
Abstract
Objectives:
Temporomandibular disorder (TMD) involves dysfunction of the temporomandibular joint and associated muscles of mastication causing pain with chewing, limitation of jaw movement, and pain. While the exact pathophysiology of TMD is not completely understood, it is thought that hyperfunction of the muscles of mastication places stress on the temporomandibular joint, leading to degeneration of the joint and associated symptoms. We hypothesize that chemodenervation of the muscles of mastication with IncobotulinumtoxinA (Xeomin) will decrease the stress on the temporomandibular joint and improve pain associated with temporomandibular joint and muscle disorder (TMJD).
Methods:
Twenty patients were randomized to IncobotulinumtoxinA (170 units) or saline injection of the masticatory muscles. Patient-reported pain scale (0-10) was recorded at 4-week intervals following injection for 16 weeks. Patients who received saline injection initially were assessed for reduction in pain at the first 4-week interval and if still had significant pain were rolled over into the IncobotulinumtoxinA arm.
Results:
Preinjection pain scores were similar between patients. While there was a statistically significant reduction in pain score in the placebo group one month, there was an overall larger drop in average pain scores in those patients injected with IncobotulinumtoxinA initially. All patients initially injected with placebo crossed over into the IncobotulinumtoxinA group. Similar results were seen when examining the composite masticatory muscle tenderness scores. There was no significant change in usage of pain medication.
Conclusions:
We demonstrate utility of IncobotulinumtoxinA in treating patients with TMD with pain despite pain medication usage and other conventional treatments.
Temporomandibular disorder (TMD) is a nonspecific term used to describe joint and muscle disorders that affect the masticatory system. It has been reported that about 5% to 12% of the US population is affected by TMD, and the annual cost of managing TMD, excluding cost related to imaging, is about $4 billion. 1 Plesh and colleagues 2 reported that in the 2000-2005 US National Health Interview Survey (NHIS), which included a total of 189 977 people, 4.6% (n = 58 964) of people had experienced temporomandibular joint and muscle disorder (TMJD).
Symptoms are commonly related to pain surrounding the joint and may include referred ear pain, headache, transmitted neck pain, decreased jaw mobility, difficulty and/or pain while chewing, and crepitus or other noise within the joint with movement. In general, TMD is divided into myofascial TMD or arthrogenic TMD. Myofascial TMD is associated with the pain from hyperfunctioning muscles of mastication leading to chronic myositis. In contrast, arthrogenic TMD is associated with intracapsular pathology, with pain at the level of the joint itself, often confused with ear pain. 3
Temporomandibular disorder encompasses many clinical abnormalities, which may include spasm of the masseter, temporalis, and/or pterygoid musculature. Pain associated with TMD may be muscular or joint in origin. Current treatments for TMD include measures such as exercise and massage; systemic anti-inflammatory medications such as NSAIDs, muscle relaxants, and tranquilizers; and various types of occlusal devices to offset the strain on the muscles and joint. However, there is a lack of evidence that any one treatment is more effective than another. For example, a systematic review performed on orthodontics for treating TMD was unable to find a single article to match their inclusion criteria. 4 Another systematic review comparing interventions for TMD showed equivalent pain reduction with splints versus diclofenac sodium and that glucosamine was as effective as ibuprofen for pain management; however, the review did comment on the lack of high level evidence. 5
IncobotulinumtoxinA (brand name: Xeomin, manufactured by Merz North America Inc, Raleigh, North Carolina, USA) is a neurotoxin that blocks presynaptic acetylcholine release. Local injections of IncobotulinumtoxinA have been FDA approved for therapy for blepharospasm and cervical dystonia and the management of frown lines. Botulinum toxin has also been used for other types of focal dystonia such as spasmodic dysphonia, oromandibular dystonia, and occupational writer’s cramp and spasticity.6 -11
We hypothesize that a major factor leading to pain associated with TMD is related to excess strain placed on the temporomandibular joint by hyperfunction and spasms of the masseter, temporalis, and pterygoid musculature. In theory, weakening these muscles with botutlinum toxin injection should lead to relief of symptoms. There is also evidence that the botulinum toxins also decrease pain by the effect on the afferent nerves and decrease the release of inflammatory mediators (Substance P, CGRP, Glutamate). 12 This study is intended to examine the effectiveness and safety of IncobotulinumtoxinA in relieving the subject’s muscle spasm and pain associated with TMD.
Study Design
The study was monitored and approved by the Western Institutional Review Board (WIRB) in Seattle, Washington, USA. The study duration was 4 months. Subjects were recruited from a variety of dental and otolaryngology practices where patients had failed standard treatments. Those who volunteered for the study were screened for specific inclusion and exclusion criteria (described in the following). Approximately 50% of the subjects who volunteered were recruited for the study. Subjects who completed the study attended a total of 5 study visits 1 month apart and 1 telephone interview at 1 week after injection. At the initial visit (day 0), patients were screened, reviewed informed consent, and answered a questionnaire. Females who met inclusion criteria were screened with a pregnancy test. Subjects who met all inclusion criteria were then randomized via random computer generated number to 1 of the 2 double-blinded treatment groups, placebo versus IncobotulinumtoxinA injection. Patients receiving IncobotulinumtoxinA were injected under EMG control with 50 units into each masseter muscle, 25 units into each temporalis muscle, and 10 units into each external pterygoid muscle using a 27-gauge monopolar electrode injection needle. Patients receiving placebo received an equal volume of normal saline into each muscle injected with the same needle. Patients were then sent home with a pain diary and at 1 week completed a telephone interview. Patients were also asked for adverse event occurrence such as pain at the injection site, local reaction to the injection, and difficulty chewing. Patients returned at 1 month. In those patients who did not have at least a 50% reduction in pain, an unblinded nurse reviewed which injection they had initially received. Those who were injected with placebo initially and did not report at least a 50% reduction in pain received IncobotulinumtoxinA injection, and those initially injected with Incobotulinumtoxin A were injected with saline (placebo). Patients then returned each month for review of their diary and examination (a total of 4 months after the blinded second injection).
Objective/purpose of study
The primary objective of the trial is to examine the efficacy of IncobotulinumtoxinA at a total of 170 units (50 units to each masseter, 25 units to each temporalis, 10 units to each external pterygoid) compared to placebo in the treatment of TMD in a double-blind trial measured by a decrease in pain on a 1 to 10 scale.
Primary objective
Evaluate for decrease in pain related to TMD with IncobotulinumtoxinA injection compared to placebo.
Secondary objectives
Evaluate for decrease in pain medication usage relative to placebo via a 0 to 10 pain scale.
Assess the safety of treatment with IncobotulinumtoxinA relative to placebo (incidence of adverse events).
Evaluate for a decrease in tenderness to palpation of the temporalis, masseter, and external pterygoid muscles via a composite pain scale (1 = no pain on palpation, 4 = maximal pain on palpation, scale range, 6-24).
Inclusion and Exclusion Criteria
Please see Table 1.
Inclusion and Exclusion Criteria.
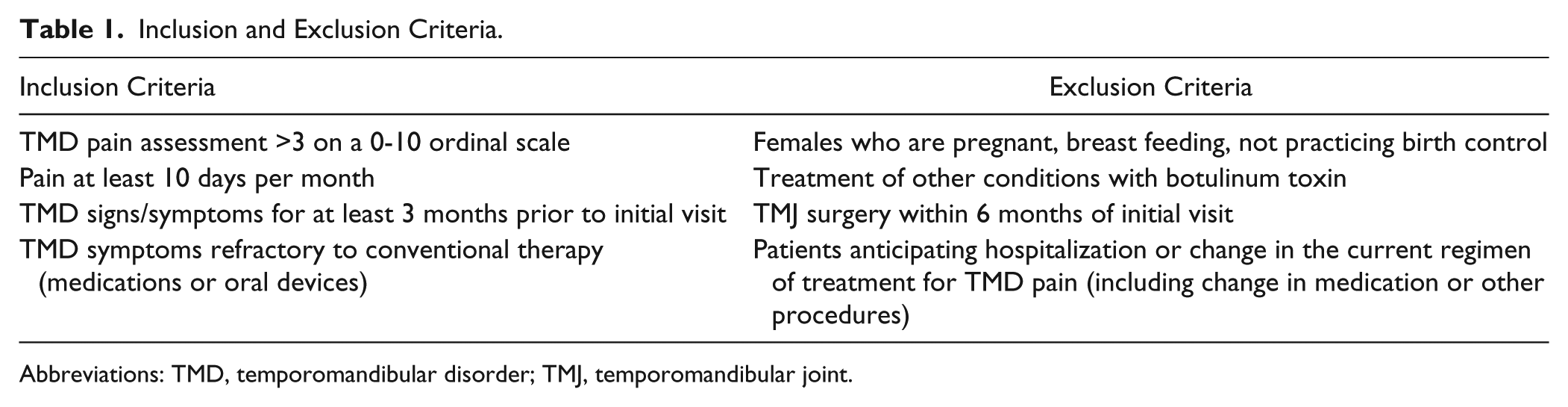
Abbreviations: TMD, temporomandibular disorder; TMJ, temporomandibular joint.
Results
Data were available for 19 of 20 patients (1 patient dropped out due to a family illness and moved out of state). Placebo group refers to those patients who received a saline as their first injection, while Incobotulinumtoxin A group refers to those patients who received IncobotulinumtoxinA as their first injection. No adverse events were noted. Initial pain scores were similar between the 2 groups (placebo group = 5.43 ± 2.6 vs IncobotulinumtoxinA group = 5.4 ± 2.1, P = .976; see Table 1). Four weeks after initial injection, change in average pain scores between each group showed statistically different decrease (placebo = 1.7, P = .01, IncobotulinumtoxinA = 4.5, P = .0002; see Table 2), with the IncobotulinumtoxinA group showing a larger drop in value than the placebo group. Despite a drop in average pain scores in the placebo group, all patients in the placebo group subjectively reported minimal to no relief and were therefore crossed over to the IncobotulinumtoxinA treatment group at 4 weeks. Average pain scores for the IncobotulinumtoxinA group at 4 weeks was statistically significantly less than the placebo group (placebo = 3.72 ± 2.5 vs IncobotulinumtoxinA = 0.9 ± 1.7, P = .009). At 2, 3, and 4 months following injection, pain scores between the 2 groups (now both active toxin) remained similar (Table 1, Figure 1). Average change in pain score also remained statistically significantly lower at 2, 3, and 4 months following injection when compared to baseline. Table 3 shows a comparison between the 2 groups with the timepoints shifted to reflect months after IncobotulinumtoxinA injection. Patients started out with no statistical difference between pain scores and showed similar decreases in pain scores at 1 and 2 months following injection with IncobotulinumtoxinA. At 3 months after IncobotulinumtoxinA injection, the placebo group had a statistically higher pain score than the injection group.
Average Reduction in Pain Scores: IncobotulinumtoxinA Versus Placebo.
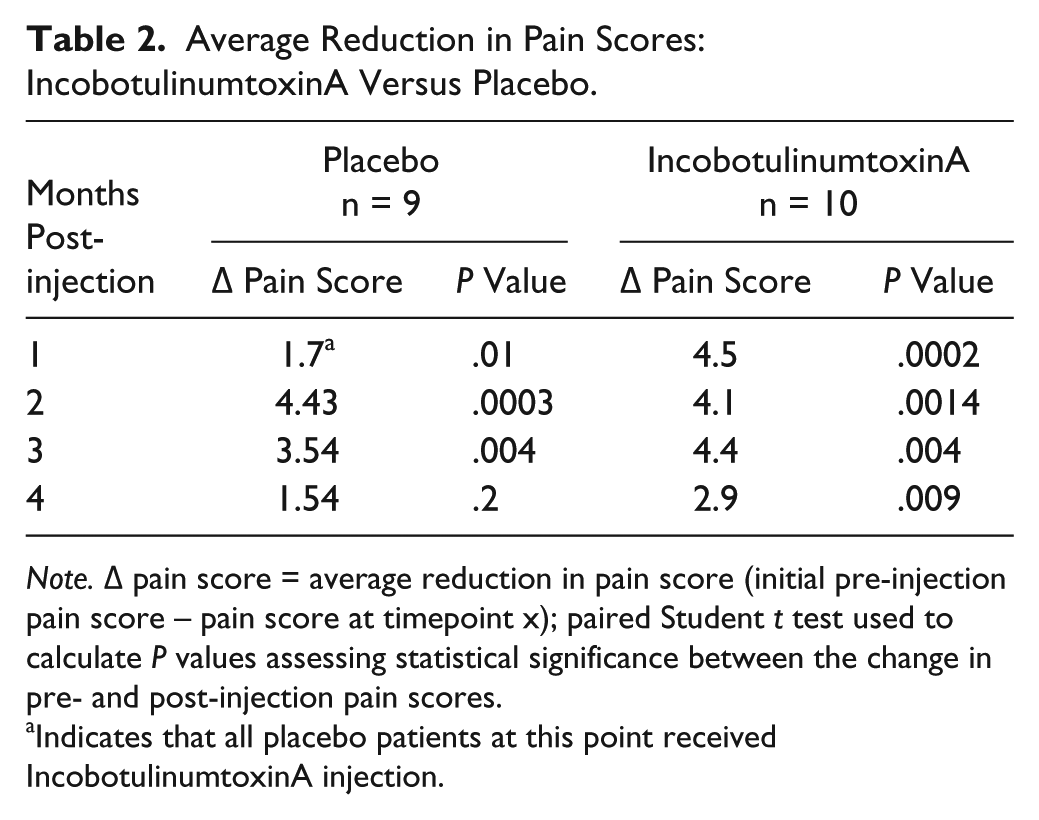
Note. Δ pain score = average reduction in pain score (initial pre-injection pain score – pain score at timepoint x); paired Student t test used to calculate P values assessing statistical significance between the change in pre- and post-injection pain scores.
Indicates that all placebo patients at this point received IncobotulinumtoxinA injection.
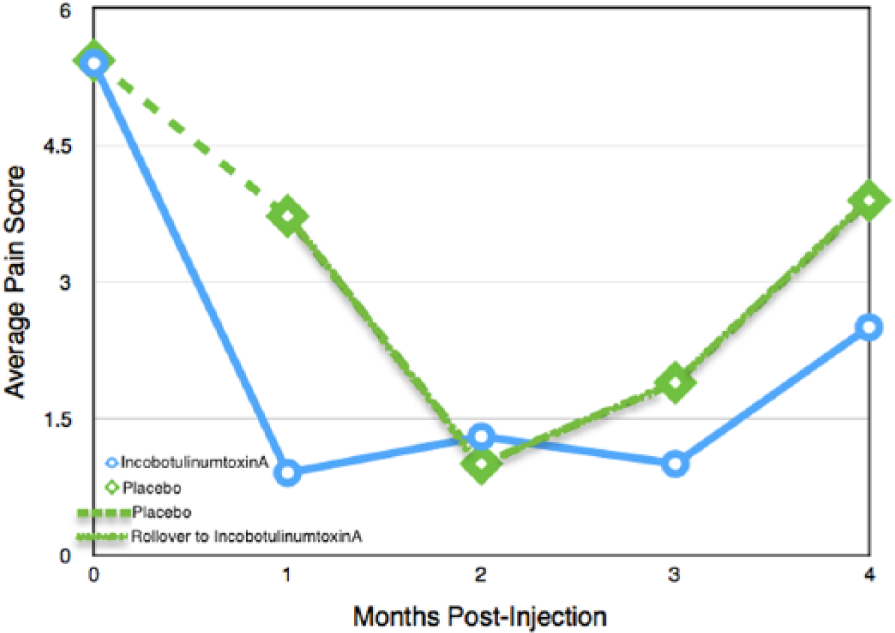
Average pain scores: IncobotulinumtoxinA versus placebo.
Average Pain Scores: Incobotulinumtoxin A Versus Placebo.
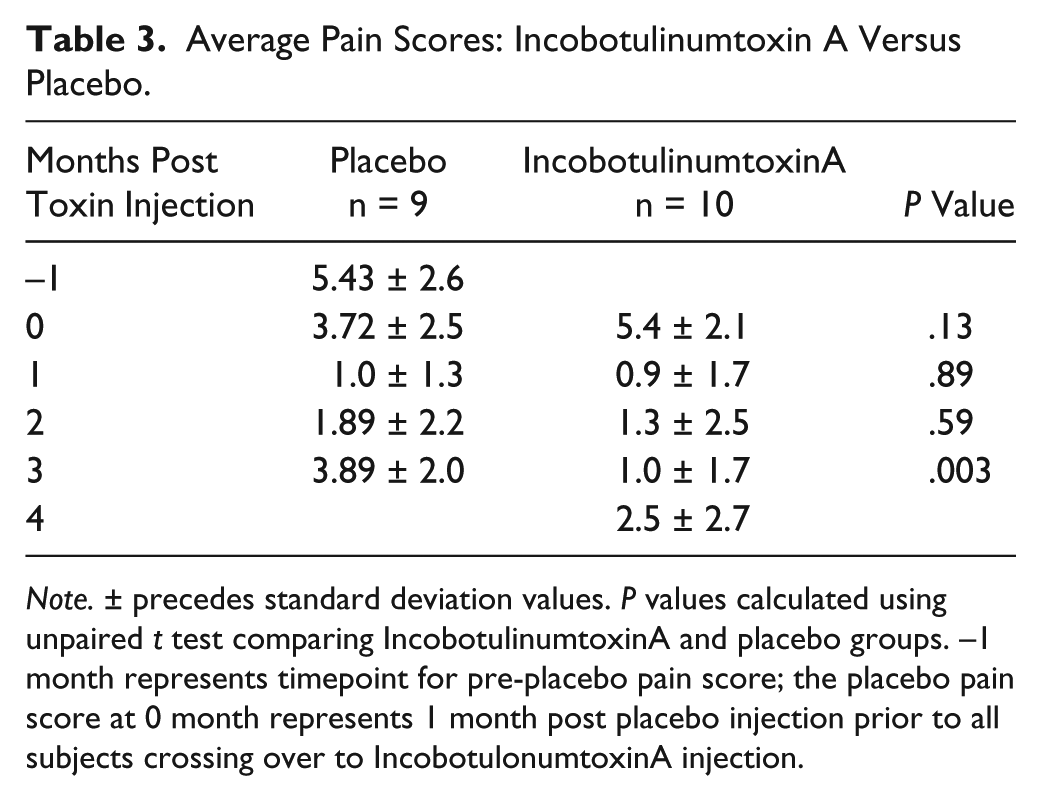
Note. ± precedes standard deviation values. P values calculated using unpaired t test comparing IncobotulinumtoxinA and placebo groups. –1 month represents timepoint for pre-placebo pain score; the placebo pain score at 0 month represents 1 month post placebo injection prior to all subjects crossing over to IncobotulonumtoxinA injection.
In terms of composite masticatory muscle pain to palpation score, initial pain scores were also similar between the 2 groups (placebo = 15.9 ± 3.3 vs IncobotulinumtoxinA = 14.9 ± 3.9, P = .566). At 1 month, there was a statistically significant difference in the groups in terms of composite pain score (placebo = 13.8 ± 3.7, IncobotulinumtoxinA = 8.6 ± 2.8, P = .003). After crossover, at 2, 3, and 4 months, similar composite scores were noted between the two 2 (Table 4, Figure 2).
Composite Masticatory Muscle Tenderness Scores: IncobotulinumtoxinA Versus Placebo.
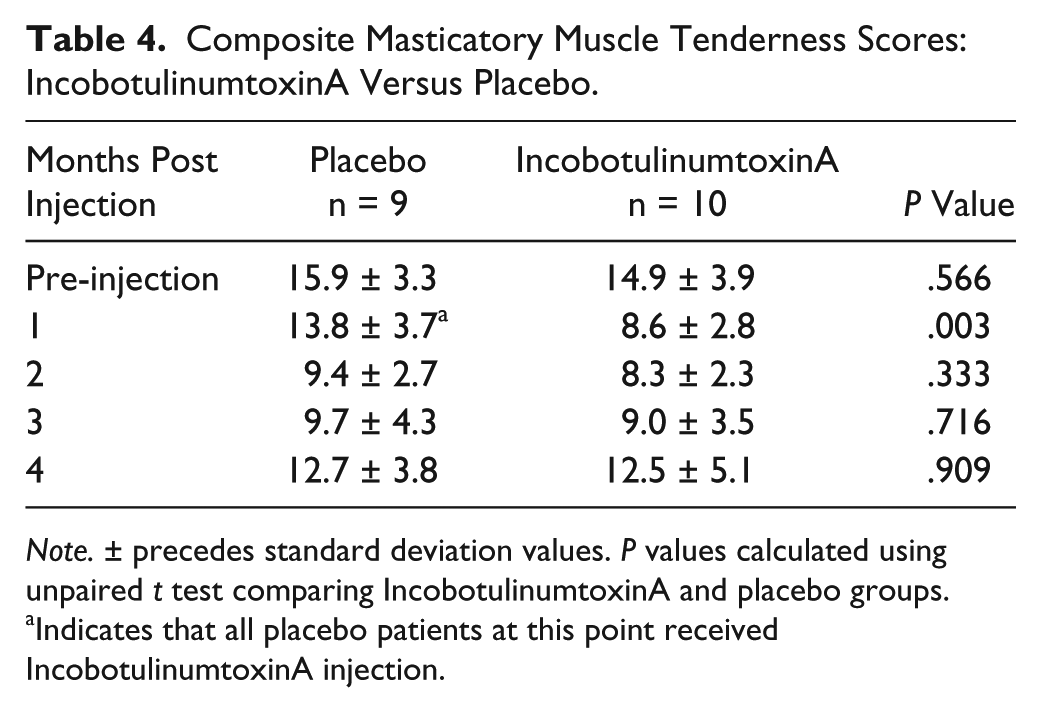
Note. ± precedes standard deviation values. P values calculated using unpaired t test comparing IncobotulinumtoxinA and placebo groups.
Indicates that all placebo patients at this point received IncobotulinumtoxinA injection.
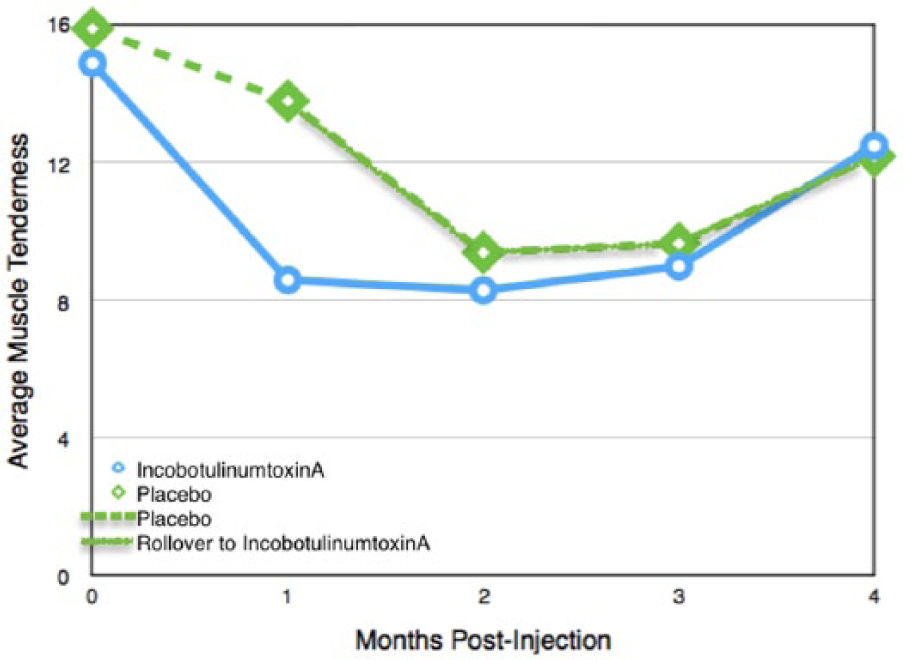
Average composite muscle tenderness scores: IncobotulinumtoxinA versus placebo.
Regarding pain medication usage, no difference was noted at baseline in terms of days of pain medication usage between the 2 groups. Interestingly, an increase in days of pain medication usage was noted in the placebo group after initial injection (17.2 ± 13.3 days of use compared with 11.2 ± 12.7 days of use in the IncobotulinumtoxinA group; Table 5, Figure 3), although this was not statistically significant. For the remainder of the study, no difference in days of pain medication use was noted at any timepoint.
Pain Medication Usage: IncobotulinumtoxinA Versus Placebo.
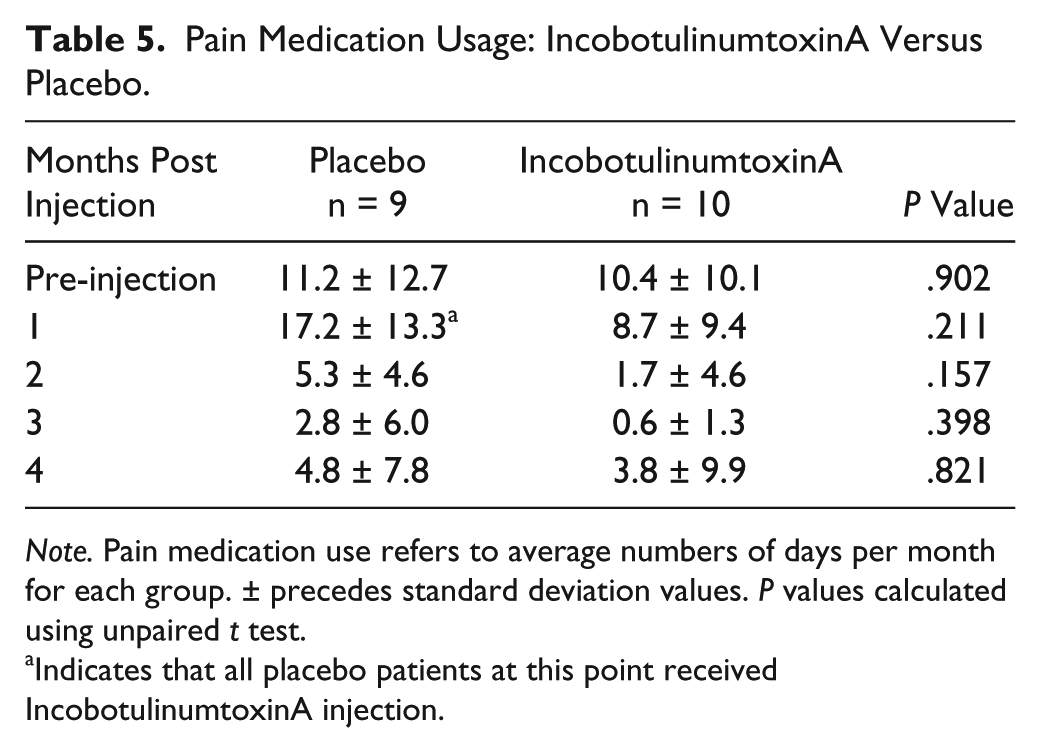
Note. Pain medication use refers to average numbers of days per month for each group. ± precedes standard deviation values. P values calculated using unpaired t test.
Indicates that all placebo patients at this point received IncobotulinumtoxinA injection.
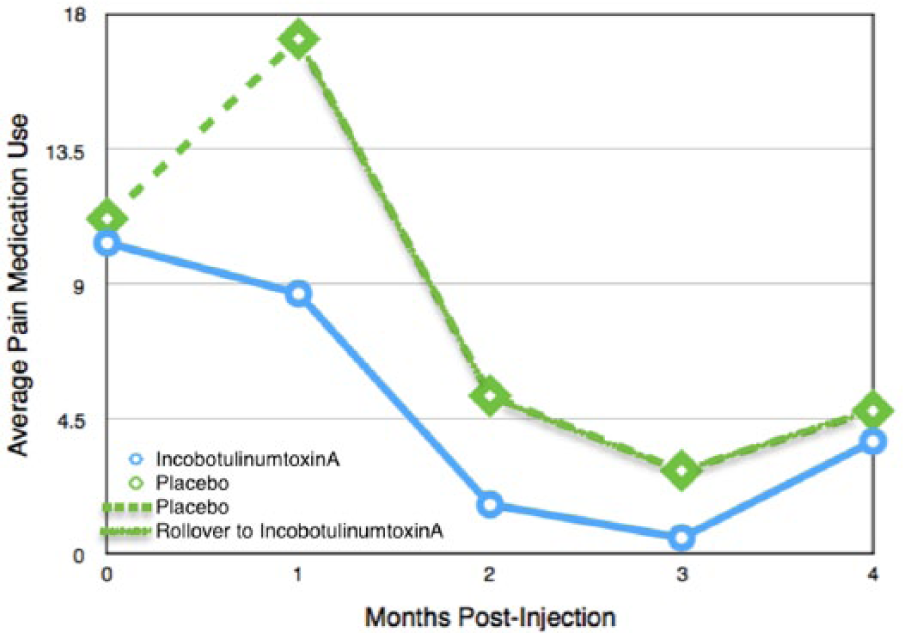
Pain medication use: IncobotulinumtoxinA versus placebo.
Discussion
Temporomandibular disorder describes a spectrum of disorders causing pain of the temporomandibular joint and surrounding structures due to hyperfunction of the muscles of mastication, specifically the masseters and external pterygoids. Previous study of injecting the muscles of mastication with botulinum toxin suggested a role in the treatment of TMD. 13 In this study, we sought to answer whether chemodenervation of these muscles with incobotulinumtoxinA (IncobotulinumtoxinA) would lead to relief of pain associated with TMD in comparison with placebo. When comparing overall pain score at 1 month after injection of placebo versus IncobotulinumtoxinA, both groups showed statistically significant drops in average pain score. It should be noted however that both groups started with a similar pain scores, and the IncobotulinumtoxinA group showed a larger drop in pain scores. While there may be a significant placebo effect, the perceived effect may be due to small sample size. Two other results from this study also argue against a placebo effect. First, when examining the composite masticatory muscle tenderness score (each muscle rated on an increasing pain scale 1-4, maximum composite score of 16), both groups started with similar composite scores. At 1 month, the placebo group showed almost no effect of injection while there was statistically significant drop in composite score in the IncobotulinumtoxinA group. Second, and perhaps even more telling, is all patients in the placebo group reported little relief from injection and were crossed over into the IncobotulinumtoxinA group.
We also examined change in days of pain medication usage. Both groups had similar rates of pain medication usage in the 3 months prior to the study commencement. Interestingly, the placebo group showed a slight uptick in days of pain medication use in the 1 month following initial injection while the IncobotulinumtoxinA group showed a slight decrease, although the difference between the 2 groups was not significant. For the other timepoints, at 2, 3, and 4 months, the number of days of pain medication use was decreased from baseline between the 2 groups, although the difference between the groups was not statistically significant.
Limitations of this study include small study size. It is possible that a truly significant drop in pain scores might be seen with a larger sample size, which is definitely suggested by the change in the composite muscle pain score. Additionally, as a pilot study, the results cannot be absolutely applied to larger generalized groups. The results are encouraging however and suggest that this may be a new way of helping patients, but a larger, multicenter study should be performed. Additionally, although validated for pain studies, there is a certain subjectivity to a 0 to 10 pain scale for overall pain as well as determining degree of muscle tenderness on a 0 to 4 pain scale. There was a suggestion of decrease in pain medication usage, although no result approached significance. This may be related to the fact that patients may have used different type of pain medications (NSAIDs vs opiates, etc) or different preparations within the same class (naproxen vs. ibuprofen, etc) or that the same dose of the same medication between different people leads to different degrees of relief.
Conclusions
We demonstrate in this trial the utility of IncobotulinumtoxinA injection in the treatment of TMD refractory to pain medication and other conventional treatments in comparison to placebo. Patients noted no adverse events during the study and reported significant reduction in pain. Use of IncobotulinumtoxinA for TMD could be considered when weighing treatment options in patients who have failed conservative management.
Footnotes
Authors’ Note
The principal investigator Andrew Blitzer had full access to all the data in the study and takes full responsibility for the integrity of the data and the accuracy of the data analysis. Presented at the 2016 Triological Association in Chicago, Illinois, USA, May 2016, as a poster presentation by Amit A. Patel, MD.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by an unrestricted research Grant from Merz North America.