
Abstract
Objectives:
Nasal irrigation is standard in the management of chronic rhinosinusitis both before and after surgical intervention. Numerous irrigation devices are commercially available. The aim of this study was to compare the efficacy of a handheld pulse irrigation device against the gold standard manual squeeze bottle after endoscopic sinus surgery (ESS).
Methods:
Five cadaveric specimens were prepared with video visualization ports into each sinus. Endoscopic sinus surgery was performed on each cadaver from minimal to maximal dissection. Sinuses were irrigated with fluorescein solution using both devices following each dissection. The irrigations were video recorded. A blinded independent observer scored each irrigation according to a defined scale.
Results:
Comparison of the 2 devices using an intraclass correlation coefficient (ICC = 0.39) showed the 2 systems differed. Observation of individual sinuses showed the squeeze bottle consistently provided greater irrigation in the maxillary (P < .006), frontal (P < .0001), and sphenoid (P < .0001) sinuses. Pulse irrigation improved only in the maxillary sinus following ESS.
Conclusion:
The squeeze bottle consistently demonstrated superior irrigation in both native and operated conditions. Interestingly, saline penetration was not significantly improved after opening of the frontal and sphenoid sinuses. This is likely due to decreased backpressure in the nasal passage after opening the sinus cavities.
Introduction
Nasal irrigation is standard practice in the medical therapy of chronic rhinosinusitis as both pre- and postsurgical intervention. In fact, irrigation has the highest evidence for any intervention performed for chronic sinusitis.1,2 Several different devices are currently used, and the existing data recommending a particular device are minimal. Thus far, there is evidence that the standard squeeze bottle is superior to other methods.3,4 There has been concern that these bottles can be a harbinger of pathogens with continual reintroduction of bacteria into the sinonasal cavity 5 ; however, other reviews have failed to show any clinically significant outcomes.6-8
The motorized NeilMed Sinugator pulsating nasal wash (NeilMed Pharmaceuticals, Santa Barbara, California, USA) was developed as a relatively inexpensive, convenient device that has the benefit of streaming fluid at a constant volume and pressure independent of the subject’s effort. It has been shown to improve both symptom and endoscopic grading scores in patients with mild chronic rhinosinusitis that underwent endoscopic sinus surgery (ESS). 9 The device’s design minimizes backwash, 10 but the clinical significance of this observation is unclear. We sought to compare this relatively novel pulsating electric nasal irrigator to the traditional manual hand-squeezed bottle irrigator in terms of delivering irrigant into different sinuses of cadavers undergoing ESS.
Methodology
Surgical Dissection
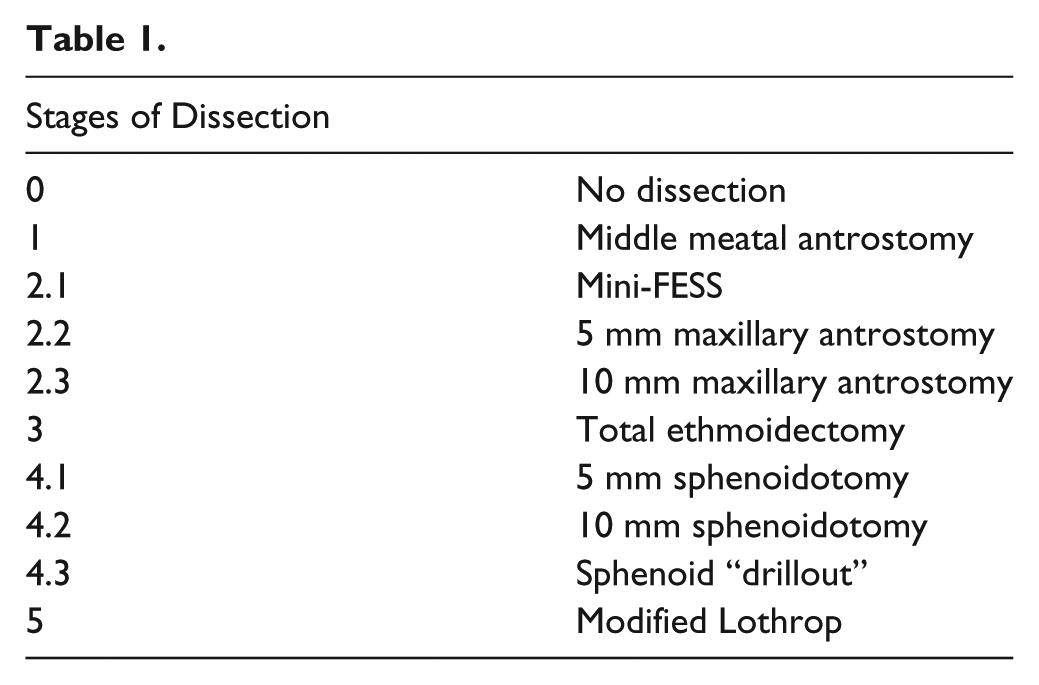
A formal request was approved for access to anatomical resources for the purposes of this research through the Head, School of Medical Sciences, The University of Adelaide. The anatomical resources are sourced from bodies donated through the statewide Body Donation Program operated by the School of Medical Sciences. Five thawed fresh-frozen human cadaver heads with the cranium and brain removed were used. Visualization ports for endoscopic evaluation sized 4.5 mm were created for each sinus with a handheld drill. Ports through the anterior table of the frontal sinus were completed 1.5 cm from the midline at the supraorbital rim to view the frontal sinus lumen. The maxillary sinuses were viewed through trephinations just below the infraorbital rim, and drilling through the planum sphenoidale allowed visualization inside the sphenoid sinus. All 5 specimens underwent stepwise endoscopic dissections by a single surgeon (P.G.C.), which ranged from undissected to “mini-FESS” (maxillary antrostomy with total ethmoidectomy) to maximal dissection with a modified endoscopic Lothrop procedure (Draf 3) and sphenoid “drillout” (removal of intersinus septum). Table 1 shows the progression of surgical dissection.
Data Collection
Measurement of irrigant penetration into each sinus was video recorded after each stage. Irrigant consisted of 0.1 ml 25% fluorescein in 1000 ml water, which was found to be the optimal concentration for adequate visualization of active flow without permanent staining of the mucosa after rinsing. Each cadaver head was situated with the nose facing 45° downward to simulate the position of actual usage. The saline reservoirs were filled completely, and each side of the nose was irrigated with a half bottle (120 ml) from each device. The Sinugator was inserted into the nostril, and the button was held until half the reservoir was used, then the remainder was used on the other side. Similarly, the rinse bottle was inserted and squeezed with constant manual pressure until the bottle was fully compressed, then immediately released, and pressure reapplied. The insertion and squeezing of the bottle was performed by a single investigator (P.G.C.), and all attempts were made to standardize this process in terms of bottle positioning and the amount and manner of manual force applied. A 30° angled endoscope placed within the port allowed viewing and recording of the irrigant penetration into the sinus ostium. The sinus cavity was emptied, rinsed with clean saline, and air dried before proceeding with the next irrigation. Two trials were performed on each side with each device, and flow through each sinus ostium was assessed after each stage of dissection.
Data Analysis
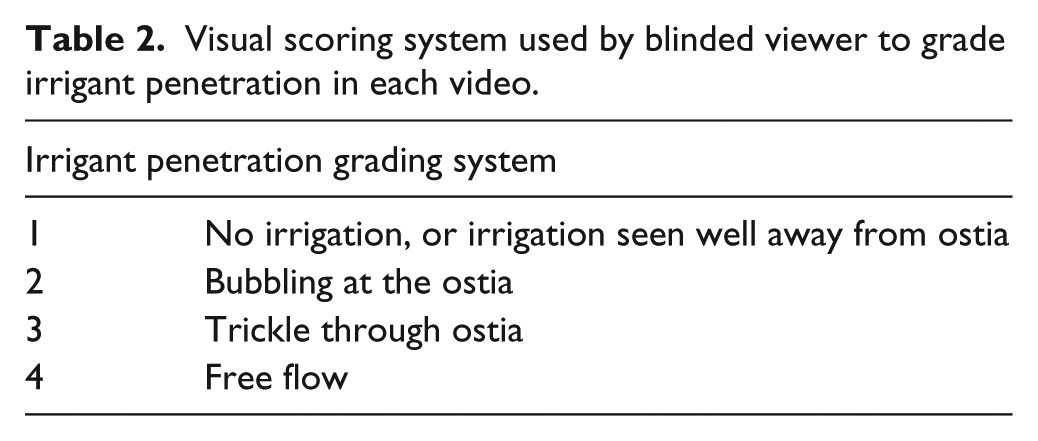
A single blinded reviewer (S.B.) assessed all videos in a random fashion. The amount of irrigant entering each sinus was recorded using an ordinal scale similar to one previously described 11 (Table 2). Analysis with a linear mixed effects model allowed comparison of each device in terms of saline penetration by sinus and stage of dissection.
Visual scoring system used by blinded viewer to grade irrigant penetration in each video.
Results
Agreement between the squeeze bottle and Sinugator methods of sinus irrigation was assessed using the intraclass correlation coefficient (ICC). The ICC was estimated from the covariance parameters of a linear mixed effects model to account for data clustered by head, sinus, side, and trial. 12 A kappa of <.40 is generally viewed as indicating poor agreement, while a kappa of .40 to .75 indicates fair to good agreement, and a kappa of >.75 indicates excellent agreement. Figures 1 through 3 demonstrate the irrigant penetration scores of each device for each sinus for progressive dissections, with brackets indicating standard deviation.
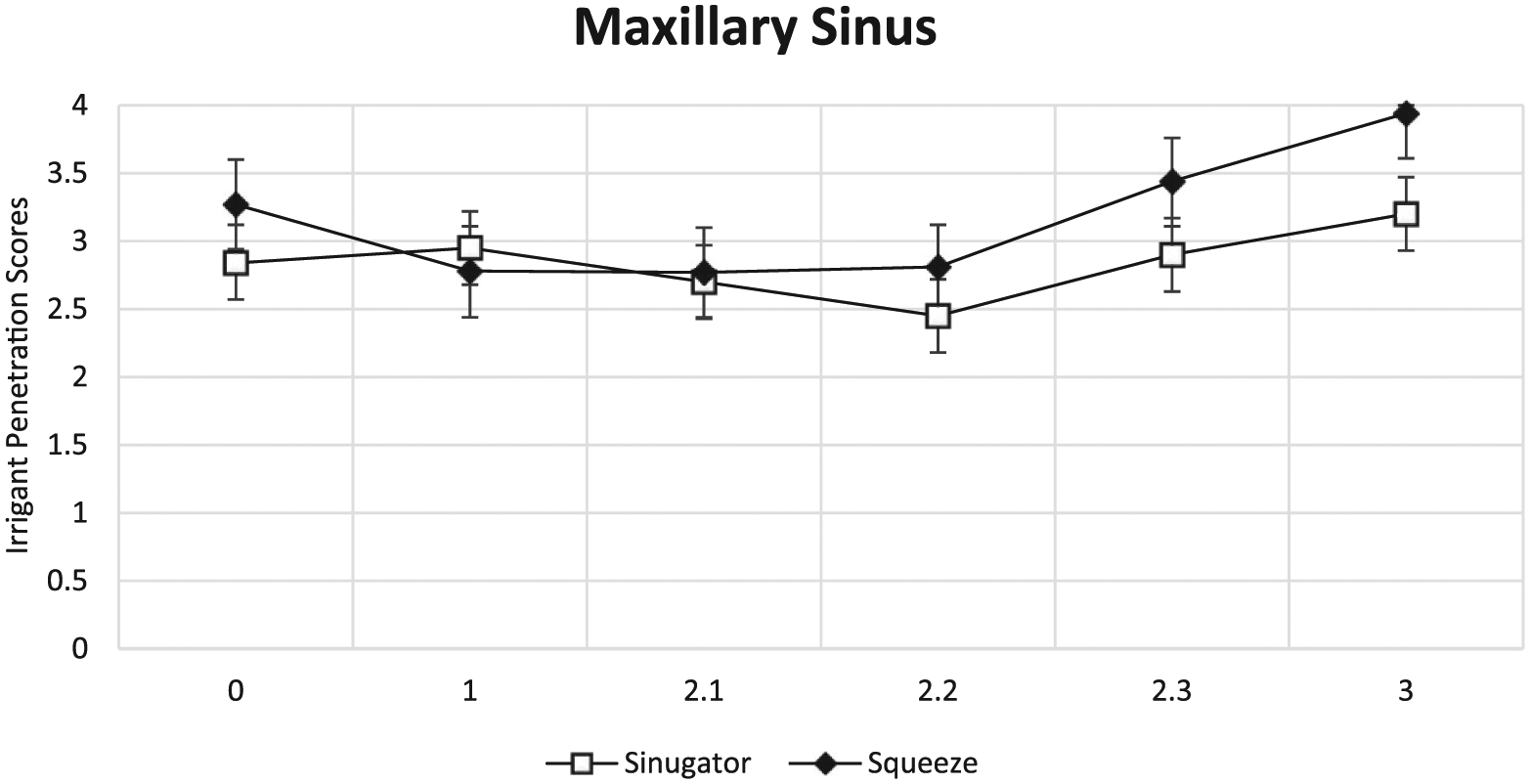
Maxillary sinus irrigant penetration visual scores with each progressive dissection for each device.
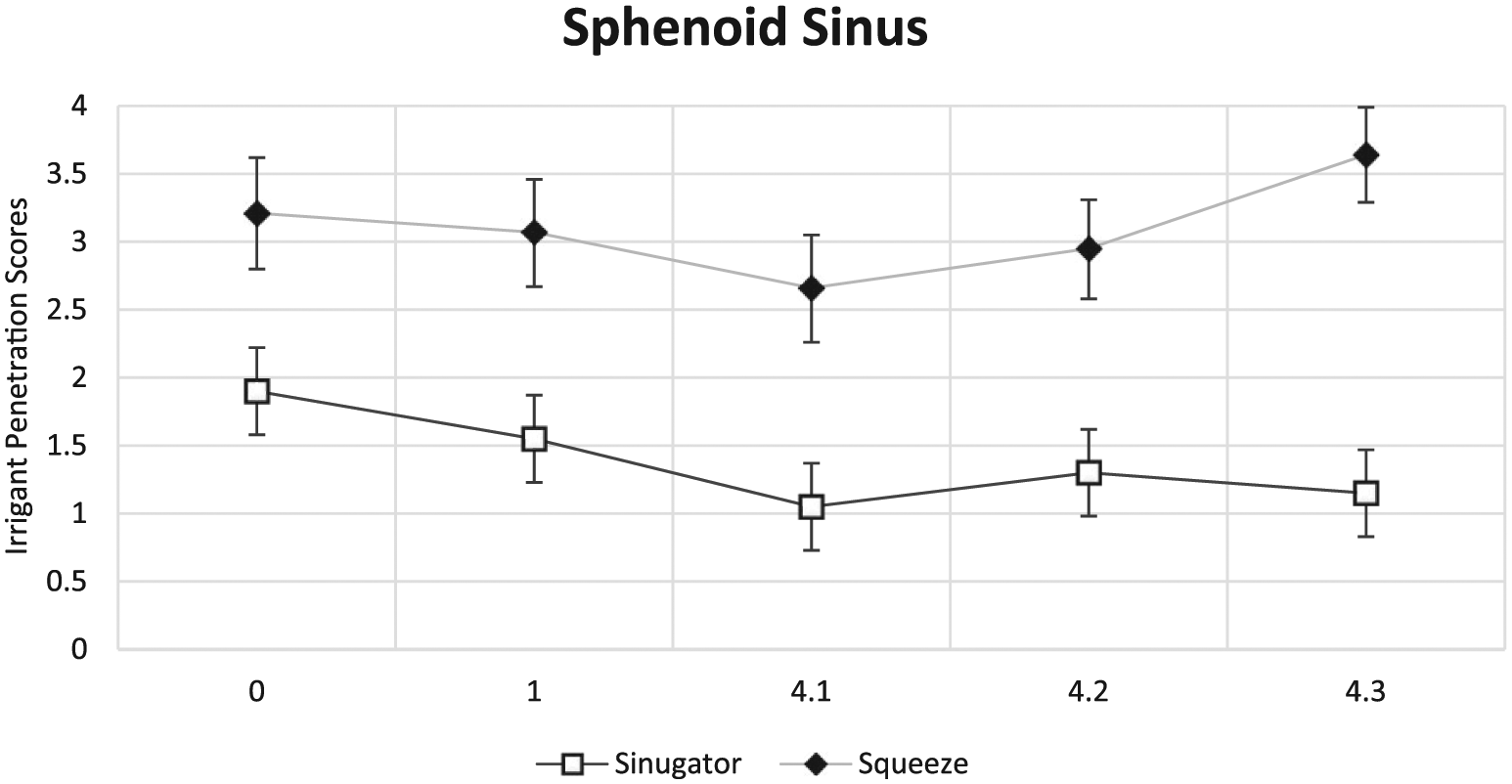
Sphenoid sinus irrigant penetration visual scores with each progressive dissection for each device.
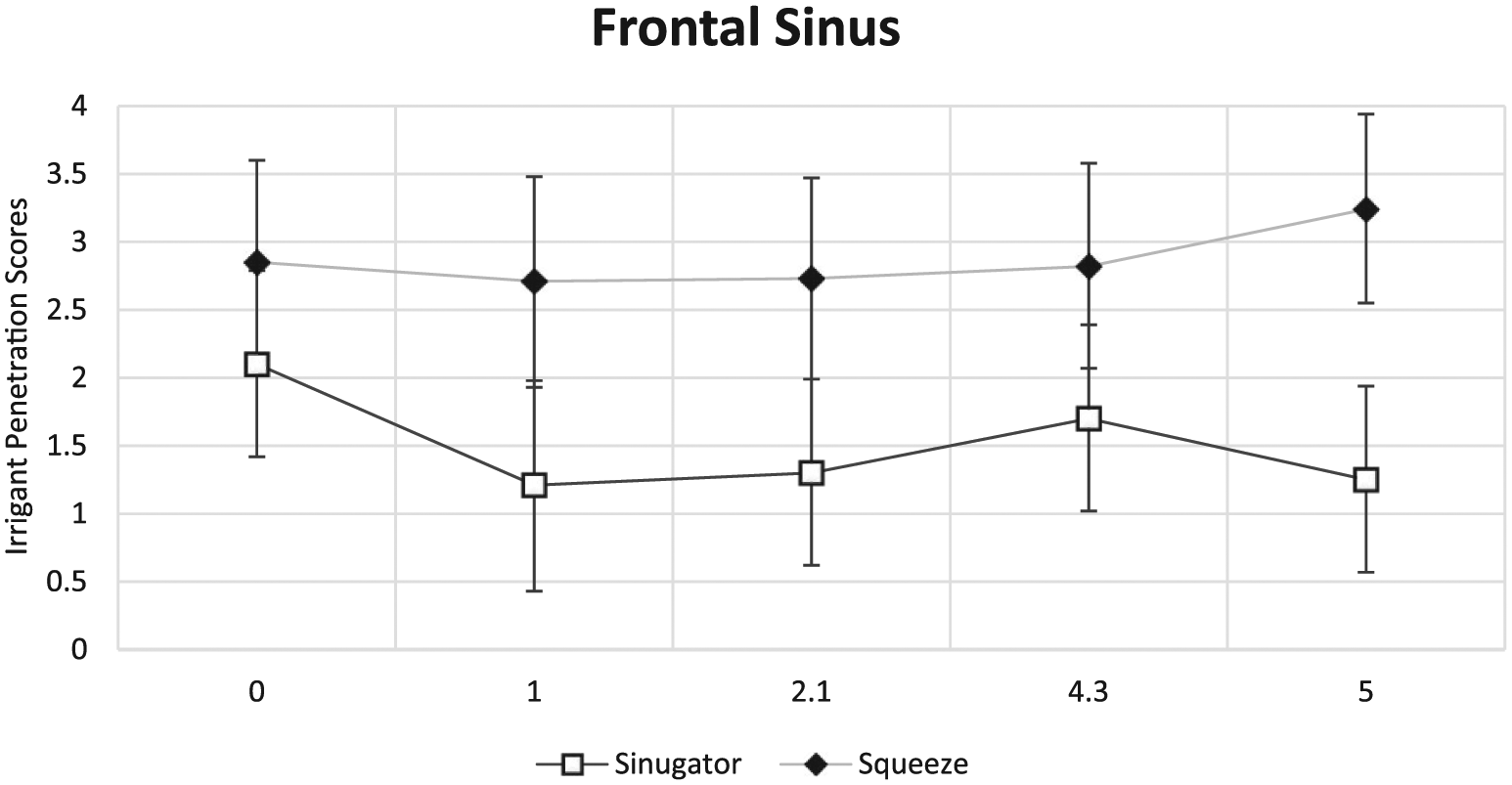
Frontal sinus irrigant penetration visual scores with each progressive dissection for each device.
Maxillary sinus analysis showed that overall the pulsatile device performed comparably to the squeeze bottle with a visual score mean difference of −0.33 (P < .006, 95% CI, −.051 to −0.14). At individual staged dissections of the maxillary sinus, the pulse irrigator again performed comparably to the manual squeeze bottle (visual score mean 3.2 vs 3.94, P = .0001) (Figure 1).
The pulsatile device also scored lower within the sphenoid sinus, demonstrating a mean visual score difference of −1.74 (P < .0001, 95% CI, −1.98 to −1.5). This was confirmed at individual stages of dissection including the native (visual score mean 1.9 vs 3.21, P < .0001) and fully dissected sphenoid sinus (visual score mean 1.15 vs 3.64, P < .0001) (Figure 2). The efficacy of pulsatile irrigation declined following sphenoid dissection with a mean difference of 0.75 from native to fully dissected (P = .0007, 95% CI, 0.32-1.18) (Figure 2).
The pulsatile irrigation also fared worse in the frontal sinus, with mean visual score difference of −1.38 when compared to the rinse bottle (P < .0001, 95% CI, −1.68 to −1.07). At each dissection stage, the squeeze bottle demonstrated significantly higher visual scores, including the modified Lothrop procedure (1.25 vs 3.24, P < .0001) (Figure 3).
Overall, the total outcome measures between the 2 devices showed a significant difference in irrigation visual scores with an ICC of 0.39 demonstrating poor agreement. Figure 4 shows the total mean visual outcomes of all trials at all stages of dissection for each location.
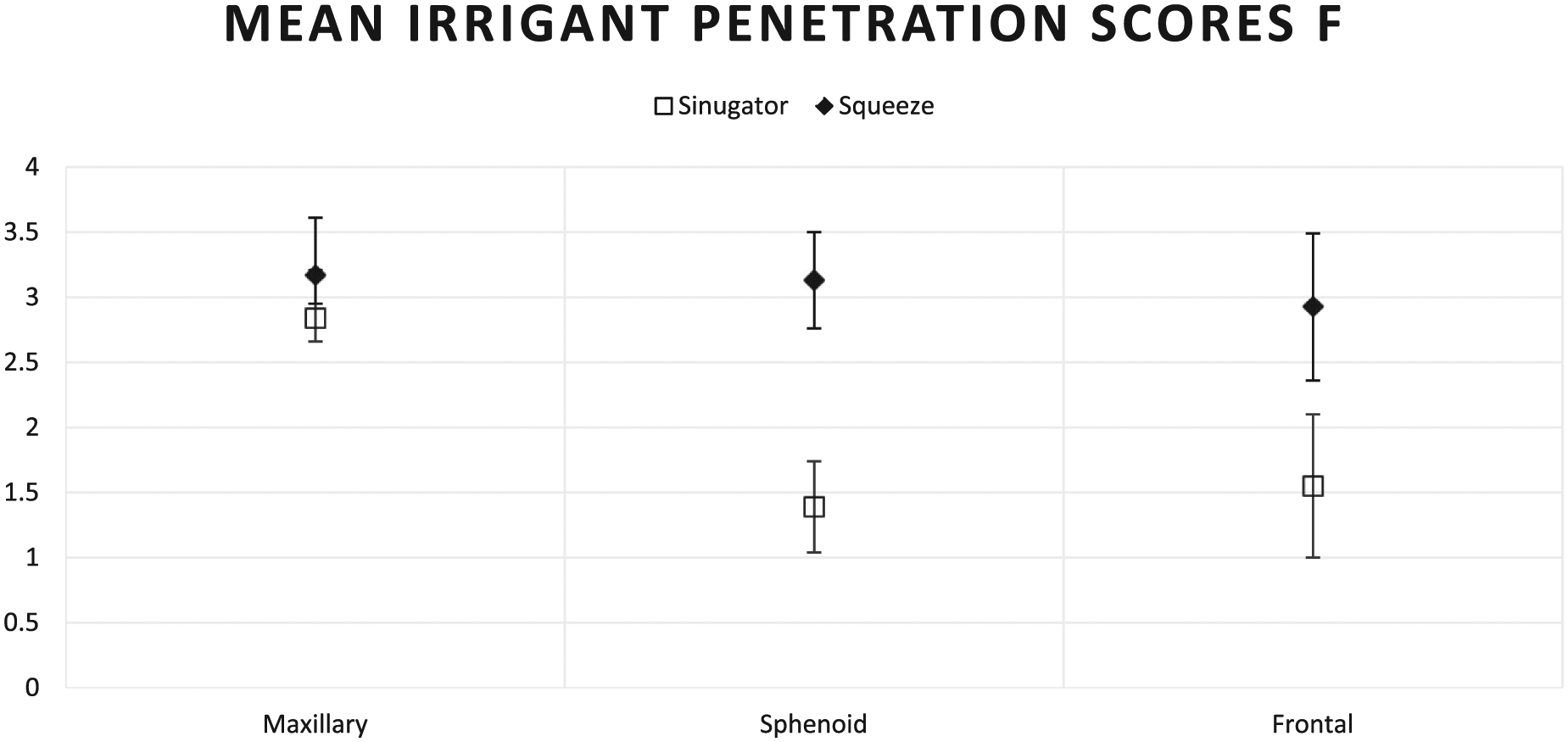
Total mean visual scores of all trials at all stages of dissection for each location.
Discussion
Nasal irrigation remains an integral and effective treatment for patients with rhinitis and chronic rhinosinusitis. It is also an effective means of maintaining nasal hygiene in the postoperative period after ESS. While there are a plethora of devices on the market with various claims of efficacy, most devices have not been thoroughly investigated.
Squeeze bottle devices are inexpensive and portable and are widely available at a multitude of stores and have proven to be effective.1,2 However, there are a number of patients who do not tolerate usage for various reasons. Anecdotally, a common reason is that the strength of irrigation can be perceived as too forceful, while others report otalgia from the irrigation entering the middle ear via the Eustachian tube.
Electronic irrigation devices with a power cord tend to be larger than squeeze bottles, which is a potential drawback for patients who travel often. In addition, the plug ensures the necessity for a power adapter when a patient travels internationally, which is just 1 more component that can negatively affect compliance. Further, these can be expensive. Nasal nebulizers are other available devices that are also costly and not easily portable. These devices may be used for drug delivery to the nasal mucosa, 13 but a review of the literature suggests that they are not as efficacious in this respect as irrigation.14,15
The Sinugator pulsatile irrigator performed similarly to the squeeze bottle with regards to the maxillary sinus but was not as effective in reaching the dissected frontal and sphenoid sinuses. Further, the ability to reach the frontal and sphenoid sinuses decreased as the extent of surgery increased. The most likely explanation for this finding is that dissection removes tissue and increases the volume of the nasal passage. The larger volume decreases the backpressure needed for the irrigation to successfully reach the frontal and sphenoid sinuses.
The positives for a motor-driven device sinus are that it may be useful for patients who have trouble squeezing a manual bottle, such as those with arthritis or carpal tunnel syndrome. The consistent pressure also removes variability often observed with manually squeezed bottles.
The main limitation of this study is that the findings in cadavers may not easily be applied to living patients, who could affect irrigant delivery by snorting, changing head positioning, or inserting/squeezing devices differently. Similarly, living patients with sinusitis could have polyps, edema, and/or secretions that could also affect results.
Conclusion
The Sinugator pulsatile irrigator performs similarly in the maxillary sinuses of patients with normal anatomy when compared to the traditional rinse bottle but distributes less irrigant to the sphenoid and frontal sinuses in both normal anatomy and operated states. This low-pressure pulsating irrigation device would be useful to patients with isolated maxillary sinus disease, nonoperated, and in those not able to tolerate a manual squeezable device.
Footnotes
Acknowledgements
We appreciate statistical support from the Department of Statistics, University of Adelaide, especially Mr Stuart Howell. We also acknowledge the hard work of the University of Adelaide School of Medical Sciences under the direction of Professor Robert Vink and the laboratory under Mr Wesley Fisk.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Peter-John Wormald, MD, receives royalties from Medtronic, Integra, and Scopis, and he is a consultant for NeilMed. The remaining authors have no conflicts or disclosures.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: NeilMed Pharmaceuticals, Inc, provided the irrigation devices and also supported procurement of study specimens. None of the sponsors or donors had any involvement in the study, including: design, performance, data collection, analysis, manuscript preparation, or decision to publish.