
Abstract
Objective:
We wished to investigate the risk factors for stoma recurrence following laryngectomy.
Methods:
PubMed, Cochrane Library, and Embase were searched to identify primary research studies published between January 1, 1967, and October 31, 2016. We only included observational epidemiological studies and used risk ratios (RRs) and 95% confidence intervals (CI) to summarize the primary risk factors associated with recurrence following laryngectomy.
Results:
A total of 44 articles, including 11 928 patients, were included in the current meta-analysis. The pooled estimates of the stomal recurrence rate and the local recurrence rate following laryngectomy were 6.60% (95% CI, 5.40-7.90) and 19.40% (95% CI, 14.00%-24.80%), respectively. For stomal recurrence, we confirmed a series of earlier identified factors, including tumor site, prior tracheotomy, tracheotomy timing, T-classification, lymph node metastases, postoperative pharyngoperistomal fistula, and a positive surgical margin. For local recurrence, postoperative radiotherapy, overexpression of p53, and overexpression of p21 were significant, while preoperative tracheostomy and postoperative pharyngoperistomal fistula had an unexpectedly low impact on risk.
Conclusion:
This study has confirmed a series of earlier identified factors for stomal recurrence and local recurrence following laryngectomy. Our results will provide important insights for clinical practice.
Introduction
Laryngeal cancer is the most common cancer of the head and neck, with almost 13 400 new cases diagnosed in the United States annually and accounts for 3.5% to 5.1% of all new malignancies worldwide each year.1,2 The treatment options for laryngeal cancer include surgery, radiation therapy, and chemoradiation therapy, alone or in combination. Total laryngectomy (TL) is usually reserved for advanced laryngeal cancer and cases that recur after radiotherapy or chemoradiotherapy due to its good local control. 3 However, tumor recurrence at the tracheal stomal following total laryngectomy for a laryngeal cancer is still a well-recognized phenomenon, with an overall incidence ranging from 2% to 15%. 4 Stoma recurrence is one of the most severe complications of laryngeal cancer and commonly considered to be incurable. Even with aggressive surgical therapy and radiotherapy, these patients usually succumb to respiratory obstruction or massive haemorrhage.
To the best of our knowledge, only 1 systematic review of this topic has been published, in 2013 in a Chinese journal, which reported that transglottic location, tumor T-staging, and preoperative tracheotomy were important risk factors of recurrence after total laryngectomy. 5 Discouragingly, authors from other countries cannot access this review due to the lack of an English version of this review. We wished to update the systematic review of this topic in English and provide the information for more authors in the world. We also wished to include papers focused on distinct recurrence and more risk factors and add some important subgroup analyses to provide a full-scale and novel information on this topic.
Materials and methods
Study Selection
We searched PubMed, Cochrane Library, and Embase to identify primary research studies published between January 1, 1967, and October 31, 2016, that reported risk factors of cancer recurrence after laryngectomy for laryngeal carcinoma. The following keywords were used in this study: stomal recurrence, tracheostomal recurrence, peristomal recurrence, local recurrence, local control, tumour recurrence, and laryngectomy. To identify other studies, we also hand searched references from the retrieved articles. We used only data from published articles and did not include data from meetings or conference abstracts. No language restrictions were applied to the search.
For inclusion, studies had to meet the following criteria:
observational epidemiological studies of the risk factors of tumor recurrence after laryngectomy for laryngeal carcinoma;
reported stomal recurrence or local recurrence after laryngectomy;
reported at least 1 risk factor potentially related to tumor recurrence;
reported the prevalence or the relative risk (RR) estimates, along with either corresponding 95% confidence intervals (CIs) or raw data enabling the calculation of 95% CIs.
We excluded studies that contained overlapping data. When there were multiple publications that used the same data set, only the largest study was included. We excluded studies utilizing animal experiments, review articles, letters, and conference abstracts. We also excluded papers reporting only cancers of the head and neck that did not clearly define stomal recurrence or local recurrence, did not include laryngectomy in laryngeal cancer patients, and had a sample size of less than 30 patients.
Two authors searched the electronic databases independently using the same methodology. The same authors determined whether abstracts and full-text articles met the inclusion criteria independently. If discrepancies occurred, a third author performed an additional assessment.
Data Extraction
Two authors extracted the data independently using a standard protocol, and a third author reviewed the results. Disagreements were resolved by discussion with our research team. For each study, the following information was extracted: first author of the paper, year of publication, type of study, country, risk factors, total sample size, mean age of the patients, definition of the patients, treatment modality, tumor recurrence types, number of tumor recurrences, and total patients in different risk groups.
We used the Agency of Healthcare Research and Quality (AHRQ) for cross-sectional study quality to rate the methodological quality of the eligible studies. The ARHQ methodology checklist is applicable for observational studies, including 11 items with a yes/no/unclear response option: Yes would be scored 1, no or unclear was scored 0, and an individual study can have a maximum of 11 quality points. Studies were deemed to be low quality (0-3), moderate quality (4-7), and high quality (8-11).6,7
Primary Outcome Measures
Laryngeal cancer recurrences were categorized as local, regional, loco-regional, or metastases at distant sites. Local recurrence was defined as any case of recurrent cancer in the central neck, around the stoma, or inside the neopharynx, esophagus, or base of tongue. Local recurrence was divided into stomal recurrences and pharyngeal/base of tongue recurrences according to recurrence site. Stomal recurrence was defined as a diffuse infiltrate of neoplastic tissue at the junction of the trachea and skin after a total laryngectomy, involving the stoma or the peristomal soft tissues in the central neck.
Meta-analysis Methods
We used odds ratios (ORs) and 95% CIs to summarize the primary risk factors associated with stoma recurrence or local recurrence following laryngectomy. We also used weighted mean difference (WMD) and 95% CI to compare the difference in the average time interval between the performance of emergency tracheostomy and laryngectomy in the patients who did and did not develop stomal recurrences (days). The degree of heterogeneity was assessed by χ2 test (P < .05) combined with the I2 method (I2 > 50% was regarded as high level of heterogeneity). 8 If the included studies have very divergent ORs of risk factors for stomal recurrence or local recurrence, we used a random effect model for meta-analysis. Otherwise, we used a fixed effect model. 9 We performed subgroup analyses by transglottic tumor (glottic-supraglottic, glottic-subglottic), intraoperative tracheostomy (intraoperative tracheostomy at start of operation, intraoperative tracheostomy at a late stage of the operation), and surgery combined with radiotherapy (preoperative radiotherapy, postoperative radiotherapy) to identify the most important risk factors of tumor recurrence. We also used meta-regression analyses to determine whether the year of publication influenced the association between risk factors and tumor recurrences. Publication bias was assessed by visual inspection of the funnel plot. If there is publication bias, for example because smaller studies without statistically significant effects remain unpublished, this will lead to an asymmetrical appearance of the funnel plot with a gap in a bottom corner of the graph. 10 Then, the funnel plot asymmetry was tested using the Egger regression test; if there is asymmetrical funnel plot, the regression line does not run through the origin, and the intercept provides a measure of asymmetry. The larger the deviation of the intercept from zero, the more pronounced the asymmetry. 11 The analyses were performed using the software Stata version 10 (StataCorp LP, College Station, Texas, USA). All P values were 2-sided. A P value of less than .05 was considered to be statistically significant.
Results
Characteristics of Eligible Studies
The study selection process is shown in Figure 1.12 -55 The search terms yielded 2375 potentially relevant papers, 2331 of which were excluded after the abstracts, and full papers were reviewed. Lastly, a total of 44 articles, including 11 928 patients, were included in the current meta-analysis. The majority of the studies (88.64%) were retrospective observations and varied in size from 43 to 1616 patients. Of these, 19 were carried out in European countries, 14 were carried out in Asian countries, 9 were carried out in American countries, and 1 was carried out in an African country. A total of 29 studies provided data for the stomal recurrences, whereas the remaining 15 analyzed the risks of local recurrences following laryngectomy.
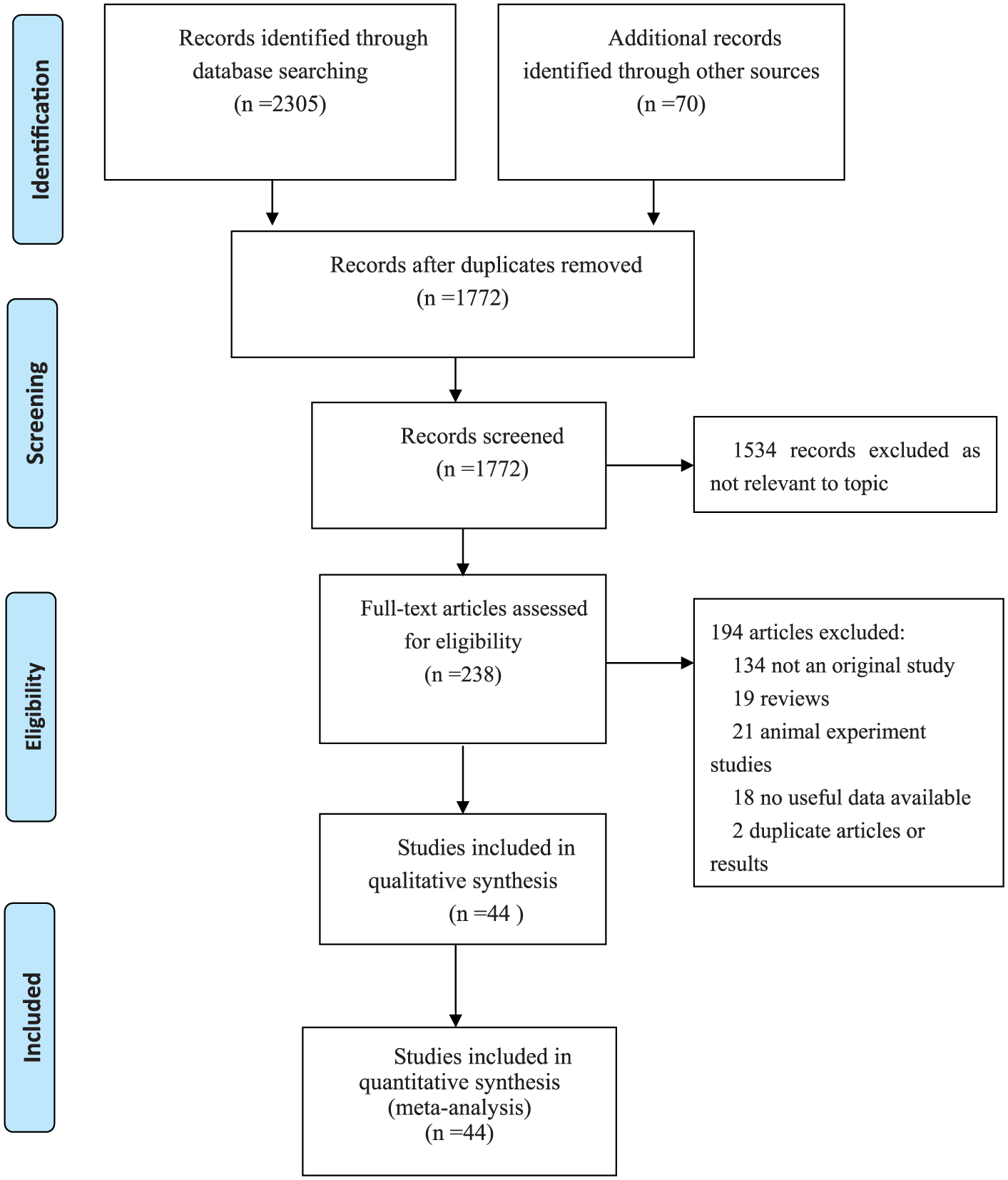
Prisma 2009 flow diagram literature search and study selection. PRISMA diagram showing the different steps of systematic review, starting from literature search to study selection and exclusion. At each step, the reasons for exclusion are indicated.
According to ARHQ, 23 studies were rated as high quality, 21 studies were rated as moderate quality, while no study was rated as low quality (Table 1).
Characteristics of the Studies Included in the Meta-analysis.
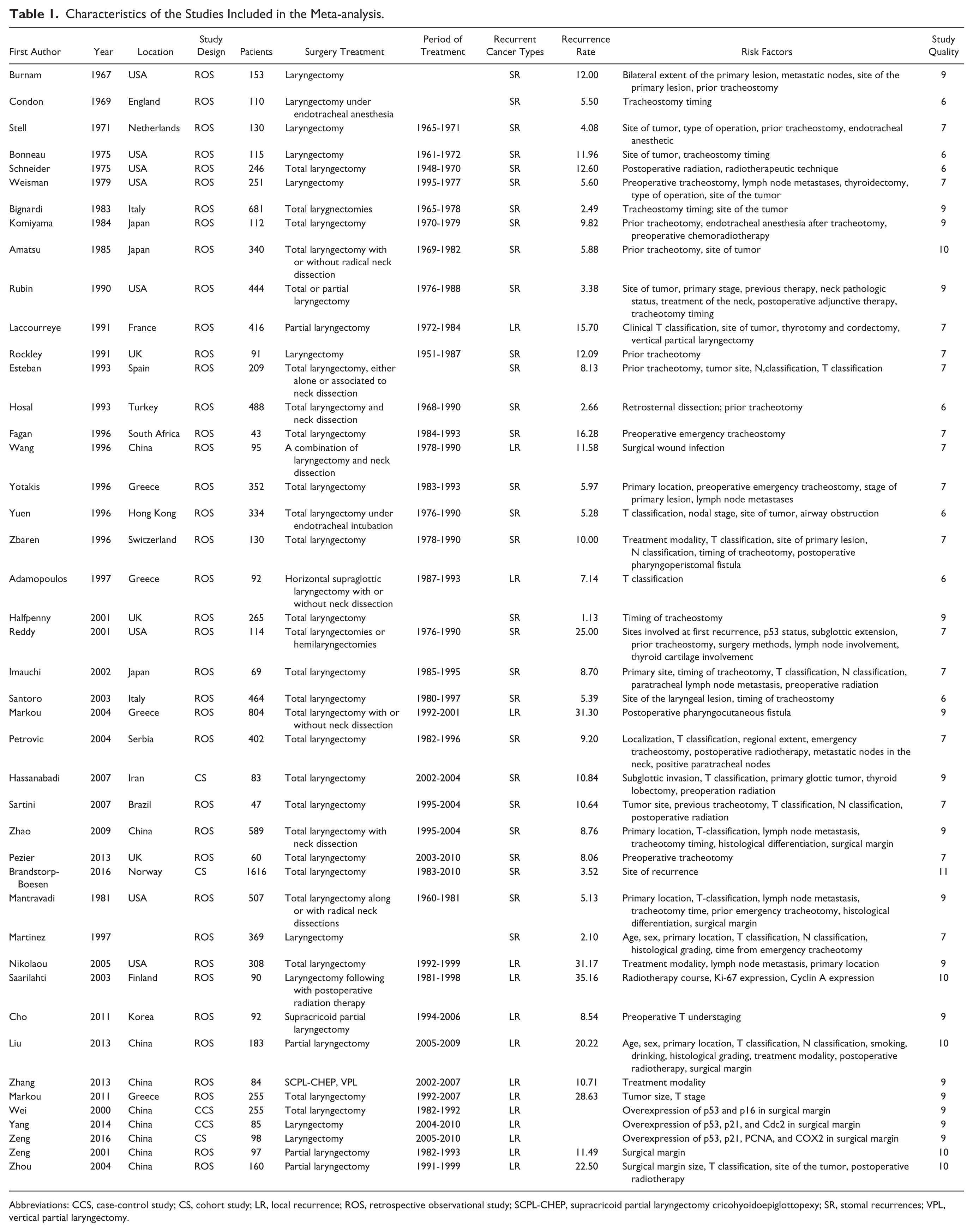
Abbreviations: CCS, case-control study; CS, cohort study; LR, local recurrence; ROS, retrospective observational study; SCPL-CHEP, supracricoid partial laryngectomy cricohyoidoepiglottopexy; SR, stomal recurrences; VPL, vertical partial laryngectomy.
The Pooled Estimate of Recurrence Rate Following Laryngectomy
The pooled estimate of the stomal recurrence rate following laryngectomy was 6.60% (95% CI, 5.40-7.90); however, high levels of heterogeneity were observed between studies (Q = 169.42, P < .01; I2 = 83.5%). Figure 2 showed that there may be significant asymmetrical appearance of the funnel plot with a gap in a bottom corner of the graph, indicating that smaller studies with lower stomal recurrence rate may have remained unpublished (t = 7.68, P < .01). Approximately 19.40% (95% CI, 14.00%-24.80%) of patients reported local recurrence following laryngectomy; however, high levels of heterogeneity were observed between studies (Q = 123.28, P < .01; I2 = 91.1%). We found no significant publication bias (t = 0.19, P = .86).
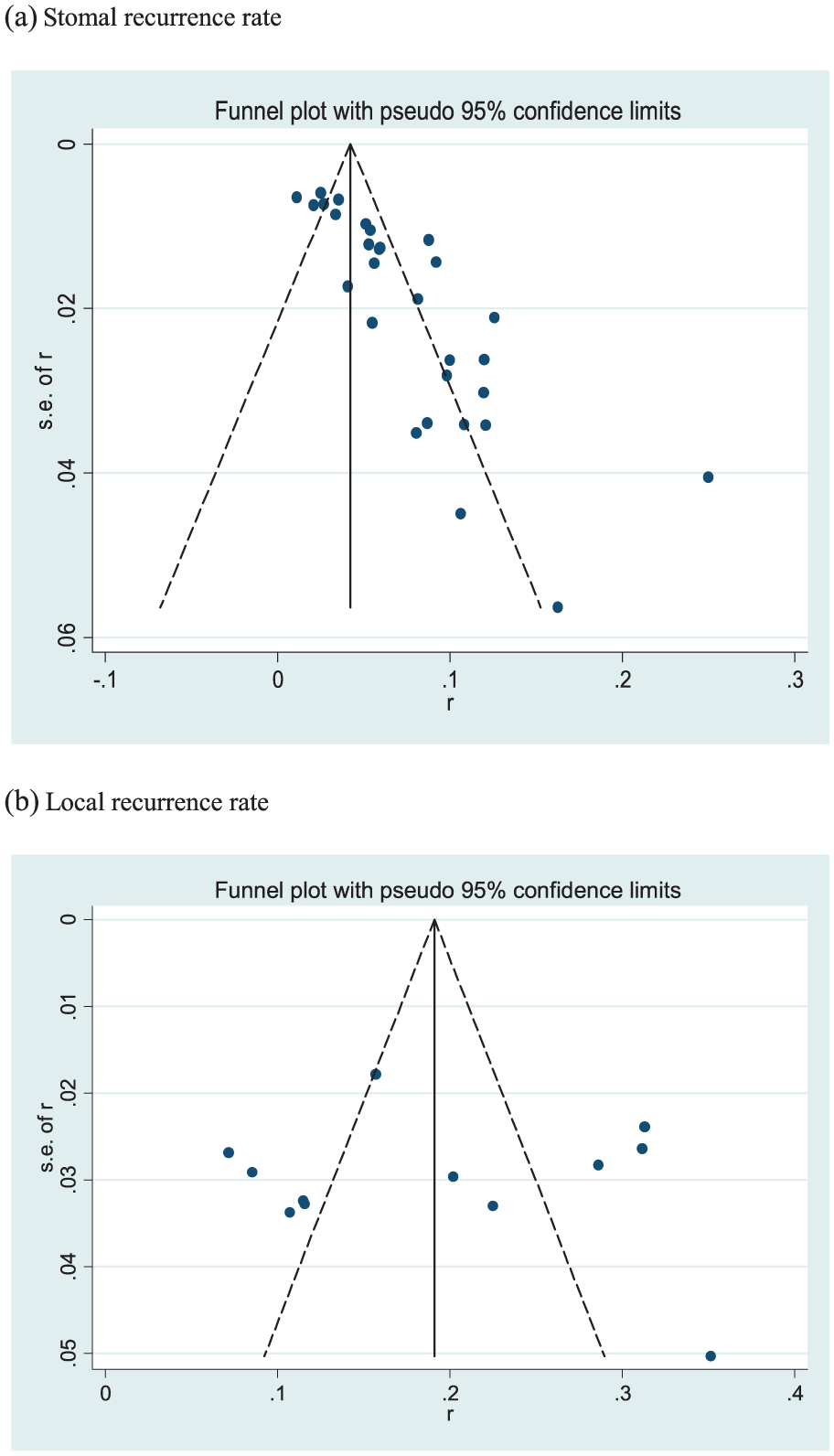
Funnel plots of stomal recurrence rate and local recurrence rate after laryngectomy among patients with laryngeal cancer. (a) Outcome was stomal recurrence rate. (b) Outcome local recurrence rate.
The stomal recurrence rate was highest in African countries (16.30%; 95% CI, 5.20%-27.30%) followed by American (9.70%; 95% CI, 6.30%-13.10%), Asian (7.10%; 95% CI, 5.30%-8.90%), and European countries (5.30%; 95% CI, 3.90%-6.80%). The stomal recurrence rate varied widely from 27.03% (95% CI; 13.37%-47.05%) in glottic-subglottic to 4.28% (95% CI; 3.42%-5.34%) in supraglottic. The stomal recurrence rate was 4 times higher in patients with preoperative tracheostomy at least 24 hours prior to surgery (15.90%; 95% CI, 11.40%-20.40%) than in patients with intraoperative tracheostomy at the time of laryngectomy (3.80%; 95% CI, 2.10%-5.60%). The stomal recurrence rate was positively associated with T staging, with the highest rate (11.80%; 95% CI, 8.30%-15.20%) occurring in patients with T4 laryngeal cancer. The patients with metastatic nodes in the neck, positive surgical margin, postoperative pharyngoperistomal fistula, and p53 overexpression all had a stomal recurrence rate of >20%, but these results should be interpreted with caution due to the small number of studies (Figure 3a).

Estimated stomal recurrence rate and local recurrence rate after laryngectomy among patients with laryngeal cancer. (a) Outcome was stomal recurrence rate. (b) Outcome was local recurrence rate.
The distribution tendency of local recurrence rates following laryngectomy was similar to the stomal recurrence rate. The local recurrence rate was highest in American countries, followed by European and Asian countries. The patients with laryngeal cancer involving the subglottic also showed a higher local recurrence rate than those who did not (Figure 3b).
We also performed meta-regressions analyses to explore the temporal trend of stomal recurrence rates and local recurrence rate following laryngectomy, and the results indicated that neither the stomal recurrence rate (t = −0.11, P = .91) nor the local recurrence rate (t = 1.18, P = .26) was affected over time (Figure 4).
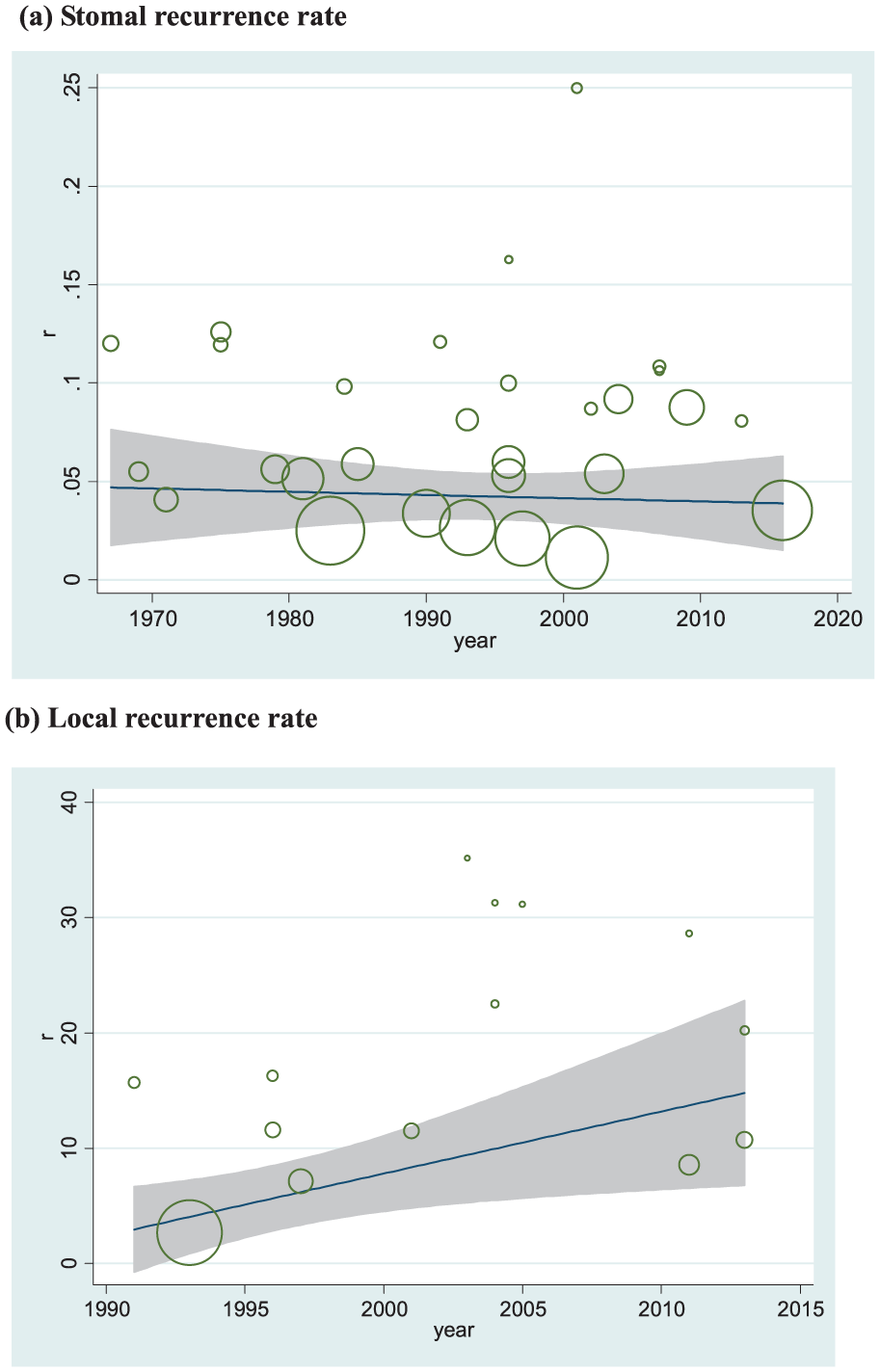
Meta-regression of recurrence rate with publication years as a moderator. (a) Outcome was stomal recurrence rate (t = −0.11, P = .91). (b) Outcome local recurrence rate (t = 1.18, P = .26). Circles present the recurrence rate reported in each study. Circle size is directly proportional to the relative weight of each study.
Meta-analyses of the Risk Factors Associated With Stomal Recurrence After Laryngectomy
The primary outcomes of the meta-analyses are shown in Table 2. Compared to the patients with supraglottic cancer, those who with transglottic cancer (OR = 3.85; 95% CI, 2.54-5.81), subglottic cancer (OR = 4.80; 95% CI, 2.73-8.46), and glottis-subglottic cancer (OR = 5.36; 95% CI, 2.65-10.87) were more likely to suffer from stomal recurrence after laryngectomy. Compared to the patients with T1-2 laryngeal cancer, those with T4 laryngeal cancer (OR = 2.13; 95% CI, 1.06-4.27) were more likely to suffer from stomal recurrence after laryngectomy.
Summary Estimates for the Risk Factors of Stomal Recurrence and Local Recurrence After Total Laryngectomy.
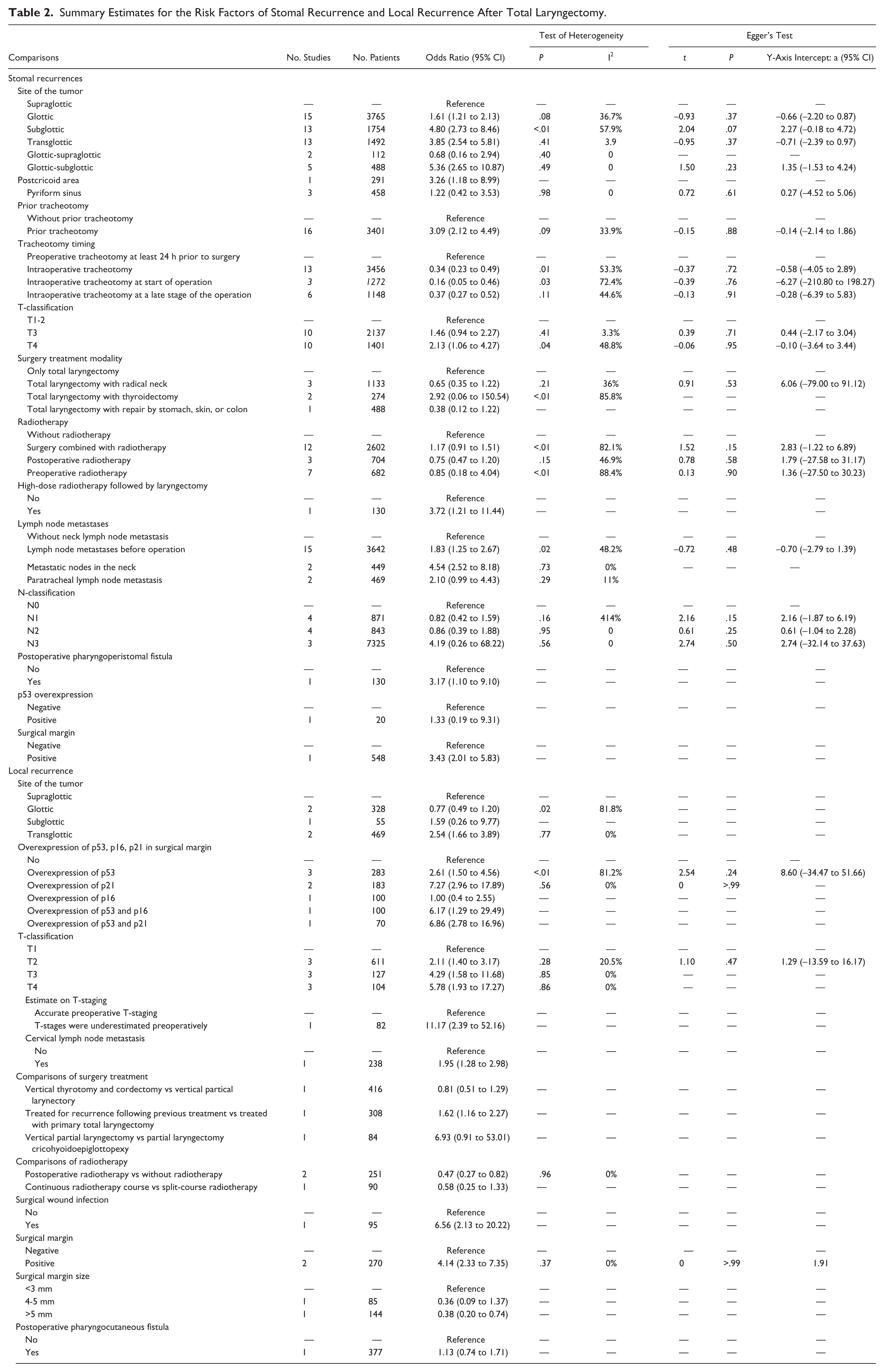
The pooled relative risk of stomal recurrence was significantly higher among patients with prior tracheotomy than among patients without prior tracheotomy (OR = 3.09; 95% CI, 2.12-4.49). Considering the tracheotomy timing, the pooled relative risk of stomal recurrence was significantly lower among patients with intraoperative tracheostomy than patients with preoperative tracheostomy at least 24 hours prior to surgery (OR = 0.34; 95% CI, 0.23-0.49). We also performed the analyses to determine the effect of treatment modality on the risk of stomal recurrence after laryngectomy. We found no significant difference between total laryngectomy only and total laryngectomy combined with radiotherapy, radical neck, thyroidectomy, and repair by stomach, skin, or colon. Interestingly, the pooled relative risk of stomal recurrence was significantly higher among patients with high-dose radiotherapy followed by laryngectomy than among patients without (OR = 3.72; 95% CI, 1.21-11.44).
The pooled relative risk of stomal recurrence was significantly higher among patients with lymph node metastases before operation, including regional cervical lymph nodes and distant metastases to the lung or other locations, than among those without (OR = 1.83; 95% CI, 1.25-2.67). Furthermore, when only including the patients with metastasis to regional cervical lymph nodes, the pooled relative risk of stomal recurrence was significantly higher among patients with metastatic nodes in the neck than among those without (OR = 4.54; 95% CI, 2.52-8.18).
Other risks, for example, postoperative pharyngoperistomal fistula (n = 1), wild type p53 overexpression (n = 1), and positive surgical margin (n = 1), were also analyzed in this study. However, these results should be interpreted with caution due to the small number of studies.
Meta-analyses of the Risk Factors Associated With Local Recurrence After Laryngectomy
The primary outcomes of the meta-analyses are shown in Table 2. We found that the overexpression of p53 (OR = 2.61; 95% CI, 1.50-4.56) and the overexpression of p21 (OR = 7.27; 95% CI, 2.96-17.89) were significantly associated with an increased risk of local recurrence after laryngectomy but had an unexpectedly low impact on risk on stomal recurrence.
We also found that the patients whose T-classification was underestimated preoperatively (OR = 11.17; 95% CI, 2.39-52.16) with cervical lymph node metastasis (OR = 1.95; 95% CI, 1.28-2.98), surgical wound infection (OR = 6.56; 95% CI, 2.13-20.22), and a positive surgical margin (OR = 4.14; 95% CI, 2.33-7.35) were more likely to suffer from local recurrence. However, these results should be interpreted with caution due to the small number of included studies.
Evaluation of Publication Bias
We assessed funnel plot asymmetry using Egger’s linear regression test, and the results are shown in Table 2. We found no significant publication bias for all primary outcomes.
Discussion
To the best of our knowledge, this is the first study to systematically analyze the risk factors of laryngeal cancer recurrence following laryngectomy in English. We subdivided cancer recurrence into stomal recurrence and local recurrence and found distinct risk factors for each. For stomal recurrence, we confirmed a series of earlier identified factors including tumor site, prior tracheotomy, tracheotomy timing, T-staging, lymph node metastases, postoperative pharyngoperistomal fistula, and positive surgical margins. However, postoperative radiotherapy, the overexpression of p53, and the overexpression of p21 were significantly associated with the risk of local recurrence but had an unexpectedly low impact on risk on stomal recurrence. Stomal recurrence is a common pattern of local recurrence and might have different causative factors with other patterns of local recurrence. This meta-analysis presented complete and reliable results regarding the risks of stomal recurrence following total laryngectomy. Over the past several years, there has been a substantial development in the strategies to treat early and advanced laryngeal cancer. The objective of laryngeal cancer management is cure with preserved larynx function. To achieve this, it is vital to assess the risk of recurrence in each patient with laryngeal cancer. Early detection of recurrent laryngeal cancer is a very important contributor to a successful disease outcome. Thus, confirmation of earlier identified factors for recurrence in our study would be highly relevant to the clinician.
We found that the stomal recurrence rate after total laryngectomy was stable over time, while the slight increase of local recurrence rate was observed from the raw figure in spite of no significant difference. Over the past 20 years, there has been a change in the strategies to treat laryngeal cancer. The operation of laryngectomy is more commonly reserved for either very advanced primary tumors or cases that fail primary nonsurgical treatment. Thus, the changes in treatment paradigms for laryngeal cancer likely contributed to stable or increased recurrence rates. We also found a variable geographical distribution of laryngeal cancer recurrence; for example, the stomal recurrence rate in African countries was about 3 times higher than that in European countries. The geographical distribution of laryngeal cancer recurrence may be explained by socioeconomic status, medical and health services, therapeutic level, and so on.
In this study, we found the presence of a cancer in the subglottis (transglottic or primary subglottic tumors) to be the most important risk factor in stomal recurrence. Moreover, the fact that glottic-subglottic cancer was more likely to cause stomal recurrence than subglottis cancer was presented in our study. Several possibilities could explain the high risk of a subglottic tumor in the development of stomal recurrence. First, subglottic cancers occur in a less common primary tumor location, and cases often present with advanced disease because the symptoms are less obvious.56,57 Second, subglottic cancers are more frequently associated with cervical node metastasis as well as critical airway obstruction, necessitating tracheostomy. 58 Lastly, subglottic cancers have a tendency toward circumferential growth and cartilage invasion. Spread tends to occur outside the larynx through the cricothyroid membrane to the trachea or hypopharynx.
Prior tracheostomy is the most frequently cited risk factor for stomal recurrence after total laryngectomy, and the impact of prior tracheostomy on local control after total laryngectomy is controversial. A total of 16 articles, including 3401 patients, were included in the current meta-analysis, and the increased incidence of stomal recurrence associated with prior tracheotomy was identified. Additionally, we also found that intraoperative tracheotomy was significantly associated with decreased risk of stomal recurrence compared to preoperative tracheotomy at least 24 hours prior to surgery. Our results indicated that tracheotomy might not be associated with an increased risk of stomal recurrence when performed during the surgical operation. In clinical practice, preoperative tracheotomy at least 24 hours prior to surgery is generally required for more advanced cancer and tumors with subglottic extension, while intraoperative tracheotomy is usually performed for the administration of anasthesia before laryngectomy, which might provide a partial interpretation of the different risk of stomal recurrence between preoperative tracheotomy and intraoperative tracheotomy.
The most common and most frequently reported complication of salvage total laryngectomy is pharyngocutaneous fistula, which occurs in 5.6% to 73% of all patients who undergo salvage total laryngectomy, according to a recent systematic review. 57 Our study uncovered an increased incidence of stomal recurrence in patients with a postoperative pharyngoperistomal fistula. This could be the result of viable dislodged tumor cells having had the opportunity to implant in the perifistular tissue near the tracheostoma. However, this result should be interpreted with caution due to the small number of included studies. Furthermore, our review also found some tumor genetic factors, for example, the overexpression of p53 and p21, were linked to an increased risk of local recurrence after laryngectomy. Discouragingly, the associations between these genetic factors with stomal recurrence were not identified due to the lack of relevant papers.
Some of the factors used in our multivariate analysis, such as postoperative infection, lack unified definition or identifying standard across studies. “Not similar enough” means the included studies are difficult to combine in a meta-analysis. Therefore, we have performed rigorous quality control by specifying eligibility criteria, developing data collection form, and assessing the risk of bias in individual primary studies based on the Non-Randomised Studies Methods Group (NRSMG) recommendations. 10 Especially, we have studied very carefully the extent and origin of heterogeneity between included studies when deciding whether to combine the effect values. If included studies were not sufficiently homogeneous to combine in a meta-analysis, we gave up pooled estimate. Considering the observed heterogeneity in the included studies, we used a random-effects model to stay on the safe side. 59
There are multiple limitations to this review. First, stomal recurrence is surely too simple a concept, while local recurrence may take the form of stomal recurrence. Therefore, we cannot ensure whether stomal recurrence and local recurrence have been counted as one in some of the publications because many authors have not provided clear definition for local recurrence in their papers, which may produce obvious information bias in our primary analyses. Second, the results should be treated with caution due to the relatively small number of included studies, highlighting the need for future studies. Third, the majority of studies in this review were retrospective and observational in nature, and patient data were collected over a long time period, producing inevitable inclusion bias. In the end, risk factors associated with laryngeal cancer, including gender, smoking, drinking, overweight/obesity, and physical inactivity, were not assessed due to a lack of data.
Conclusion
In conclusion, we have confirmed a series of earlier identified factors for stomal recurrence following total laryngectomy. These earlier identified factors included subglottic laryngeal cancer, preoperative tracheotomy, higher classification, positive surgical margin, lymph node metastases before operation, and postoperative pharyngoperistomal fistula. Furthermore, we also confirmed some special additional risks that associated with local recurrence, for example, T-classification that was underestimated preoperatively, overexpression of p53 and p21, surgical wound infection, and small surgical margin. Confirmation of these earlier identified factors for recurrence would provide important insights for clinical practice.
Footnotes
Acknowledgements
The authors would like to thank all researchers and participants for their valuable contributions to this article. This work was supported by the Key Science and Technology Project of Anhui Province (1501041147).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.