
Abstract
Objectives:
The effects of age-related hearing loss are severe. Early detection is essential for maximum benefit. However, most hearing-impaired adults delay obtaining treatment. Diagnostic hearing testing at an appropriate facility is impractical, and new methods for screening audiometry aim to provide easy access for patients and reliable outcomes. The purpose of this study was to examine the accuracy of application-based hearing screening in an elderly population.
Methods:
The uHear application was downloaded to an iPad. Application-based hearing screening was performed in a non-soundproofed quiet room, and subsequently all participants underwent full diagnostic audiometry in a soundproof booth.
Results:
Sixty patients were recruited and completed both tests. Significant differences were observed between the hearing results obtained with the application and the standard audiogram at all frequencies and in both ears. Following subtraction of a constant factor of 25 dB from the application-based results in order to compensate for ambient noise, no significant differences in pure tone average were found between the 2 methods.
Conclusions:
The uHear application is inaccurate in assessing hearing thresholds for screening in the elderly. However, when site-specifically corrected, the uHear application may be used as a screening tool for hearing loss in an elderly population.
Introduction
Age-related hearing loss (presbycusis) is the most prevalent sensory impairment in the elderly. Approximately 1 in 3 people between the ages of 65 and 74 suffer from some degree of age-related hearing loss (ARHL), and nearly half of those older than 75 have difficulty hearing. 1 Reported effects of ARHL include depression, anxiety, social withdrawal, cognitive decline, and difficulty focusing and communicating.2-6 The large longitudinal Epidemiology of Hearing Loss Study (1993-2000) demonstrated an association between the severity of hearing loss and reduced quality of life in older adults. 7 In a study of elderly male veterans, those suffering from hearing loss perceived the effects of this handicap as severe. 8 Early detection of ARHL and prompt treatment are essential for maximum benefit as the early use of hearing aids can reverse the adverse effects of hearing loss on the quality of life of elderly persons. 9 Early hearing aid users may have better eventual outcomes with amplification when compared to late hearing aid users, and plasticity effects may require less auditory retraining.10,11 However, most hearing-impaired adults delay obtaining professional help for their condition for more than 10 years after first recognizing that hearing loss is present. 12 Various initiatives around the world, including Healthy People 2020 by the US Department of Health and Human Services and AHEAD III by the European Commission Framework Program, address the public health need of improving the detection of hearing impairment and the accessibility and implementation of its treatment.13-16 Classical diagnostic audiometry involves a full diagnostic behavioral hearing test performed by a qualified audiologist at an appropriate facility. Most patients are referred for diagnostic audiometry by their primary care physician (PCP) following an office visit. However, expense and inconvenience make screening by this method impractical. Good-quality evidence supports screening tests to identify persons with hearing loss. Nevertheless, significant numbers of persons do not undergo audiometric evaluation. 17 Newly developed methods for screening audiometry such as telephone-based, Internet-based, and smartphone-based screening18,19 aim to provide easy access for patients and reliable outcomes. Although there have been advances in objective measurement methods using devices based on oto-acoustic emissions and auditory evoked responses, these are unsuitable for larger screening efforts since they require expensive equipment and trained personnel to administer the tests. 15 For this reason, simple inexpensive testing is preferable to advanced testing, at least for initial screening. Smartphone-based screening is particularly attractive because of the widespread penetration of mobile phones and cellular network reception globally.20,21 There are currently a number of smartphone and tablet computer applications available to conduct basic hearing assessments.19,22-25 One such application developed for Apple iOS devices (iPhone and iPad) called uHear (Unitron, Victoria, Canada) provides a self-directed assessment of air conduction hearing thresholds. 23 The application is user-friendly, simple to use, and can either be used by the PCP for initial screening or by the patient for screening by self-testing at home. The possible benefit from using such a screening tool is that it allows any PCP to obtain an on-the-spot initial diagnosis without additional referrals. This can save time and unnecessary referrals and promote early detection and treatment of hearing disability. The purpose of this study was to examine the accuracy of application-based screening audiometry in comparison to a standard audiogram in the evaluation of hearing thresholds in a nonselected elderly population and the acceptability of the application-based hearing screening test in this population.
Materials and Methods
The study was approved by the institutional research ethics committee and has been performed in accordance with the ethical standards as laid down in the 1964 Declaration of Helsinki and its later amendments. All participants signed an informed consent. A single dedicated iPad 2 tablet computer (Apple Inc, Cupertino, California, USA) was used in this study to avoid any possible effects of different device capabilities. It was presumed that the larger size of the iPad compared to the smartphone would make the test easier to perform in the elderly. Commercially available AKG K512 MK II headphones were used (AKG Acoustics GmbH & Co, Vienna, Austria). The uHear application is available free of charge and was downloaded to the iPad. This application has 3 modules for hearing testing. This study utilized 1 of the modules designed to test hearing sensitivity. The software determines thresholds at 6 separate frequencies ranging from 250 to 6000 Hz, following an initial assessment of ambient noise. The study hearing test can be completed in an average of 6 minutes. Patient input consists of touching a specific area of the screen every time a sound is heard. Thus, the level of fluency in English does not affect the ability to perform the test or the results. 25 The hearing thresholds are grouped into 6 grades from normal hearing to profound hearing loss. Patients 65 years of age or older hospitalized for any reason in an internal medicine department were included in the study. Application-based hearing testing (ABHT) was performed immediately before the standard hearing tests. Those refusing or unable to sign an informed consent or unable to perform a standard hearing test were excluded. All ABHT was performed in the same non-soundproofed quiet room in order to provide an environment that is similar to a home or a primary care clinic. Following ABHT, all participants underwent a full behavioral diagnostic audiometry in a soundproof booth. The hearing levels at each of the frequencies 500, 1000, 2000, 4000, and 6000 Hz were compared between ABHT and the standard audiogram. Subsequently, the pure tone averages (PTA) for frequencies of 500, 1000, and 2000 Hz according to the ABHT were compared to the PTA according to the standard audiogram.
Morris 26 has shown that hearing aid acceptance and benefit after screening has been shown to be largely dictated by better ear average (BEA) hearing threshold level. In a study by Davis et al, 11 the mean BEA of those accepting intervention after screening was 32 dB HL. A recent UK Health Technology Assessment (HTA) report concludes that adult hearing screening is acceptable and beneficial to 55- to 74-year-olds and that an audiometric screen for BEA 35 dB HL is most appropriate. 11 Based on the aforementioned, the pass/fail rate of both tests was compared using a PTA of 35 dB HL in the better ear as a cutoff point. Participants filled out a short demographic questionnaire including age, gender, number of years of formal education, and experience in the use of computer-based technology. Participants were asked to rate the difficulty in completing the ABHT on a Likert scale of 0 to 4. For categorical variables, summary tables are provided giving sample size and absolute and relative frequencies. For continuous variables, summary tables are provided giving arithmetic mean (M) and standard deviation (SD). Pearson chi-square or Fisher’s exact test was applied for testing the differences between the study groups for the categorical parameters. The 2-sample t test was applied for testing differences between the study groups for quantitative parameters. All tests applied are 2-tailed, and P value of <.05 was considered statistically significant. The data were analyzed using the SPSS version 20.0.0.2 (SPSS Inc. Chicago, Illinois, USA).
Results
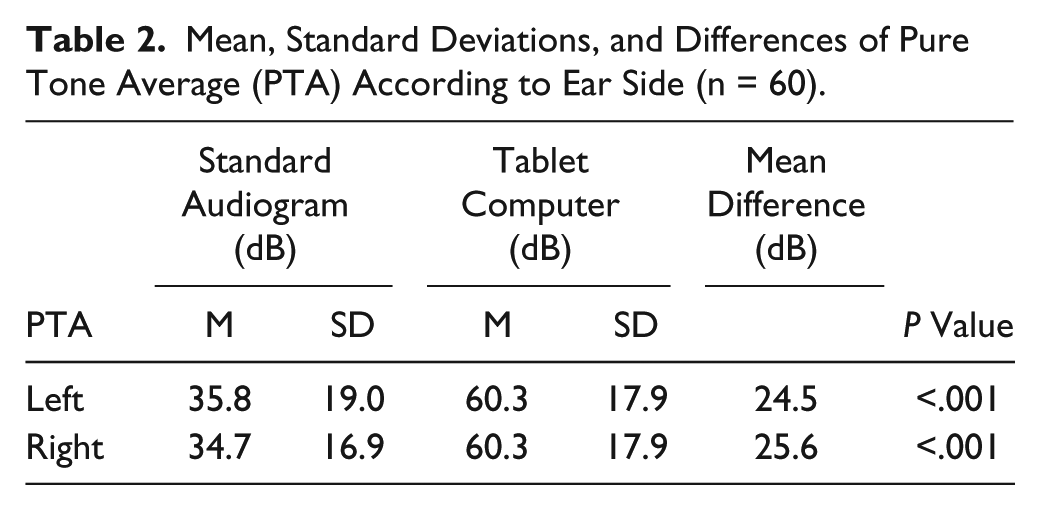
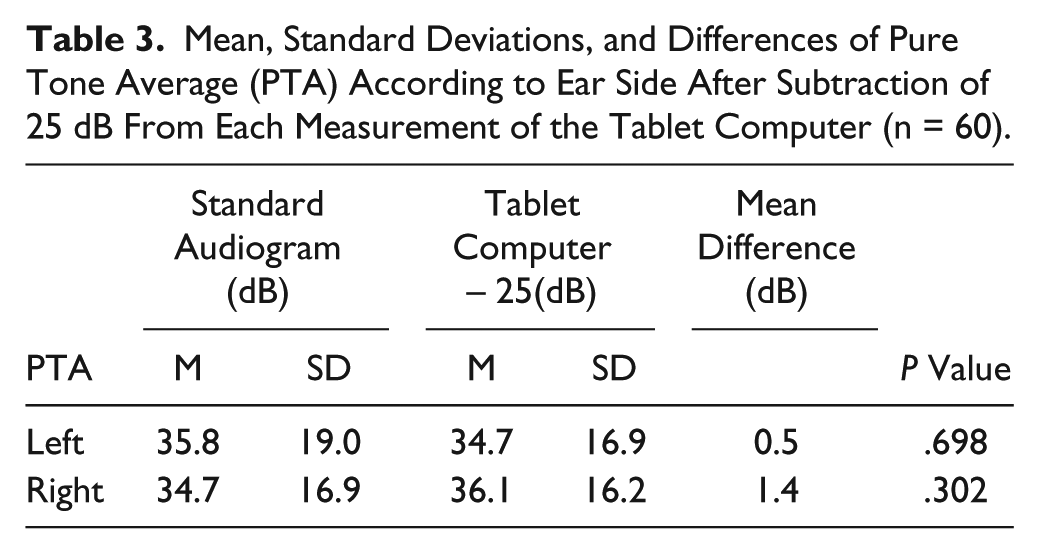
Seventy-seven patients were asked to participate in this study. Seventeen refused to sign an informed consent and were therefore excluded. Sixty patients were recruited and completed both ABHT and standard diagnostic audiometry. Table 1 summarizes participant demographics. Significant differences (P < .001) were observed between the hearing results obtained with ABHT and the standard audiogram at all frequencies and in both ears (Figure 1). Subpopulation analysis according to age revealed that in a group of participants aged 75 years or less, the same significant differences between the tests still existed. We attributed this result to the testing conditions in a non-soundproofed room and to possible suboptimal fitting of the earphones, resulting in leakage of acoustic energy and introduction of ambient noise. 27 Previous studies have found consistently worse hearing thresholds for the uHear application compared to diagnostic audiometry.27,28 Our results indicated that the average difference between the ABHT thresholds and the diagnostic audiometry thresholds for PTA frequencies of 500, 1000, and 2000 Hz was 24.47 dB for the left ear and 26.4 dB for the right ear. Based on these findings, we decided to subtract a constant factor of 25 dB from the ABHT results for each of the frequencies in order to compensate for ambient noise and possible visual distractions. Following this correction, no significant differences between the 2 testing methods were found for the frequency of 2000 Hz in the left ear and the frequencies of 1000, 2000, and 4000 Hz in the right ear (Figure 2). When the PTA for frequencies of 500, 1000, and 2000 Hz were calculated, the uncorrected ABHT results were significantly worse than the standard audiogram results (Table 2). However, when corrected by the same constant factor of 25 dB, no significant differences were found between the 2 testing methods (Table 3). Using a better ear PTA of 35 dB HL as a threshold for hearing aid acceptance and benefit, the corrected results of the ABHT were found to have a sensitivity of 76.5% and a specificity of 90.7% for screening. On a Likert scale of 0 to 4, the average difficulty in completing the tablet-based hearing test was 1.4 with a standard deviation of 0.8. Previous smartphone users reported a significantly higher degree of comfort in using the tablet computer (mean = 1.1 ± 0.2 vs mean = 1.5 ± 0.9, P = .008).
Demographic Characteristics of the Study Group a (n = 60).
Values are means ± 1 SD or frequencies and percentages.
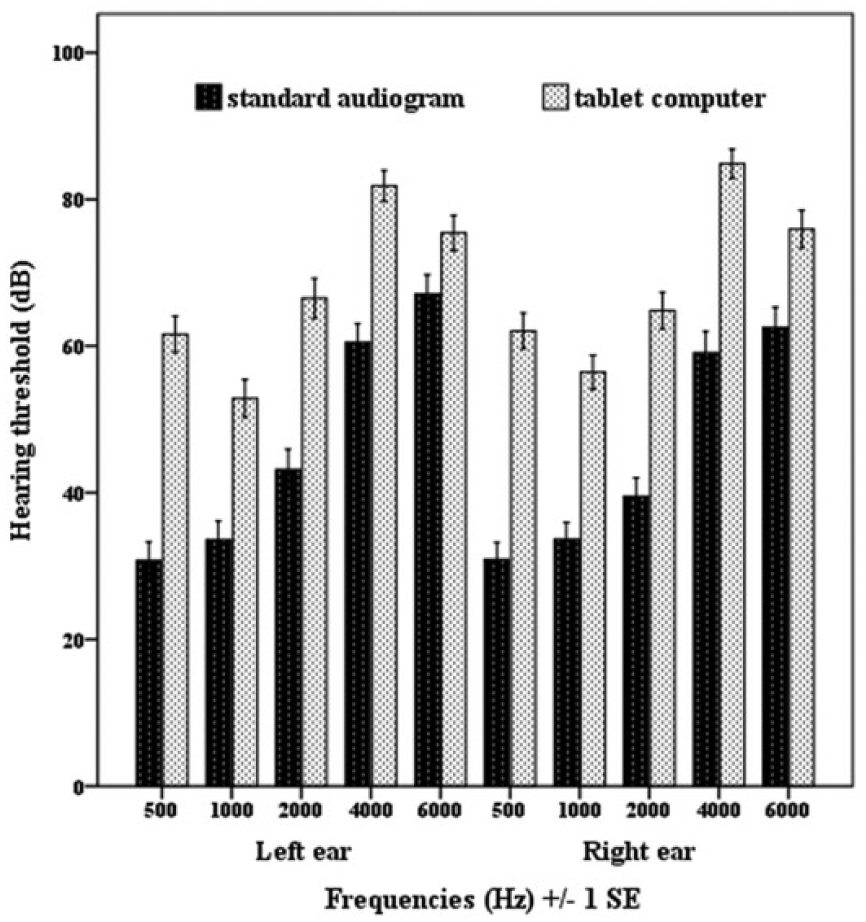
Mean hearing thresholds according to ear side and frequencies, ranging from 500 to 6000 Hz (n = 60). All differences between testing methods for both ears at all frequencies are statistically significant (P < .001).
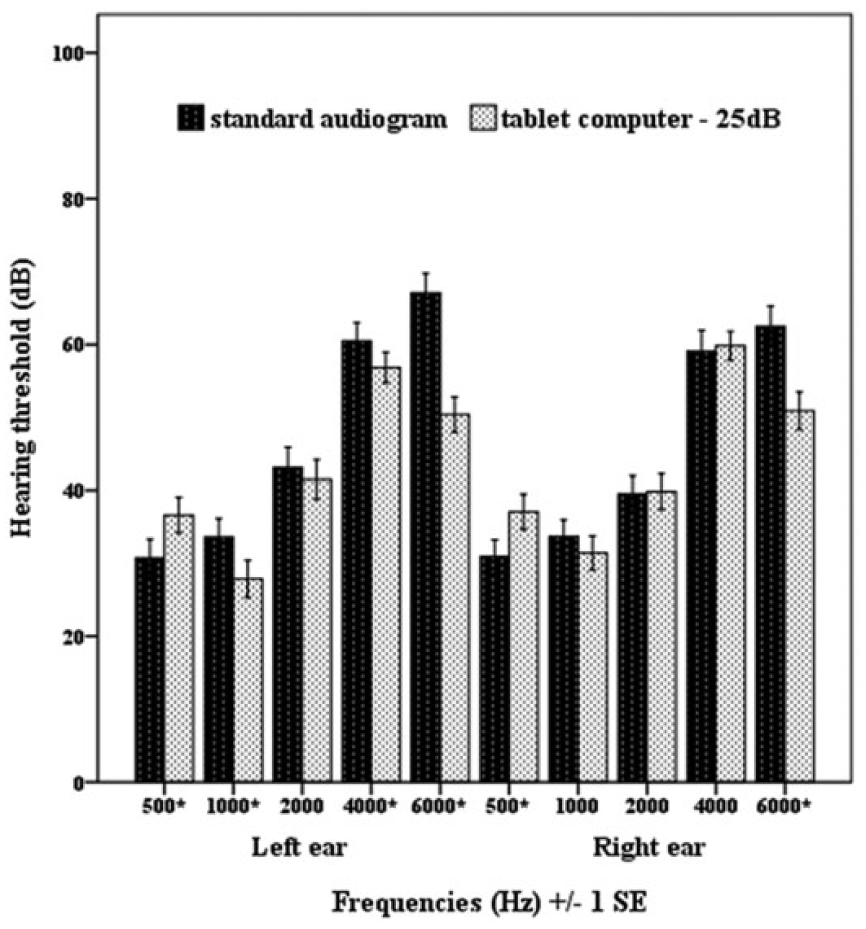
Mean hearing thresholds according to ear side and frequencies, after subtraction of 25 dB from each measurement of the tablet computer, ranging from 500 to 6000 Hz (n = 60).
Mean, Standard Deviations, and Differences of Pure Tone Average (PTA) According to Ear Side (n = 60).
Mean, Standard Deviations, and Differences of Pure Tone Average (PTA) According to Ear Side After Subtraction of 25 dB From Each Measurement of the Tablet Computer (n = 60).
Discussion
A formal audiometric evaluation is the gold standard for the diagnosis of hearing loss, but it may not be readily available, especially in rural or underserved areas, since it requires a soundproof testing environment and trained personnel. A smartphone- or tablet-based application for hearing evaluation offers the possibility of screening by self-testing at home or easy and accessible screening in the primary care or geriatric clinic. We used the uHear application (Unitron, Victoria, Canada). This application is available free of charge and was downloaded to an iPad. Three published studies have compared the performance of this application for hearing assessment in adults.27-29 In a group of adults, Szudek et al 28 demonstrated reasonably accurate results for ruling out moderate hearing loss and quantifying a general degree of hearing loss. In normal-hearing persons, however, it proved to be inaccurate with overestimation of thresholds. A clinical study by Handzel et al 29 of patients with unilateral sudden onset hearing loss demonstrated that the uHear application was useful to categorize the type of loss during otological consultations with a sensitivity of 76% and specificity of 91%. The mean age of participants in the study performed by Szudek et al 28 was 46 years and in the study performed by Handzel et al, 29 51.4 years. In a recent study evaluating smartphone-based audiometric testing for screening hearing loss in the elderly, Abu-Ghanem et al 27 evaluated the uHear application in a selected population of elderly patients. They found that for this population, the application has a sensitivity of 100% and specificity of 60% for screening. It should be noted that Abu-Ghanem et al 27 excluded patients with dementia and non-native English speakers and used a portable audiometer and not a soundproof testing environment as the base for comparison. Also, the study was conducted with a relatively small sample size of 26 patients with an average age of 84.4 years. To our knowledge, ours is the first study to examine the accuracy of ABHT in the evaluation of hearing thresholds in an elderly population in comparison to a standard audiogram. The participants’ average age in this study was 74.6 years. This age group better represents the population that could be potential candidates for ABHT. The uHear thresholds were increased in comparison to the standard audiogram. We attribute this to the testing conditions in a quiet but non-soundproofed room. Ambient noise and visual distractions could potentially explain the constant overestimation of hearing loss by an almost constant factor of 25 dB. 30 The uHear application performs an initial measurement of ambient noise levels prior to hearing testing, but this measurement seems to be ineffective. After appropriate correction, the application accurately predicted the true PTA for both ears. Using a BEA threshold of >35 dB as a cutoff point for referral for full audiometric evaluation and possible hearing aid fitting, the sensitivity and positive predictive value of ABHT were both 76.5%. The specificity and negative predictive value of ABHT were both 90.7%. Four of the 60 participants would have been unnecessarily referred for diagnostic testing (false-positive), and 4 participants in need of further diagnostic testing would have been missed (false-negative). Our results indicate that ABHT for screening using the uHear application is inaccurate in comparison to the gold standard and uncorrected cannot be effectively used as a screening tool. However, when appropriately and site-specifically corrected, the uHear application could be used, mainly in order to rule out significant hearing loss in an elderly population. On average, participants had very little difficulty completing the tablet-based testing. It is worth mentioning that the legal status of ABHT is yet to be determined and it is currently inadequate for medico-legal use. The ABHT should only be used for aiding the decision whether an individual should be referred for additional testing.27,29 Several possible limitations of this study should be mentioned. The study population was recruited from an internal medicine department, and the results may therefore not be generalizable to the entire elderly population. However, although this is a population typically suffering from chronic illness, patients in acute physical or emotional distress were not asked to participate in the study. As the participants of this present study were not screened for dementia, digital literacy, or level of English, we believe that they can represent the general elderly population. Accuracy of ABHT depends not only on the characteristics of the selected application but also on the qualities of the earphones and on the levels of ambient noise. 29 In this study, the uHear application was initially found to be inaccurate, and only after appropriate correction were we able to obtain useful results. This correction may only be applicable to our specific software and hardware and to our specific testing conditions. Other factors of correction may be applicable in different circumstances, and ABHT should be performed after appropriate and site-specific calibration. Pure tone average for ABHT should be obtained in the proposed testing environment and then compared to PTA for full behavioral diagnostic audiometry in a soundproof booth. This comparison will then enable the calculation of the site-specific correction factor.
Patient-generated data, much of it depending on mobile technology, are expected to become more and more widespread. Application-based hearing testing is an example of this. It is important for physicians to appreciate the benefits and also the limitations of these technologies that will be used by patients who will then seek professional advice regarding further evaluation and treatment.
Conclusions
The uHear application is inaccurate in assessing hearing thresholds for screening purposes in the elderly. However, when properly and site-specifically corrected, tablet-based hearing testing using the uHear application is well accepted by the elderly and can be used as an effective screening tool for hearing loss in an unselected elderly population, mainly in order to rule out significant hearing loss.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.