
Abstract
Objectives:
Surgery for recurrent pleomorphic adenoma (PA) can be challenging and may increase the risk of operative complications, particularly facial nerve weakness. As observation may be a viable alternative to surgery for slow-growing tumors, our objective was to assess the growth rate of recurrent PAs.
Study Design:
This study is a case series of patients at our tertiary academic medical center with recurrent PA. Two magnetic resonance images (MRI) were compared; total volume (TV) of recurrent tumor on both studies was calculated to obtain our main outcomes of percent change in TV and tumor growth rate.
Results:
Fourteen patients with recurrent PA had a median interval time between MRI of 12.8 months. Though growth rates were variable, the median continuous compound growth per year was 10.2%. Notably, 3 patients (21%) had no growth, and 2 patients (14%) had a reduction in TV.
Conclusions:
The median growth rate for enlarging tumors is estimated at 10.2% per year. Due to variability, tumor growth rate should be estimated on an individual patient basis. For slow-growing tumors, physicians may weigh the risk of this slow growth with the morbidity of reoperation.
Introduction
Recurrent pleomorphic adenoma (PA) is a vexing problem to patients and surgeons alike, and currently, there is little established evidence of the growth rate of these tumors. Recurrent PA is likely most often associated with enucleation procedures or inadvertent capsule rupture with tumor spillage but can occur following parotidectomy with negative margins at a rate of 2% to 3%.1,2 Revision surgery of what are often multiple foci 3 of recurrence can be technically challenging with increased morbidity especially to the facial nerve with the potential for 15% to 37% partial facial nerve paresis and 5% to 18% permanent paralysis.4-9
Given the high morbidity of revision surgery, observation of recurrent PA is a potential management choice for select patients. Observation carries the risks of continued tumor growth and malignant transformation. To our knowledge, there is no established data on the growth rate of recurrent PA. To better inform management decisions regarding recurrent PA, the aim of our study was to assess the growth rate of recurrent pleomorphic adenoma at our institution.
Materials and Methods
Institutional Review Board approval was obtained for this study. We performed a retrospective chart review, identifying all cases of recurrent PA at our tertiary academic medical center between the years of 2003 and 2013. Patients were included if they had documented cytologic confirmation of recurrent PA and at least 2 interval magnetic resonance images (MRI) completed at our institution without intervening surgical management or radiation therapy.
A neuroradiologist calculated total volume (TV) assuming an ellipsoid shape of the recurrent tumor on all available imaging studies. This was completed by following the formula (4π/3 × a × b × c) with a, b, and c being the greatest radius in the anterior-posterior, cranio-caudal, and transverse planes, respectively, in millimeters. In cases of multifocal disease, the largest nodule was used for measurement as an estimate of overall tumor burden. The main outcome measures were percent change in TV and tumor growth rate. Management of the tumor and presence of residual disease were also recorded.
Results
Forty-eight patients were diagnosed with recurrent pleomorphic adenoma in the study time period. Fourteen of 48 (29%) of these patients had 2 MRI without intervening definitive management (surgery or radiation).
Fourteen patients were included in the final study, though only 9 tumors showed growth between the 2 MRIs. There were 5 (36%) male and 9 (64%) female patients. The average age was 53.8 years old (range, 23-95 years, median = 55.5). Six patients (67%) had undergone previous resections for recurrent PA and thus were being managed for re-recurrence. Recurrent PA affected the parotid gland in 12 patients and the submandibular gland in the other 2 patients. Ten (71%) of the recurrences were multifocal, with 4 (29%) being unifocal. The average time between scans was 568 days (range, 44-2533 days).
The percent change in total volume ranged from –11.45% to 1023% (Table 1). The average percent change in volume between the 2 imaging studies was 91.6% (range, –11.45% to 1023.66%, SD = 269.90); the median change in volume was 11.15% (IQR = 49.23). Annual percent change was calculated as a continuous compound growth rate for all tumors. The average percent change was 33.4% per year (range, –24.4% to 239.5%, SD = 66.7%). Given the variable growth between the 2 MRIs, median growth is likely more reflective of the natural history of recurrent pleomorphic adenomas. The median growth rate per year was 10.2%.
Volumetric Growth of Recurrent Pleomorphic Adenomas Between 2 Consecutive MRIs. a
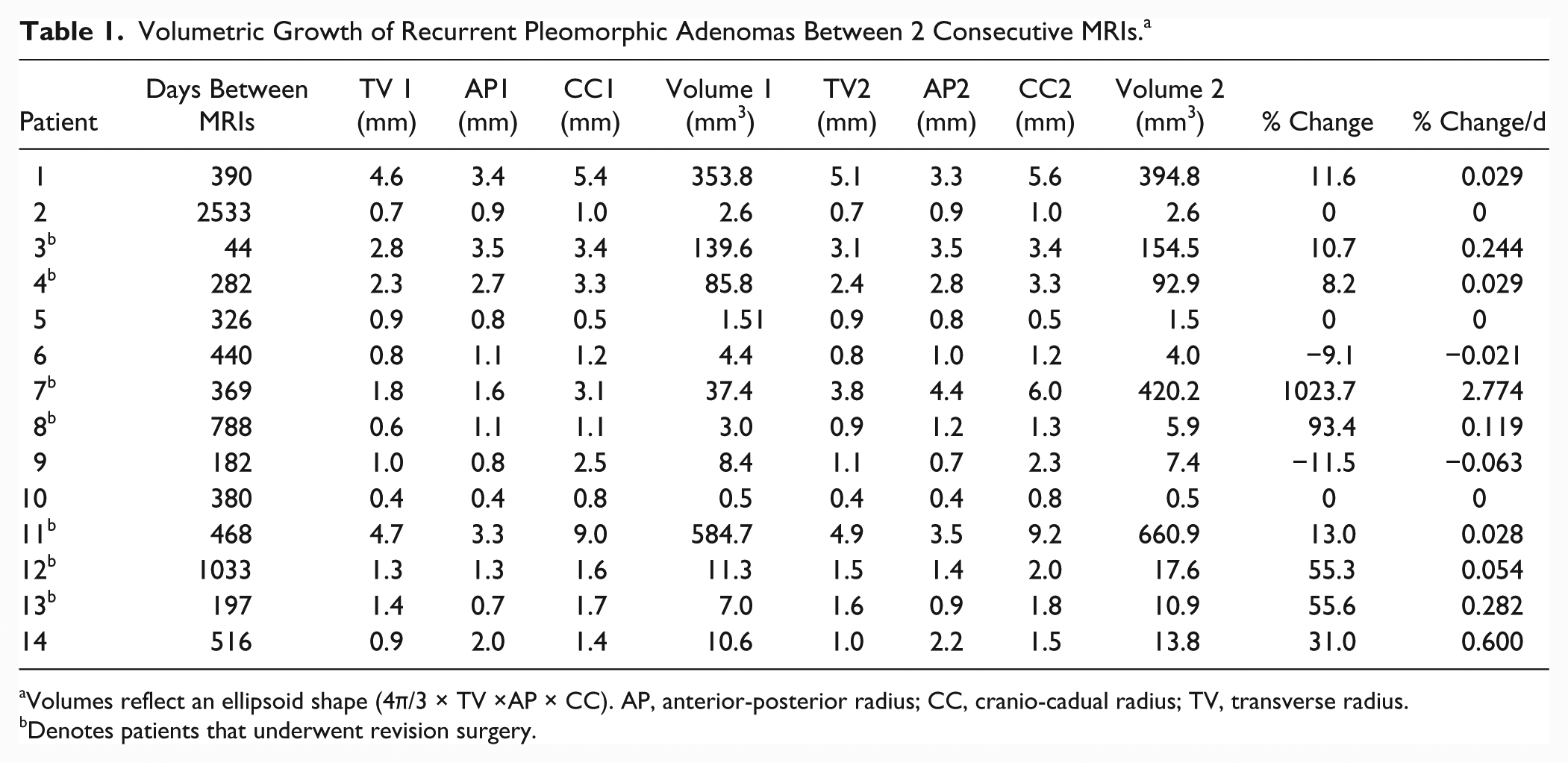
Volumes reflect an ellipsoid shape (4π/3 × TV ×AP × CC). AP, anterior-posterior radius; CC, cranio-cadual radius; TV, transverse radius.
Denotes patients that underwent revision surgery.
Of the 9 patients whose tumors grew, 7 underwent revision surgery. Of this group, the 3 patients not surgically treated were the only 3 patients over the age of 60. Three complications were reported in 3 of the individuals who underwent surgical resection. One patient experienced a facial nerve paralysis (2/6 on the House-Brackmann scale), 1 developed pneumonia, and 1 patient formed a hematoma requiring drainage. Three patients underwent radiation therapy. One patient received radiation and no surgical intervention, and the 2 others received postoperative adjuvant radiation therapy.
With respect to the 5 patients without any growth demonstrated on imaging, and all of these patients were observed.
No patients had evidence of malignant transformation, but the mean follow-up time ranged from only 0 to 5 years.
Discussion
This study demonstrates that the growth rate of recurrent PAs is variable. This is clearly shown by the fact that 2 patients had tumors that appeared to decrease in size, 3 patients had no growth, and rates of growth ranged dramatically for the 9 tumors that did grow. When aggregated, the median annual growth rate can be extrapolated to 10.2% per year.
One patient in particular appeared to skew the data, demonstrating a continuous compound growth rate of 239% per year. This patient presented to our institution after several prior resections at outside hospitals as well as prior radiation therapy. In her chart, a pathology report had noted presence of carcinoma. Pathology at our institution found no evidence of carcinoma on the outside slides nor any evidence of carcinoma following her salvage resection at our hospital. She underwent postoperative radiation following surgery.
Recurrence is a rare but serious complication that may occur following surgery for pleomorphic adenomas of the major salivary glands. Discontinuous capsules, pseudopodia, and multifocality are all inherent tumor characteristics that may all increase the risk of inadvertent tumor spillage.10-12 Iatrogenic rupture of the capsule and seeding of the resection bed is also a well-recognized cause of recurrence when enucleation is performed. 13
To obtain negative margins and avoid the risk of inadvertent capsule rupture, superficial or total parotidectomy is often promoted by surgeons. Recurrence rates occur in 1% to 4% of patients following a superficial parotidectomy and in 0% to 0.4% of patients’ status post a total parotidectomy. 14 Time to recurrence is known to be variable 15 but in general occurs 6 to 10 years following the surgery.16-19
An MRI has been the imaging modality of choice to follow pleomorphic adenomas. 20 Given that yearly MRIs are costly and require scheduling, some physicians have used ultrasound (US) to evaluate for pleomorphic adenoma.21,22 Though it has been shown to be effective to identify PA in the preauricular, submental, and cheek region, 21 it has not been reliably tested to identify the parapharyngeal portion of the parotid. Case reports an endo-cavitary ultrasound has been used to assess and biopsy this area, 23 but this is not universally performed yet in practice. In our series alone, 2 of the 14 patients with recurring PA had parapharyngeal involvement of the parotid. As growth rates continue to be elucidated, US should continue to be studied to determine if it may serve as an adjunct to MRI.
Surgical treatment of recurrent PA can be challenging. Complete excision of multifocal disease in a previously operated surgical field may be difficult unless aggressive wide margins are obtained. Aggressive resection, however, carries with it the risk of facial nerve damage. Wittekindt et al 4 found that only 44% of patients had normal facial nerve function immediately following reoperation for recurrent PA. Some degree of facial nerve dysfunction can be expected in 14% to 18% of patients at long-term follow-up.4,5,7
Though prior studies suggested that untreated PAs have as high as a 24% transformation rate over time, 24 recent evidence also indicates that the rate of ex-pleomorphic carcinoma in recurrent PAs is low. Andreasan et al 1 studied a total of 151 patients with recurrent pleomorphic adenoma and found that malignant transformation occurred in only 3.3% of patients. With such a low rate of malignant transformation, observation may be considered in select cases. Given the morbidity of re-resection, observation is already recommended for the medically frail and elderly. 20
Our data would suggest that for some select patients, regardless of their age or medical co-morbidities, observation may be a viable option. The variable nature of growth of recurrent PAs warrants individualized decision making on whether to attempt surgical resection. Slow-growing or stable tumors may obviate the need for surgical resection. Serial imaging with MRI can help identify a patient’s individual growth rate.
There are several limitations to this study. First, the generalizability of these results is weakened by the small number of patients. The prevalence of recurrent PA is low, and having 2 sequential MRIs for recurrent PA without intervention (surgery or radiation) is rare. Second, given the great amount of variability of change in growth, the averages may not have a significant clinical impact. Given that rates have not been elucidated previously, these rates still have academic value. Third, we did not measure each foci of recurrent tumor separately, instead relying on the largest tumor to represent the rest. This could result in a distortion of the true growth rate. Additionally, not every single focus of presumed tumor on imaging was biopsy-proven PA. Given the low number of patients and inconsistent reporting prior to presentation to our institution, we were unable to comment on any trends in growth regarding age, sex, location, gland, or interval from original surgery. Finally, the follow-up time was short, and in combination with the low number of patients included, this is unlikely to provide any meaningful data on the risk of malignant transformation.
Conclusion
The growth rate of recurrent PA is variable. The median growth rate for tumors is estimated at 10.2% per year. The tumor growth rate should be estimated on an individual patient basis, with rate established by MRIs. For slow-growing tumors, physicians may weigh the risk of this slow growth with the morbidity of reoperation.
Footnotes
Acknowledgements
The authors would like to acknowledge Azina Uzelac, assistant clinical professor of neuroradiology, for her effort and collaboration.
Authors’ Note
Triological Combined Sections Meeting, January 23, 2016, Miami, Florida, USA.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.