaryngologic surgeries (OS) in children with EoE has not been analyzed. The present study aims to describe the frequency and types of OS in a pediatric population with EoE. This information may provide an opportunity to increase awareness of an EoE and potential practice changes if a significant association is made between OS and EoE.
Methods
A retrospective chart review was performed for all pediatric patients with an International Classification of Diseases (ICD)-9 diagnosis of EoE seen at Children’s Hospital of Wisconsin (CHW), a tertiary care academic facility, from January 2007 to January 2012. Institutional review board approval was obtained for this 5-year period. A preliminary computer-based ICD-9 search reported 435 patients over this period. Individual review of these charts revealed a true diagnosis of EoE in 378 patients, with 57 of the original patients found to have a diagnosis of eosinophilic gastroenteritis, a diagnosis of EoE based on clinical symptomatology that was eventually ruled out upon biopsy, or in a few cases, a probable coding error. Final diagnosis of EoE was made based on clinical suspicion and confirmed with esophageal biopsy. Five of the 378 patients with a diagnosis of EoE had insufficient information in the medical chart, excluding them from further analysis. In addition, patients were excluded from this analysis if they had other disease processes that may contribute to the need for otolaryngologic surgeries. Eleven patients were identified with a documented history of cleft lip/cleft palate, Pierre Robin sequence, trisomy 21, or other chromosomal abnormalities that may cause otolaryngologic disease, or chromosomal abnormalities that are not well defined. These patients were then excluded. The remaining 362 patients’ charts were reviewed for the date of EoE diagnosis based on the date of endoscopic esophageal mucosal biopsy, history of having an OS, personal and family history of atopic disease, household exposure to tobacco, and family history of EoE. With respect to the OS, charts were reviewed for surgical history in physician notes, patient intake forms, and anesthesia records where available to ensure that all procedures were accounted for, including those done by providers outside of the CHW system. Procedures, such as reductions of nasal fractures or those repairing other traumatic facial injuries, were not included in our analysis.
Results
Of the 362 patients analyzed, 119 patients (32.9%) had an OS performed, with 75 patients (20.7%) requiring multiple surgeries, resulting in 275 total surgeries being performed on the study population. The majority of the surgeries were performed by providers at a facility outside of CHW. The average age at the time of first OS was 3.2 ± 2.7 years, and the average age of EoE diagnosis was 7.4 ± 4.9 years (mean ± standard deviation). The population was characteristically male (74.9%) and had a high frequency of personal (82.6%) and family (63.9%) history of atopic disease (Table 1). Four (1%) patients in this cohort of patients who had an OS performed reported household tobacco exposure, and 9 (2%) had a family history of EoE.
Patient Demographics of Study Population.
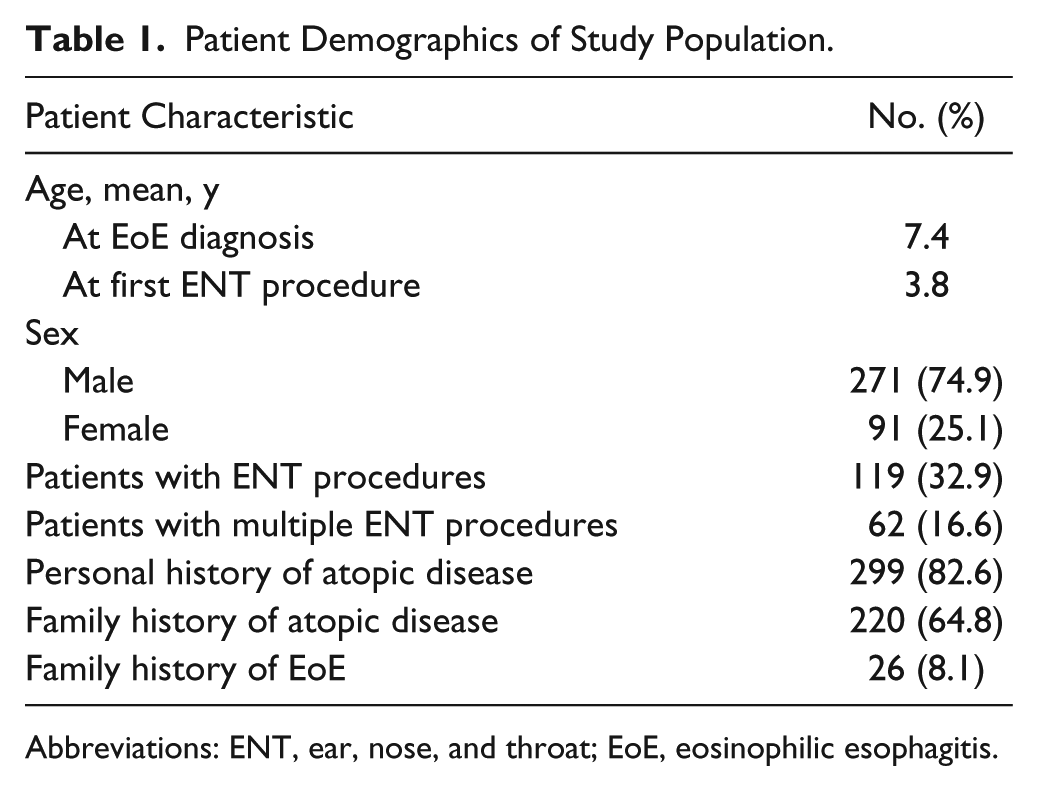
Abbreviations: ENT, ear, nose, and throat; EoE, eosinophilic esophagitis.
With respect to surgeries in the study population, the most frequently performed surgery was bilateral myringotomy with tube placement (BMT) (20%), followed by adenoidectomy (18.5%) and tonsillectomy (14.1%). Airway evaluations via rigid bronchoscopy accounted for 4.1% of cases. Minimally represented were maxillary tap irrigation or antrostomy (1.4%) and laryngotracheoplasty (LTP)/anterior cricoid split (1.4%) (Table 2).
Otolaryngologic Surgeries Performed in Patients With Eosinophilic Esophagitis.
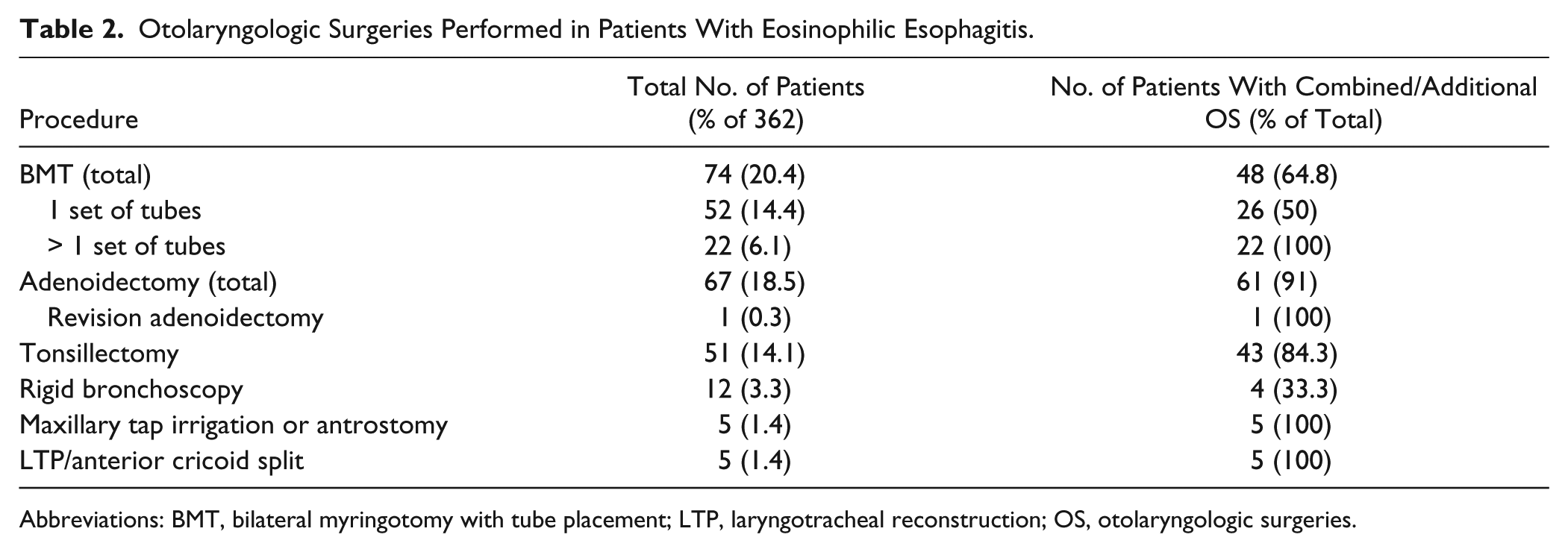
Abbreviations: BMT, bilateral myringotomy with tube placement; LTP, laryngotracheal reconstruction; OS, otolaryngologic surgeries.
A majority of patients (75.6%) were diagnosed with EoE after their initial OS. On average, EoE was diagnosed approximately 3.8 years after the initial OS. An additional 12.6% of patients received an EoE diagnosis from biopsies performed at the time of their initial OS. A minority of patients (11.7%) had an EoE diagnosis prior to having any procedure.
Five patients required anterior cricoid split or LTP; of these, 2 patients had an EoE diagnosis prior to surgery, with the other 3 being diagnosed between 8 months and 3 years following airway reconstruction. Four of the patients had successful operative outcomes; 2 required excision of subglottic granulation tissue in the postoperative period and the other 2 patients did not require any further surgical intervention. One patient failed airway reconstruction.
Chi-square analysis was performed to evaluate for a difference in surgery rates for EoE patients with or without history of atopic disease. The test did not indicate a significant difference, χ2(1) = 0.16. However, the study was initially designed to determine the prevalence of OS in patients with EoE and not powered to investigate the differences in patients with and without atopic disease. For any surgery performed, 33.4% of patients with atopy had surgery and 31.7% of patients without atopy had surgery with P = .67. For BMT, 21.7% of patients with atopy and 15% of patients without atopy had surgery with P = .32 (Figure 1).
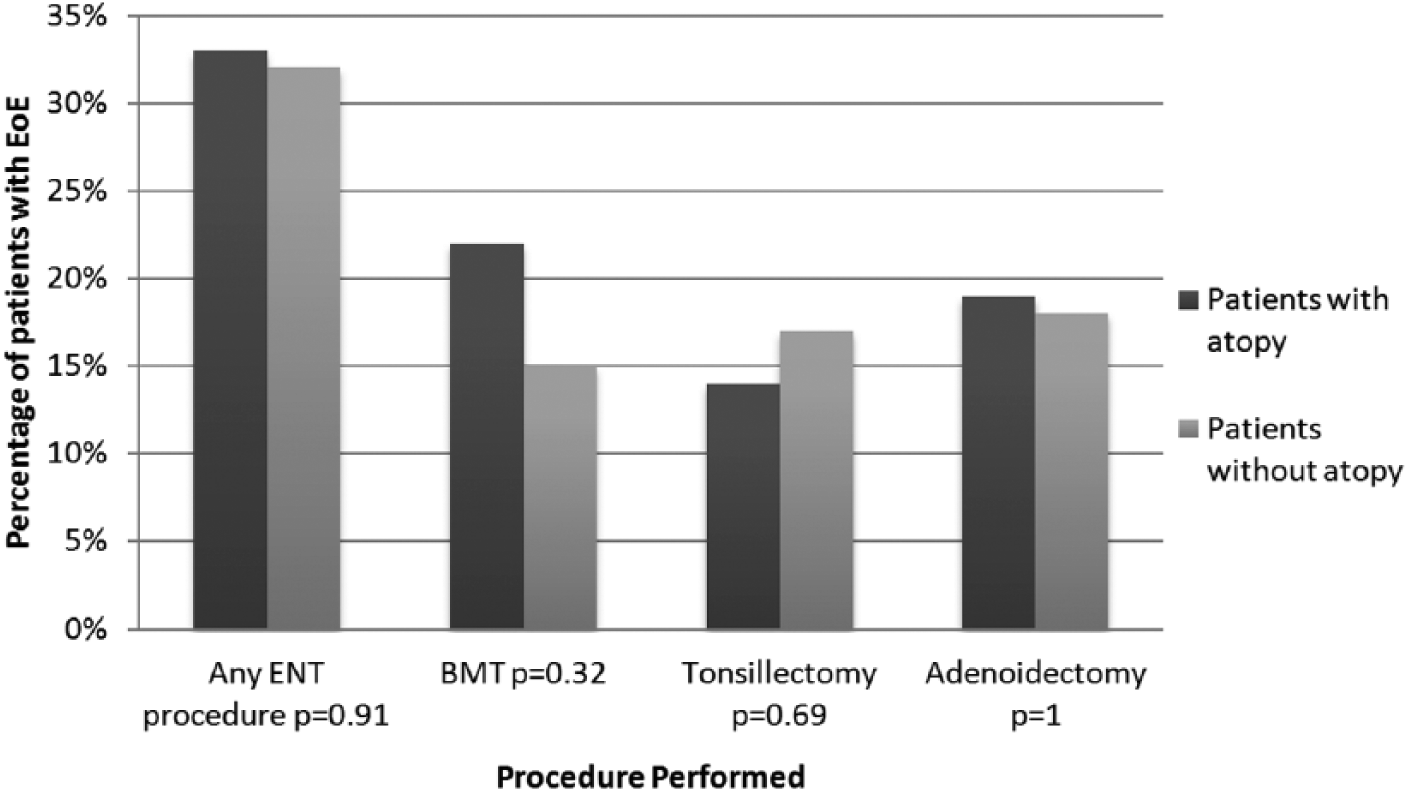
Influence of atopic disease on performed otolaryngologic surgeries in children with EoE.
Discussion
Interest in the clinical manifestations and the underlying pathophysiology of EoE has grown among otolaryngologists, as patients occasionally present to otolaryngologists for initial evaluation of dysphagia or airway symptoms. Prior studies provided analysis regarding the otolaryngologic diagnoses in patients with EoE and demonstrated that Eustachian tube dysfunction and adenotonsillar hypertrophy with sleep disordered breathing were among the most common coincident otolaryngologic diagnoses. 9 We present the first study investigating the incidence of OS in the pediatric EoE population.
Overall, the demographics of our patient population were consistent with published studies on pediatric EoE. 11 There is a clear male predominance (75%), common atopic history (83%), and average age of diagnosis at 7.5 years.1-3,9,11 Although we were unable to determine the average age of patients’ initial symptoms from our retrospective review, prior studies quoted a median age of 4 years for symptom onset with a median age at diagnosis of 7 years. 11 Patients in our cohort, on average, presented to an otolaryngologist prior to a gastroenterologist with an average age of initial OS at 3.8 years old, 4 years less than the average age of EoE diagnosis. This temporal relationship between age of OS and EoE diagnosis is similar to the time frame between symptom onset and diagnosis seen in prior studies. Often, patients present with nonspecific symptoms, making diagnosis difficult initially, and receive treatment for gastroesophageal reflux disease prior to considering diagnosis of EoE. 11 The data obtained from this study would suggest that there may be an association with an EoE diagnosis and need for OS, specifically tympanostomy tubes. The higher incidence of EoE in patients who have undergone OS suggests that simple screening questions for EoE while taking a patient’s history and increased awareness by the provider of the incidence of EoE may allow for an earlier diagnosis. A recently published study describes the average age of esophageal biopsy and EoE diagnosis to be 4.4 years, possibly due to increased awareness of this disease process. 15
Although our study does not have a cohort of children without EoE for comparison, 32.8% of the patients in our study population underwent an OS, which appears to be a relatively high percentage. More than half of these patients had more than 1 OS performed. A study from the Children’s Hospital of Philadelphia calculated that 21.9% of children with EoE were evaluated by an otolaryngologist before or after EoE diagnosis, 9 a number lower than our cohort’s 32.8%. One probable explanation for the discrepancy could be the inclusion of OS performed by community physicians; of the 119 patients included in our study who underwent an OS, 35 had the surgery performed at a tertiary care center, whereas the remaining 84 had them performed out in the community. We were unable to ascertain if patients had been to an outside otolaryngologist provider but not had surgery. Therefore, unlike the Children’s Hospital of Philadelphia study, we were unable to accurately present a breakdown of these patients’ otolaryngologic diagnoses.
Differences among the type of OS performed in children with EoE can be compared to the published frequency of these surgeries in children without EoE. In a national study, 6.8% of children needed at least 1 set of tympanostomy tubes inserted during their first 3 years of life. 16 Comparatively, 15% of our study population required tubes by the age of 3 years. Of note, 30% of our patients who had tympanostomy tubes inserted required multiple sets of tubes. This is higher than previously cited rates for multiple sets of tubes of 17.6% to 20%.17,18 Although this study was designed to primarily assess the incidence of OS, we can only hypothesize the reason for these differences in the rates of tympanostomy tube placement. Patients with EoE frequently have coincident atopic disease and have a strong development of eosinophilic inflammation from external allergic triggers and intrinsic Th2 cytokines. 1 As mucosal eosinophilia is not directly extended proximally from the esophagus to the pharynx, airway inflammation could be mediated via cytokines and other inflammatory agents. 14 The association of allergy and middle ear disease requiring tympanostomy tube placement has been controversial.19-21 Although our study was not designed to settle this controversy, a chi-square analysis was performed to evaluate whether atopic disease is an independent reason for the increased number of OS in our EoE population. No significant differences were observed between the 2 groups. A limitation of this study is the inability to delineate the indication for tympanostomy tube replacement in our retrospective cohort.
Unlike the high representation of BMT in our population, we were surprised to see only 1.4% of the population requiring sinus surgery, especially given the high association with atopy in patients with EoE. In our cohort, 18.5% of the patients underwent an adenoidectomy, but indications were not provided in all medical records. The adenoidectomy may have been performed for chronic rhinorrhea and sinusitis, but indications for a majority of our patients were unknown. The incidence of tonsillectomy in this study population also raises some points of interest, as the frequency of tonsillectomy performed in this population was observed to be 14%. Although our EoE population cannot be generalized to the general pediatric population, slightly more than 500 000 tonsillectomies are performed per year in an estimated population of children 0 to 18 years of age to be 73.9 million in 2011.22,23 There appears to be a greater incidence of tonsillectomies in that EoE population. However, our data on indications for performing the tonsillectomy are limited, as many were performed by community physicians and up to 49% of patients did not have a specific reason stated in the medical record for further analysis. There has been some investigation of the inflammatory role in the development of adenotonsillar hypertrophy. Release of inflammatory cytokines observed in patients with EoE could be hypothesized to contribute to adenotonsillar hypertrophy leading to symptomatic patients and need for tonsillectomy.
Published reports have also implicated EoE in the development of airway pathology.5,12,13 An increased failure rate after airway reconstructive surgery was previously observed in patients with EoE.15,24 Otteson et al 15 described several patients who required tracheotomy after LTP in long-term follow-up of patients diagnosed with EoE in the interim. Our study had only 5 patients (< 2% of cohort) who underwent LTP or anterior cricoid split, and 4 had successful operative outcomes. Two of these patients underwent LTP after diagnosis of EoE and treatment with swallowed topical glucocorticoids. The other 2 patients were diagnosed 8 months and 3 years after LTP and treated with swallowed topical glucocorticoids at that time without subsequent airway interventions needed. One patient with a complicated medical and neonatal history had EoE diagnosed after having both an anterior cricoid split and an LTP and failed airway reconstruction. This patient was born prematurely at 24 weeks’ gestation and developed subglottic stenosis secondary to prolonged intubation. An anterior cricoid split was performed at 3 months of age. He continued to have significant subglottic edema postoperatively and eventually required tracheostomy tube placement. He was never decannulated and subsequently required an LTP at 2 years of age. He continued to have difficulties with decannulation and was diagnosed with EoE at age 3. He was started on swallowed topical glucocorticoids at that time with eventual control of inflammation. He is still tracheostomy tube dependent at 5 years of age and his airway outcome is pending. Although his neonatal course was complicated by sepsis, prematurity, and tracheitis, EoE as the lone factor in failed airway reconstruction is unlikely. Although 4 out of 5 patients in our study had successful airway reconstructions, this subpopulation was not well represented in our cohort and we cannot draw broad conclusions beyond noting that EoE may be associated with failed airway reconstruction in some cases.
The retrospective study has limitations that should be taken into account. The data were obtained from a single tertiary care center and surrounding community and may represent only this geographical region. The retrospective nature of the study can lead to bias in data selection and inability to determine the effect of unidentified confounding variables. Therefore, only associations were able to be observed from this study. The data available to determine the indications for specific procedures that were more common in patients with EoE are limited and prevent the opportunity to provide further conclusions on these observed trends. In addition, the limited access to community physician records precluded further data collection regarding indications for the surgeries performed and timeframe for initial EoE symptoms. Also, an age-matched cohort with atopy or allergic disease was not included to provide direct comparison of incidence of these OS in patients without EoE. However, in comparison to historical incidence of the number of myringotomies with tubes in children (6.8%), our cohort did have a higher incidence than this average.
In our cohort, 75.6% of our patients had a diagnosis of EoE following an OS. This finding is contrary to the study by Smith et al, 9 which had 54.9% of patients having a pre-existing diagnosis of EoE at the time of their otolaryngologic consultation. Furthermore, Otteson et al 15 diagnosed 92 children from 2429 patients undergoing esophageal biopsy from a pediatric otolaryngology practice. Although these 2 studies indicate an awareness of EoE by otolaryngologists and a large percentage of children presenting to an otolaryngologist following EoE diagnosis, our cohort may suggest that awareness of EoE may still be insufficient. Including a brief inquiry of a young patient’s feeding ability and any further gastrointestinal symptoms in the initial evaluation and having an elevated awareness of this disease process may improve the earlier recognition of EoE. As the association of otolaryngologic disease and EoE is being developed, further research may focus on the etiology of this association and the potential need for different management of these otolaryngologic disease processes.
Conclusion
Nearly one-third of children in our EoE cohort required an OS, often prior to diagnosis of EoE. The incidence of BMT and need for additional myringotomy and tube placement was higher than prior reports, suggesting an association between EoE and middle ear pathology. Furthermore, 5 patients in our cohort underwent airway reconstruction, with 1 continued tracheotomy decannulation failure that could be attributed to inflammation associated with EoE. Last, a suspicion for EoE should be considered, especially when children with a history of feeding difficulty or other gastrointestinal symptoms may require general anesthesia for an otolaryngologic surgery. Whereas the understanding of EoE and its natural history continue to evolve, children with EoE may have overlapping presentation of otolaryngologic pathology and are better served by otolaryngologists who are aware of EoE and able to properly refer for treatment.
Footnotes
Acknowledgements
The authors thank Aniko Szabo, PhD, for biostatistics consultation and assistance with data analysis.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The statistical support and interpretation of the data is provided, in part, by grant 1UL1RR031973 from the Clinical and Translational Science Awards program of the National Center for Research Resources, National Institutes of Health.