
Abstract
Objectives:
To evaluate long-term hearing changes and surgical outcomes for middle ear cholesteatoma with labyrinthine fistula following complete surgical removal of the cholesteatoma matrix.
Methods:
Consecutive samples of 43 patients who underwent 1-stage complete resection of the cholesteatoma matrix overlying a labyrinthine fistula were obtained. Immediate and long-term hearing changes were analyzed in association with fistula size. Accuracy of various diagnostic examinations was assessed.
Results:
Immediately postsurgery, the average bone conduction threshold (43.34 dB) did not differ significantly from the preoperative value (36.66 dB, P = .083). There were also minimal changes thereafter (45.63 dB) without recurrent case over an average follow-up time of 38.3 months (range, 17-69 months). More than 10 dB hearing loss was found in 7 patients with a case of intraoperative perilymph leakage (2.3%), although 5 of them had had preoperative air conduction threshold above 90 dB. Their fistulas were significantly larger than those of patients without hearing loss (P = .027).
Conclusion:
Although caution is required for total removal of a large fistula, owing to increased risk of postoperative hearing deterioration, 1-stage complete resection of cholesteatoma matrix on labyrinthine fistula could be effective in disease control and long-term hearing preservation.
Introduction
Labyrinthine fistula is a severe complication of middle ear cholesteatoma, with reported prevalence ranging from 4.9% to 12.7% of cholesteatoma cases.1-4 Lateral semicircular canal is involved in about 90% of cases because of its nearby location.5-7 Multiple fistulas are found in about 10% of cases.2,5 Management of a labyrinthine fistula has been an object of debate for a long time. Some surgeons have argued for conservative management, leaving the overlying cholesteatoma matrix undisturbed for cases with large-sized fistulas, while others prefer complete removal of the matrix regardless of size.5,6,8-12 Supporters of conservative management warn against postoperative sensorineural hearing loss caused by potential intraoperative opening of the labyrinth, whereas advocates of complete matrix removal point out that the remaining matrix could predispose to further progression, leading to suppurative labyrinthitis.6,8,13-15
Because these debates have not yet been resolved, the optimal approach to management still needs to be examined.14,16-20 Herein, we present a case series of cholesteatoma-related labyrinthine fistulas for which the matrix was completely removed at the initial surgery. Analyses are focused on immediate and delayed postoperative hearing changes and the clinical outcome, including recurrence. The accuracy of preoperative diagnostic methods and the incidence of postoperative complications are also discussed.
Materials and Methods
Participants and Surgical Procedures
A total of 43 patients were included who underwent surgical treatment for an established diagnosis of labyrinthine fistula caused by middle ear cholesteatoma at Korea University Ansan Hospital between May 2010 and June 2016. All patients underwent complete resection of the cholesteatoma overlying the labyrinthine fistula at the initial surgery. A mastoidectomy was performed as necessary to achieve sufficient exposure of the entire cholesteatoma matrix, including the fistula. The surrounding cholesteatoma matrix as well as any keratinaceous materials that were not connected to the fistula were excised, leaving the matrix in place over the fistula until the end of the surgery. The involved matrix was then gently peeled off using a small cotton ball, under continuous irrigation. The exposed fistula was promptly covered by a piece of prepared fascia, and further closure was carried out using cartilage slices and fibrin glues. Institutional Review Board approval was obtained at Korea University Ansan Hospital (No: AS1715-001).
Data Collection and Analyses
A retrospective chart review was carried out focusing on fistula size, hearing changes, surgical outcome, and recurrence. Diagnostic accuracy and correlations of various laboratory studies and physical findings was evaluated as follows: (1) correlations between the fistula size and the findings on fistula test, spontaneous nystagmus (SN), post–head shaking nystagmus (HSN) or canal paresis (CP) of bithermal caloric irrigation and (2) sensitivity of preoperative temporal bone computed tomography, fistula test. The size of each labyrinthine fistula was measured in the surgical field as its longest diameter (mm). The average threshold for bone conduction and air conduction pure tone audiometry were analyzed based on the AAO-HNS criteria (at 0.5, 1.0, 2.0, and 3.0 kHz) preoperatively, postoperatively (mean 2.4 ± 1.3 months) and at the last visit (mean 38.3 ± 18.7 months) for 38 patients who completed the 3 hearing tests. The speech discrimination score (SDS) of speech audiometry was also analyzed at the same time points. Only patients who completed more than 12 months of follow-up after surgery were included. A change of 10 dB or more in bone conduction threshold was considered clinically significant. Detailed demographic data and subjective symptoms and signs were also analyzed.
Statistical analyses were performed using Student’s t test, the paired t test, Pearson’s correlation test, and the chi-square test (or Fisher’s exact test) using SPSS (Version 18.0; SPSS, Inc, Chicago, Illinois, USA). A P value less than .05 was considered significant.
Results
Patient Characteristics and Basic Diagnostic Examinations
Among the 43 patients, 31 were male, and the mean age was 55.07 ± 19.94 years old (range, 23-79 years). On average, the onset of symptoms occurred 7.22 months (range, 0.2-120 months) prior to visiting the clinic. The fistula involved the right ear in 23 cases and the left ear in 20. The mean follow-up duration was 26.1 months (range, 17-69 months). Otorrhea (74.4%, 32 cases) was the most frequently reported symptom, followed by dizziness (41.9%, 18 cases). Attic destruction (58.1%, 25 cases) was the most frequently observed finding on physical examination, followed by tympanic membrane perforation (30.2%, 13 cases). A few patients exhibited SN (9.3%) without significant relationship with fistula size (P = .329, Student t test, Table 1). The direction of SN was contralateral in 3 cases and ipsilateral in 1 case, which involved a 4 mm fistula and 82% of CP in a bithermal caloric test. In contrary, HSN was observed in most cases (37 cases, 86.0%), including those who had SN with the same direction. There was no significant difference in fistula size between cases with positive (2.43 ± 1.10 mm) and negative (2.40 ± 1.20 mm) HSN (P = .951). The direction of HSN was contralateral in 28 cases (71.8%) and ipsilateral in 9 cases (28.2%). The time from the onset of symptom was longer in cases with contralaterally beating HSN (1.84 ± 3.19 months) than those with ipsilateral HSN (0.99 ± 1.17 months), with borderline statistical significance (P = .071); however, the individual symptom duration was widely varied according to the individual cases, especially for the cases with contralateral nystagmus. The fistula test was positive in only 23.3% of the cases (10/43), indicating relatively low sensitivity, whereas temporal bone computed tomography successfully detected the labyrinthine fistula in 97.7% of the cases (42/43). There were no significant differences in fistula size between the cases with positive and negative results in these examinations (Table 1).
Sensitivity of Various Clinical Findings and Their Relation With Fistula Size. a
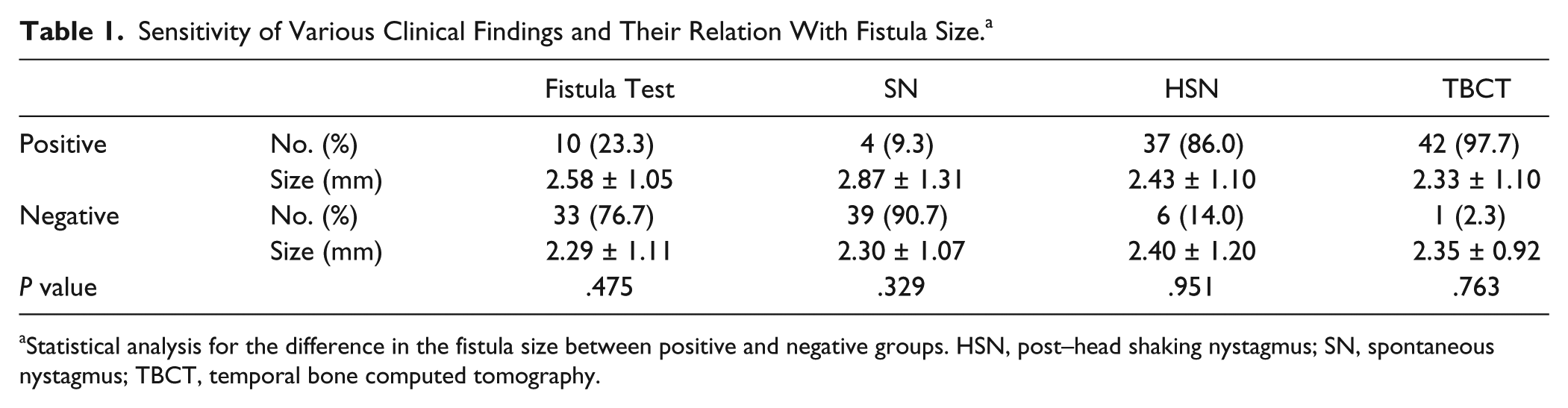
Statistical analysis for the difference in the fistula size between positive and negative groups. HSN, post–head shaking nystagmus; SN, spontaneous nystagmus; TBCT, temporal bone computed tomography.
Surgical Procedures and Management
Appropriate antibiotics were used to control infections prior to the surgery. A canal wall down mastoidectomy was carried out for most cases (35 cases, 81.4%). For some cases with profound air conduction hearing loss, a radical mastoidectomy was carried out (7 cases, 16.3%). In 1 case with a small (1.4 mm) lateral canal fistula with minimal hearing loss (22.4 dB of air conduction threshold), a canal wall up mastoidectomy was carried out, which maintained the ossicular chain intact without recurrence for 38 months. Perilymph leakage was found in 1 patient with a 3 mm cochlear fistula, resulting in complete loss of hearing postoperatively. All other cases achieved complete cholesteatoma matrix removal with preservation of the endosteum. Fallopian canal exposure was observed in 33 cases (76.7%) and dura exposure in 12 cases (27.9%). Among these cases, 1 patient with extensive fallopian canal erosion involving the tympanic and mastoid segments experienced delayed facial palsy at 1.5 weeks after surgery but later showed complete recovery. Ossiculoplasty was carried out simultaneously at the initial surgery in 6 cases (1 total ossicular replacement and 5 partial ossicular replacements). Postoperatively, the tympanic and mastoid cavities were regularly examined to detect the recurrence of cholesteatoma easily with a widely opened cavity. No recurrent case has been found during an average follow-up time of 38.3 months after surgery.
Hearing Changes
Preoperatively, the patients had an average bone conduction threshold of 36.6 ± 21.7 dB and an average air conduction threshold of 69.5 ± 25.7 dB, resulting in a 32.9 dB air-bone gap. Twenty-nine cases (70.7%) had air conduction thresholds above 55 dB prior to surgery, including 15 cases with profound hearing loss (air conduction threshold greater than 90 dB). In terms of bone conduction threshold, 15 cases (39.5%) showed a hearing loss of more than 55 dB. The contralateral side showed an average bone conduction threshold of 20.2 ± 10.4 dB and an average air conduction threshold of 30.6 ± 17.7 dB. Cases with multiple fistulas had worse hearing thresholds (P = .038, Student’s t test, Table 2).
Preoperative Hearing Threshold.
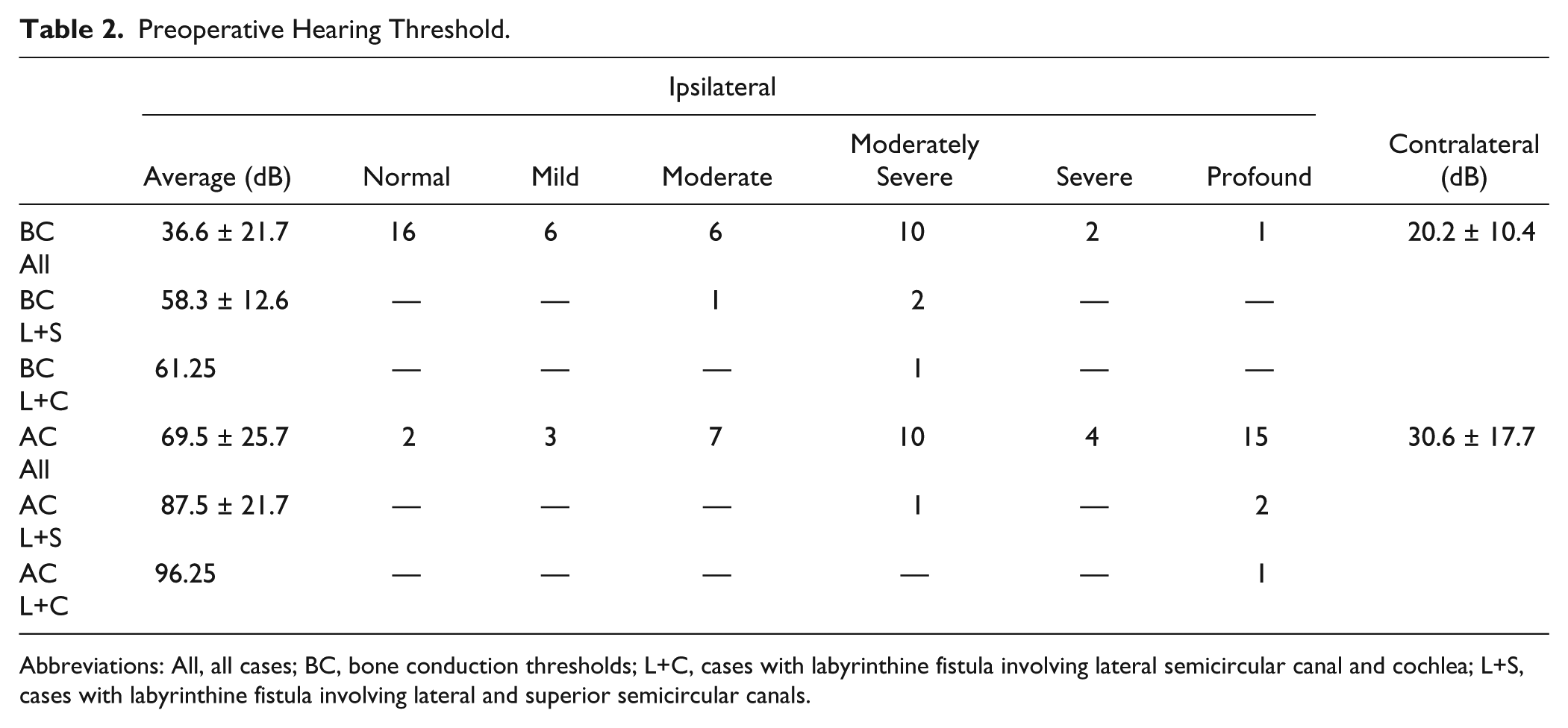
Abbreviations: All, all cases; BC, bone conduction thresholds; L+C, cases with labyrinthine fistula involving lateral semicircular canal and cochlea; L+S, cases with labyrinthine fistula involving lateral and superior semicircular canals.
Postoperatively, 25 out of the 38 patients who received complete hearing tests (65.8%) showed changes of less than 10 dB in bone conduction threshold. Deterioration in the bone conduction threshold of more than 10 dB was observed in 7 patients (18.4%), whereas 6 patients (15.8%) experienced more than 10 dB improvement in bone conduction threshold. Most hearing changes were apparent by the first postoperative audiometry tested at 3 months after surgery, and additional hearing loss was minimal thereafter (Figure 1). The average bone conduction hearing threshold changed from 36.55 dB preoperatively to 43.34 dB on the first postoperative test (P = .083) and to 45.63 dB on the final hearing test (P = .023). However, the air conduction threshold showed relatively minimal changes, from 69.53 dB (preoperative) to 70.82 dB (last hearing test).
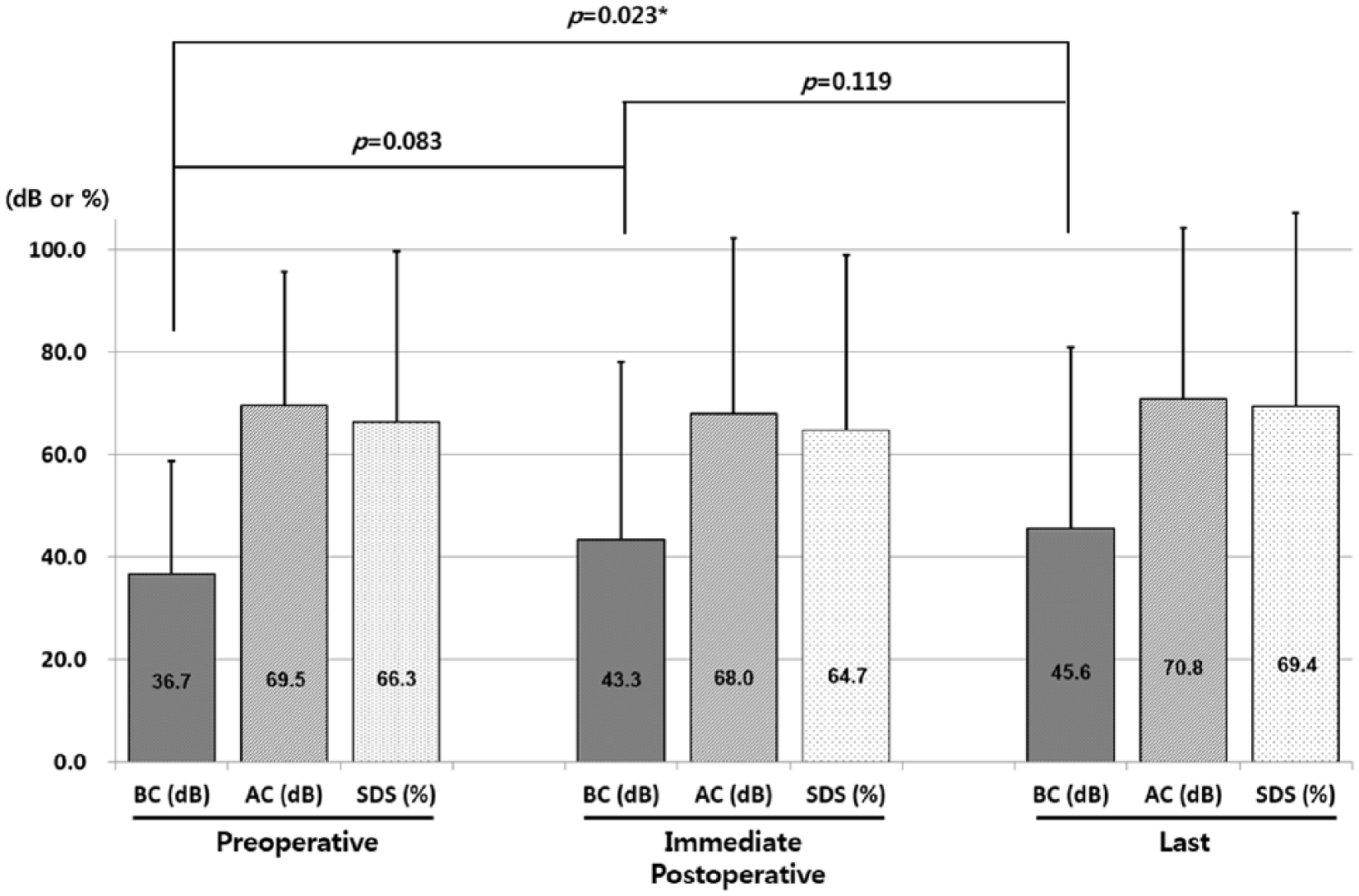
Changes in average hearing thresholds, in decibels. Major changes in bone conduction threshold occurred immediately after the surgeries, and further hearing deterioration was minimal thereafter. Significant differences in bone conduction threshold were confirmed between the preoperative and final examinations (P = .023, Student’s t test). Changes in air conduction thresholds were minimal throughout the series of measurements. The speech discrimination score showed minimal changes over time.
To investigate the factors affecting these postoperative hearing changes, we compared preoperative bone conduction threshold, the size of the fistula and canal paresis as measured using the bithermal caloric test among groups classified as >10 dB worsening, >10 dB improvement, or <10 dB change. A significant difference was found for fistula size (P = .027, Kruskal Wallis test), with an average of 3.07 ± 1.13 mm in the >10 dB worsening group, in contrast to 1.37 ± 0.75 mm in the >10 dB improvement group. The <10 dB change group showed an intermediate size, 2.05 ± 1.03 mm (Table 3A). In a reverse analysis, giving the number in each hearing-change group as a function of fistula size, there was a similar relationship with a significantly more cases with >10 dB postoperative hearing loss in cases with > 4 mm sized fistula (p=0.006, Fisher’s exact test) (Table 3B). However, if the fistulas are divided at 2 mm (P = .385) or 3 mm (P = .197), no significant difference in the number of cases with >10 dB postoperative hearing loss was found. There was also a significant correlation between postoperative bone conduction threshold changes and fistula size (P = .007, Pearson’s correlation test, R2 = 0.1896, Figure 2). No postoperative hearing change was noted for any of the cases with multiple fistulas (<10 dB change). Among 7 patients who experienced >10 dB postoperative hearing loss, 5 had no detectable bone conduction postoperatively. However, 4 out of these 5 patients already had bone conduction thresholds above 55 dB preoperatively, and all 5 had air conduction thresholds above 90 dB, which means the patients hardly experienced perceptible changes (Table 4).
(A) Variables Associated With Hearing Aggravation and (B) Changes in the Bone Conduction Threshold According to the Fistula Size (B).
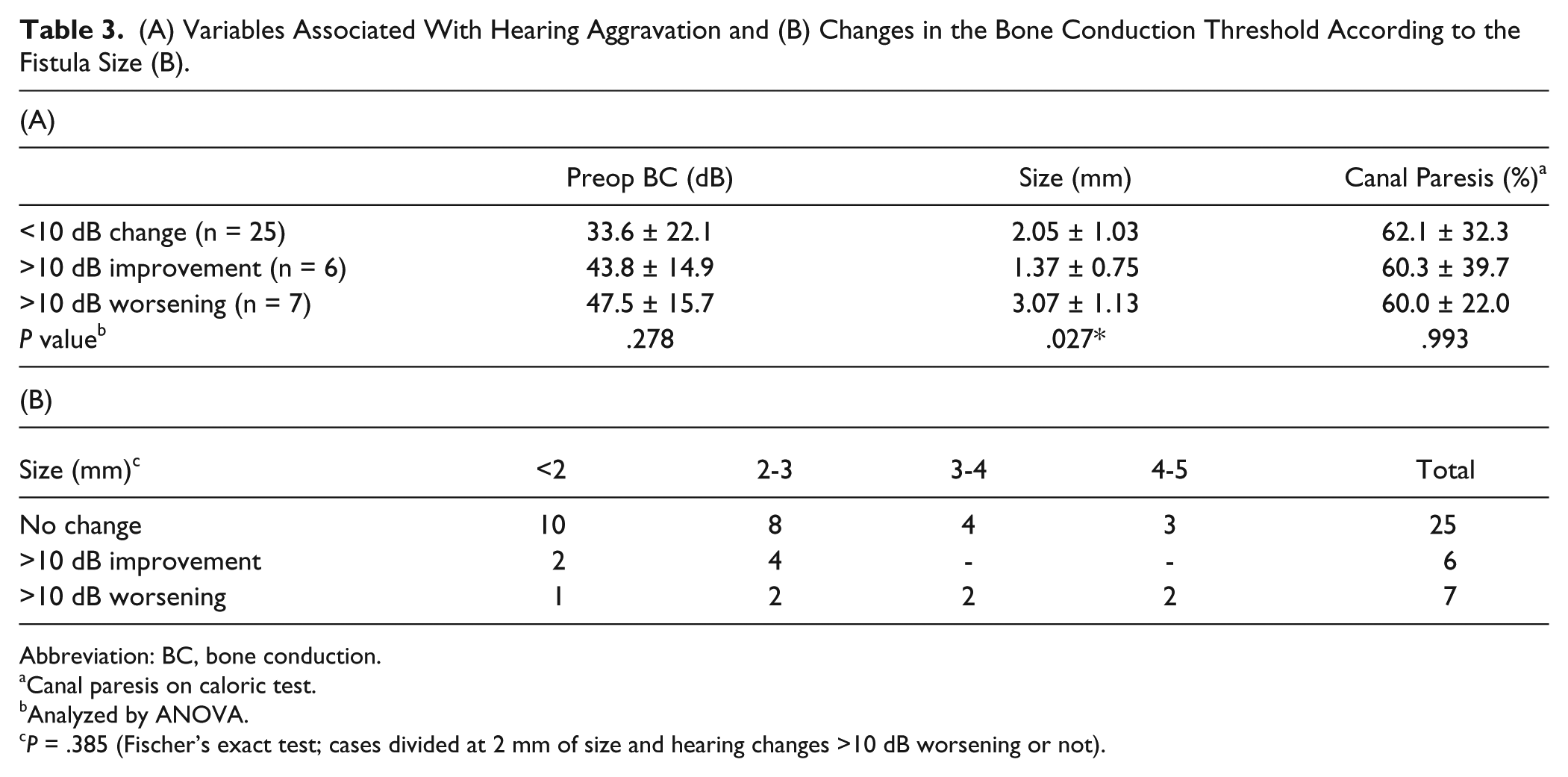
Abbreviation: BC, bone conduction.
Canal paresis on caloric test.
Analyzed by ANOVA.
P = .385 (Fischer’s exact test; cases divided at 2 mm of size and hearing changes >10 dB worsening or not).
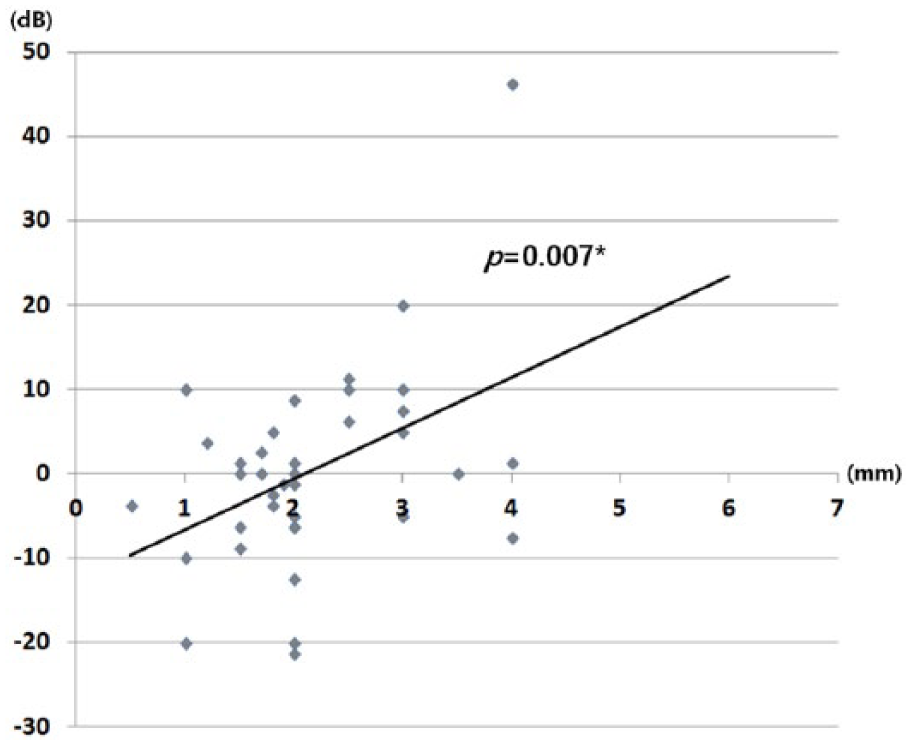
A significant correlation was confirmed between postoperative bone conduction threshold changes and labyrinthine fistula size (P = .007, Pearson’s correlation test, R2 = 0.1896).
Various Clinical Characteristics of Patients With More Than 10 dB Hearing Aggravation.
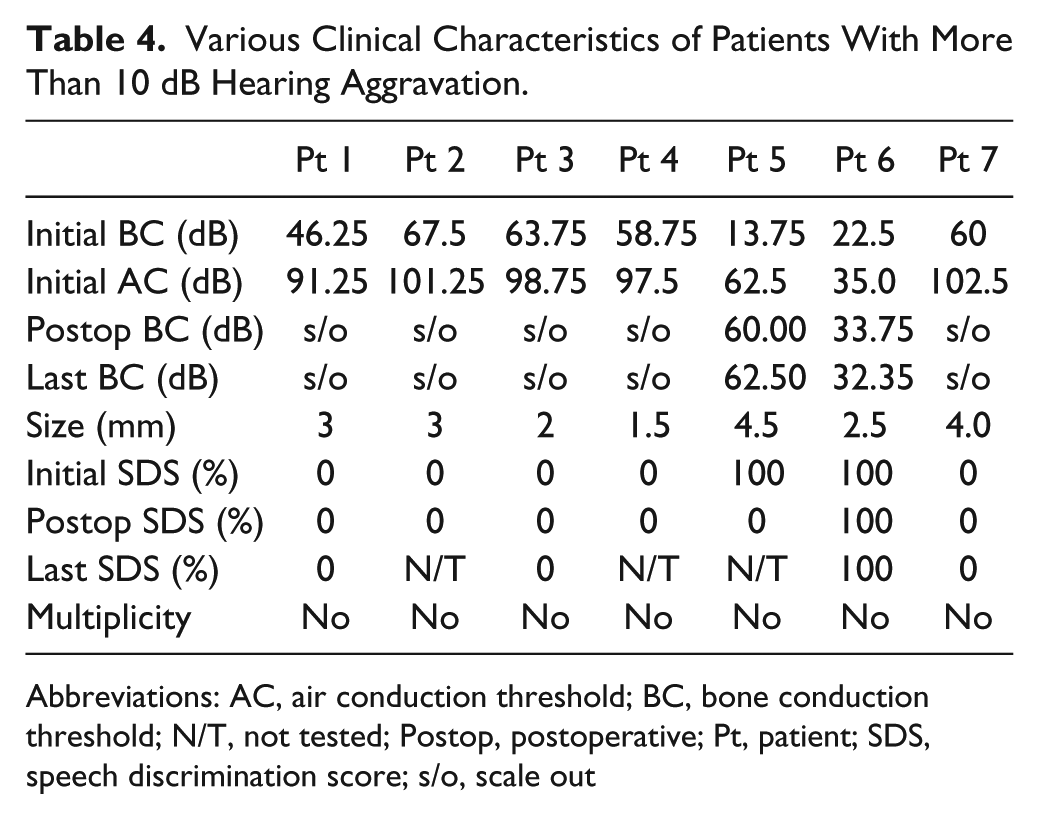
Abbreviations: AC, air conduction threshold; BC, bone conduction threshold; N/T, not tested; Postop, postoperative; Pt, patient; SDS, speech discrimination score; s/o, scale out
The SDS was 66.3% preoperatively, becoming 64.7% immediate postoperatively and 69.4% in last speech audiometry without statistical significance (P = .483, ANOVA). Among 7 cases who experienced >10 dB hearing deterioration in pure tone audiometry and 5 cases who experienced complete hearing loss postoperatively, the SDS was already 0% preoperatively with >90 dB preoperative air conduction threshold. Among another 2 cases, the SDS of a case who experienced a considerable hearing loss from 13.75 dB to 60.0 dB of bone conduction threshold became 0% from 100% in preoperative speech test with undetectable air conduction threshold. The other case maintained 100% of SDS postoperatively because the patients experienced a relatively small bone conduction changes from 22.5 dB to 32.35 dB with 41.5 dB of postoperative air conduction threshold.
Discussion
Currently, the choice of surgical intervention for labyrinthine fistula is mainly based on the size of the fistula. The length of the bony crater created by the fistula seems to be the most widely accepted criterion, owing to its ease of use.5,21,22 Despite continuing controversy regarding the size that justifies initial complete resection, it seems to be most widely accepted that a diameter less than 2 mm is less likely to involve the endosteum because the cholesteatoma matrix can be supported mainly by the bone. 22 Based on those conclusions, some researchers suggested that the cholesteatoma matrix should be removed only in cases with a fistula diameter less than 2 mm.5,21,22 As per our data, postoperative hearing deterioration was also minimal in such cases. For those with fistulas larger than 2 mm, matrix preservation rather than complete removal was favored by some researchers,5,21,22 while others have reported safe removal of the overlying matrix.6,8,13,14 These suggestions were based on findings that the differences in postoperative hearing between cases of complete and partial removal were minimal.23,24 In the current study, the fistula size was significantly larger in patients who experienced more than 10 dB postoperative bone conduction deterioration (P = .027, Student t test), and the fistula size had a significant correlation with postoperative hearing changes (P = .007, Pearson’s correlation test). However, in most cases, patients might have little opportunity to experience perceptible hearing deterioration postoperatively. Among 15 cases with fistulas larger than 2 mm, 6 experienced more than 10 dB hearing deterioration after surgery, but 5 of them already had air conduction thresholds above 60 dB; indeed, 4 showed a hearing loss of more than 90 dB. We were unable to determine any threshold for fistula size that allows complete resection with complete safety. The postoperative hearing changes were not significantly different when fistula sizes were divided at 2, 3, or 4 mm diameter.
Among 43 cases of 1-stage complete resection, intraoperative perilymph leakage was observed in only 1 patient, who had a 3 mm cochlear fistula located adjacent to the oval window and experienced complete hearing loss postoperatively. Despite this case, iatrogenic intraoperative perilymph leakage seems to be a rare problem overall, occurring only in 2.3% of cases. Previous studies also reported relatively infrequent occurrence of perilymph leakage (2/38 cases, 5.3%), even when initial complete resection was performed. 1 Fistulas located over the oval window and adjacent cochlea promontory were common in both case series. Fistulas that invade the vestibule, cochlea, or promontory were classified as high stages (stage V, VI) in a fistula staging system previously suggested by Quaranta et al, 3 with very high risk of sensorineural deafness after matrix removal. Thus, caution needs to be exercised in choosing complete resection for such cases. Nevertheless, although immediate hearing loss caused by intraoperative rupture of the labyrinth is a major concern in choosing initial complete resection of the overlying matrix for relatively large-sized fistulas, it seems to occur rarely in practice. One-stage complete matrix removal has the advantage of allowing more effective control of the ensuing complications. Any remaining overlying cholesteatoma matrix could cause continuous bony erosion and finally result in complete hearing loss due to the occurrence of suppurative labyrinthitis.3,25 In the present study, additional hearing changes after the immediate postoperative loss were minimal. Previously, it was reported that the rate of long-term postoperative total deafness was lower in a complete removal group (12%) than in a partial removal group (26%). 6 Based on these findings, even if there might be a greater potential for immediate postoperative hearing loss in cases with larger fistulas, this could work as a kind of “trade-off” with decreased chances of additional delayed hearing loss or complications. In some cases, the bone conduction threshold improved after surgical resection. Possible mechanisms include elimination of the toxic influence of inflammatory mediators from middle ear inflammation or serous labyrinthitis or restoration of the middle ear cavity and auditory ossicular chain.26,27
Overall SDS was minimally changed without statistical significance over time with a slight improvement immediate postoperatively, as was in accordance with previous reports. 6 A total of 4 cases had >15% improvement of SDS postoperatively, whereas only 2 cases experienced >15% decrease. That might be explained by the fact that most cases (28 cases, 73.7%) received some kind of ossicular restoration simultaneously (6 cases of artificial ossicular prosthesis, 20 cases with T1, T3, or T4 type of Wullstein tympanoplasty classification) with eradication of middle ear pathology. 28 The cases with ossicle reconstruction had an average of 51.0 dB of postoperative air conduction threshold from 58.7 dB of preoperative value with 89.4% of postoperative SDS from 91.1% preoperatively. In contrast, the remaining cases without ossicle reconstruction had 92.5 dB of preoperative average air conduction threshold with 12.6% of preoperative average SDS, which were changed to 104.8 dB and 11.2%, respectively, at postoperative hearing tests. The change of SDS for patients with hearing deterioration was rather simple because most of them (5/7 cases) already had >90 dB of air conduction threshold preoperatively. They also had 0% of SDS preoperatively with around 60 dB of bone conduction threshold (Table 4). Only a case who experienced a significant hearing loss down to nonresponsive air conduction threshold with 60.0 dB of bone conduction threshold became 0% of SDS from 100% preoperatively.
With regard to the type of mastoidectomy chosen, sufficient exposure was preferred for safe and complete removal of all middle ear pathologies. There were also needs for an enhanced detection of postoperative recurrence with simple examination of the cavity anywhere other than our clinic because most of the patients had various reasons that limited frequent postoperative visits to our clinic. As a result, canal wall down mastoidectomy was preferentially performed (42/43 cases). Fallopian canal dehiscence is a problem frequently associated with labyrinthine fistulas. The correlation between lateral semicircular canal (LSCC) fistula and fallopian canal dehiscence caused by cholesteatoma has been widely accepted.18,29 Recently, it was reported that the incidence of fallopian canal dehiscence in subjects with LSCC fistula was 83.3% to 84.6%.18,29 In the current study, the incidence of facial nerve canal dehiscence was 76.7%, slightly lower than that observed in previous studies.
High-resolution temporal bone computed tomography was found to be very sensitive in detecting labyrinthine fistulas, as might be expected given its excellent resolution for bony structural changes. Similar findings have been reported in previous studies, with sensitivity and specificity up to 100%.6,30 In contrast, physical examinations, such as the fistula test or observation of the nystagmus, showed low sensitivity. In our data, SN was observed only in 4 cases, contralaterally beating in 3, ipsilaterally beating in 1. However, if HSN is added, the detection of nystagmus could be enhanced. The patients with ipsilaterally beating HSN included more cases with normal function on bithermal caloric test without notable vestibular abnormality on the other side; however, still the direction of the nystagmus hardly carries any conclusive information for the underlying vestibular function. The predictive value of the direction of nystagmus has been controversial.4,31 It could be related to multiple factors, such as the severity of the primary insult (determined by the fistula location and size) and the time course and degree of contralateral compensation. 6
Conclusions
Our data indicate that 1-stage complete resection of cholesteatoma could be a reasonable option even for large fistulas, especially in preventing long-term hearing loss and disease recurrence. However, careful case selection is still important, especially for large or cochlea-involved fistulas.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by Basic Science Research Program through the National Research Foundation of Korea (NRF) funded by the Ministry of Education (Grant No. 2017R1D1A1B03036131).