
Abstract
Objectives:
We describe a novel use of cortical auditory evoked potentials in the preoperative workup to determine ear candidacy for cochlear implantation.
Methods:
A 71-year-old male was evaluated who had a long-deafened right ear, had never worn a hearing aid in that ear, and relied heavily on use of a left-sided hearing aid. Electroencephalographic testing was performed using free field auditory stimulation of each ear independently with pure tones at 1000 and 2000 Hz at approximately 10 dB above pure-tone thresholds for each frequency and for each ear.
Results:
Mature cortical potentials were identified through auditory stimulation of the long-deafened ear. The patient underwent successful implantation of that ear. He experienced progressively improving aided pure-tone thresholds and binaural speech recognition benefit (AzBio score of 74%).
Conclusions:
Findings suggest that use of cortical auditory evoked potentials may serve a preoperative role in ear selection prior to cochlear implantation.
Introduction
Cortical auditory evoked potentials (CAEPs), typically measured in research settings, demonstrate responses of the auditory cortex to peripheral auditory stimulation. Mature CAEPs for adult, normal-hearing listeners consist of positive peaks—P1 (approximate latency 50 milliseconds) and P2 (150 milliseconds)—separated by a distinct negative N1 peak (100 milliseconds). These responses reflect activation along the thalamic-cortical pathway as well as within and surrounding the primary auditory cortex.1,2 Although much less is known about the effects of hearing loss on CAEPs, Oates and colleagues 3 demonstrated that amplitude measures tended to be highly variable in both adults with and without hearing loss. On the other hand, latencies of CAEP components were prolonged to a degree commensurate with the magnitude of hearing loss.
Assessment of CAEPs has been performed to track the cortical development of pediatric cochlear implant (CI) users as well as cortical plasticity in adults after implantation.4-9 Generally, experienced adult CI users demonstrate CAEP responses similar in morphology and peak latencies when compared with normal-hearing listeners, although N1 peak amplitude may be reduced. 10 Earlier P2 peak latency and greater N1-P2 amplitudes have been associated with better speech recognition.11,12
Previous studies, however, were conducted in patients who had already received CIs. It may be possible to use CAEPs to indicate the state of the auditory cortex for patients who are potential candidates for CIs. Here, we report the novel use of CAEPs to select a candidate ear for implantation in an adult with a long duration of hearing loss.
Materials and Methods
A 71-year-old male with bilateral hearing loss presented to The Ohio State University for CI candidacy evaluation. He was diagnosed with hearing loss at age 3 years but likely had congenital loss. He had worn a hearing aid (HA) in the left ear since the age of 6 years and had learned to rely solely on that ear, with subsequent progression of left-sided hearing loss. His language development as a child was entirely oral/aural in a mainstream setting. He had never worn an HA in the right ear due to the severity of his hearing loss in that ear. The patient expressed interest only in a right CI, in order to maintain use of his left HA, on which he relied heavily.
Audiometry confirmed bilateral severe-to-profound sensorineural hearing loss, worse on the right (Figure 1). Air-conduction pure tone averages (500, 1000, 2000, and 3000 Hz) were 92 dB HL in the right and 88 dB HL in the left ear. His CNC word recognition scores were 0% in the right and 28% in the left. The patient’s best-aided sentence recognition scores using AzBio sentences in quiet were 0% (right ear only), 24% (left ear only), and 20% (binaural best-aided condition).
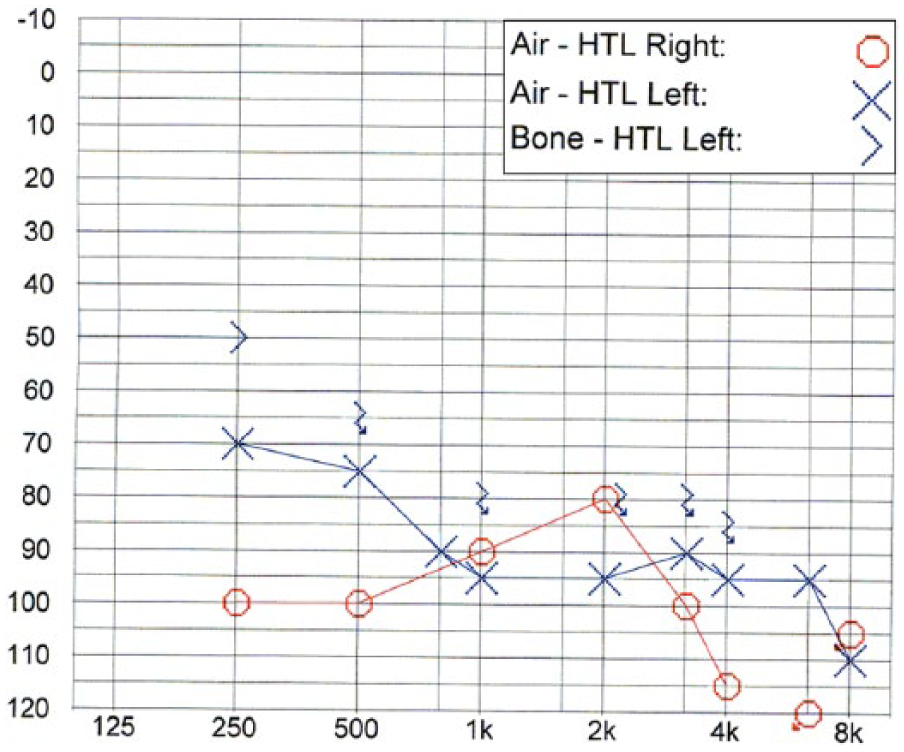
Patient’s preoperative pure tone audiogram.
The clinical concern was whether the patient would benefit from implantation of his right ear, which had profound hearing loss, unaided for over 70 years. It was thought that CAEPs might provide useful supporting information regarding the integrity of the entire auditory pathway to the cortex. The hypothesis was that if auditory stimulation of the right ear resulted in relatively normal CAEP morphology, this would suggest that the auditory pathways were intact and somewhat functional. If no CAEP responses were identified, this could suggest that those auditory pathways were nonfunctional and/or that the auditory cortex had undergone cross-modal plastic changes. When deprived of auditory stimulation for a prolonged period of time, the auditory cortex is usurped by other sensory modalities, usually visual. 13 More extensive cross-modal changes of the auditory cortex are related to poorer outcomes for pediatric CI users. 13 In our patient’s case, a lack of CAEPs on stimulation of the right ear might suggest that implantation of that ear would likely result in a poor outcome.
The patient underwent CAEP assessment, with free field auditory stimulation of each ear independently with the contralateral ear plugged. Free field stimulation was used to avoid vibrotactile responses from using earphones. Plugging the contralateral ear was done to avoid cross-stimulation as much as possible; masking the contralateral ear could not be done because it would affect CAEP responses. Electroencephalographic testing was performed during a passive auditory task involving presentation of pure tones at 1000 and 2000 Hz. Stimuli were presented at approximately 10 dB above the patient’s clinically measured unaided pure-tone threshold for each frequency and for each ear. See Supplemental Digital Content in the online journal for information regarding the CAEP testing protocol.
Results
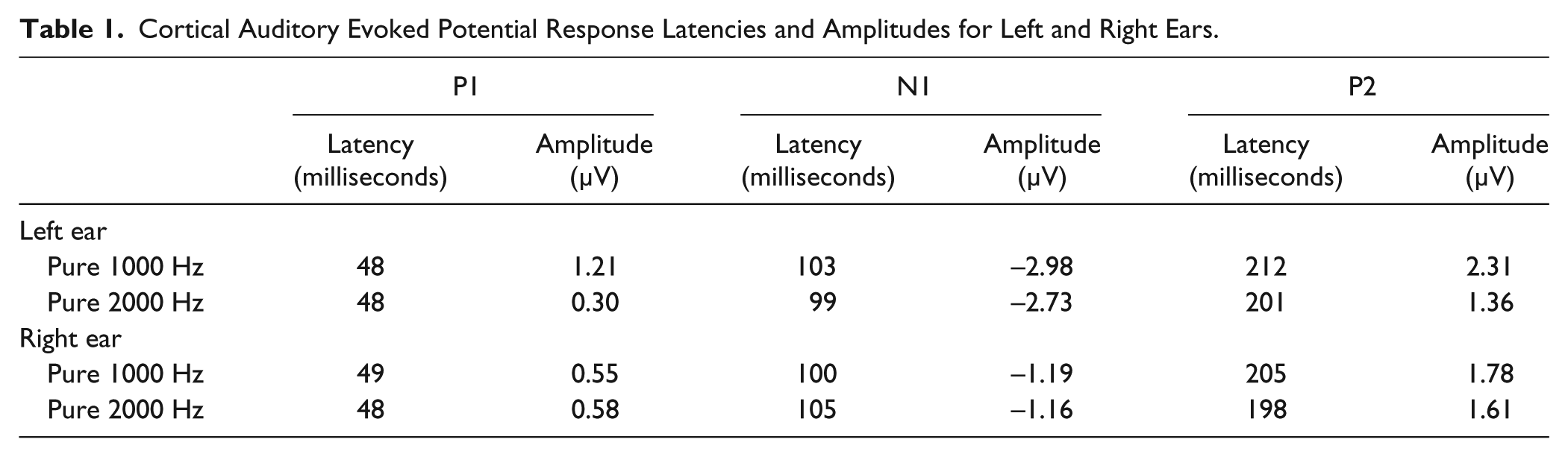
The patient’s CAEPs upon stimulation of the left ear had normal morphology, with distinct P1, N1, and P2 peaks at latencies of 60, 90, and 180 milliseconds, respectively (Figure 2). The CAEPs from the right ear also had normal P1, N1, and P2 peak latencies, although lower response amplitudes were identified relative to the left ear. Response latencies and amplitudes are listed in Table 1.
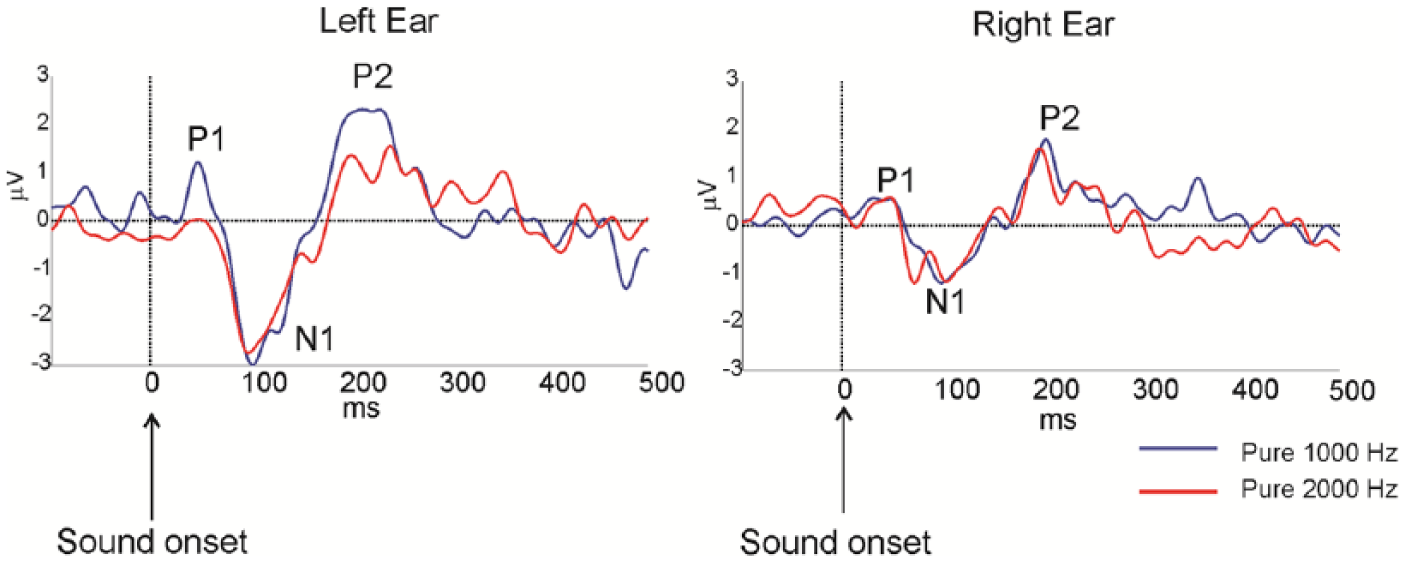
Patient’s cortical auditory evoked potentials preoperatively, recorded at the vertex channel (Cz).
Cortical Auditory Evoked Potential Response Latencies and Amplitudes for Left and Right Ears.
Because relatively mature CAEPs were identified, the patient underwent implantation of the right ear, using an Advanced Bionics device. Following implantation, the patient engaged in extensive aural rehabilitation over 6 months, including use of computerized auditory training as well as speech tracking with a speech-language pathologist. He noted continuous, gradual improvement in binaural hearing in the bimodal condition. Audiometric testing at 1 year post implantation revealed that his right ear CI-aided pure tone average had improved to 37 dB HL, from 60 dB HL at initial stimulation. Aided AzBio sentence scores in quiet at this time were 0% on the right (CI), 58% on the left (HA), and 74% in the binaural condition.
Discussion
The use of CAEPs in patients with CIs has mostly examined the cortical development of children, with P1 latency serving as a biomarker for development of the auditory cortex. 3 Newborns with normal hearing typically demonstrate P1 latencies of 300 milliseconds, shortening to 60 milliseconds by adulthood. Assessment of CAEPs has been used in children with cochlear nerve deficiency to determine if they would benefit from implantation. 14 To our knowledge, CAEP measurements have not been used preoperatively in adult CI candidates.
In this case, CAEPs were used in an elderly adult patient with congenital hearing loss. This patient continued to receive subjective benefit from his left HA and did not want to risk loss of that residual hearing. Thus, the question arose as to whether he would likely benefit from a right CI, which had never been aided, leading to doubts as to whether the auditory cortex would show mature activity. The central auditory pathways are highly plastic during the first few years of life and require stimulation to develop normally. 9 Our patient’s CAEP waveforms surprisingly showed similar peak latencies bilaterally, despite the right ear never having been aided. This suggests that his early right ear hearing loss was not so severe as to preclude relatively normal maturation and that cross-modal plastic cortical changes had not occurred sufficiently to result in a loss of CAEPs. We interpreted findings to suggest that a right CI might be beneficial.
Interestingly, while the patient did receive CI benefit when listening in the binaural aided condition (74% with both HA and CI, vs 58% in the HA-only condition), his speech recognition score was still 0% with CI alone. This may have been a result of the CI delivering speech cues that supported speech recognition in the binaural but not monaural condition. Regardless, the finding that the patient’s monaural speech recognition using his CI was still 0% suggests that CAEPs, at least when measured using this protocol, cannot tell us much about an individual’s likely ability to recognize speech through an implant. However, this is not surprising, as the CAEP responses primarily arise from the primary and nonprimary auditory cortex while understanding speech involves higher level auditory regions and the speech-motor cortex. Also, our patient was 71 years old at the time of testing and implantation. Elderly individuals probably experience less extensive and slower neuroplastic adaptation than younger individuals after implantation, which has been evidenced by continued improvement for some elderly CI users beyond 2 years post implantation. 15
Preoperative CAEP findings from this case add to a small number of studies examining postoperative cortical potentials in adult CI users. McNeill et al 7 evaluated CAEPs on a 63-year-old male with right-sided unilateral hearing loss that went unaided, who developed sudden hearing loss on the left as an adult. This patient underwent implantation of the long-deaf ear. At 3 months postoperatively, CAEPs were present for the CI-only condition and progressively developed into more mature morphology by 12 months. Pelizzone et al 5 reported results of CAEP testing postoperatively for a patient with bilateral long-term deafness for more than 50 years. The patient underwent bilateral implantation, after which electrical stimulation elicited persistently abnormal responses 2 years postoperatively.
An interesting consideration for future studies of preoperative CAEP measurements is which measures to obtain. In this study, we examined P1-N1-P2 responses. However, these responses may primarily represent early “sensory” cortical processing, which may not be as affected by peripheral hearing loss as higher level “nonsensory” cortical processing. 3 Assessing higher level measures (eg, the P3 response) may provide greater information regarding the potential benefits of implantation of the tested ear.
Clearly, strong conclusions cannot be made based on 1 patient, and even deducing general principles regarding this patient should be done cautiously. In particular, in this single patient, we could not statistically compare the amplitudes and latencies of CAEP responses between the patient’s 2 ears or between this patient and adults with normal hearing. Before collecting CAEPs for this patient, we discussed whether or not results would change our management since we could not assume that we were correct in recommending implantation only if CAEPs were relatively normal in that ear. We can conclude, however, that in the binaural condition, the patient did receive benefit to speech recognition. It is likely that this binaural improvement was optimized by intensive postoperative aural rehabilitation.
Conclusion
Cortical auditory evoked potentials are a potential tool for assessment of CI candidacy and ear selection in adults. An ear that has not received auditory stimulation for decades may elicit a relatively mature CAEP waveform, suggesting that benefit may result from implantation. Further studies are needed to examine CAEP responses preoperatively in additional CI candidates to determine how amplitude and latency characteristics of these responses relate to postoperative speech recognition outcomes.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Work described in this manuscript was supported by R03-DC011168 from NIDCD awarded to Antoine J. Shahin.