
Abstract
Objective:
Despite advances in technology and instrumentation, access to the lateral frontal sinus remains a challenge for surgeons. We sought to quantify the reach and applicability of the upper blepharoplasty approach (UBA) to the frontal sinus.
Methods:
Twelve cadaveric specimens were obtained for anatomic research and frontal sinuses divided into 3 zones. Zone 1 was defined as medial to the supraorbital neurovascular bundle (SON). The remaining orbit was then bisected to define zone 2 (centrally) and zone 3 (laterally). Twenty-four UBAs were performed followed by 12 modified endoscopic Lothrop procedures (MELP). The ability to instrument each wall of the frontal sinus was recorded for the MELP, UBA, and combined approach.
Results:
The UBA provided excellent access to the lateral frontal sinus in zones 2 and 3 (89% and 100%). The MELP provided poorer access in zone 3 (67%) but improved access in zone 1 (83%-100%). Access for zone 1 through the UBA was limited. The combined approach yielded 100% access to each frontal sinus boundary.
Conclusion:
The MELP in combination with the UBA/lateral trephination provides excellent access to each frontal sinus boundary. The UBA provides excellent access to the lateral frontal sinus but is limited medially by the SON.
Keywords
Introduction
Frontal sinus pathology presents several unique challenges for the rhinologic surgeon. Benign and malignant sinonasal pathology may involve the anterior or posterior table, orbit, lateral frontal sinus wall or extend intracranially (encephalocele, frontal sinus fractures, malignancies, etc). Access to these anatomical areas and lateral frontal sinus can be challenging via a single approach, and a combination of endoscopic and open approaches has significant utility in more complex cases.1-4 While the coronal approach has the advantage of wide exposure, known risks include scarring, cosmetic deformity, alopecia, and supratrochlear/supraorbital neurovascular bundle injury. 5 The upper blepharoplasty approach offers an alternative to the traditional brow line or sub-brow incisions that are used most frequently for frontal sinus trephination. Upper blepharoplasty incisions are well hidden within the supratarsal crease and offer a cosmetically appealing scar. 6 Further, the upper blepharoplasty approach readily identifies and preserves the supraorbital neurovascular bundle and can allow for placement of a trephine lateral to the neurovascular bundle, allowing direct access to lateral frontal sinus pathology. To date, there have been descriptions of upper blepharoplasty approaches to the frontal bone and sinus, including an approach descried by Moe et al 7 via a transorbital neuroendoscopic surgical approach (TONES). 6 The objective of this cadaveric study was to investigate whether upper blepharoplasty approach provides comprehensive exposure to the orbital roof and lateral frontal sinus while simultaneously allowing access to the medial frontal sinus structures.
Methods
Subjects
A total of 12 cadaver heads were obtained by the University of California Davis Body Donation Program. This study qualifies as exempt status as per the “nonhuman subject research” protocol set by the Institutional Review Board of the institution. Cadaveric heads were deemed appropriate for inclusion in the study if they had pneumatized bilateral frontal sinuses. Exclusion criteria included absent frontal sinuses or prior evidence of frontal sinus trauma. Preoperative cone-beam volumetric computed tomography (CT) (MiniCat, Xoran, Ann Arbor, Michigan, USA) was performed on each specimen.
Baseline measurements detailing aeration of the frontal sinuses were documented and each pattern of aeration characterized into 3 zones. Zone 1 was defined as the area of the frontal sinus medial to the supraorbital neurovascular bundle (SON). The remaining orbit was then bisected to define zone 2 (centrally) and zone 3 (laterally) (Figure 1). Within each zone, access to the frontal sinus was determined by principle investigators (T.O.S. and E.B.S.) to be feasible if the surgeon could both visualize and instrument that region of the frontal sinus. A 70° 4-mm diamond burr was chosen as the instrument to measure with due to its commonality of use during endoscopic frontal sinus surgery (Medtronic-Xomed, Jacksonville, Florida, USA). 8
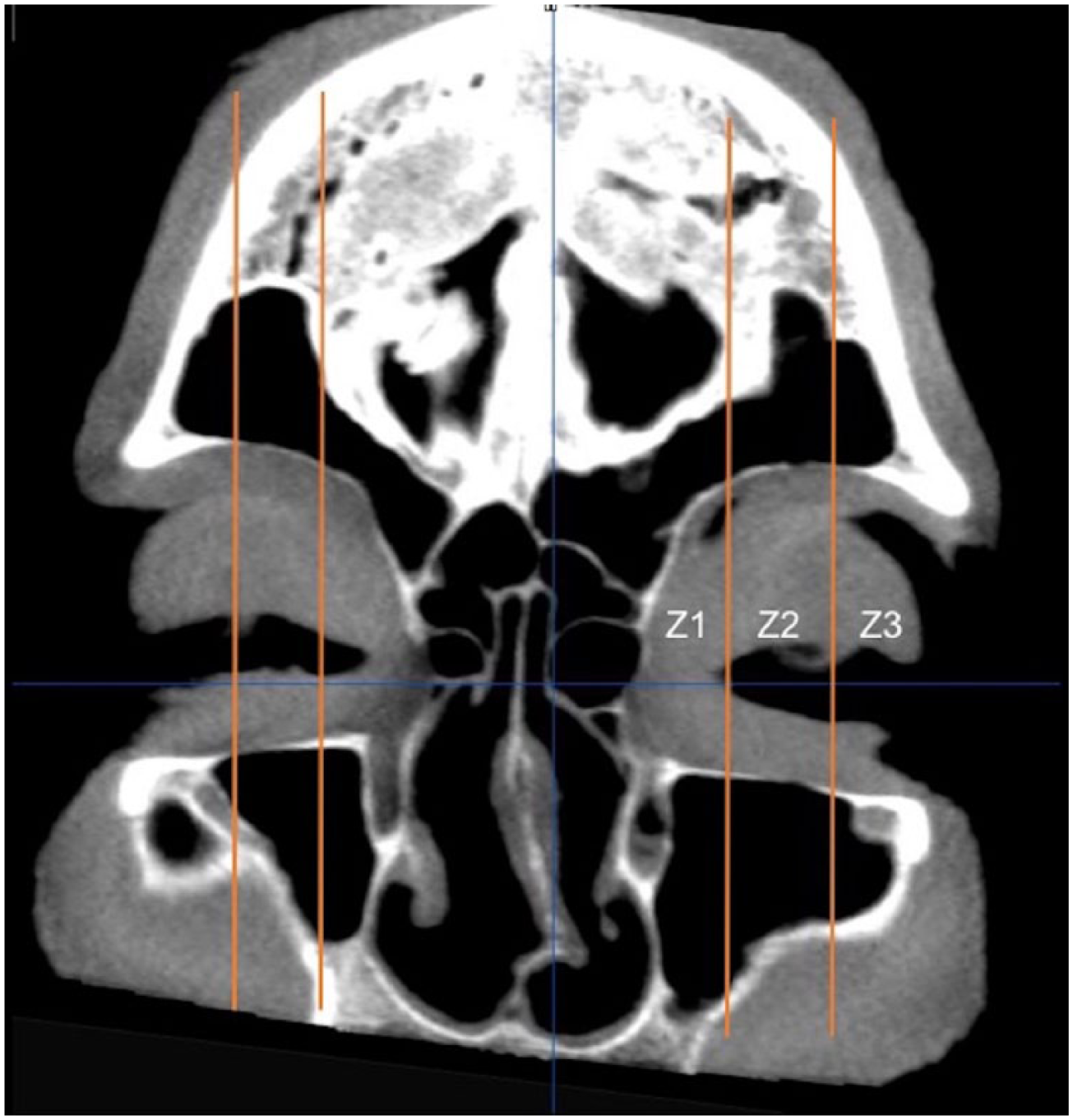
Zones of the frontal sinuses as determined using the supraorbital neurovascular pedicle as delineation between zone 1 and 2. Midpoint between the remainder of the orbit separates zones 2 and 3.
Four walls were evaluated in each zone; A: anterior wall of frontal sinus (A1–zone 1, A2–zone 2, A3–zone 3), P: posterior wall of frontal sinus (P1–zone 1, P2–zone 2, P3–zone 3), O: orbital roof (O1–zone 1, O2–zone 2, O3–zone 3), L: lateral boundary (L1–zone 1, L2–zone 2, L3–zone 3). If the specimen did not contain a zone 2 or zone 3, then only access to zone 1 was measured (eg, no defined access for A2/3, P2/3, R2/3, or L2/3). An intraoperative image guidance system (IGS) (BrainLab Inc, Munich, Germany) was used to confirm access to each zone (Figure 2).
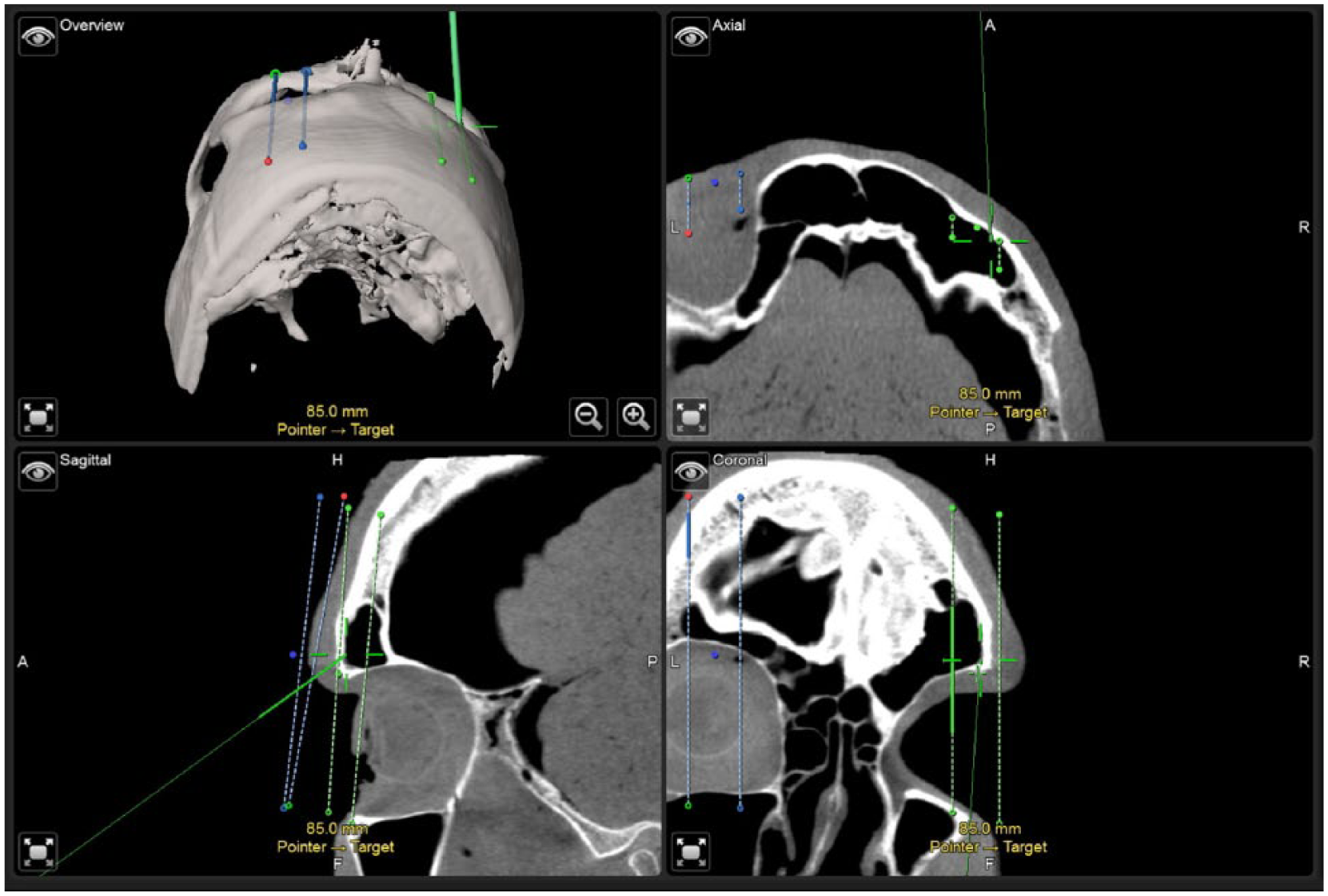
Image depicting confirmation of instrument access to lateral and anterior frontal sinus walls.
An upper blepharoplasty approach was performed through the right and left upper eyelid on each head for a total of 24 approaches. Modified endoscopic Lothrop procedures (MELPs) were then performed on all 12 specimens to access the bilateral frontal sinuses. The zone accessed after completion of the MELP was considered the maximal area that was clinically obtainable. Once blepharoplasty exposure was completed, IGS was utilized to place the frontal sinus trephination at the lateral most aerated aspect of the frontal sinus, lateral to the SON. Each frontal trephination measured approximately 6 mm × 12 mm in size. This was designed to allow dual instrumentation (4-mm endoscope and a 4-mm instrument [drill] or suction, simulating an actual procedure).
Surgical Technique
Upper Blepharoplasty Approach
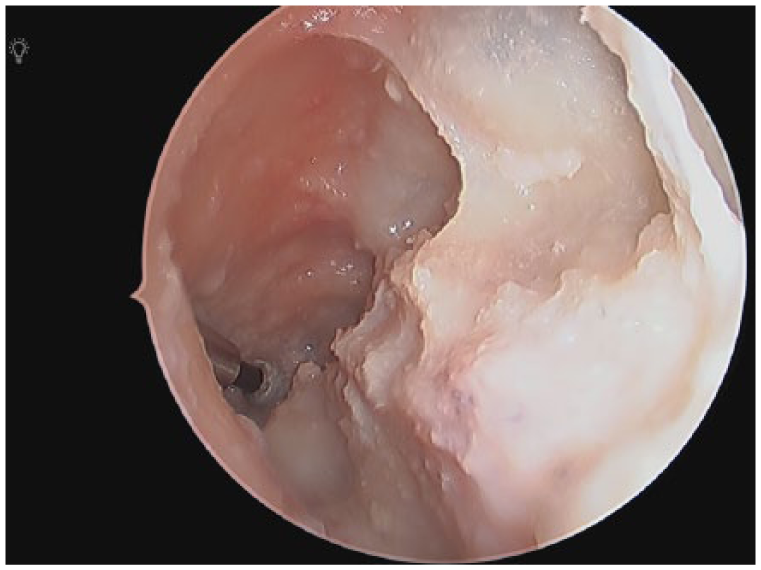
An incision is placed in the supratarsal crease approximately 10 to 12 mm above the eyelid margin. It extends from the supraorbital notch to the lateral canthus. It is initially carried through the skin and orbicularis oculi muscle, allowing the surgeon to identify the orbital septum. Care is taken to avoid violation of the orbital septum as transgression could result in orbital fat herniation and exposure of levator palpebrae superioris. Traction is then applied to the brow, elevating the incision over the bony orbital rim. Electrocautery with a microtip needle is then used to dissect directly onto the frontal bone. Once the rim is palpated, electrocautery is used to incise the periosteum and expose the frontal bone in a subperiosteal plane. The supraorbital neurovascular bundle is identified and preserved. The IGS is used to identify the lateral wall of the frontal sinus. Lastly, a trephination is performed at the lateral most extent of the frontal sinus using copious irrigation (Figure 3).
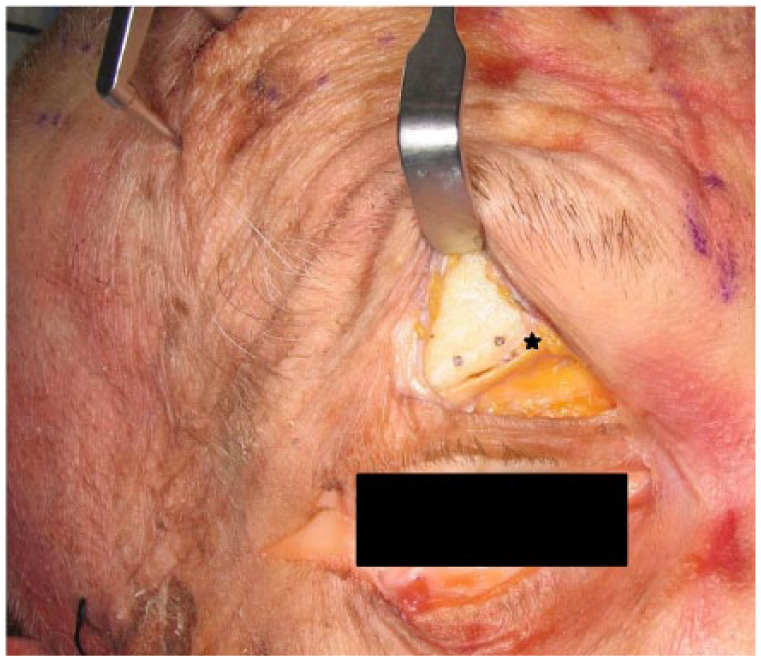
Right lateral frontal sinus trephination site. The supraorbital neurovascular bundle is labeled with a star.
Modified Endoscopic Lothrop Procedure
The MELP, as described by Wormald et al, 9 begins following ethmoidectomy and identification of the ethmoid skull base and lamina papyracea. The floor, posterior wall, and roof of the agger nasi cell are removed utilizing angled telescopes (30°, 45°, or 70°) and through cutting instrumentation. Once the frontal recess has been dissected and an endoscopic view of the frontal sinus is achieved, the same procedure is then performed on the contralateral side. Next, a superior septectomy is performed to achieve bilateral access to the floor of the frontal sinus. Beginning approximately one-third above the base of the middle turbinate, monopolar cautery is used to incise the septal mucosa. This incision is carried superiorly to the roof of the nose and then laterally onto the ascending process of the maxilla. This mucosa may be harvested for later frontal beak mucosal grafting, depending on surgeon preference. The posterior limit of the dissection is the first olfactory neuron. A septectomy is performed to identify the floor of the frontal sinus. Drilling then proceeds from lateral to medial, first identifying the periosteum of the nasal root. The floor of the frontal sinus is then removed, and the true frontal recess is connected to the frontal neo-ostium to create a horseshoe-shaped cavity. The frontal beak is drilled down until periosteum is reached anteriorly.
Results
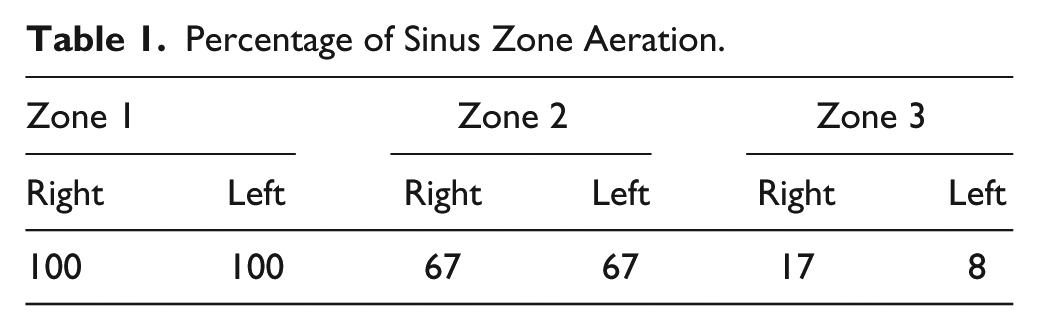
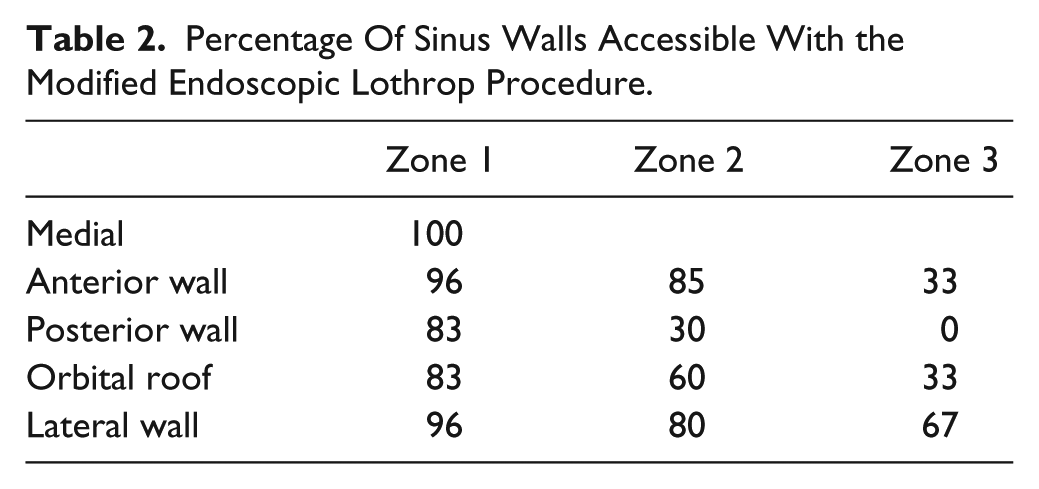
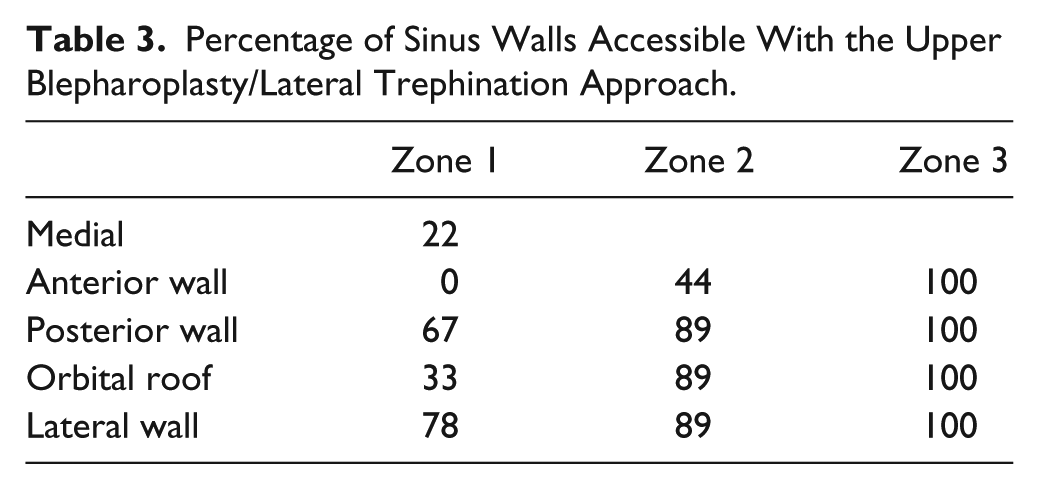
The MELP was performed on all 12 cadaver heads, followed by 24 upper blepharoplasty approaches. In the cadaveric specimens in which the frontal sinus was solely pneumatized to zone 1, a lateral frontal sinus trephination was not possible. In total, lateral frontal sinus trephination was performed in 9 of 24 approaches. The supraorbital neurovascular bundle was identified and preserved in 100% of upper blepharoplasty approaches. Three of 12 cadaveric heads contained pneumatization to zone 3 (Table 1). The MELP provided excellent visibility and instrumentability in zone 1 and zone 2. The most common MELP access limitations included the posterior wall in zone 2 and zone 3, with 30% and 0% of walls being accessible, respectively (Table 2). The most common limitation encountered during upper blepharoplasty and trephination approach was the SON leading to limited medial frontal sinus access. Access to the lateral frontal sinus through the upper blepharoplasty trephination approach provided instrumentation and visibility in 100% of cases in zone 3 (Table 3). Utilizing a combined upper blepharoplasty and MELP, 100% of sinus walls were both visible and accessible under endoscopic visualization (Figure 4).
Percentage of Sinus Zone Aeration.
Percentage Of Sinus Walls Accessible With the Modified Endoscopic Lothrop Procedure.
Percentage of Sinus Walls Accessible With the Upper Blepharoplasty/Lateral Trephination Approach.
Combined access to the lateral frontal sinus through the upper blepharoplasty/trephination and modified endoscopic Lothrop with endoscopic visualization from the endonasal approach.
Discussion
Frontal sinus malignancy, inverted papilloma, encephaloceles, and other rarer sinonasal pathology may involve the lateral and posterior frontal sinus walls, making instrumentation and visualization of the lesion difficult (Figure 5). This study quantifies the exposure that can be achieved using the upper blepharoplasty approach to the lateral frontal sinus. Findings from this study indicate that the upper blepharoplasty approach provides excellent access to the lateral frontal sinus (zones 2 and 3) but is limited when accessing frontal sinus boundaries medial to the supraorbital notch. The upper blepharoplasty approach was found to be an excellent adjunct to the MELP, achieving full access to each bony boundary of the frontal sinus when combined with the upper blepharoplasty. While visualization is vital to tumor surveillance, the ability to manipulate tissue and/or drill bone is of upmost importance to improve the surgeon’s ability to confidently address the source or attachment of the frontal sinus pathology.
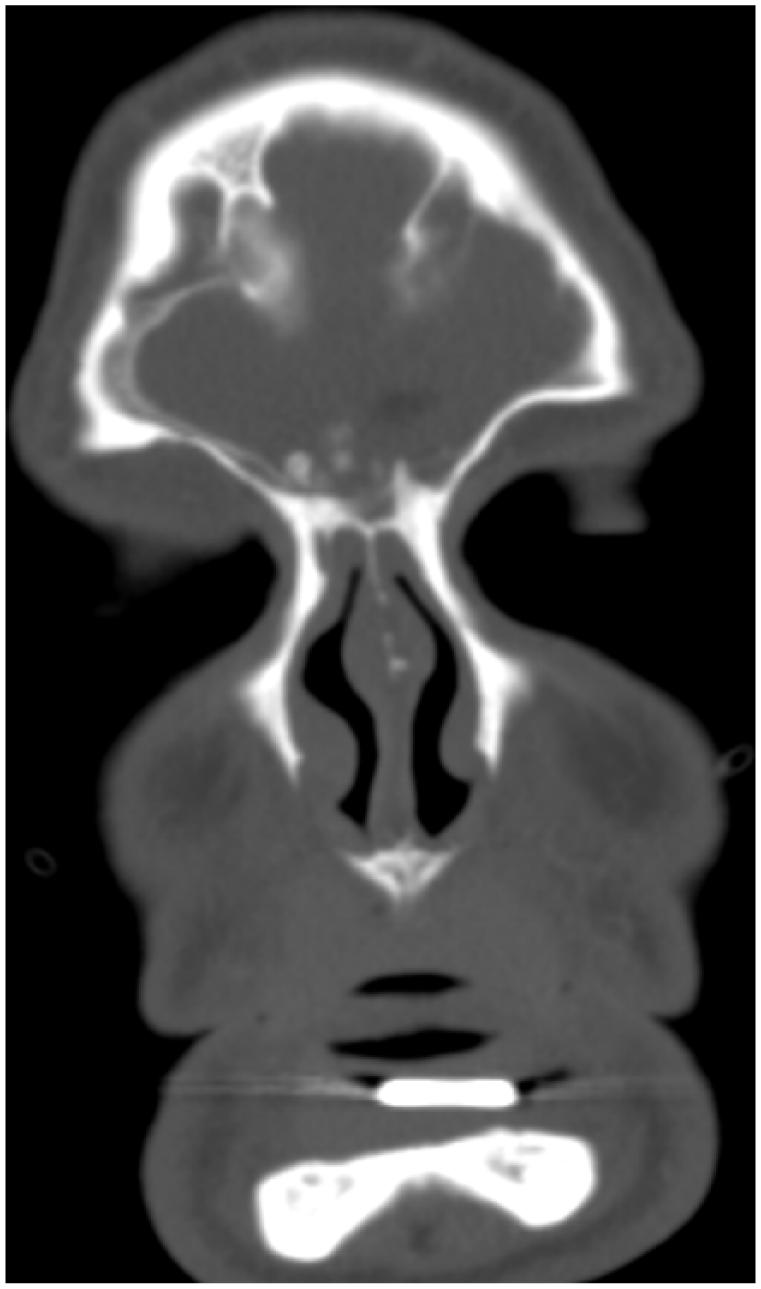
Coronal computed tomography image depicting a mucocele of the right frontal sinus with lateral extension of the bony margin.
Several reports exist examining the feasibility and application of the upper blepharoplasty approach to the frontal sinus. Knipe et al 6 initially described the trans-blepharoplasty approach to the frontal sinus in 2007, performing an upper blepharoplasty approach to the lateral frontal sinus in a series of 5 patients with varied frontal sinus pathology. Importantly, this case series demonstrated that none of patients who underwent the upper blepharoplasty approach developed levator aponeurosis injuries or wound healing problems and all were satisfied with the cosmetic result of the operation. 6 Seiberling et al 10 utilized the upper blepharoplasty approach to the frontal sinus and orbital roof successfully for resection of a frontal sinus osteoma with no reported complications. In 2010, Chu et al 3 described a patient who underwent upper blepharoplasty approach for repair of a superolateral frontal sinus cerebrospinal fluid leak with excellent 1-year cosmetic results and successful closure of the skull base defect, further demonstrating the applicability of the upper blepharoplasty approach to the frontal sinus. TONES as an approach as previously described has been shown to be a viable approach to the orbital apex and optic nerve dissections. 7 The craniotomy created differs based on area of interest. Although upper blepharoplasty approaches are similar, this study presents quantification of accessibility, thereby improving the surgeon’s ability to generate a preoperative plan.
Advantages of the upper blepharoplasty approach include excellent access to the lateral frontal sinus wall, orbital roof, and posterior table of the frontal sinus. The trephination is made lateral to the SON, which is identified and preserved, limiting the potential for forehead paresthesia and avoiding manipulation of the frontal recess mucosa. In addition, the upper blepharoplasty incision is placed within the supratarsal crease and has been reported to result in excellent cosmetic outcomes while avoiding the potential for a more perceptible scar within or just inferior to the brow. Drawbacks include limited medial access to frontal sinus structures, an upper lid incision with the potential for levator aponeurosis injury, and limited applicability for more diffuse frontal sinus pathology.
While the MELP has been employed for frontal sinus pathology for many years, initial long-term patency data suggest that up to 30% of frontal sinuses will reobstruct and require revision surgery. 11 More recent studies, however, indicate that the MELP can be successfully employed for varying frontal sinus pathologies with limited surgical failures. 12 Smith 13 highlighted several recent technological advances thought to decrease stenosis rates, including the implementation of high speed (30k-60k) burrs, improved topical drug delivery, and advent of angled instrumentation and burrs (70°), which allow creation of a larger frontal neo-ostium and improved postoperative medical care. Access to the boundaries of the frontal sinus are dependent on the instrumentation used and endoscopic visualization. Limitations in access to the orbital floor and lateral wall of the frontal sinus have been described. Timperley et al 14 demonstrated access to the lateral frontal sinus in 95% of cases using MELP, though access to the anterior, posterior, and inferior walls of the frontal sinus was more difficult, with less than 55% of each wall accessible. Becker et al 15 described limitations via MELP in accessing the superior and lateral aspect of the frontal sinus, which were only achievable in 54% of cases. Findings from this study are in line with these previous published reports. Of those frontal sinuses with pneumatization to zone 3, the lateral aspect of the frontal sinus was accessible via MELP and a 70° burr in 67% of specimens.
Similar to Timperely et al, 14 the 70° burr was chosen as the instrument to determine access. Access with the drill is important for both frontal sinus malignancy and inverted papilloma as tumor rests may exist within areas of bony osteitis in the sinus. Dual internal and external endoscopic approach allows improved elimination of underlying osteitis, which is considered paramount to prevent recurrence. 16 Pre-dissection CT provides critical information on presence or absence of frontal sinus pneumatization, including information on lateral extent of the frontal sinus. In this study, frontal sinus pneumatization was found to be 100% at zone 1 bilaterally, 67% at zone 2 bilaterally, and on the right 17% and left 8% at zone 3. These findings are similar with the study performed by Timperly et al, 14 which demonstrated 100% pneumatized to zone 1, 57% in zone pneumatization, and only 10% of sinuses pneumatized beyond the midorbital point.
In this study, the most challenging region to access via the MELP was the posterior wall of zone 3. Access was hindered secondary to the curvature of the 70° burr and the anterior projection of the anterior cranial fossa. Woodworth et al 17 suggested that any lesion attached beyond the midorbital point cannot be accessed reliably via MELP, suggesting that surgeons consider ancillary approaches as first line. Our data show that the upper blepharoplasty trephination allows access of endoscopic instrumentation to the lateral wall of zone 3 in 100% of dissections. Zone 2 dissection demonstrated the least amount of access via both MELP and upper blepharoplasty, individually. When approaching zone 2 via MELP, the anterior table was accessed in 85% of specimens compared to 44% via upper blepharoplasty. Conversely, when approaching zone 2 via upper blepharoplasty approach, the orbital floor was accessed in 89% compared to 60% for MELP. Based on these findings, the surgeons may incorporate both a MELP and upper blepharoplasty trephination to fully access the frontal sinus when the origin of the frontal sinus pathology is in zone 2 or zone 3. Critical review of imaging will assist in determining candidacy for each approach.
While this study provides novel data quantifying access to the frontal sinus through the upper blepharoplasty approach, several limitations warrant consideration. The determination of “accessibility” was subjective, and this may introduce bias. Additionally, cosmetic concerns with the upper blepharoplasty approach such as scarring, ptosis, and lagophthalmos were not evaluated because it was a cadaver-based study.
Conclusion
The MELP in combination with the upper blepharoplasty trephination approach provides excellent access to the entire frontal sinus and should be considered when approaching lateral frontal sinus pathology. The supraorbital neurovascular bundle limits medial access to the sinus via an upper blepharoplasty approach; consequently, it has limited utility for far medial frontal sinus pathology.
Footnotes
Acknowledgements
The authors would like to acknowledge Ryan Strong for his assistance with study conduct.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.