
Abstract
Objective:
Sulcus vocalis and vocal fold scar involve derangement of the superficial lamina propria of the vocal fold, which results in significant dysphonia. Many options exist for treatment, most of which have unsatisfactory and unpredictable outcomes. Autologous transplantation of temporalis fascia into the vocal fold (ATFV) has the potential to be a better treatment option, but long-term outcomes have not been well studied.
Methods:
Retrospective chart review and patient survey. Twenty-one patients diagnosed with vocal fold scar or sulcus vocalis and treated with ATFV with at least 1-year follow-up were included. Voice Handicap Index 10 (VHI-10) questionnaires were collected preoperatively and 6 months postoperatively. Patients were reached at the time of the study to complete another VHI-10 and a Likert scale survey.
Results:
The mean decrease in VHI-10 scores between preoperation and 6 months postoperation was 8.35 (P < .001). From preoperation to the time of the study (average 44 months; range, 12-72 months), the VHI decreased 13.53 (P < .001). Eighty-eight percent of patients reported they would recommend this surgery to others with the same diagnosis. Only 1 minor self-limited complication occurred.
Conclusion:
Autologous transplantation of temporalis fascia into the vocal fold for the treatment of vocal fold scar and sulcus vocalis is a safe surgery with good long-term outcomes and high patient satisfaction.
Keywords
Introduction
Sulcus vocalis and vocal fold scar are vocal fold disorders that historically have been very difficult to treat. Each process involves an abnormality of the superficial lamina propria (SLP). While vocal fold scar is primarily a deposition of abnormal tissue within the SLP, sulcus vocalis is characterized by an absence of SLP. 1 The pathophysiology for sulcus vocalis and vocal fold scar are still not fully understood, and it is likely that each disease process may develop via several different mechanisms. They may also cause severe dysphonia with a raspy, thin voice marked by vocal strain and decreased projection.2-4
Several different operations have been developed to remove or modify the disorganized SLP in these disorders with inconsistent results. In 1999, Tsunoda et al 5 introduced the use of the autologous temporalis fascia into the vocal fold (ATFV) as a potential treatment for sulcus vocalis (Figure 1). Tsunoda and colleagues6,7 later published a long-term follow-up that included a total of 10 subjects. These results were promising but lacked the power to demonstrate statistical significance for any vocal measures. Other authors have also shown positive results with this surgery, albeit again using small sample sizes, and in 2 reports, ATFV results were combined with alloderm results.8-11 We first published the results of our use of the ATFV in 2014, which included the analysis of 10 subjects. 12 The current research was designed to be a larger and long-term follow-up of our original report, with the intent of investigating the enduring effects of this procedure on the voice.
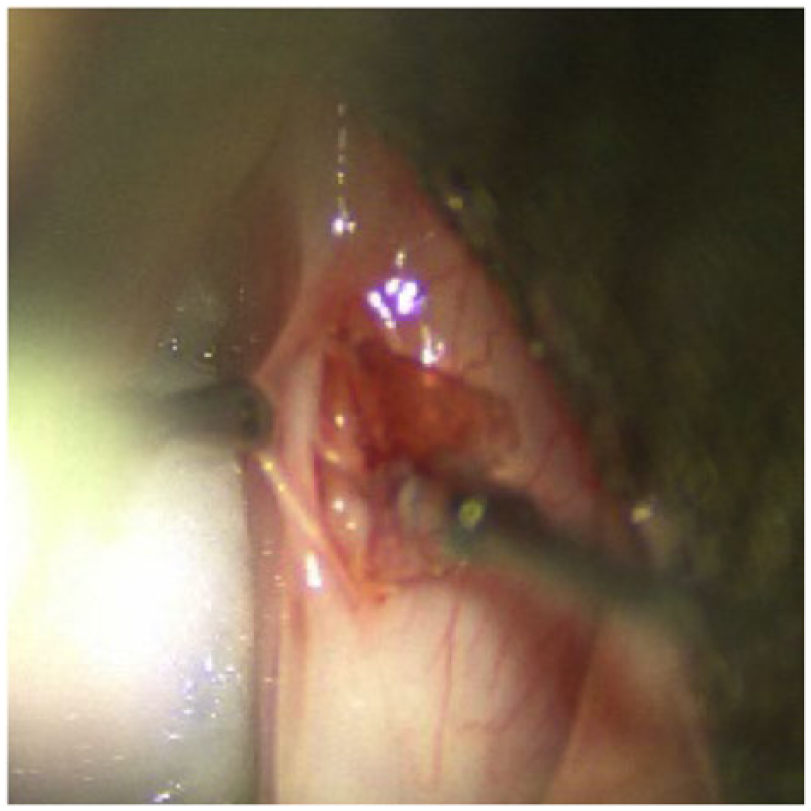
Placement of temporalis fascia. Placement of pressed temporalis fascia into a pocket created in Reinke’s space after elevating the epithelium of a sulcus vocalis.
Methods
This study consisted of a retrospective review and a patient survey. It was approved by the Institutional Review Board of the New York Eye and Ear Infirmary of Mount Sinai. To be included in this study, patients must have received an ATFV by the senior author (M.J.P.), as identified via a CPT code search of a billing database and review of the corresponding operative reports. The surgery was performed as described by Tsunoda et al 7 with the modification that most incisions had fibrin glue applied to the incision in addition to the single suture. 12 The surgery must have occurred at least 1 year prior to the time of the study, and patients had to have at least 1-year follow-up. Patients must have been diagnosed with either sulcus vocalis or vocal fold scar and undergone voice therapy that resulted in unsatisfactory outcomes. Those patients who had moderate to severe dysphonia and failed conservative management, including voice therapy, were offered ATFV. A presumptive diagnosis of sulcus vocalis or vocal fold scar was made using stroboscopy and confirmed during direct laryngoscopy in the operating room. Each patient was scheduled for postoperative follow-up on day 5, 1 month, 3 months, 6 months, and 1 year. They were also prescribed postoperative voice therapy, starting as early as 1 week following their procedure, with the prospect of 4 to 6 voice therapy sessions. Four patients were excluded from the study for not having in-office follow-up for at least 6 months.
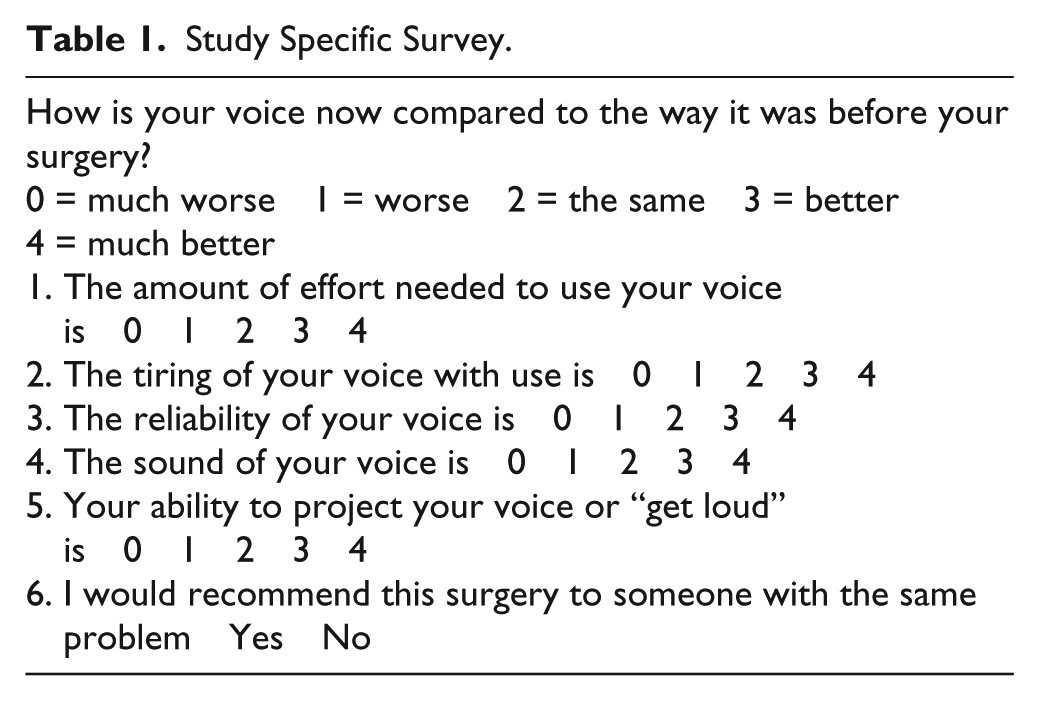
At the preoperative and 6-month postoperative visits, patients underwent acoustic recording and completed a Voice Handicap Index 10 (VHI-10) questionnaire. These voice samples were graded at the time of the patient visit by a speech language pathologist specializing in the care of voice patients on a scale of 0 to 3 using the grade, roughness, breathiness, asthenia, and strain (GRBAS) scale. Paired t tests were performed to compare the individual GRBAS components and totals at the preoperative and 6-month postoperative visits. To perform the questionnaire portion of this study, patients were contacted via phone or email to answer another VHI-10 in addition to a study-specific questionnaire. This questionnaire included 5 Likert scale questions and 1 yes/no question (Table 1). The average amount of time between their surgery and contact with these questionnaires was 44 months (range, 12-78 months).
Study Specific Survey.
A total of 21 patients were enrolled in the study. The 10 patients in our first ATFV study were also included in this cohort. Of these, 16 patients had preoperative and 6-month postoperative VHI-10s, and 17 had preoperative and 6-month postoperative vocal recordings. Paired t tests were performed on the VHI-10 scores, comparing those completed at the preoperative versus 6-month postoperative visits. This was also performed comparing the VHI-10 scores obtained at the preoperative visit versus those obtained at the time of the study completion as well as comparing the VHI-10 scores at 6-month postoperative visits versus those at the time of the study completion. Eighteen of the subjects included in this study were reached to complete these surveys. As the study-specific Likert scale survey was a nonvalidated study, no t test was performed for analysis.
Results
Of the 21 patients included in this study, 62% were female, 67% had bilateral pathology, and 86% had a sulcus vocalis. Of the 35 vocal folds treated in this study, only 5 of them had vocal fold scar. Fourteen patients had bilateral vocal fold surgery, and 7 received unilateral surgery. Patients were contacted at the time of study to answer a VHI-10 and the additional study specific survey. The average amount of time between their surgery and this contact was 44 months (range, 12-78 months). The VHI-10 scores had a mean decrease of 8.75 (P < .001) between the preoperative and 6-month postoperative visits (Table 2). This improvement was even greater when comparing the preoperative visits to those completed at the time of this study (Table 2), with a mean decrease in VHI-10 of 13.53 (P < .001). Comparing the VHI-10 scores of their 6-month postoperatove visit to those completed at the time of the study showed a mean decrease of 4.87, falling short of statistical significance (P = .734).
Statistical Evaluation of VHI-10. a
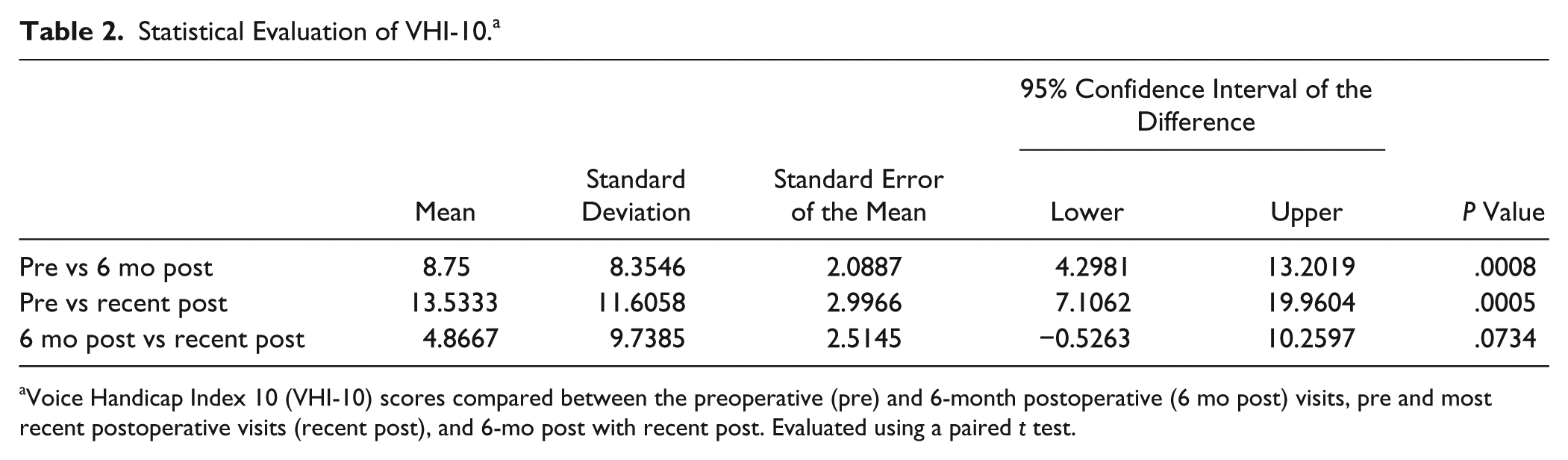
Voice Handicap Index 10 (VHI-10) scores compared between the preoperative (pre) and 6-month postoperative (6 mo post) visits, pre and most recent postoperative visits (recent post), and 6-mo post with recent post. Evaluated using a paired t test.
The VHI-10 scores collected at the preoperative (pre) and 6-month postoperative (6-mo post) visits were evaluated using a paired t test on 16 subjects. The mean postoperative VHI-10 score is significantly decreased compared to the preoperative VHI score (P = .0008). The VHI-10 scores collected at the preoperative and most recent postoperative visits (recent post) were evaluated. This analysis included 15 subjects. Again, the mean postoperative VHI score is significantly decreased compared to the preoperative VHI score (P = .0005). Fourteen subjects were included in the comparison of 6-mo post VHI-10 scores with those collected at their recent post visit. The VHI-10 scores remained stable without a statistically significant change (P = .0734).
The mean decrease in total GRBAS scores between the preoperative and 6-month postoperative visits was 3.31 (P < .001) (Table 3). This statistically significant result was demonstrated in each of the subsets of the GRBAS scale. The mean decreases were: Grade = 0.62 (P = .005), Roughness = 0.59 (P = .017), Breathiness = 0.50 (P = .026), Asthenia = 0.71 (P < .001), and Strain = 0.90 (P < .001). The study-specific survey showed that 50% of patients responded that their voice was currently better or much better to question 1 (vocal effort), 67% to question 2 (tiring of voice), 72% to questions 3 and 4 (vocal sound and reliability), and 61% to question 5 (ability to project). Only 17% of patients stated their voice was worse to question 1; 0% to questions 2, 3, and 4; and 6% to question 5. Out of 108 total questions, only 4 were scored as worse, and zero were scored much worse in response to any of the questions asked. When asked if the patient would recommend this surgery to someone else with a similar problem, 89% said that they would recommend it.
Statistical Evaluation of GRBAS. a
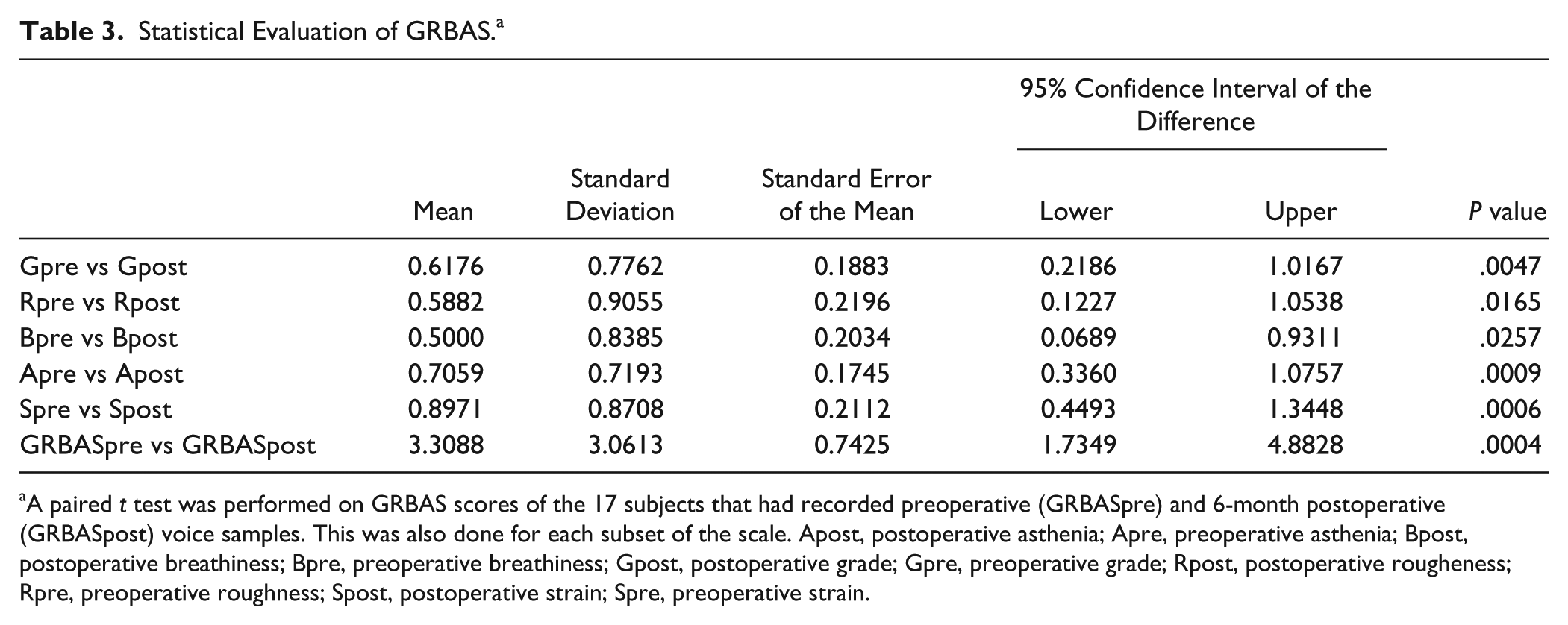
A paired t test was performed on GRBAS scores of the 17 subjects that had recorded preoperative (GRBASpre) and 6-month postoperative (GRBASpost) voice samples. This was also done for each subset of the scale. Apost, postoperative asthenia; Apre, preoperative asthenia; Bpost, postoperative breathiness; Bpre, preoperative breathiness; Gpost, postoperative grade; Gpre, preoperative grade; Rpost, postoperative rougheness; Rpre, preoperative roughness; Spost, postoperative strain; Spre, preoperative strain.
A paired t test was performed on the GRBAS scores of the 17 subjects that had recorded preoperative (GRBASpre) and 6-month postoperative (GRBASpost) voice samples. The mean postoperative GRBAS score is significantly decreased compared to the preoperative GRBAS score (P = .0004). Each subset of this scale was also compared from preoperative to 6-month postoperative visits.
Discussion
Both sulcus vocalis and vocal fold scar have abnormalities of the SLP with similar effect on phonatory vibration. There is currently no gold standard for the treatment of sulcus vocalis or vocal fold scar. Both entities should initially be managed conservatively with voice therapy. Unfortunately, many patients will fail to achieve a satisfactory result from conservative management because it fails to address the underlying structural pathology. If the patient’s dysphonia continues to have a substantial negative effect on their quality of life, surgery must be considered.
The ultimate goal for treatment of these disorders is to restore the natural function of the vocal fold cover and correct glottal insufficiency with improvement in phonation. In practice, however, most surgeries only attempt to fix 1 of these 2 problems. These surgeries include but are not limited to microflap elevation with or without excision, laser treatment, mucosal slicing technique, type-I laryngoplasty, photoangiolytic laser, and injection augmentation.9,10,13-17 Unfortunately, many of these techniques have demonstrated inconsistent or unsatisfactory results. The implantation of autologous fat into Reinke’s space theoretically addresses both problems, but the technique, either transoral or through a gray minithyrotomy, is fraught with handling of the fat and an unpredictable resorption rate of anywhere between 20% and 90%. 18 In the only scientific evaluation of this technique, the outcomes are difficult to assess based on the information provided in the manuscript. In addition, the manuscript does not evaluate voice outcomes and suggests that multiple implantations are necessary. 19 In contrast, ATFV has been shown to improve the voice and correct both glottal insufficiency and the lack of mucosal wave in patients suffering from sulcus vocalis and scar.5,12 The goal of this study was to increase our understanding of the long-term outcomes of ATFV and patient satisfaction.
This investigation found that ATFV results in significant improvement in phonatory function that persists over time. There was statistically significant improvement of all subscales of the GRBAS perceptual analysis between the preoperative and 6-month postoperative visits. There was also a significant decrease in VHI-10 between the preoperative and postoperative visits. This improvement was the most dramatic over the first 6 months and continued for months to years afterward (Figure 2). Only a small percentage of patients reported that certain aspects of their voice were worse at the time of the study. The majority stated they had continued improvement in multiple areas of vocal function. None of the patients stated that their voice was much worse for any question in the survey-specific study. Three patients did feel they were worse relative to “the amount of effort needed to use your voice.” It is unclear why this was the case for these select patients, who had improvements in many of the other areas questioned. Together, these results stress the lower risk of negatively affecting a patient’s voice with this procedure and the high likelihood of vocal improvement in many areas of vocal function about which patients with the disorder complain. Most telling, patients were satisfied with their vocal outcome as evidenced by the fact 89% would recommend the surgery to others with the same problem. When counseling patients, it is important to convey that while the risk of a significant deterioration of the voice may be low, the rate of satisfactory improvement is 80% to 90%, not 100%. Some patients will go through the extended healing time and have vocal function similar to their preoperative status.
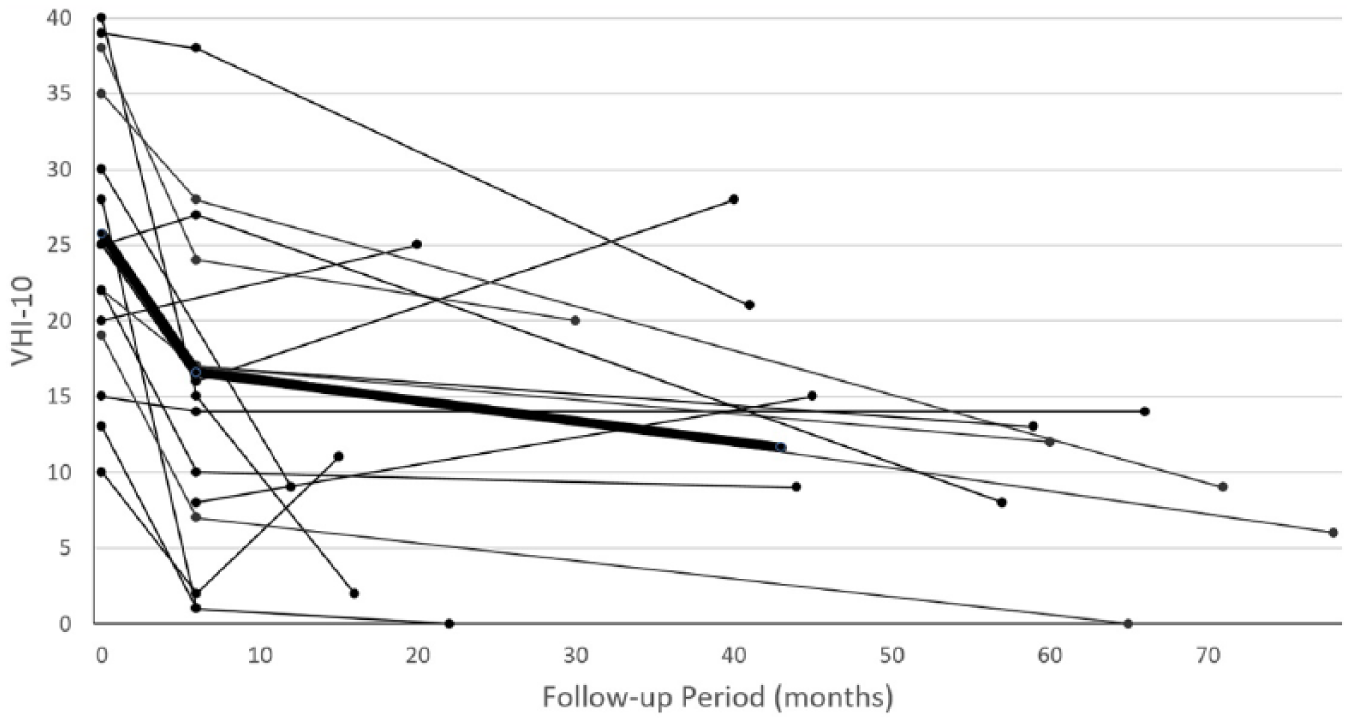
Voice Handicap Index 10 (VHI-10) of each patient represented over time. Included in this graph are all 13 subjects that had preoperative, 6-month postoperative, and at time of study VHI-10 scores. Subjects that did not have all 3 timepoints were excluded from this graph. The mean VHI-10 score for these patients is in bold.
Autologous transplantation of temporalis fascia into the vocal fold appears to address the issues of both glottal closure and vocal fold cover function. 12 Yet the precise mechanism through which the temporalis fascia corrects the underlying dysfunctional SLP has not yet been fully elucidated. We hypothesize that the temporalis fascia acts in part as a scaffold for regeneration while also providing growth factors to spur fibroblast activity. 5 A complementary hypothesis is that the harvested fascia carries with it other supportive cells, such as fibroblasts.18,19 These adherent cells could also be instrumental in local remodeling.
The only complication noted in this series was a partial graft herniation in subject No. 3 that resulted in a self-limited granuloma. The first 3 subjects received single suture closure of their vocal fold incision, but because of this complication, the procedure was modified to include the addition of fibrin glue (Baxter International, Deerfield, Illinois, USA) following suture closure. The procedure was subsequently modified for subject Nos. 20 and 21, with the replacement of fibrin glue with dermabond (Ethicon US LLC, Somerville, New Jersey, USA). This has been found to be a satisfying change and has been used on more recent patients not included in this investigation. It should be noted that the recovery period for ATFV patients is substantial. While some patients have significant improvement in just a few weeks, it is not uncommon for patients to be severely dysphonic for 4 weeks with significant improvement taking 2 to 3 months. This is an important consideration when counseling patients prior to treatment to appropriately manage expectations.
A limitation within this study was the lack of a control group. As a result, it is possible that the self-reported ratings of vocal handicap could have been confounded by a placebo effect and/or the passage of time. The final questionnaire and VHI were performed over the phone instead of in private, which could have been confounding. In addition, this series was from a single surgeon. There have only been 3 other significant published series regarding ATFV, all from single surgeons as well. Further studies including multiple surgeons will be needed to evaluate the generalization of the outcomes reported here.
Conclusion
Sulcus vocalis and vocal fold scar are disorders that are debilitating and extremely difficult to treat. While the results of most treatment options are unsatisfactory, the findings of this study demonstrate that ATFV is a good surgical option. Treatment results in long-term vocal improvement with significant and persistent changes with an average follow-up of over 3.5 years. Patient satisfaction is high, and nearly all patients would recommend the surgery to others with similar pathology. In addition, ATFV is safe, with low risk of associated vocal deterioration. Autologous transplantation of temporalis fascia into the vocal fold should be considered for patients who fail conservative management for sulcus vocalis or vocal fold scar.
Footnotes
Acknowledgements
Special thanks to Dr Codruta Chiuzan for her team’s help with statistical analysis.
Authors’ Note
Presented at Combined Otolaryngology Spring Meetings, American Laryngological Association, April 28, 2017, San Diego, California, USA.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This publication was supported by the National Center for Advancing Translational Sciences, National Institutes of Health, through (Grant No. UL1 TR000040). The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH.