
Abstract
Objective:
To investigate the clinical features and vestibular symptoms of patients with abnormal ocular vestibular evoked myogenic potentials (oVEMPs) and/or cervical VEMPs (cVEMPs) in the presence of normal caloric responses.
Study Design:
Retrospective chart review.
Setting:
Tertiary referral center.
Methods:
One thousand five hundred twenty-one consecutive patients with balance problems who underwent the caloric, cVEMP, and oVEMP tests were included, and patients who showed abnormal oVEMPs and/or cVEMPs in the presence of normal caloric responses were selected. Clinical characteristics, diagnoses, and vestibular symptoms of the patients were analyzed.
Results:
Of the 1521 patients, 227 (15%) were found to have abnormal oVEMPs and/or cVEMP responses with normal caloric responses. Benign paroxysmal positional vertigo (BBPV), Meniere’s disease, and vestibular migraine were the common diagnoses of these patients. Eighty-one patients (36%) could not be diagnosed with a recognizable disease. Multiple episodes of spinning vertigo with a duration of seconds to hours were their most common vestibular symptoms.
Conclusion:
BPPV, Meniere’s disease, and vestibular migraine are the most frequent diagnoses showing abnormal oVEMP and/or cVEMPs without canal paresis. Apart from these clinical entities, a portion of undiagnosed patients with multiple episodes of vertigo might have a disease that involves the otolith organs only.
Introduction
The vestibular labyrinth, which is composed of 2 otolith organs and 3 semicircular canals, provides a sense of balance and orientation. Dysfunction of the vestibular labyrinth causes various kinds of vertigo and/or dizziness depending on the time-course of the disease and the extent of the lesion in the inner ear. 1 Lateral semicircular canal function in patients with vertigo or dizziness has been widely evaluated with caloric testing,1,2 and hence it is well known that rotatory vertigo is the most common symptom of patients with acute dysfunction of their semicircular canals. On the other hand, less is known about the vestibular symptoms caused by dysfunction of the otolith organs since evaluation of the function of otolith organs has previously been difficult.
Vestibular evoked myogenic potentials (VEMPs) recorded by surface electrodes have been used clinically to assess vestibular function.3-5 Cervical vestibular evoked myogenic potentials (cVEMPs) that are recorded from the sternocleidomastoid muscles (SCMs) in response to air-conducted stimulations (ACS) have been used to evaluate the function of the saccule and its afferents.3,5 Recent investigations have revealed that VEMPs can also be recorded from muscles beneath the eyes in response to ACS and bone-conducted vibration (BCV). 6 These potentials are called ocular vestibular evoked myogenic potentials (oVEMPs) and are considered to represent the function of the utricle and its afferents mediated by a crossed otolith-ocular pathway.7-10 Combined use of cVEMPs, oVEMPs, and caloric testing has enabled us to examine the function of the saccule, utricle, and lateral semicircular canals separately.
Previous studies have reported that patients who have characteristic vestibular symptoms, such as drop attacks, tilting, or translational sensation, tend to show abnormal cVEMP and/or oVEMP responses.11-15 However, it is still unclear whether dysfunction of the otolithic organs causes other types of dizziness. We previously studied the clinical features of diseases showing abnormal cVEMPs to ACS in the presence of normal caloric responses 16 and reported that some patients who were diagnosed as having a disease involving the saccule and its afferents showed various types of vertigo or dizziness, including rotatory vertigo, tilting sensation, and disequilibrium. In the present study, we examine the clinical features and vestibular symptoms of patients who show abnormal oVEMP and/or cVEMP responses in the presence of normal caloric responses.
Materials and Methods
Patients
This retrospective data collection study was approved by the regional ethical standards committee in the Faculty of Medicine at the University of Tokyo (No. 2487) and conducted according to the tenets of the Declaration of Helsinki.
We reviewed the clinical records of 1521 consecutive patients with dizziness who underwent caloric, cVEMP, and oVEMP testing at the Balance Disorder Clinic at the University of Tokyo Hospital between January 2009 and December 2013. All of these patients had received a detailed history taking and a battery of tests including a physical examination and standardized neurological, neurotological, and audiological examinations. The neurotological examination included testing for spontaneous nystagmus with and without Frenzel goggles, nystagmus evoked by head shaking, positional nystagmus in the supine and head-hanging positions, as well as gaze-evoked nystagmus in the horizontal and vertical plane. Smooth pursuit and saccades were also tested, as well as the vestibulo-ocular reflex (VOR) in response to a head impulse test in the horizontal plane. Balance tests included the Romberg test and walking in a straight line. Neuroimaging studies such as computed tomography and magnetic resonance imaging of the brain were performed in 54% of the patients.
Clinical diagnoses of benign paroxysmal postural vertigo (BPPV), 17 Meniere’s disease, 18 vestibular migraine, 19 psychiatric dizziness, 20 and inferior vestibular neuritis 21 were made according to published criteria for those conditions. Classification of vestibular symptoms were made according to the Barany Society’s International Classification of Vestibular Disorders (ICVD). 22 In this ICVD, vertigo is defined as a false or distorted sense of rotation, translation, or tilt of self-environment; dizziness is defined as a non-vertiginous sense of disturbed or impaired spatial orientation; and unsteadiness as a feeling of swaying, rocking, instability while sitting, standing, or walking.
Vestibular Function Tests
oVEMPs to ACS and BCV
The methods for recording oVEMPs to ACS and BCV have been described in detail elsewhere.7,10,23 In brief, with the subject in a supine position, EMG electrodes were placed on the skin 1 cm below (active) and 3 cm below (indifferent) the center of each lower eyelid. The ground electrode was placed on the chin. During testing, the subject looked up approximately 30º above straight ahead and maintained their focus on a small dot approximately 1 m from their eyes. The signals were amplified by a differential amplifier (bandwidth: 0.5-500 Hz), and the unrectified signals were averaged (n = 50) using Neuropack Σ (Nihon Kohden, Tokyo, Japan).
The ACS stimuli were short tone bursts of 4 ms duration at 500 Hz (rise/fall time = 1 ms and plateau time = 2 ms) presented separately to each ear through calibrated headphones (type DR-531, Elega Acoustics Co, Ltd, Tokyo, Japan). The stimulus intensity was set at 135 dB SPL. The stimuli were delivered 5 times per second. When using ACS, the n10 responses were measured beneath the eye contralateral to the stimulated ear; 7 the amplitude of these contralateral responses was used for calculation of the asymmetry ratio when using ACS. The BCV stimuli were 4 ms tone-bursts of 500 Hz vibration delivered by a handheld 4810 mini-shaker (Bruel and Kjaer, Naerum, Denmark) fitted with a short rod terminated in a bakelite cap 1.5 cm in diameter, which was placed, without pressure, perpendicularly on the forehead at the hairline in the midline (Fz). The driving voltage was 80 V peak to peak, and it produced a peak force level of 128 dB re 1 μN. This BCV caused a linear acceleration in the inter-aural axis at the mastoids with a maximal acceleration of approximately 0.4 g peak to peak as measured by linear accelerometers placed on the skin over the mastoid. The stimuli were applied 3 times per second, and the time window for analysis was 50 ms. Two sets of 50 stimuli were averaged.
We analyzed the amplitude of the first negative peak (n10). The latency was measured from the onset of the stimulus to the peak. The amplitude was measured from the baseline to the peak. We calculated the asymmetry ratio (AR) for n10 amplitude (oVEMP AR) with the following formula using the n10 amplitude beneath the eye ipsilateral to the affected side (Aa) and beneath the eye ipsilateral to the un affected side (Au):

The upper limit for the normal oVEMP AR was set at 27.3 for oVEMPs to BCV 23 and at 34.4 for oVEMPs to ACS. 7 When no reproducible n10 was present in 2 runs, we classified the response as being “absent.” When a reproducible n10 was present and the AR was greater than the normal upper limits, we classified the response as “decreased.” We regarded both “absent” and “decreased” responses as abnormal responses for the purpose of our analyses. With regard to oVEMPs to ACS, we judged only the patients with unilaterally abnormal responses as abnormal, excluding the patients with bilaterally absent responses from the abnormal group, since oVEMPs to ACS are reported to be absent in approximately 10% of normal healthy subjects. 24
cVEMPs to ACS
To record cVEMPs, the EMG electrodes were placed at symmetrical sites over the upper half of the sternocleidomastoid muscles, with reference electrodes on the side of the upper sternum. The ground electrode was placed on the nasion. The signals from the stimulated side were amplified by a differential amplifier (20-2000 Hz), and the unrectified signals were averaged (n = 100). Short tone bursts (500 Hz, 4 ms, 135 dBSPL) were delivered through headphones. The patients were instructed to contract their SCM during testing by lifting their head off the pillow. During the recording, EMG activity of the SCMs was monitored on a display to ensure that muscle activity was maintained at a sufficient level (>150 μV) in each patient. We analyzed the first biphasic responses (p13-n23) from the ipsilateral SCM to the stimulated side. We calculated the asymmetry ratio for the amplitude of cVEMPs (cVEMP AR) with the following formula using the amplitude of p13-n23 on the affected side (Aa) and that on the unaffected side (Au):

On the basis of results from normal subjects, the upper limit for the cVEMP AR was set to 34.0. 25 When no reproducible p13-n23 was present in 2 runs, we regarded it as an “absent” response. When a reproducible p13-n23 was present and the AR was greater than the predefined upper limit for normal subjects, we regarded it as a “decreased” response. Both “decreased” and “absent” responses were classified as abnormal responses.
Caloric tests
Caloric testing was performed by irrigating the external auditory canal with 2 ml ice water (4°C) for 20 seconds followed by aspiration of water. This method of caloric stimulation is easier to perform than bithermal irrigation with water at 30° and 44° C and has been shown to have a high sensitivity and specificity for detecting canal paresis (CP) based on Jongkee’s formula. 26 Caloric nystagmus was recorded, in a darkened room, using an electronystagmograph. We defined an abnormal caloric response by either of the following criteria: (1) CP percentage >20% 16 and (2) maximum slow phase eye velocity <10°/s bilaterally. 27
Classification of patients
We classified patients based on the results of oVEMPs and cVEMPs. Patients who showed abnormal oVEMP responses with normal cVEMP responses were classified as oVEMP−/ cVEMP+, those who showed normal oVEMP responses with abnormal cVEMP responses as oVEMP+/ cVEMP−, and those who showed abnormal oVEMP responses as well as abnormal cVEMP responses as oVEMP−/ cVEMP−.
Statistical analysis
A comparison of the age and sex in each group was made using the Kruskal-Wallis test (P < .05); the Steel-Dwass multiple comparison test was performed to compare all pairs of means (P < .05). IBM SPSS statistics 21 (IBM Corporation, New York City, New York, USA) was used for the statistical analysis.
Case Report
A 51-year-old man suddenly felt a to-and-fro sensation with nausea lasting 5 minutes while sitting on a chair in his office. He had no associated complaints of hearing loss, tinnitus, fullness in the ears, headache, or changes in his strength or sensation. After this episode, he had similar episodes a few times per week. He had no previous history of vestibular symptoms. There was no significant past medical history. The family history was not contributory.
On examination at 1 month after the onset of symptoms, he underwent audio-vestibular testing. He had a spontaneous, right-beating nystagmus under Frenzel goggles, but it disappeared without the goggles. Turning the head to the left in the supine position increased the slow-phase eye velocity of the spontaneous nystagmus, but this patient did not have BPPV. The Romberg test and Fukuda (Unterberger) test both gave negative results. A pure-tone audiogram revealed normal hearing in both ears. The head impulse test and caloric test showed normal semicircular canal function in the horizontal plane. In oVEMPs to BCV, the n10 response recorded from the right eye was absent, while the response from the left eye showed normal n10 responses (Figure 1). cVEMPs to air-conducted sound were normal on both sides. Magnetic resonance imaging of the brain showed normal findings.
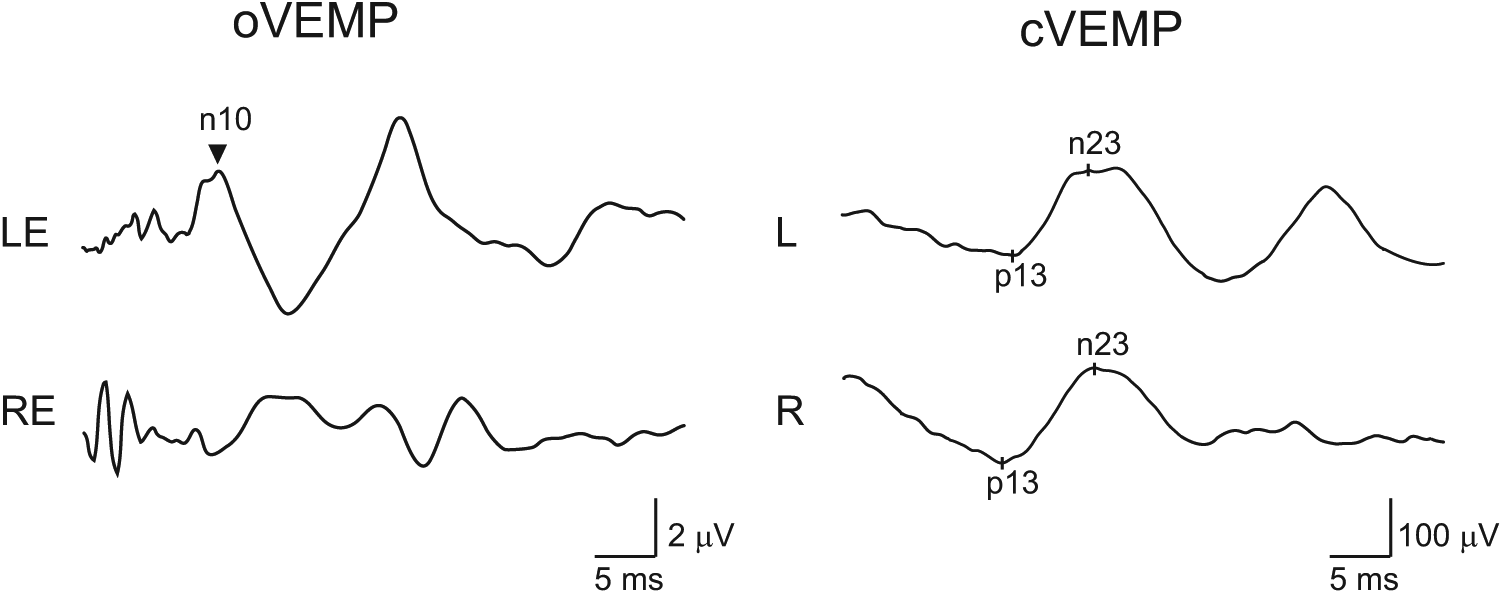
oVEMP and cVEMP in a patient (51-year-old) classified into the oVEMP−/cVEMP+ group. In oVEMPs to bone-conducted vibration (left panel), the n10 response recorded from the right eye was absent, while the response from the left eye showed normal n10 responses. cVEMPs to air-conducted sound were normal on both sides. Magnetic resonance imaging of the brain showed normal findings.
The patient was diagnosed as having otolithic dysfunction and was classified as oVEMP−/cVEMP+.
Results
Of the 1521 patients who underwent oVEMP, cVEMP, and caloric testing, 227 patients (15%; 91 men and 136 women; mean age ± SD: 51.4 ± 17.5 years) were found to show abnormal oVEMP and/or cVEMP responses with normal caloric responses. All of these patients showed normal responses in horizontal head impulse test bilaterally. Among them, 53 patients (23%; 20 men and 33 women; 51.3 ± 18.3 years) showed abnormal oVEMP responses with normal cVEMP responses (oVEMP−/cVEMP+), 102 patients (45%; 43 men and 59 women; 50.2 ± 17.7 years) showed normal oVEMP responses with abnormal cVEMP responses (oVEMP+/cVEMP−), and the remaining 72 patients (32%; 44 men and 28 women; 53.4 ± 16.5 years) showed abnormal oVEMP responses as well as abnormal cVEMP responses (oVEMP−/cVEMP−). The majority of the oVEMP−/cVEMP− group were male, while the majority were female in the other 2 groups. There was a significant difference in the sex ratio among the 3 groups (P < .05). There was no significant difference in the mean ages among the 3 groups (P > .7).
Table 1 shows the clinical diagnoses of patients who showed abnormal oVEMPs and/or cVEMPs without canal paresis. BPPV and vestibular migraine were the most common diagnoses in the oVEMP−/cVEMP+ group, whereas Meniere’s disease was the most common in both the oVEMP+/cVEMP− and the oVEMP−/cVEMP− groups. BPPV, vestibular migraine, psychiatric dizziness, and Meniere’s disease comprised approximately 40% of the diagnoses in each group. Other diagnoses included vestibular schwannoma, orthostatic hypotension, and vertebrobasilar insufficiency. Eighty-one (36%) of the patients who showed abnormal oVEMPs and/or cVEMPs without canal paresis did not have a recognized disease entity.
Clinical Diagnoses of Patients With Abnormal oVEMPs and/or cVEMPs Without Canal Paresis.
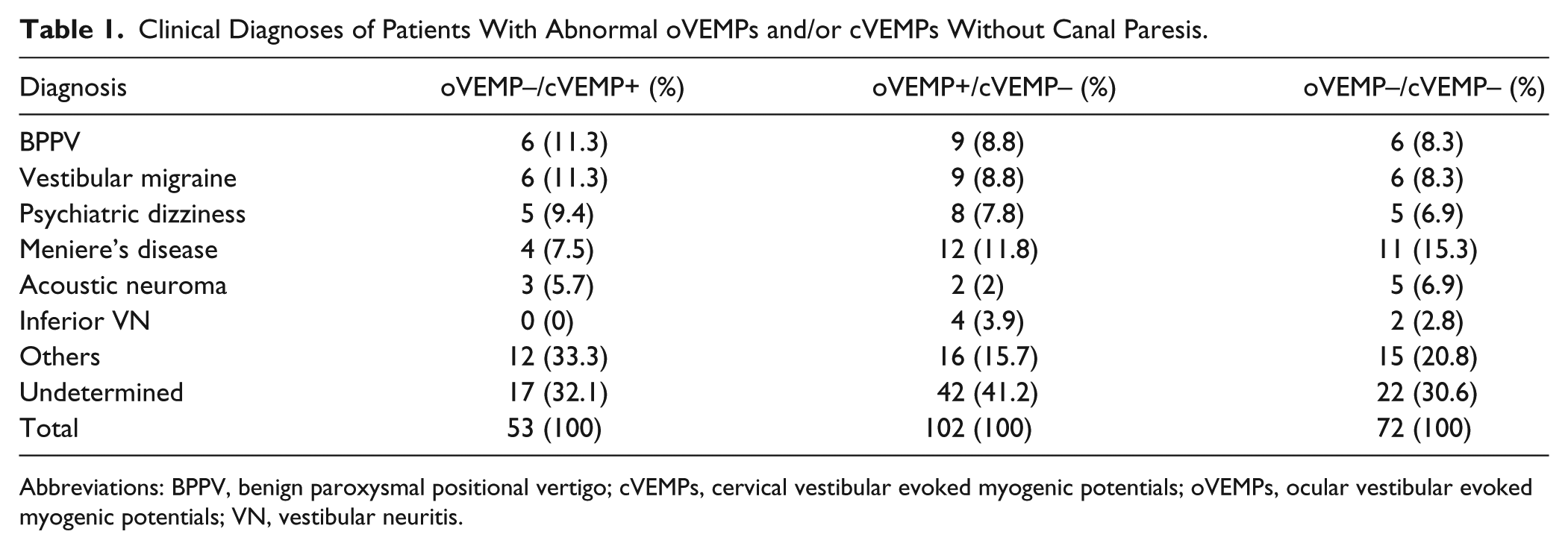
Abbreviations: BPPV, benign paroxysmal positional vertigo; cVEMPs, cervical vestibular evoked myogenic potentials; oVEMPs, ocular vestibular evoked myogenic potentials; VN, vestibular neuritis.
Table 2 shows the clinical characteristics of patients without diagnoses who had abnormal oVEMPs and/or cVEMPs without canal paresis. The mean ages of all 3 groups were in the mid 50s. Male patients were predominant in the oVEMP−/cVEMP+ group (59%), whereas female patients were predominant in the oVEMP+/cVEMP− group (55%) and oVEMP−/cVEMP− group (55%). Spontaneous nystagmus was observed under Frenzel goggles in approximately 20% of the patients in each group, most of which was horizontal. One patient in the oVEMP+/cVEMP− group and 1 patient in the oVEMP−/cVEMP− group had downbeat and upbeat components of nystagmus, respectively, which were mixed with horizontal components.
Clinical Characteristics of Undiagnosed Patients With Abnormal oVEMPs and/or cVEMPs Without Canal Paresis.
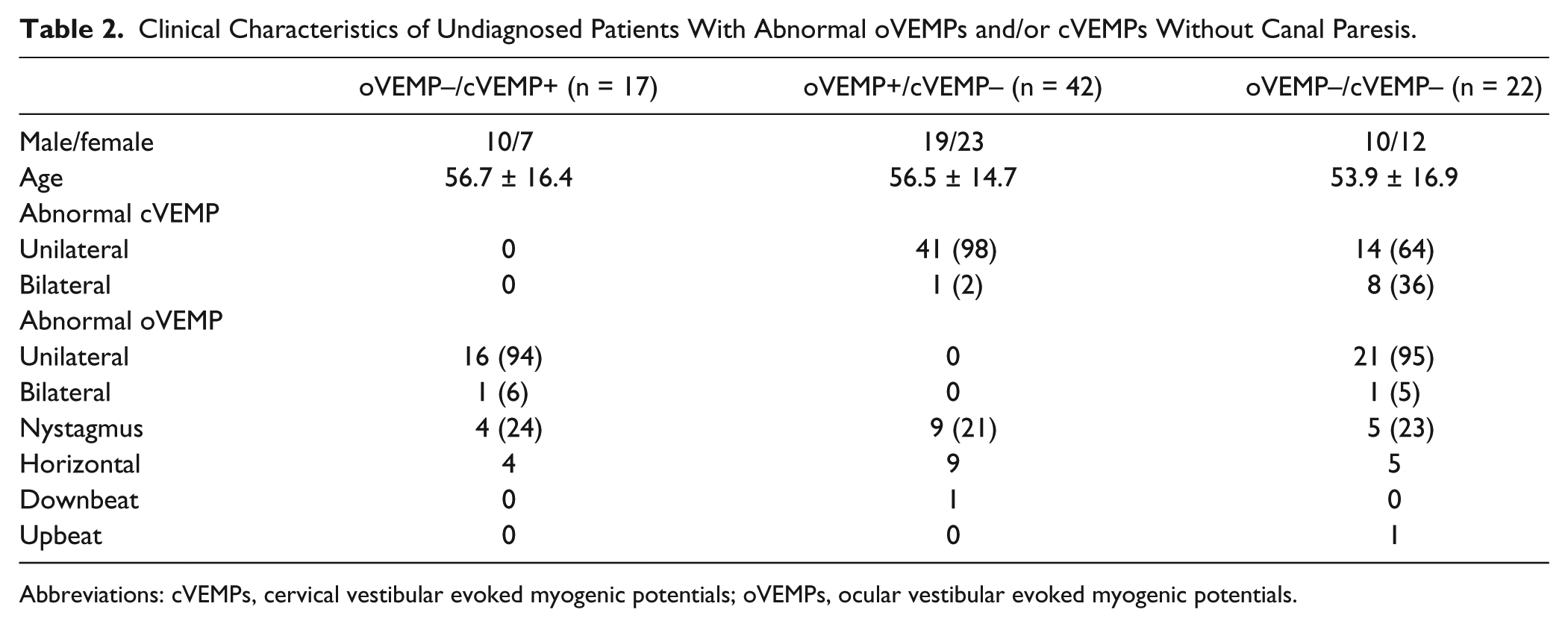
Abbreviations: cVEMPs, cervical vestibular evoked myogenic potentials; oVEMPs, ocular vestibular evoked myogenic potentials.
Table 3 shows the vestibular symptoms in undiagnosed (undetermined) patients with abnormal oVEMPs and/or cVEMPs without canal paresis. The majority of patients in each group had experienced multiple episodes of vestibular symptoms. Vertigo had been experienced by approximately 50% of the patients in each group. In the oVEMP−/cVEMP+ group, a half of the patients had spinning vertigo with a duration of minutes to hours while the others showed non-spinning vertigo, most of which lasted less than 1 minute. In the oVEMP+/cVEMP− and oVEMP−/cVEMP− groups, most patients experienced the spinning form of vertigo. Symptoms of non-spinning vertigo included swaying (n = 2) and tilting (n = 1) sensations. Approximately half of the patients in each group had dizziness or unsteadiness. Among these patients, spontaneous dizziness was most frequent in the oVEMP+/cVEMP− and oVEMP−/cVEMP+ groups, whereas positional or orthostatic dizziness were most frequent in the oVEMP−/cVEMP− group. A drop attack, which is classified as directional pulsion, was observed in only 1 patient in the oVEMP+/cVEMP− group.
Vestibular Symptoms in Patients With Abnormal oVEMPs and/or cVEMPs Without Canal Paresis.
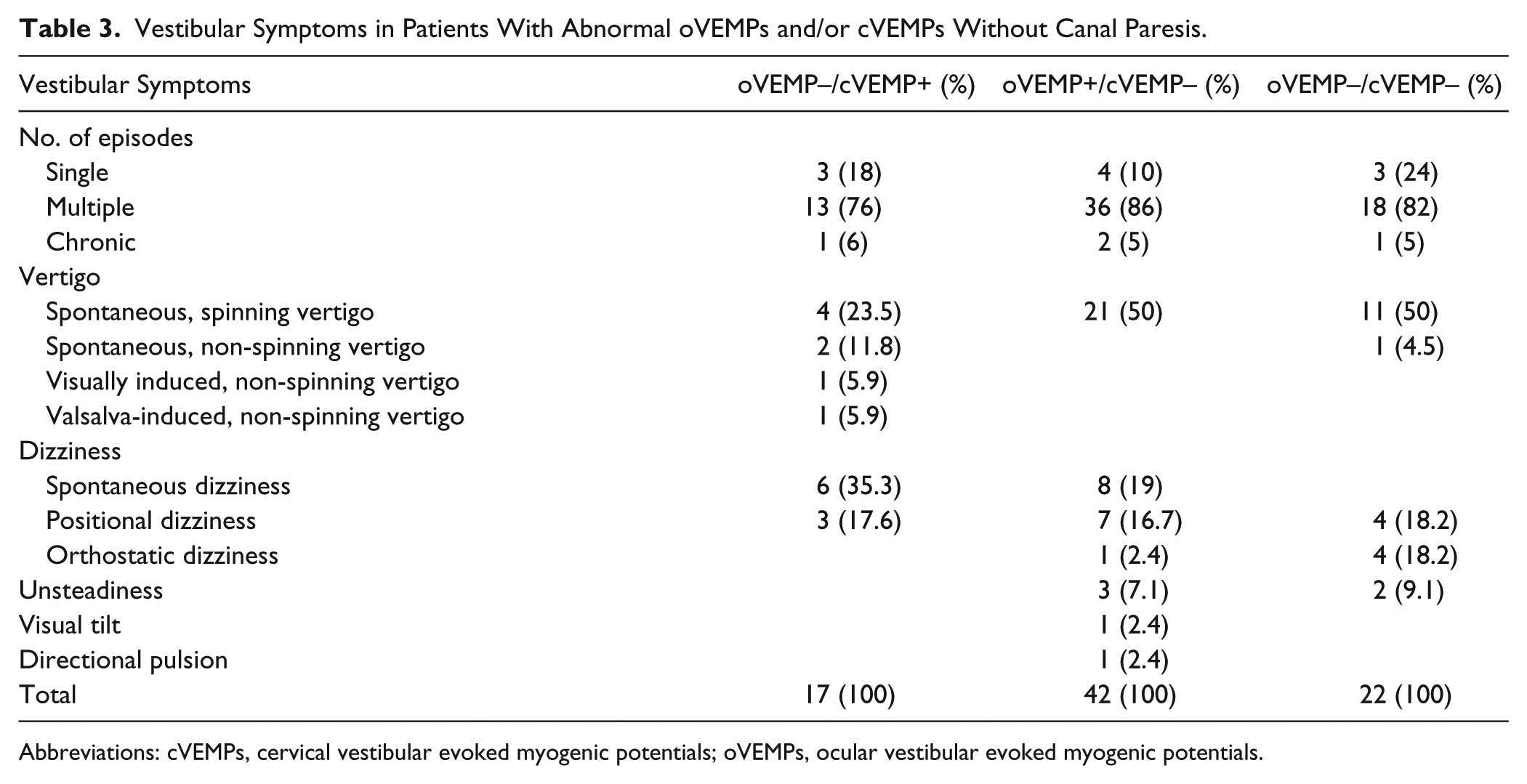
Abbreviations: cVEMPs, cervical vestibular evoked myogenic potentials; oVEMPs, ocular vestibular evoked myogenic potentials.
Discussion
The use of oVEMPs as well as cVEMPs has enabled clinicians to explore vestibular abnormalities in more detail.4,5 Clinical and neurophysiological studies have suggested that cVEMPs in response to ACS reflect function in the saccule and inferior vestibular nerve, 5 whereas oVEMPs to ACS as well as BCV primarily reflect function in the utricle and superior vestibular nerve.8,9 Combined use of cVEMPs, oVEMPs, and caloric testing has enabled us to examine the function of the saccule, utricle, and the lateral semicircular canals separately. To clarify the clinical features of dizziness caused by the otolithic organs, we retrospectively studied the clinical characteristics of patients with dizziness who showed abnormal oVEMP and/or cVEMP responses with normal caloric responses.
In the present study, approximately 15% of patients with dizziness showed abnormal oVEMP and/or cVEMP responses with normal caloric responses. Among them, the oVEMP+/cVEMP− group was the most frequent (45%), followed by the oVEMP−/cVEMP− group (32%) and oVEMP−/cVEMP+ (23%) group. The clinical diagnoses of the patients were different among these 3 groups: BPPV and vestibular migraine were most frequent in the oVEMP− /cVEMP+ group, while Meniere’s disease was most frequent in both the oVEMP+/cVEMP− and oVEMP−/cVEMP− groups. BPPV has been considered to be caused by canalolithiasis and cupulolithiasis in the semicircular canals. 28 In addition to these mechanisms, utricular dysfunction has also been suggested as a possible mechanism of BPPV. 29 Nakahara et al 29 reported that patients with BPPV have a tendency to show abnormal oVEMPs more frequently than cVEMPs, consistent with our study. Vestibular migraine is increasingly recognized as a frequent cause of vestibular symptoms. 19 Its pathophysiology is still unclear, and there is ongoing debate as to whether its origin is central or peripheral. 30 It has been reported that patients with vestibular migraine show abnormal oVEMPs as well as cVEMPs more frequently than normal subjects, suggesting that at least a portion of patients with vestibular migraine have dysfunction of the otolithic organs or their afferents.31,32 Abnormal cVEMPs as well as oVEMPs in Meniere’s disease have been reported by several groups, and approximately half of Meniere’s disease patients show abnormal cVEMPs and/or oVEMPs during the quiescent period.33,34 A human temporal bone study showed that endolymphatic hydrops was most frequently observed in the saccule, followed by the cochlear, utricle, and the semicircular canals. 35 Young et al 34 advocated the use of oVEMP, cVEMP, and caloric tests to assess the extent of endolymphatic hydrops in the inner ear in Meniere’s disease.
In the current study, 36% (81/225) of the patients who showed abnormal oVEMPs and/or cVEMPs with normal caloric responses could not be diagnosed with an established clinical entity. Most of these patients showed normal results on audiologic and neurotologic tests, except for VEMP responses. Since oVEMP as well as cVEMP responses are considered to be clinical tests of the otolith organs, dysfunction of the otolith organs sparing the semicircular canals were considered to be present in these patients. Such patients would be expected to have vertical or vertical/torsional nystagmus during attacks since electrical stimulation of the saccule or the utricle produces vertical or vertical torsional nystagmus in mammals.36-38 However, in the present study, only approximately 20% of these patients showed spontaneous nystagmus during testing, and this was mostly horizontal. Recently, Manzari et al 39 reported an unsteady patient with horizontal nystagmus who showed normal head impulse tests but abnormal oVEMPs to BCV unilaterally. They speculated that spontaneous horizontal nystagmus could be caused by dysfunction of the utricle, since otolithic stimulation generated by linear acceleration modulates the slow-phase eye velocity of horizontal nystagmus via the widespread convergence of neural inputs from the otoliths onto horizontal canal neurons in the vestibular nuclei. 40
Vestibular symptoms caused by otolithic dysfunction have traditionally been suggested as a tilting sensation, a sense of moving to and fro, lateropulsion, or feelings of falling, based on physiological evidence that the otolithic signals play an important role in the sense of uprightness and postural control and in the perception of linear motion. 41 Recent studies have shown that patients who complained of a forward or backward pulling sensation, episodic tilt, or a translational sensation have a tendency to show abnormal oVEMP and/or cVEMPs, suggesting these symptoms are caused by dysfunction of the otolith organs.11-15 In the present study, spinning vertigo was the most frequent vestibular symptom in undiagnosed patients showing abnormal oVEMP and/or cVEMPs without canal paresis. Although the direction of the spinning vertigo was not known in most patients, they might include vertigo in the yaw, roll, or pitch planes since stimulation of the saccule or utricle can produce horizontal, 40 vertical, or vertical-torsional nystagmus. 36 Non-spinning vertigo, such as swaying and tilting, was more frequently observed in the oVEMP−/cVEMP+ group than in the other 2 groups, suggesting an association of the symptoms with utricular dysfunction.12,13 Spontaneous and positional dizziness were also common in all the 3 groups, and these symptoms have been regarded as indicative of otolith dysfunction.29,41 Although Tumarkin’s drop attacks have been implicated as a representative symptom of utricular dysfunction, 42 there was only 1 patient in the oVEMP+/cVEMP− group who experienced these attacks. Patients with Meniere’s disease who had experienced drop attacks were reported to show abnormal oVEMPs as well as cVEMPs more frequently than those who had not expereinced drop attacks. 43
The etiologies of otolith dysfunction are unknown and may be heterogeneous. Since most patients had multiple episodes of vertigo or dizziness with the duration from seconds to hours, they might have a distinct pathology other than vestibular neuritis, such as endolymphatic hydrops, ischemia, or an autoimmune condition. Calzada et al 44 examined the otolithic membrane of patients who had had multiple episodes of Tumarkin’s drop attacks without Meniere’s disease and reported that they had damaged otolithic membranes in the utricle. They speculated that the underlying pathology in drop attacks results from injury to the otolithic membrane, resulting in free-floating otoliths and atrophy, although it remains unclear how the damaged otolithic membranes cause multiple vestibular drop attacks.
Our study has some limitations. First of all, this is a retrospective study. There might be some bias in the distribution of the patients who showed abnormal oVEMP and/or cVEMP responses with normal caloric responses. Second, there are differences in the sensitivity and the specificity among oVEMPs, cVEMPs, and caloric tests. They might affect the classification of the patients. Third, the responses of the anterior or posterior canals were not measured. To measure function of these canals, a quantitative head impulse test is required. Fourth, vestibular functions was measured in the quiescent period. It is possible that vestibular symptoms were caused by semicircular canals dysfunction, which had returned to normal before the vestibular testing was performed.
In conclusion, we sought patients who had vestibular symptoms and showed abnormal oVEMP and/or cVEMPs without canal paresis. Among these patients, BPPV, vestibular migraine, Meniere’s disease, and psychiatric dizziness were the most frequent diagnoses. At least a portion of the undiagnosed patients might have had vestibular symptoms caused only by dysfunction of the otolith organs. Their symptoms were various, but the most frequent vestibular symptoms were multiple episodes of spinning vertigo with a duration of seconds to hours. The underlying pathologies are still unknown. To clarify these, a more elaborate estimation of the function of the otolith organs and semicircular canals and accumulation of pathological evidence are required.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.