
Abstract
Objective:
The aim of this study was to determine if external subglottic air flow (ESAF) influences swallowing frequency in severely dysphagic tracheotomized patients with brain injury.
Methods:
Ten patients were recruited at the neurological intensive care unit. The ESAF intervention was provided through the standard cuffed suction aid tracheotomy tube, which primarily is used to suction residual secretion volume from the subglottic area. Sessions were 150 minutes, and ESAF was provided at 60-65, 90-95, and 120-125 minutes at 3 L/min. Outcome measures included swallowing frequency (swallows/5 min) at 0-5 minutes (pre-baseline), 25-30 and 55-60 minutes (baseline/control), and 85-90, 115-120, and 145-150 minutes (postintervention). The residual secretion volume (ml) from the subglottic area was collected using a syringe at 0 minutes (pre-baseline), 30 and 60 minutes (baseline/ control), and at 90, 120, and 150 minutes (postintervention).
Results:
The mean (±SEM) swallowing frequency (swallows/5 min) increased from 0.60 ± 0.30 to 2.10 ± 0.70 during the ESAF intervention (P < .001). The mean (±SEM) residual secretion volume reduced from 3.10 ± 0.31 ml to 0.50 ± 0.30 ml after the ESAF intervention (P < .001).
Conclusion:
The increase in swallowing frequency and reduction in residual secretion volume may indicate that ESAF influences swallowing parameters in patients with tracheotomy tubes.
Introduction
Patients with severe acquired brain injury (ABI) experience a wide range of neurological changes, including a reduced conscious state, respiratory problems, and dysphagia.1,2 Dysphagia occurs in 37% to 78% and 25% to 61% in stroke and traumatic brain injury cases, respectively.3,4 Patients with ABI also have compromised respiration. 4 Therefore, patients require tracheotomy tubes for ventilation and secretion management. A recent epidemiological study showed that 65% to 68% of patients with severe ABI are tracheotomized in neurorehabilitation units. 5
Tracheotomy tubes are vital for airway management; however, oropharyngeal residual secretions often pool above the tracheal cuff. Over time, the residual secretions eventually leak around the cuff and result in tracheobronchial colonization. 6 Additionally, the incidence of aspiration with tracheotomy tubes is 65% to 87%. 7 The removal of the tracheotomy tube is a priority but at times is not possible as removal could cause increased morbidity and mortality.8-10 Studies have demonstrated that suction of subglottic residual secretions above the tracheal cuff delays and decreases the incidence of pneumonia.11,12 The use of specific suction aids with continuous and intermittent suctioning reduces tracheal aspiration. 13
Long-term tracheotomy tubes negatively influence the pharyngeal stage of swallowing, which results in an increased incidence of aspiration (50%-87%).14,15 In ABI patients, tracheotomy tubes might also impair motor function and sensation, leading to disordered deglutition. 16 The severity of sensory deficits from the laryngo-pharynx might be responsible for dysphagia and is a possible contributor to silent aspiration. 17 In healthy participants, Jafari et al 18 demonstrated that swallowing depends on superior laryngeal nerve feedback using a bilateral bupivacaine block of the internal branch of superior laryngeal nerve. The block induced a loss of sensation of swallowing and a large increase in aspiration in healthy volunteers. 18 The deglutitive subglottic air pressure (DPsub) theory of swallowing is widely accepted and states that laryngeal mechanoreceptors have a role in the regulation of swallowing function.16,19 Gross et al 20 examined various healthy participants and demonstrated that afferent feedback from the respiratory system was used in swallowing.
The aforementioned studies demonstrate the importance of mechanoreceptors for swallowing. Due to the inflated cuff, airflow bypasses the natural laryngeal path and flows through the tracheotomy tube. Hypothetically, the lack of natural airflow in the larynx compromises the afferent signaling. Theoretically, it is therefore possible to provide artificial airflow to the laryngeal area to elicit normal conditions.
The cuffed suction aid tracheotomy tube features an integral suction lumen to assist in the removal of residual secretions from above the cuff (subglottic area). The residual secretions are usually removed from the internal suction lumen by suctioning with a syringe. In our rehabilitation center, we introduced a novel system to provide external air flow through the same lumen (named external subglottic air flow, ESAF). External subglottic air flow has been used in our neurorehabilitation setup for 8 years. Over this time, ESAF evolved and is now standardized within our rehabilitation setup. Therefore, in the current study, parameters such as flow rate, number of exposures, and time between exposures for ESAF are similar to the parameters delivered in the clinical setting.
The purpose of this explorative pilot study was to investigate the effect of ESAF on swallowing frequency in severe dysphagic tracheotomized patients with brain injury in a neurological intensive care unit. The hypothesis is that ESAF (flow rate: 3 L/min; episode of exposure: at 30-minute interval × 3 time points), provided in a timely manner, will increase the swallowing frequency and decrease the accumulated residual secretions above the cuff.
Methods
Ten dysphagic tracheotomized patients with brain injury (8 men, 2 women; mean age [±SEM]: 49.4 ± 5.12 years; range, 19-78 years) were recruited from the neurological intensive care unit. Patients were included if they had a functional oral intake scale score (FOIS) of 1 (no oral intake). 21 All patients were tracheotomized due to severe brain injury lesions and dysphagia and were fed using percutaneous gastric endoscopy. Four out of 10 patients could breathe unaided, and the tracheotomy cuff of all patients was inflated continuously. The study was approved by the data handling agency (equivalent to Institutional Review Board, journal number: 1-16-02-561-14) and performed in accordance with the Declaration of Helsinki II. Patient consent was not required as the intervention is routine clinical practice in the Danish neurorehabilitation setting.
The demographic characteristics, clinical scores, and ventilator status of the patients are shown in Table 1. Clinical scores included the FOIS, Ranchos Las Amigos Scale (RLAS), 22 Early Functional Abilities (EFA), 23 and Functional Independency Measurement (FIM). 24 These were recorded prior to the session to identify the severity of dysfunction, level of arousal, level of awareness, and functional ability of the patients (Table 1). Overall, these patients had a low functional level with low arousal. The data were collected by experienced occupational therapists trained to observe manual swallowing (observing the jaw-pumping movement followed by duration and extent of laryngeal excursion [Adam’s apple], considering both anterior and superior movement).
Demographic and Clinical Information.
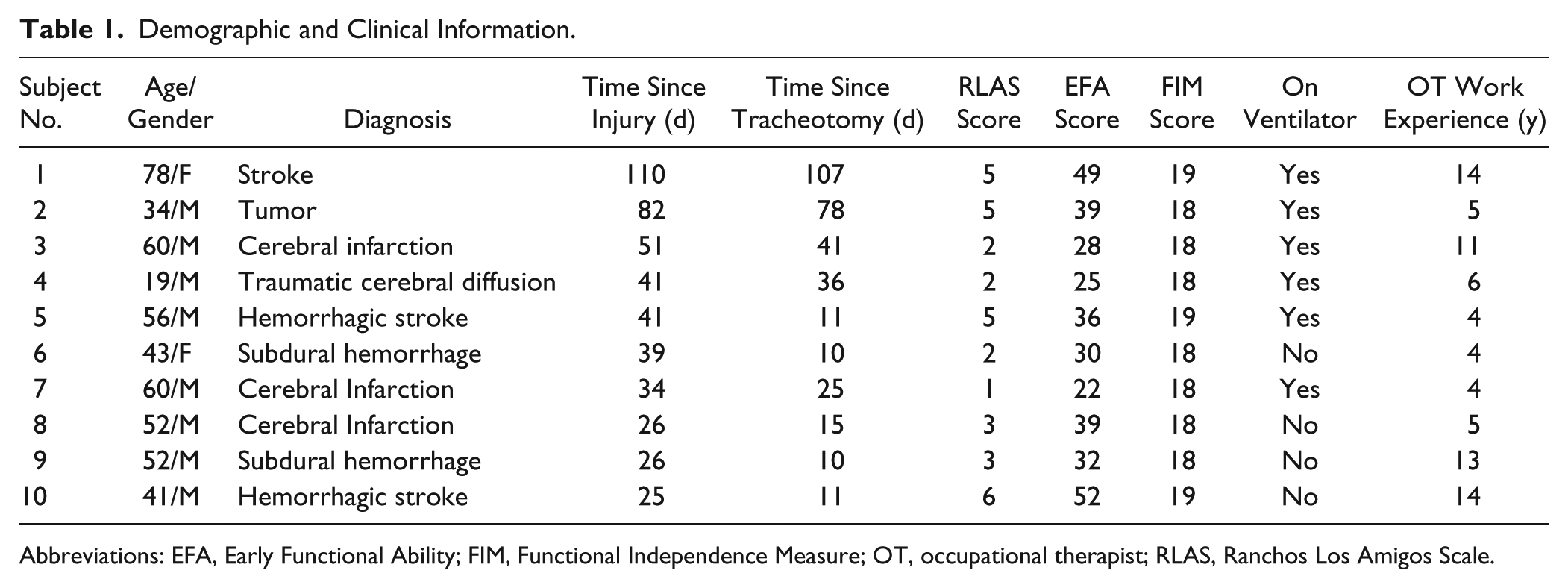
Abbreviations: EFA, Early Functional Ability; FIM, Functional Independence Measure; OT, occupational therapist; RLAS, Ranchos Los Amigos Scale.
The Blue Line Ultra Suction tracheotomy tube is a cuffed tube that has an above-cuff/subglottic suction line. The suction line allows the removal of pooled subglottic residual secretions using a disposable syringe (Figure 1). This type of suctioning maintains a clean, hygienic, and unobstructed upper airway. 25 At our neurorehabilitation center, the Blue Line Ultra suction aid has been modified to provide additional ESAF to the subglottic area (Figure 1).
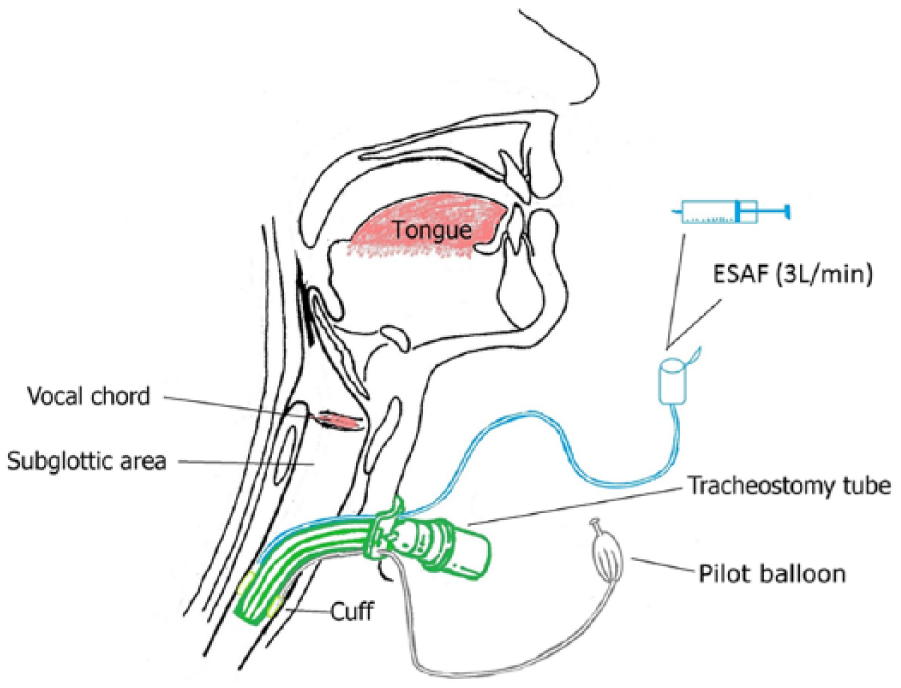
Schematic illustration of the method used to provide the external subglottic air flow (ESAF). The same lumen was used to evaluate the amount of subglottic residual secretions (ml).
The testing session took 150 minutes. Patients were positioned at a 45° recline left side body position as the cuffed suction aid lumen opened on the left side. This allowed for maximum suctioning of the residual secretions and provided the most natural position for swallowing. 26 Patients remained in the same position throughout the session unless movement was unavoidable due to a lack of patient compliance. No oral interventions such as brushing or oral stimulation were performed 1 hour before or during the session. During the 150-minute testing session, ESAF was administered at 60-65, 90-95, and 120-125 minutes. On the commencement of ESAF, air was delivered at 1 L/min for the first 5 seconds and was constant at 3 L/min thereafter. The 5-minute ESAF intervention is shown in Figure 2.
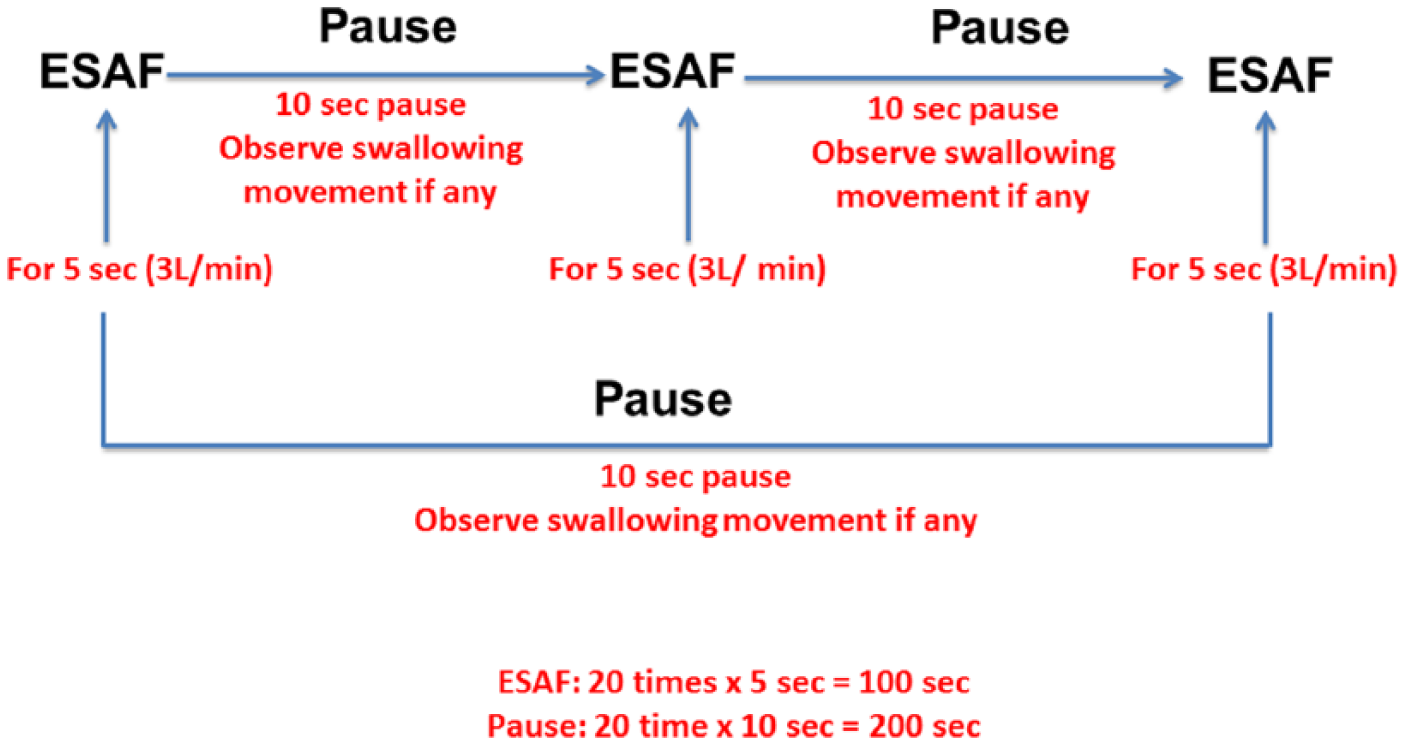
External subglottic air flow (ESAF) for 5 minutes at 3 time points: 60-65, 90-95, and 120-125 minutes.
The swallowing frequency (swallow counts/5 min) was measured at 25-30 and 55-60 minutes (baseline measurement) and at 85-90, 115-120, and 145-150 minutes (postintervention measurement). The subglottic residual secretion volume (ml) was recorded through a disposable syringe at 30 and 60 minutes (baseline measurement) and at 90, 120, and 150 minutes (postintervention measurement). Pre-baseline recordings for swallowing frequency and residual secretion volume were performed at 0 minutes, when the suction tube was first emptied. This occurred so that all patients commenced the experiment with the same residual secretion volume (0 ml). Baseline measurements occurred before each ESAF measurement. Therefore, patients served as their own controls.
SPSS software (version 13.0, Apache Software Foundation, Forest Hill, Maryland, USA) was used for data analysis. Pearson’s chi-square test was used to assess the swallowing frequency over the assessed time points. Subglottic salivary residual secretions were analyzed using Wilcoxon signed rank tests at different time points. The relationship between swallowing frequency and subglottic residual secretion volume was analyzed using Spearman’s rho correlation. The level of significance was set at P < .05.
Results
All data are presented in Tables 2 and 3.
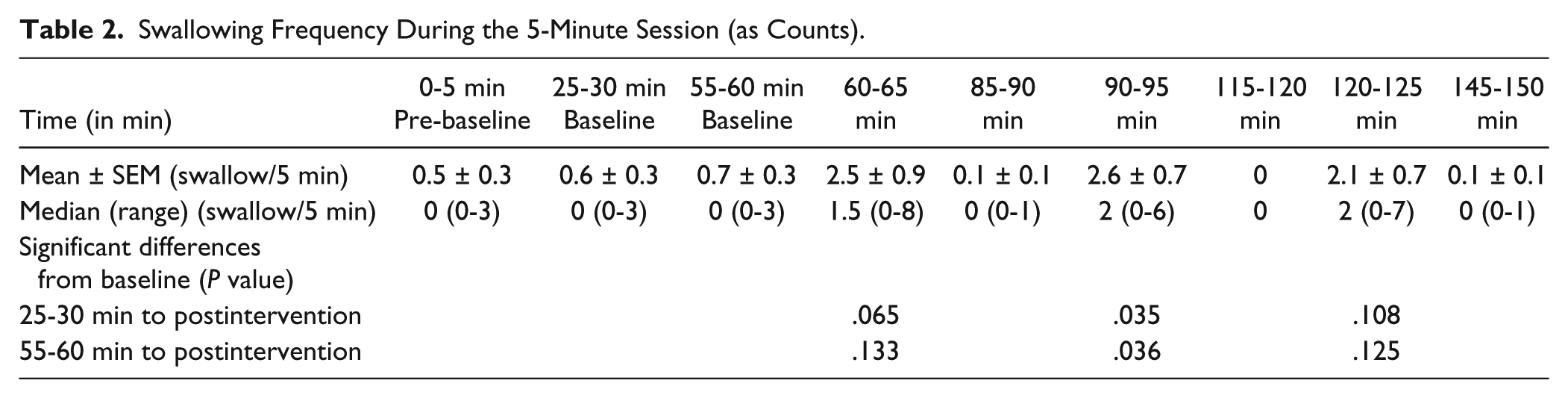
Swallowing Frequency During the 5-Minute Session (as Counts).
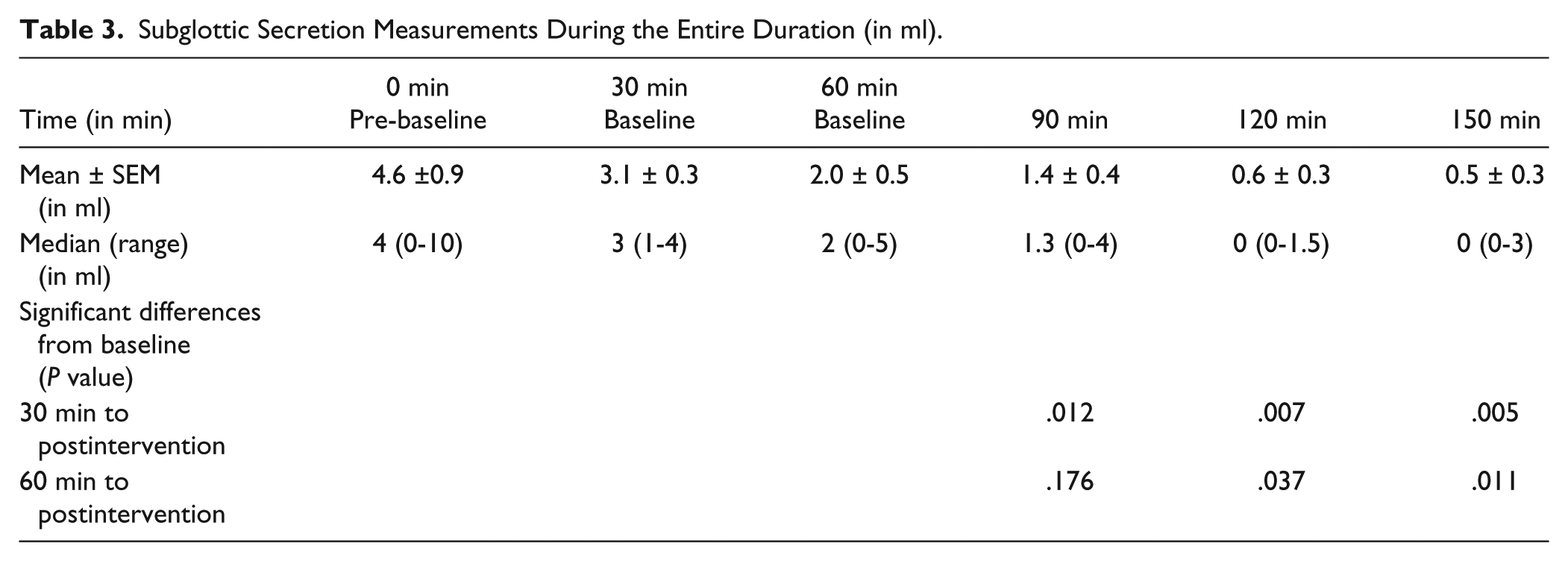
Subglottic Secretion Measurements During the Entire Duration (in ml).
Swallowing Frequency
Overall, the mean (±SEM) swallowing frequency (swallows/5 min) significantly increased from 0.60 ± 0.30 (baseline) to 2.10 ± 0.70 during the ESAF intervention (P < .001) (Table 2). Further analyses revealed that the 25-30–minute baseline swallowing frequency was significantly different from 90-95 minutes (P = .035) but not significant from 120-125 minutes (P = .108). The 55-60–minute baseline recordings were significantly different from 90-95 minutes (P = .036) swallowing frequency but not from 60 minutes (P = .133) or 120 minutes (P = .125) (Table 2).
Volume of Residual Secretions
Overall, the mean (±SEM) residual secretion volume for all participants reduced from 3.10 ± 0.31 ml (baseline) to 0.50 ± 0.30 ml after the ESAF intervention (P < .001). Further analyses showed that the baseline measurement at 30 minutes was significantly different from each postintervention time point (90, 120, and 150 minutes) (P < .012). Sixty-minute baseline measurements were significantly different from the postintervention time points of 120 (P = .037) and 150 minutes (P = .011) but not from 90 minutes (P = .176) (Table 3).
Relationship Between Volume of Secretions and Swallowing Events
Spearman’s correlation analyses showed no relationship between the reduction in subglottic secretions and the increase in swallowing frequency (−0.108 < δ < 0.357; P = .311).
Discussion
The current study explored if providing external subglottic air flow improves swallowing frequency and reduces residual subglottic secretions. The results showed that there was an increase in swallowing frequency during the ESAF intervention, which might support the use of ESAF as an adjunctive treatment for tracheotomized patients suffering from dysphagia (Table 2).
The theory behind ESAF is that it stimulates the subglottic mucosa innervated by the internal branch of superior laryngeal nerve, which assists in the brief closure of the vocal folds. 18 Therefore, ESAF may assist in creating subglottic pressure and increasing the probability of a laryngeal adductor reflex (closure of the vocal folds).16,19 Although speculative, this is possibly similar to the experiments of Aviv et al, 27 who used air puff stimulation to the laryngeal mucosa over the arytenoid cartilage to elicit the laryngeal adductor response. This hypothesis is further supported by a study on healthy participants that shows that laryngeal mechanoreceptors could regulate swallowing function. 20
Another important finding was the reduction in subglottic residual secretion volume over time, which was significantly different from the baseline measurements. Timely removal of subglottic residual secretions reduces the risk of aspiration 16 and reduces the likelihood of respiratory pathogen colonization.1,28 Therefore, this intervention could be beneficial to patients with increased residual secretions.
Once patients no longer require a cuffed tracheotomy tube, they are transitioned to weaning process. This transfer often involves using a Passy-Muir valve and deflated cuff, which allows them to breathe more naturally and create a positive subglottic pressure. 19 This provides the patients with subglottic airflow for possible safer deglutition. However, a substantial number of patients without a ventilator continue to have signs of aspiration and compromised respiratory function. Hence, these patients have an inflated cuff and would require positive subglottic pressure, aided by ESAF.
Limitations
The study has a small sample size, which increases the risk of both type 1 and type 2 statistical errors. Therefore, although this study presents an interesting concept, firm conclusions should be cautioned.
Patients were used as their own control as there was a large variability in the swallowing frequency between patients, from no swallowing to normal swallowing events. 3 Due to this, it is difficult to find control populations for the included patients. In addition, differences in lesion site and diagnosis made it difficult to match patients with controls. As using ESAF is routine in Danish hospitals, we were unable to use patients as their own control on a subsequent day as this would deviate from standard treatment in our hospital. Future studies should aim to perform the same measurements on a subsequent day or over a longer time window without any intervention. This would provide a more reliable baseline measurement of swallowing frequency and residual secretion amount.
Swallowing measurements in the current study were based on a set of criteria; however, these criteria were based on visual analysis by an occupational therapist. To reduce the effect of human error, there is a requirement for a noninvasive objective measurement to determine swallowing events to have a more accurate measure of the effect of ESAF.
Throughout the experiment, patients were at reclined left sided body position so that maximum subglottic secretions could be withdrawn. It was sometimes difficult to maintain the same position for the entire session due to a lack of patient compliance. Additionally, it is possible that all subglottic secretions were not suctioned because cuff sealing of 100% was not possible. This may have led to some aspiration and a reduction in the measured residual secretion volume.
Randomized control trials are required to investigate the effect of ESAF. In addition, functional measurements of swallowing should be observed by endoscopic evaluation or quantifying residual secretion through modified barium swallow or a radiolabeled saliva studies. It has been shown, using fMRI, that air-puff stimulation significantly increases the activation of sensory projections to laryngeal area of the somatosensory cortex. 29 Therefore, an interesting line of research could be to explore the influence of ESAF on the excitability of the laryngeal area of the somatosensory cortex.
Conclusion
The increased swallowing frequency probably indicates an improvement in swallowing and reduction in residual secretion volume, which might indicate reduced risk of aspiration and tracheobronchial colonization. Future studies are required to explore the possible link and the consequences for the weaning process.
Footnotes
Acknowledgements
We would like to acknowledge Peter William Stubbs for reviewing the English in the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The project was funded by Regional Hospital, Hammel.