
Abstract
Objectives:
In the emergency department, fish and chicken bone impactions are typically evaluated with screening x-rays. We sought to determine whether this modality ultimately improves system outcomes, including length of stay (LOS), cost, and radiation dosage.
Methods:
We reviewed patients ≥18 years old presenting to an urban academic emergency department over a 4-year period who received a screening soft-tissue x-ray to determine the presence of a retained fish or chicken bone. We calculated the diagnostic accuracy of x-ray and computed tomography (CT) evaluations, respectively, in addition to system outcomes.
Results:
Twenty-seven of the 78 patients included for analysis were ultimately positive for bone impaction. Initial x-ray interpretations demonstrated a sensitivity of 24.0% (95% CI, 9.4%-45.1%) and a specificity of 90.0% (95% CI, 78.2%-96.7%). However, initial CT interpretation (ie, a preliminary read from on-call residents) demonstrated a sensitivity of 75% (95% CI, 19.4%-99.4%) and a specificity of 100% (95% CI, 59.0%-100%). LOS, cost, and radiation dosage were not significantly different between patients who ultimately had true bone impactions and those who did not (P > .05).
Conclusions:
X-rays are poor screening tools in determining fish or chicken bone impactions with poor diagnostic and system utility. Further studies should be performed to evaluate the role of a low-radiation CT screen.
Introduction
The most common foreign body impactions in adults are caused by food boluses, in particular fish and chicken bones. 1 Fish bones are the most common upper respiratory and digestive tract foreign bodies necessitating evaluation, found in 71% of adults who presented with foreign body ingestion in a large case series. 2 Although rare, complications of retained fish bones in this area can lead to retropharyngeal abscess, mediastinitis, pulmonary abscess, and perforated bowel. 3 For this reason, prompt identification and removal of the embedded foreign body is essential.
Unfortunately, the management of a patient who presents with a potential fish or chicken bone impaction can be challenging. A large, prospective study found that of 358 patients presenting with a complaint of fish bone ingestion, only 114 (31.8%) actually had the fish bone identified. 4 Only 18% of bones could be identified and removed with direct visualization, and presenting symptoms such as foreign body sensation, dysphagia, or sense of obstruction were not associated with actual presence of the foreign body. Chicken bone impactions are similarly prevalent and difficult to evaluate. Unfortunately there are no codified diagnostic guidelines for evaluation of suspected foreign body impactions.
A typical course of action for patients with potential fish or chicken bone ingestion with question of retained foreign body is to undergo initial imaging with a plain film of the neck and otolaryngology consultation for flexible endoscopy in an attempt to visualize the foreign body. Obtaining plain films is controversial, as only about one-third of patients presenting with fish bone ingestion will have a diagnostic plain radiograph, and another third of patients will have false positive findings on plain lateral neck x-ray. 4 The primary reason for the low sensitivity is that the majority of fish bones are not radiodense compared to the structures in the upper airway, and calcification of the laryngeal structures in older patients may prompt false positive interpretation of plain radiographs.5,6 Despite the low diagnostic accuracy of plain films, this modality is currently utilized for initial evaluation due to the perception that they are more cost-effective and lead to a more timely diagnosis with reduced radiation dosage. 7
When plain film imaging is inconclusive and the patient shows no evidence of foreign body on direct observation or flexible endoscopy, a computed tomography scan (CT) can be ordered to determine the presence of foreign body. CT scans are especially helpful when foreign bodies are in the low hypopharyngeal or esophageal regions, where the yield of flexible endoscopy is limited. In a review of 4 small prospective, nonrandomized studies comparing plain radiographs to CT, CT had a sensitivity of 100% in all 4 studies and there was just 1 false positive in all 80 patients pooled from the studies. 8 In a recent study by Park et al, 9 64-slice multidetector computed tomography (MDCT) demonstrated 100% sensitivity among 66 patients, versus 51.7% among plain radiographs. With this apparent superiority in mind, the clinician must balance the associated time, cost, and radiation of CT against the poor performance of clinical evaluation and plain radiographs. Likewise, inconclusive plain films with subsequent direct visualization, CT, and/or consults can be time-consuming and costly for the patient.
While the poor sensitivity and specificity of plain films in this scenario have been described in the literature, the perception may be that initial plain films lead to more timely and cost-effective evaluation with lower radiation dosage. However, if plain films are truly an effective tool in screening for bone impactions, we should expect the time, cost, and radiation to be significantly different between the true positive and true negative patient populations. This is presumably the justification for screening patients with plain films: those without true bone impactions would be spared the subsequent confirmatory diagnostic workup. In this study, we hypothesize that the poor sensitivity of plain film necessitates further diagnostic evaluation (with CT or fiberoptic examinations) and thereby negates the potential reductions in time, cost, and radiation dosage. To answer this question, we sought to quantify (1) the accuracy of plain film and CT evaluations, respectively, and (2) if time, cost, or radiation dosage was reduced in the patients without true impactions.
Materials and Methods
We conducted a retrospective case series of patients who visited Tufts Medical Center (TMC), an academic level l trauma center adjacent to Boston’s Chinatown. Eligible patients were those 18 years and older who received a soft-tissue plain film of the neck due to a suspected fish or chicken bone ingestion, presenting to the hospital’s emergency department (ED) between March 1, 2009, and March 1, 2013.
Electronic charts (ED notes from Medhost, Plano, Texas, USA, and hospital notes from Soarian, Siemens, Washington, DC, USA) were accessed to ascertain demographics, presenting symptoms, management decisions, and outcomes, including age, gender, ethnicity, duration of impaction, length of ED stay (LOS), fish or chicken bone, any diagnostic tests in addition to the plain film (CT, chest x-ray [CXR], abdominal x-ray [KUB], fiberoptic exam [FOE], endoscopy), any consult services used (otolaryngology [ENT], gastroenterology [GI]), and extraction method (forceps in ED, endoscopy or laryngoscopy in operating room [OR]). Initial and final reads of diagnostic studies were compared, in addition to the time elapsed between and during imaging studies. After compiling the aforementioned data, radiation dosages and cost data were calculated for each patient.
Effective radiation doses for the various diagnostic imaging studies (plain film soft-tissue neck, CXR, CT soft-tissue neck, and KUB) were adapted from Mettler et al. 10 The estimated doses for each of the imaging studies are included in Table 1. Compounded doses from all modalities are displayed in millisieverts (mSv), which is defined as the radiation dose produced by 1 milligray (mGy) of radiation exposure. One mSv is defined in the SI system as the average accumulated background radiation dose to an individual for 1 year, exclusive of radon, in the United States. 10
Radiation Dose per Diagnostic Imaging Study.
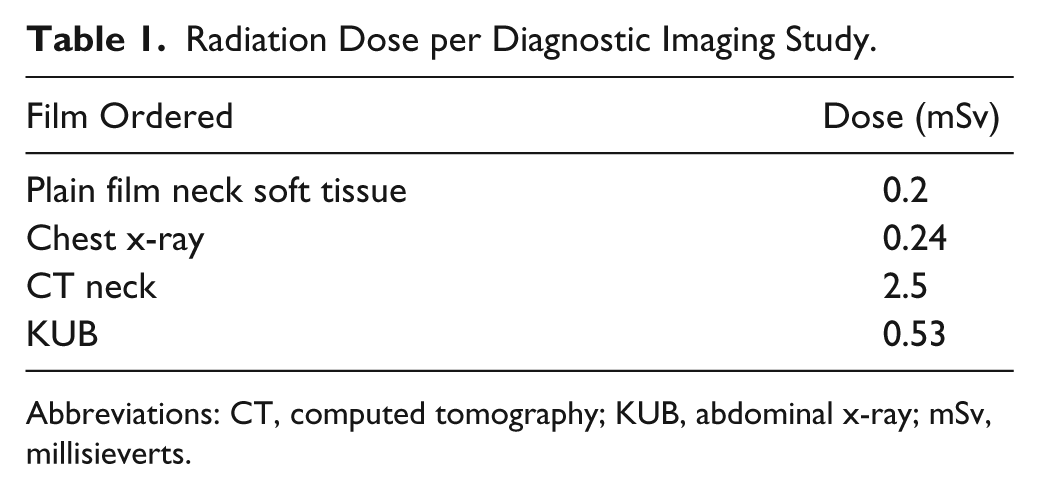
Abbreviations: CT, computed tomography; KUB, abdominal x-ray; mSv, millisieverts.
For this study, we sought to analyze the economic impact of each diagnostic approach. However, there is great variability within charges, reimbursements, and variable costs dependent on payers and the hospital. Medicare reimbursements, however, vary only by region. These reimbursements follow a strict schedule based on Current Procedural Terminology (CPT) code, which is a medical code designated for therapeutic and diagnostic procedures set by the American Medical Association (AMA). Thus, we assumed Medicare reimbursements for each patient as a standardized means of evaluating the costs to the health care system as it differs among imaging, intervention, and staffing. The AMA site was used to look up the current fee schedule of the various CPT codes assigned to the patient encounters in question. 11 Once a CPT code was identified for each consult (GI and/or ENT), imaging study (CXR, plain film neck, CT, KUB), and procedure (FOE, upper GI endoscopy), a cost estimate could be assigned (Table 2).
CPT Codes and Costs for Each Test/Procedure.
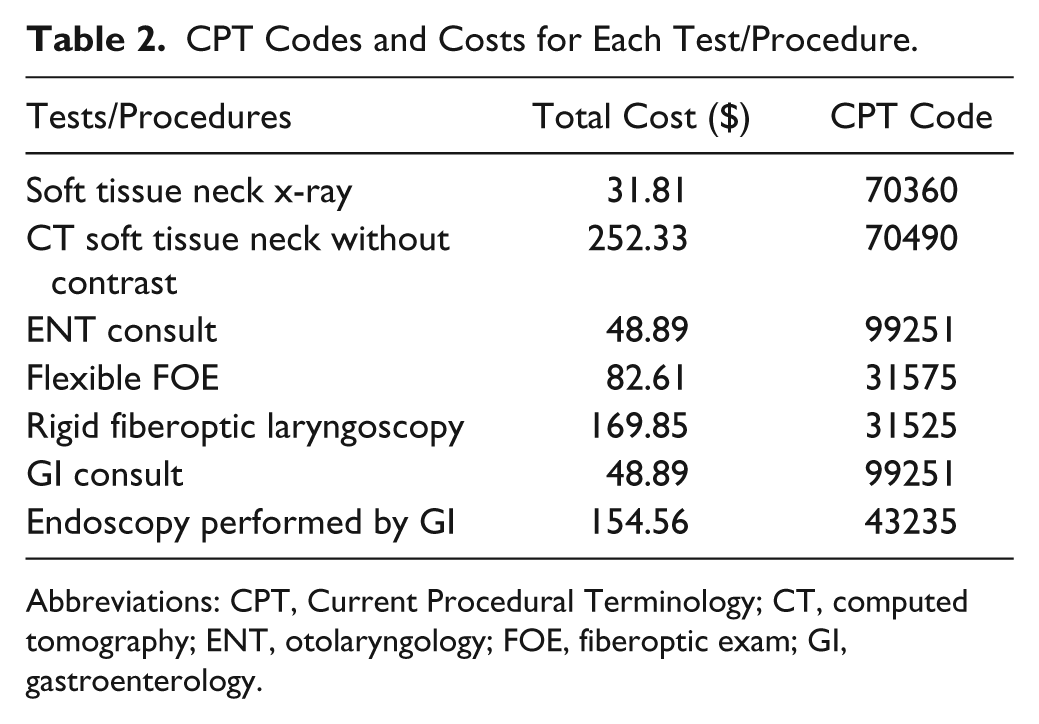
Abbreviations: CPT, Current Procedural Terminology; CT, computed tomography; ENT, otolaryngology; FOE, fiberoptic exam; GI, gastroenterology.
The CPT codes and their respective associated costs, however, do not take into account the costs associated with length of stay (ie, the overhead costs) in the ED. To quantify this value, we sought the direct and indirect variable costs to our ED. Existing fixed costs of any hospital (eg, CT scanner) would not change with management decisions because these costs have already been incurred, and therefore these costs were not included in our analysis. At TMC, the average total variable costs per ED patient visit for FY13 YTD April was $247.76. Using the most recent Press Ganey report on LOS averages in US EDs (4.17 hours), the average total variable costs were divided by the average LOS per ED patient visit, resulting in the total variable cost per hour in the ED ($60.18). This hourly variable cost was multiplied by the individual patient’s LOS (in hours) to get the individual total variable cost incurred. Finally, this cost component was added to the previous CPT code–related costs to arrive at the total cost incurred by each patient’s stay. This methodology followed guidelines set by the NIH Cost Analysis Methods. 12
The accuracy of each diagnostic modality (ie, plain film, FOE, or CT) was compared against whether the event was a “true positive” or “true negative.” The gold standard assessment of a foreign body would be a direct laryngoscopy under general anesthesia in the operating room. However, this procedure is unwarranted in most situations, especially when foreign body is removed in the ED with using direct observation or flexible laryngoscopy guidance. Thus, in our study in certain scenarios the true positive and negative events were determined by a combination of clinical outcome and image-guided diagnostics.
All of the aforementioned data were compiled in order to view differences in LOS, cost, radiation dose, and outcomes based on diagnostic and therapeutic management decision. The initial plain film or CT review represented the read by the ED physician and any consulting services. In our ED, if the patient has since become asymptomatic and the initial CT is negative, the patient will typically not receive further workup. This read may be confirmed by an on-call radiologist attending if requested. The final plain film or CT review represents the read confirmed by an attending radiologist, which can occur the following day.
Data Analysis
Data analysis was performed using SAS 9.3 (SAS Institute, Cary, North Carolina, USA). Differences in demographic and clinical characteristics (Table 3) of the sample were described using frequencies and proportions for categorical variables and means and standard deviations for continuous variables. The sensitivity and specificity of plain film and CT reads (both initial and final reviews) were calculated, along with exact 95% confidence intervals.
Mean Demographic and Clinical Characteristics of Patient Sample. a
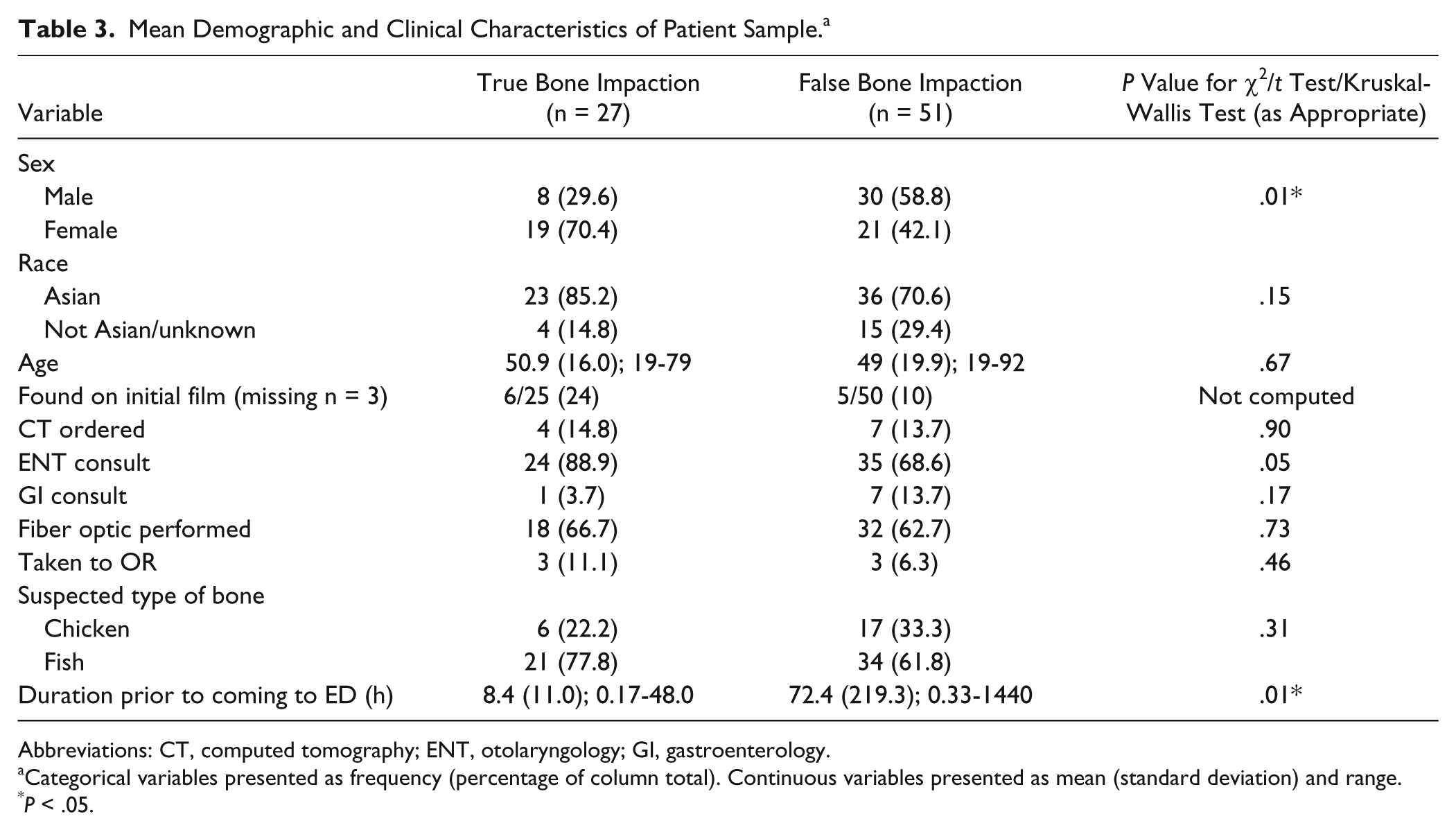
Abbreviations: CT, computed tomography; ENT, otolaryngology; GI, gastroenterology.
Categorical variables presented as frequency (percentage of column total). Continuous variables presented as mean (standard deviation) and range.
P < .05.
While this study was not powered to detect significant group differences, preliminary statistical tests were performed on these groups to help guide subsequent studies. Differences in categorical variables were examined via chi-square tests and odds ratios for categorical variables and either t tests or Kruskal-Wallis tests for continuous variables, depending on the skew of their distributions. All statistical testing was 2-sided with α = 0.05.
Results
Eighty-four patient visits met the inclusion criteria. From the original pool of entries, 4 were excluded: 2 patients had left against medical advice before being seen by ENT, 1 patient was found to have a “pork-chop bone” rather than fish or chicken, and the final entry was excluded because the same patient presented to the ED twice within a 48-hour period. Two of the remaining patients had other foreign bodies in addition to fish or chicken bones and were excluded: 1 had metal bristles from a grill brush, and 1 had a wooden splinter from a chopstick. Of the final 78 patients evaluated for fish or chicken bone impactions, 27 were true positives and 51 were true negatives. The selection of patients in this study is summarized in Figure 1.
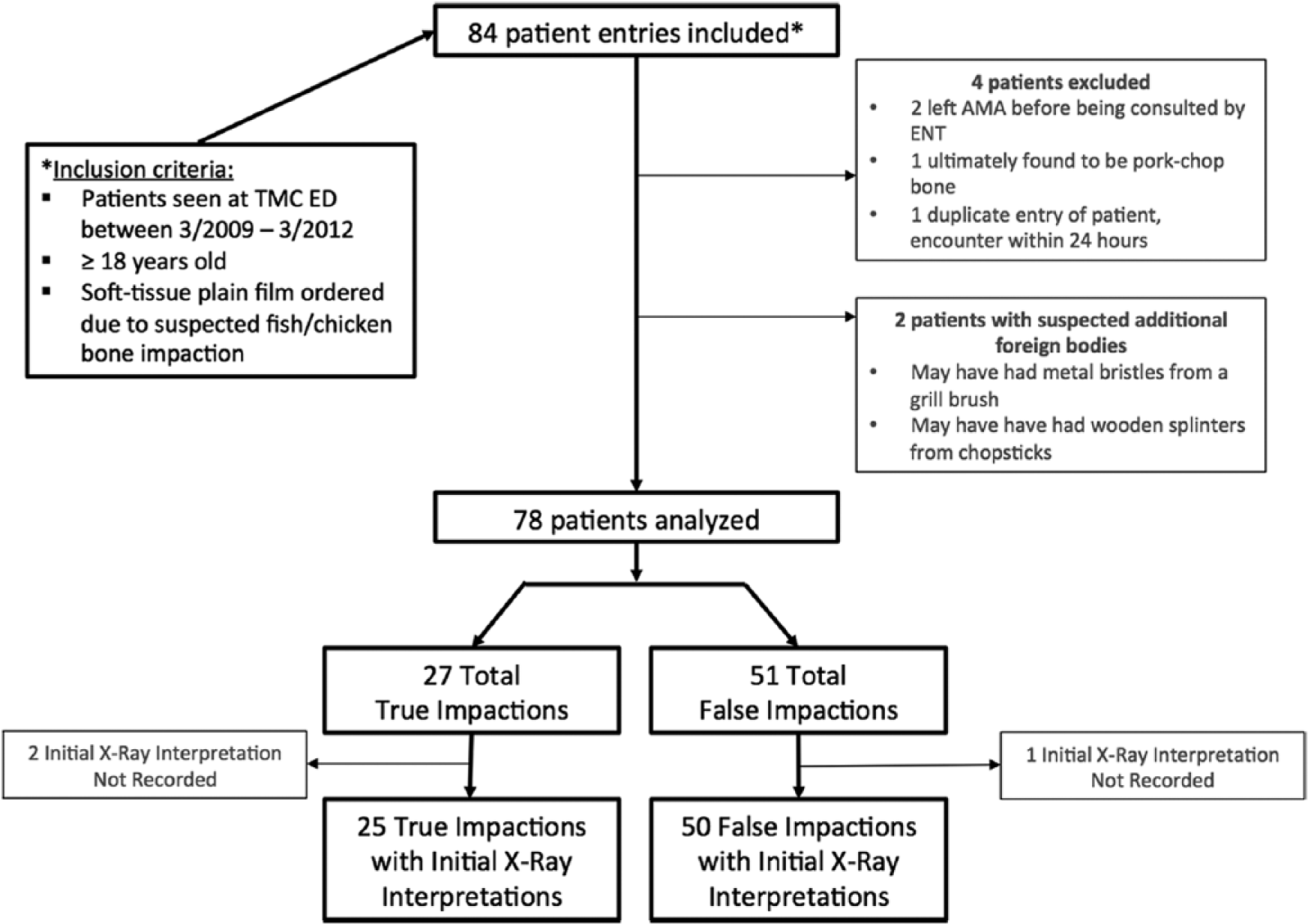
Flow chart of patient selection.
Table 3 highlights the demographic and clinical data that were obtained during this study. Fifty-five of the patients were evaluated for suspected fish bone impactions and 23 for chicken bone impactions. Of note, the majority of the patients in whom a bone was ultimately found were female (70%), odds ratio (OR) = 3.4 (95% CI, 1.3-9.2; P = .014). Asian patients comprised 87.3% of fish bone impaction cases and 47.8% of chicken bone impactions. Furthermore, patients without bone impaction had a longer duration of symptoms prior to ED presentation (72.4 hours) versus those who were ultimately found to have a bone impaction (8.4 hours); P = .01. The most common presenting symptoms were odynophagia and foreign body sensation (Figure 2).
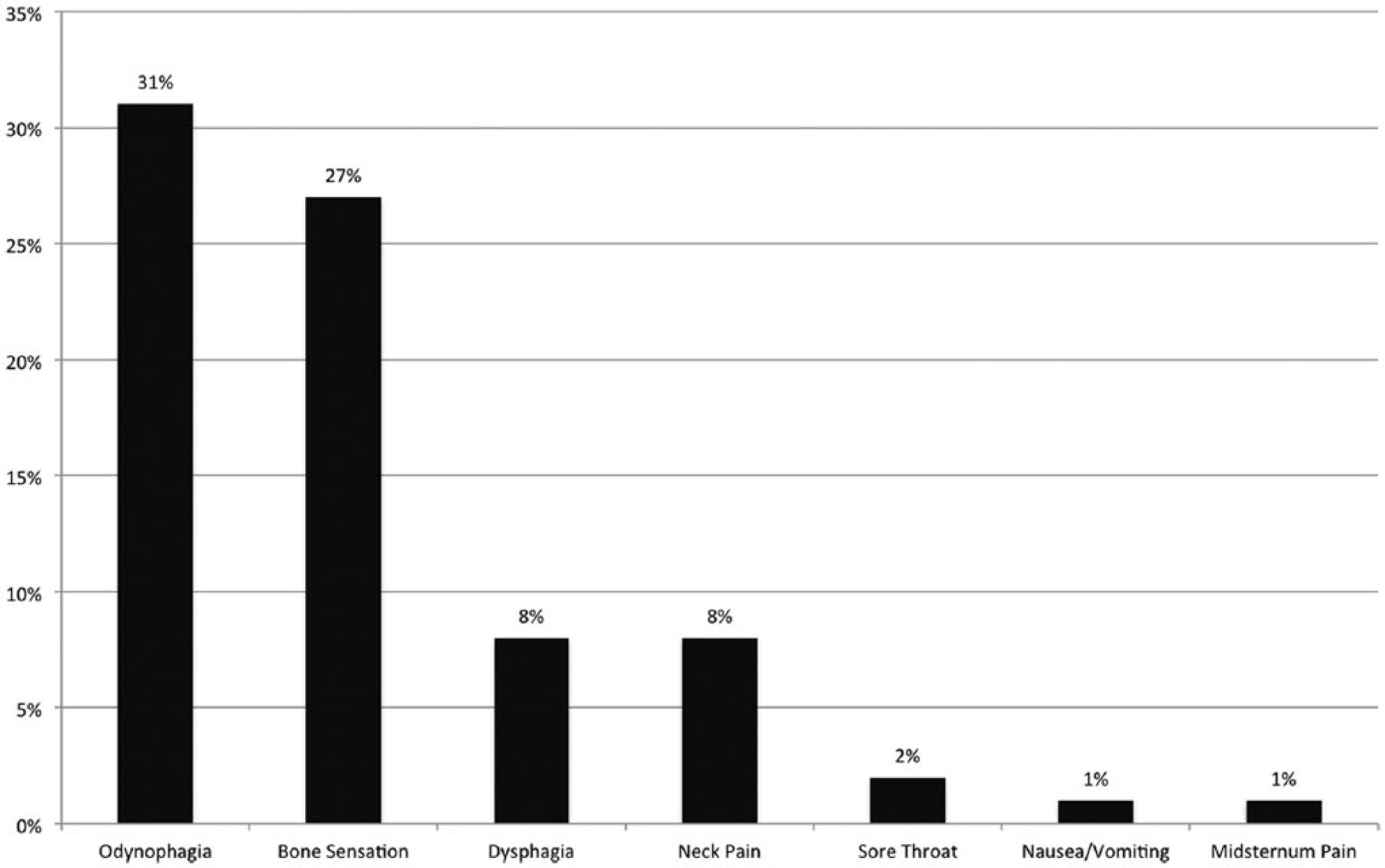
Frequency of presenting symptoms. Y-axis indicates frequency; X-axis, presenting symptom.
Initial plain film interpretations could not be found for 2 of the 27 true bone impactions and 1 of the 51 patients without true impaction (Figure 1). All other final plain film reads and initial/final CT reads were available within electronic medical records (EMR). Of initial plain films, only 6 of the 25 true bone impactions were classified as such on plain film read in the ED, a sensitivity of 24.0% (95% CI, 9.4%-45.1%). Forty-five of the 50 initial plain film interpretations correctly concluded absence of bone impactions among patients without true impactions, a specificity of 90.0% (95% CI, 78.2%-96.7%). Final plain film sensitivity and specificity showed only moderate improvement compared to initial interpretations. For initial CT reviewed in the ED, sensitivity was 75.0% (95% CI, 19.4%-99.4%), and specificity was 100% (95% CI, 59.0%-100%). CT determinations of bone impactions resulted from direct identification on imaging, rather than observation of indirect signs, such as edema or free air. The sensitivity and specificity of plain film and CT interpretations, respectively, are represented graphically in Figure 3.
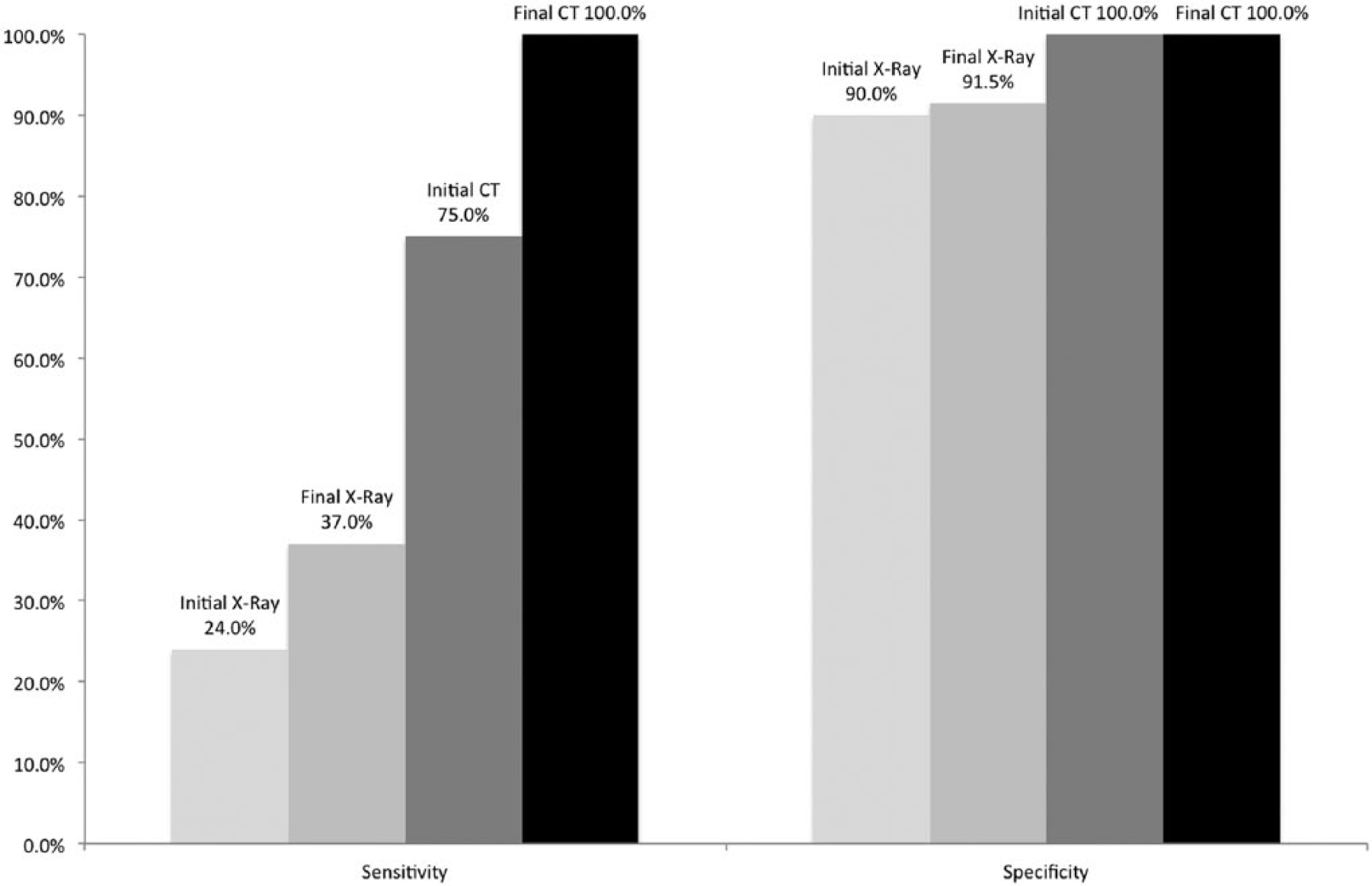
Accuracy of diagnostic imaging. Y-axis indicates percentage; X-axis, diagnostic evaluation (initial and final).
The system outcome measures of each patient visit were determined to be the ED LOS, hospital costs, and radiation dose received, none of which demonstrated statistically significant differences between patients with true bone impactions and those without (Table 4). The mean ED LOS for patients with true bone impactions was 4.2 ± 2.1 hours versus 4.3 ± 3.2 hours in patients without true impaction (P = .75). Similarly, the cost of patient visit to the hospital was $200.0 ± $178.4 for true bone impactions versus $209.8 ± in those without (P = .34). Finally, average radiation dose among patients with confirmed bone impactions was 0.58 mSv versus 0.56 mSv in those without (P = .93). These outcome measures are represented in Figure 4.
Patient Outcome Measurements Between True and False Bone Impactions. a

Outcome measures presented as mean (standard deviation) and range.
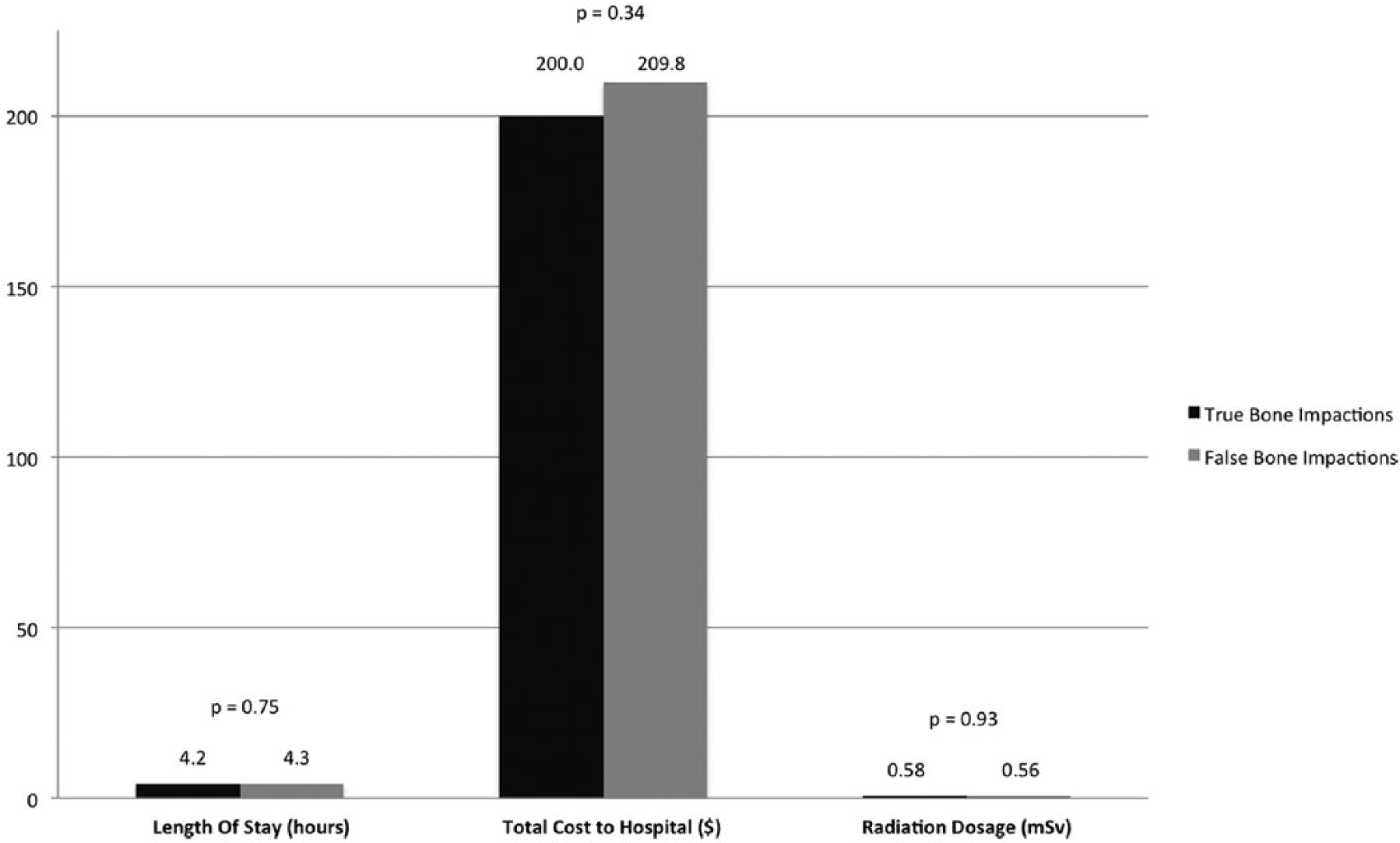
Outcome measures among true and false bone impactions. Among true and false fish bone/chicken bone impactions, no statistically significant differences were found when measuring emergency department length of stay (LOS; in hours), total cost to the hospital (in dollars, $), and radiation dosage (in mSv). None of the differences between groups were statistically significant. Dark shading indicates true bone impaction; light shading, false bone impaction.
Discussion
This study ultimately examined 78 patients presenting with concern for bone impactions who received an initial plain film evaluation. The majority of patients in this study presented to the ED with a concern for fish bone impaction (71%), as opposed to chicken bone (29%). This would be expected given TMC’s proximity to the Boston’s Chinatown, where many Asian cuisines incorporate fish and often include small, imperceptible fish bones. Indeed, the majority (87.3%) of fish bone patients were Asian, compared to a more heterogeneous ethnic distribution among those who presented with chicken bone impaction. In addition, the majority of patients presented with odynophagia and foreign body sensation, which is consistent with previous studies of fish or chicken bone impaction. 4
The finding that patients without bone impaction had a longer duration of symptoms prior to ED presentation than those with bone impaction likely demonstrates the more acute nature of true bone impactions. While imaging remains the mainstay of evaluation, further studies could quantify the utility of gestation period and duration of symptoms in determining true versus false bone impactions.
The sensitivity of plain film was 24.0% on final read by radiologist with specificity of 90%. This is consistent with many prior studies, demonstrating that plain film is a poor diagnostic tool for the initial evaluation of fish bone or chicken bone impaction. 6 Our analysis of initial CT read was limited by the low number of patients for whom this was performed; however, sensitivity in our center was 75% and specificity was 100%. The low numbers of patients are reflective of our current practice in the ED in obtaining the initial plain film. The delay in interpretation of plain film along with ENT evaluation could lead to longer wait times in the eventual decision to obtain a CT.
Hospital costs and ED length of stay among the group of patients without a foreign body were comparable to those patients in whom a foreign body was present. This observation likely reflects the ambiguity of the plain film screen leading to further testing and delays in treatment. Obtaining an initial CT scan instead could shorten the duration of ED stay and reduce the costs to the hospital, particularly in the group without a bone actually present. A low-dose radiation protocol (fish bone/chicken bone CT without IV contrast) would occur immediately after the initial oral cavity exam by the emergency physician to assess whether the fish or chicken bone is easily accessible within the tonsils, and so on. With expeditious CT evaluations, a patient would know whether a foreign body is present, and if negative, the patient would be spared a fiberoptic exam, the expense of consultations, and a lengthy ED stay.
While imaging studies add to the cost of patient care, radiation dose itself must be examined to ensure long-term patient safety. 13 The ideal diagnostic algorithm minimizes length of stay, cost, and radiation dosage while optimizing outcomes.
Radiation dose did not differ between patients with and without fish or chicken bones present (P = .93). This might simply point to the use of imaging studies as a screening tool for all suspected bone impactions.
Radiation dosage findings may play a larger role in our upcoming prospective study, which determines the effectiveness and system utilization of an initial CT screen in the management of suspected bone impactions. Based on the results of this study and the reported sensitivity of MDCTs, 9 we hypothesize that a low-dose radiation protocol MDCT would serve as a highly sensitive screening tool and obviate the need for further imaging studies, direct visualization, and the associated time delay and cost.
Conclusion
This is a pilot study to obtain information on current management of fish and chicken bone impaction in patients presenting to an emergency department. The aim of the study was to identify the lack of clinical and cost benefits offered by plain film screening of suspected bone impactions. A robust screening tool should not only help rule out the disease in question but also spare the true negative patients from further workup, costs, and radiation exposure. In this study, not only did the initial plain films demonstrate poor sensitivity, the system outcome measures (ED LOS, hospital costs, and patient radiation dose) all failed to show statistical difference between the true bone impactions versus patients without. While the poor sensitivity of soft-tissue plain films in evaluating bone impactions has been previously described, this study shows that initial x-rays fail as a diagnostic screening tool from a systems perspective as well.
The variable cost and radiation of CT evaluation is greater than that of soft-tissue plain film but also results in higher specificity and sensitivity. If a low-radiation dose CT screen for bone impactions is implemented, true positive patients could receive more expeditious treatment while true negative patients would be identified earlier, helping them avoid multiple radiation exposures and prolonged length of stay. Further studies should be performed to quantify how a low radiation CT screen would affect patient outcome measures and system utilization and cost.
Footnotes
Acknowledgements
The authors would like to thank Janis Breeze for the statistical analysis of our data, Dr Lindsey Lavoie and Dr Harprit Bedi for their help quantifying radiation exposures and dosages of common diagnostic modalities, and Dr Deeb Salem and Tracy Ryan for their help accessing hospital cost data and the expenditures associated with our patient population.
Authors’ Note
Please contact Karthik Devarajan (
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.