
Abstract
Objectives:
In Ethiopia, 2-stage operations with middle ear prostheses are economically unfavorable. We hypothesized that single-stage autologous ossiculoplasty results in acceptable tympanic membrane (TM) and hearing improvements in a setting of limited resources.
Methods:
One hundred eighty-eight patients (197 ears) who underwent 1-stage autologous ossiculoplasty for ossicular dysfunction are presented. All but 14 of these ears also had perforations of the TM. Conditions of the middle ear were granulation tissue, ossicular disruption only, tympanosclerosis, and cholesteatoma. Reconstructions of the ossicular chain were performed with autologous ossicles only.
Results:
The closure rate of TM perforations was 95%. Preoperative air bone gaps were 27 to 60 dB (mean [SD] = 44 [7] dB); postoperative air bone gaps were 0 to 50 dB (average [SD] = 23 [10] dB), for an average improvement of 21 dB across all reconstruction types (P < .001). The largest favorable changes in air bone gaps were with incus and malleus columellas from the footplate to the TM (33 and 23 dB, respectively) (P < .001). No patient had worsening of sensorineural hearing levels or extrusion of the reconstructed ossicles.
Conclusion:
Autologous ossiculoplasty performed well in this setting. Acceptable TM closure rates and improvement of air bone gaps were seen in 1-stage operations without the use of prostheses.
Introduction
Ethiopia is among the poorest nations in the world with limited resources for medical care. Otolaryngologists number just 28 people in a country of more than 100 million. 1 Otolaryngology is a young specialty there, with the oldest residency program established in 2009. In addition, medical disposables and ossicular prostheses must be imported from overseas, are subject to customs and importation restrictions, and are prohibitively expensive. Access to otologic surgery, particularly ossiculoplasty, is therefore restricted by these limitations.
It is clear that there are challenges in Ethiopia associated with otologic training opportunities, trained otolaryngologists, supplies, and implants. However, these obstacles can be addressed and overcome in a systematic fashion. One previous report presented a novel approach to tympanosclerosis surgery in Ethiopia that reduces the cost of care, without compromising patient safety or outcomes. 2 In this context, identifying safe and effective strategies for ossicular reconstruction when there is no access to prostheses would be valuable, also.
We suspected, based on the experience of the senior author of this report, that acceptable outcomes for reductions in air bone gaps in ossiculoplasty were being obtained in Ethiopia, using only 1-stage operations without a prosthesis. This brief original research will outline the reconstructive strategies and operative results that support this hypothesis.
Materials and Methods
Institutional Review Board
This study was performed consistent with the standards of the Declaration of Helsinki and involved minimal risk to the participants. However, it was nonetheless also reviewed and approved by the OtoRino-ENT Specialty Clinic’s own Ethics and Patient Protection Committee, of which neither author was a member.
Study Design
This is a retrospective review of the medical records of a single otologist.
Setting Description
The surgeon was an Ethiopian national who obtained his medical and otology training at the University of Leipzig in Leipzig, Germany, from 1982 to 1988 and practiced there after graduation from 1990 to 1997. From 1999 to 2017, he has equipped and worked in an ear, nose, and throat clinic in Addis Ababa, Ethiopia, using the YZ2OP5 operating microscope from China and Zeiss OPMI® pico clinic microscopes from Germany. Otology drills used were the Karl Storz Unidrive® ENT drill from Germany and the NSK Surgic Pro® drill from Japan. Electrocautery devices were used intraoperatively, but facial nerve monitoring was not available. Audiometry was performed by audiometry technicians without formal training—there are no audiometry or audiology programs in Ethiopia. Testing was conducted in a dedicated room with padding on the walls, using Maico® and Amplivox® audiometers and Otowave® tympanometers. Pure tone thresholds for air and bone (masked) were obtained. Word recognition testing materials were not available in Ethiopia until late 2017, 3 and therefore, no word recognition scores were obtained.
Operations—Equipment and Materials
All operations were performed by the same senior surgeon under local anesthesia with sedation, without a facial nerve monitor. All drumhead defects were grafted in an underlay fashion, with tragal perichondrium, or tragal perichondrium with free tragal cartilage island in 2 layers. The perichondrial grafts were sized to extend to the bony annulus for support against medialization and displacement, and the external canal skin and tympanic membrane (TM) remnants were replaced laterally. No prosthetic materials were used in these operations. Ossicular reconstructions were as follows:
Capitulum-incus-manubrium. The incus was removed, reshaped, and repositioned between the capitulum and the manubrium (Figure 1). The drumhead was either intact or grafted.
Capitulum-incus-TM. The incus body was reshaped and positioned atop the capitulum to reach the TM beneath a layer of tragal perichondrium and a layer of free tragal cartilage island (Figure 2).
Capitulum-malleus head-TM. The malleus head was repositioned atop the capitulum to reach the TM beneath a layer of tragal perichondrium and a layer of free tragal cartilage island (Figure 2).
Incus from footplate to TM. The incus was refashioned to a 4.5-mm length and repositioned from the mobile oval window footplate to reach the TM beneath a layer of tragal perichondrium and a layer of free tragal cartilage island (Figure 3).
Malleus from footplate to TM. The malleus was refashioned to a 4.5-mm length and repositioned from the mobile oval window footplate to reach the TM beneath a layer of tragal perichondrium and a layer of free tragal cartilage island (Figure 3).
Type III reconstruction with the TM repositioned directly on the stapes capitulum without any strut or graft.
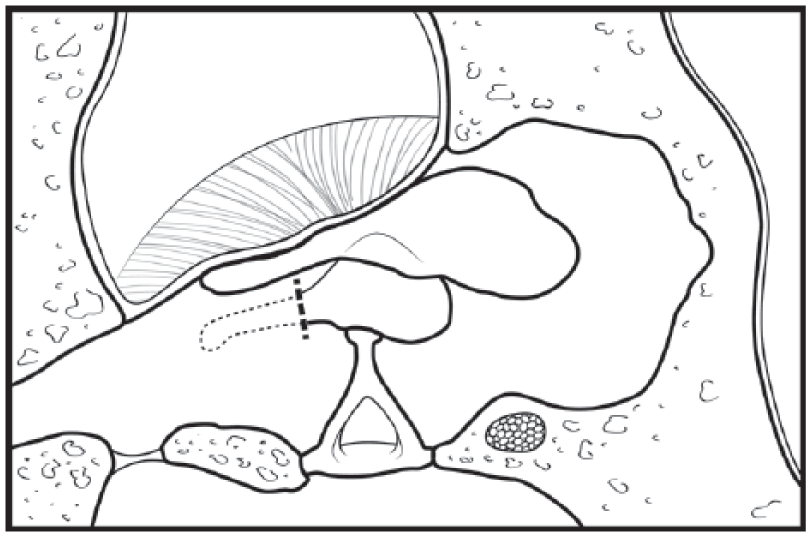
Capitulum-incus-manubrium reconstruction. The incus is pictured, having been removed, reshaped, and repositioned between the capitulum and the manubrium. Tympanic membranes in these cases were intact, or perforated and grafted in 2 layers.
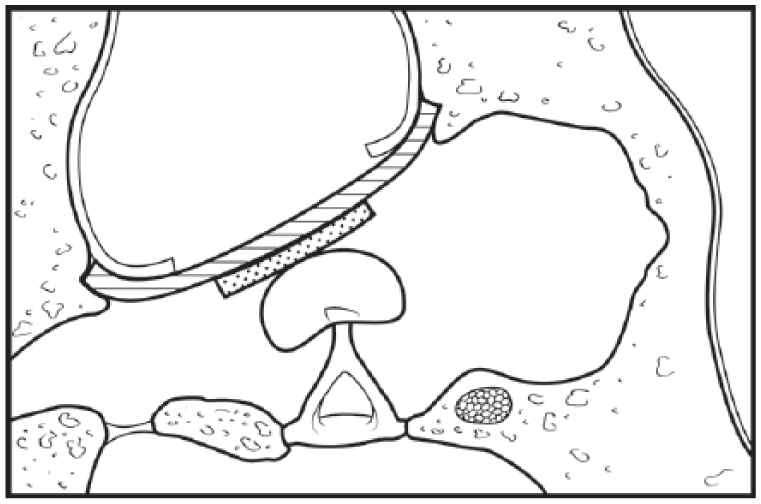
Capitulum-malleus head-tympanic membrane (TM) reconstruction. The malleus head is pictured, having been repositioned atop the capitulum to reach an intact TM, or beneath a layer of tragal perichondrium and a layer of free tragal cartilage island. In a similar way, the capitulum-incus-TM reconstruction (not pictured) reshaped the incus and positioned it atop the capitulum.
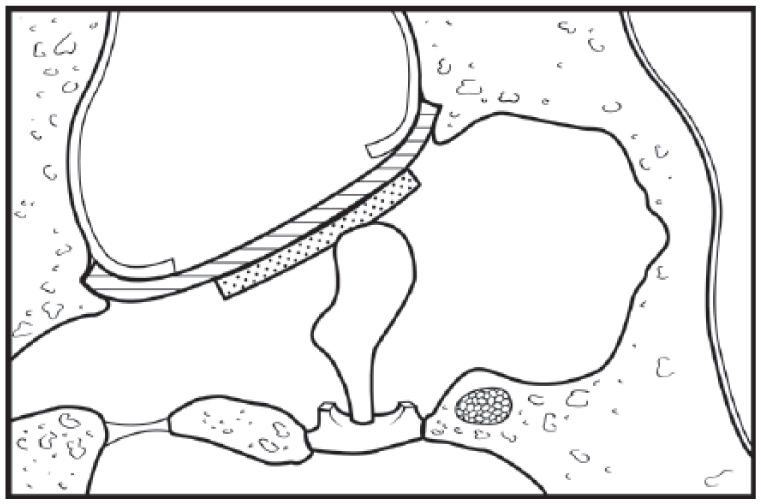
Malleus from footplate to tympanic membrane (TM). The malleus is pictured, having been refashioned to a 4.5-mm length and repositioned from the mobile stapes footplate to reach the TM beneath a layer of tragal perichondrium and a layer of free tragal cartilage island. A similar construction of the incus from the mobile stapes footplate to the TM is not pictured. (The incus was similarly refashioned to a 4.5-mm length and repositioned from the mobile footplate to the TM grafts.)
Participant Selection and Preparation
This is a retrospective study. Participants were patients who presented from 2011 to 2017 with TM perforations or conductive hearing loss with an intact TM and who were later found at operation to have ossicular discontinuity. Patients with infected or draining ears or evidence of otomycosis were treated first and reassessed for operation only after their ears were dry. All participants who agreed to an operation were included in this study, except those who lived in remote areas of the country and who did not return for follow-up examination. (This is routine behavior in Ethiopia, where medical practitioners can be very far removed, and these patients who did not return for follow-up were excluded from this retrospective series.) There was no age restriction on patient selection. Patients with cholesteatoma, tympanosclerosis, or granulation tissue were included for analysis if they had shown ossicular discontinuity on middle ear exploration. Patients with glomus tumors were excluded from even middle ear exploration because of the lack of embolization technology.
Outcome Measures
Outcomes of interest were closure of the original TM perforation and the change (improvement) in the air bone gap in dB averaged over 500 Hz, 1 kHz, 2 kHz, and 4 kHz (extended pure tone average [PTA]). To determine closure of the TM perforation, tympanometry was not used as per the senior author’s preferences. Instead, graft integrity was determined with clinic microscope evaluation with the Zeiss OPMI pico. Postoperative microscope and audiometric evaluations were attempted at 6 months; however, some patients had to be contacted and encouraged to come for follow-up because they were asymptomatic and had failed to return. This extended the variation of follow-up times. In cases of several postoperative audiograms, the latest one (furthest postoperation) was selected for analysis.
Descriptive statistics were used where appropriate, performed using the SPSS 20 statistical analysis package. 4
Results
Preoperative Conditions
Participants were 188 patients (197 ears), ages 12 to 56 (average = 26) years. One hundred twenty-six participants were female (64%) and 71 male (36%). All ears were dry and uninfected on the day of surgery. Follow-up examinations occurred from 3–33 (average = 7) months postoperation. Preoperative TM perforation sizes were > 60% in 93 ears (47%), 31% to 59% in 65 ears (16%), and < 30% in 21 ears (11%), and TM was intact in 14 ears (7%). Conditions of the middle ears were as follows: 52 with granulation tissue (26%), 29 with cholesteatoma (13%), 71 with tympanosclerosis (36%), and 45 with ossicular chain disruption only (23%). The stapes suprastructure was absent in 11 patients (6%). It should be clarified that the cases of cholesteatoma involved matrix on the ossicles only, not extending into the epitympanum or additus ad antrum, and not requiring mastoidectomy.
Ossicular Pathology on Middle Ear Exploration/Reconstruction
Incus long process erosion with malleus and stapes, normal middle ear height, and TM intact or perforated: reconstructed with capitulum-incus-manubrium ossiculoplasty (Figure 1): 61 ears (31%);
Incus long process erosion with TM intact or perforated, medialized malleus, and reduced middle ear height: reconstructed with capitulum-incus-TM chain (Figure 2): 34 ears (17%);
Extensive incus erosion with TM intact or perforated, medialized malleus, and reduced middle ear height: reconstructed with capitulum-malleus head-TM chain (Figure 2): 83 ears (42%);
Large TM perforation without stapes suprastructure, with a mobile footplate and residual incus of at least 4.5 mm in length: reconstructed with incus from footplate to TM graft (Figure 3): 2 ears (1%);
Large TM perforation without stapes suprastructure, with a mobile footplate and residual malleus of at least 4.5 mm in length: reconstructed with malleus from footplate to TM graft (Figure 3): 9 ears (5%); and
Large TM perforation, with extensive erosion of the malleus and incus but intact stapes: reconstructed with classic type III tympanoplasty-TM grafts directly onto stapes capitulum: 8 ears (4%).
Preoperative Hearing Loss
Table 1 depicts the distribution of hearing loss (extended PTA air bone gap) corresponding to the intraoperative ossicular findings. Pathologies were as follows:
Incus long process erosion with normal middle ear height,
Incus long process erosion with a medialized manubrium/reduced middle ear height,
Extensive incus erosion with medialized manubrium/reduced middle ear height, and
Two groups combined for analysis—erosion of the stapes suprastructure and extensive incus and malleus erosion.
Hearing Levels in Preoperative Ears: Distribution of Extended PTA Air Bone Gaps Preoperatively, Parsed by Ossicular Pathology. a
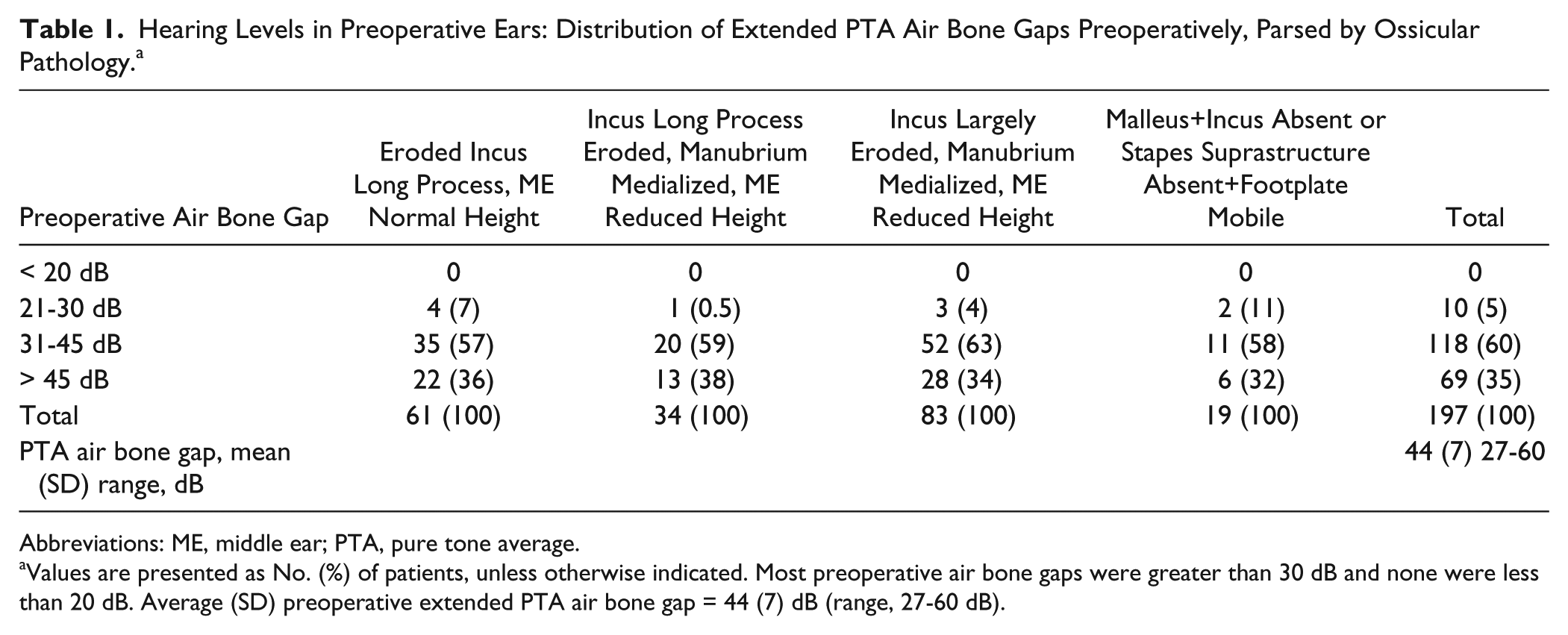
Abbreviations: ME, middle ear; PTA, pure tone average.
Values are presented as No. (%) of patients, unless otherwise indicated. Most preoperative air bone gaps were greater than 30 dB and none were less than 20 dB. Average (SD) preoperative extended PTA air bone gap = 44 (7) dB (range, 27-60 dB).
The distribution of hearing is depicted in Table 1 according to the Committee on Hearing and Equilibrium of the American Academy of Otolaryngology–Head and Neck Surgery recommendations for reporting changes in conductive hearing loss. 5 Specifically, as recommended, these are organized into decibel-interval bins. The preoperative extended PTA air bone gap range was 27 to 60 (average [SD] = 44 [7]) dB, with 187 of 197 ears showing preoperative air bone gaps greater than 30 dB (95%), and no ear showing a preoperative air bone gap better than 20 dB.
Postoperative Hearing Loss
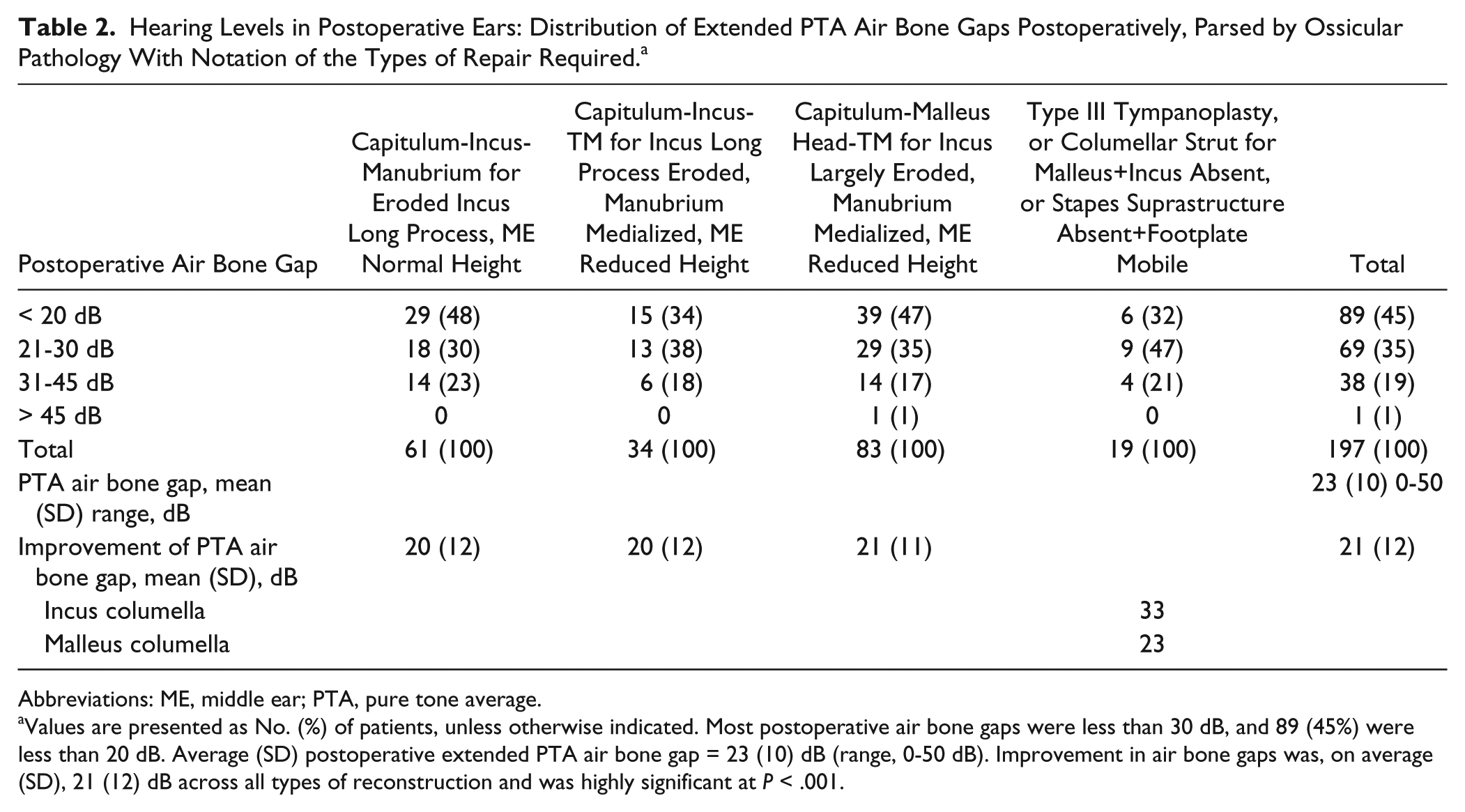
Table 2 shows the distribution of postoperative extended PTA air bone gaps: The range of air bone gaps was 0 to 50 (average [SD] = 23 [10]) dB, with 158 of 197 ears showing postoperative air bone gaps better than 30 dB (80%), and 89 of 197 showing postoperative air bone gaps better than 20 dB (45%). The best hearing improvements were in the context of a missing stapes suprastructure, a mobile footplate, and a 4.5-mm columellar strut from footplate to TM (Figure 3). The incus struts showed 33 dB improvement, on average, and the malleus struts 23 dB. The hearing improvements for the columellar strut reconstruction were the largest of all the reconstructions. Paired 2-tailed t tests found the differences in reconstruction to be at the 99% confidence level (P < .001), but there were only 2 and 9 patients in these 2 reconstruction groups, respectively. On average, all reconstructions showed 21 dB air bone gap improvement. Paired 2-tailed t tests found significant differences between the pre- and postoperative air bone gaps at the 99% confidence level (P < .001) for all reconstructive types (Figure 4).
Hearing Levels in Postoperative Ears: Distribution of Extended PTA Air Bone Gaps Postoperatively, Parsed by Ossicular Pathology With Notation of the Types of Repair Required. a
Abbreviations: ME, middle ear; PTA, pure tone average.
Values are presented as No. (%) of patients, unless otherwise indicated. Most postoperative air bone gaps were less than 30 dB, and 89 (45%) were less than 20 dB. Average (SD) postoperative extended PTA air bone gap = 23 (10) dB (range, 0-50 dB). Improvement in air bone gaps was, on average (SD), 21 (12) dB across all types of reconstruction and was highly significant at P < .001.
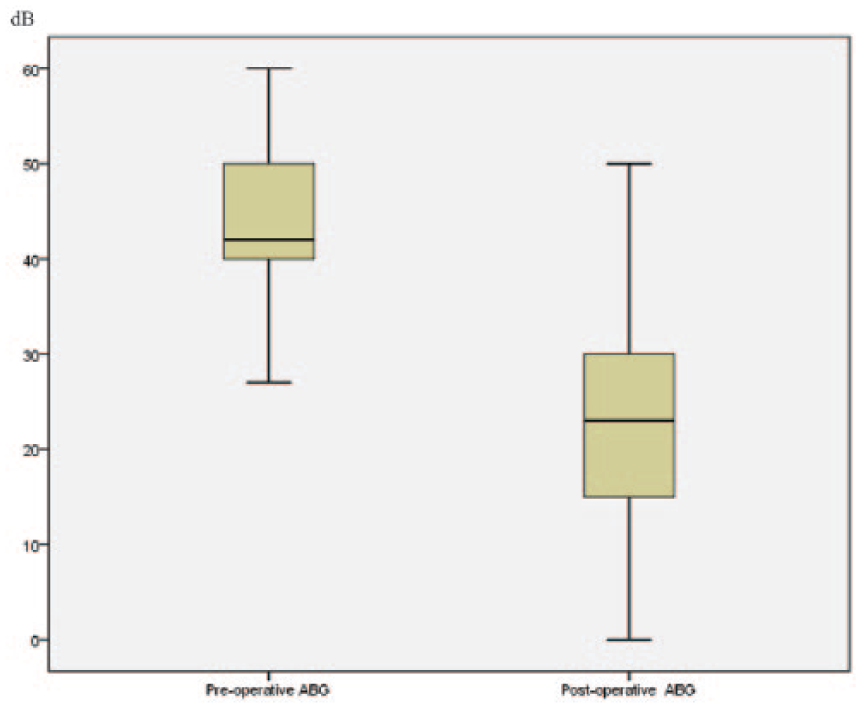
Box and whisker plots showing preoperative extended tone pure tone average (PTA) air bone gaps (ABG) with average (SD) values of 44 (7) dB (range, 27-60 dB). Average (SD) postoperative extended tone PTA ABG = 23 (10) dB (range, 0-50 dB). As shown in Table 2, the average (SD) improvement of extended tone PTA ABG = 21 (12) dB; the change between pre- and post-ABG was statistically significant at P < .001 (paired 2-tailed t test).
Tympanic Membrane Closure/Reoperation
Closure of TM perforations occurred in 173 of the 183 ears with perforations (95%), and the 10 failures had to undergo repeat myringoplasties. Adhesions were released in 14 ears, and the ossicles had to be readjusted in 3 ears.
Complications
Complications were 1 episode of stapes luxation and 2 instances of transient facial nerve weakness resulting from removal of tympanosclerosis from the horizontal facial canal. There were no instances of sensorineural hearing loss and no extrusions of the repurposed ossicles.
Discussion
We found, during review of the otologic literature relating to ossiculoplasty, that much of the discussion of repurposing of the native ossicles took place decades ago in the 1970s and 1980s.6-9 More recent reports have served as a reminder that these techniques are still viable, even with the availability of prostheses. 10 However, the patient’s own ossicles may be the only option for ossiculoplasty, as literature that is not from Europe or the United States reminds us. 11 Indeed, the patient’s ossicles have several positives: they are available in the patient, they can be banked in soft tissue for reuse later, 11 they do not extrude or dissolve in place, 12 and they do not cost anything.
This brief report outlined the use of patient ossicles for ossiculoplasty. We have been careful to comply with the current standards of reporting otologic operative results: presence of stapes suprastructure, type of graft used, and air bone gap average. 13 In reporting the hearing of these patients pre- and postoperatively, however, we had to forgo the use of the scatterplot as a standard presentation of hearing loss and hearing change. As the authoritative work on this subject, the article by Gurgel et al 14 noted that many countries (and Ethiopia is one of them) do not use word recognition testing, thereby eliminating 1 axis of the scatterplot. And in the cases of changes in conductive hearing loss, Gurgel et al advised the reader to use the change in PTA air bone gap model as described by the American Academy of Otolaryngology–Head and Neck Surgery Committee on Hearing and Equilibrium. 5
Our preoperative hearing findings were uniform across the different types of ossicular pathology. About 60% of all pathologies fell within the 30 to 45 dB air bone gap range, and no preoperative ear showed an air bone gap better than 20 dB. Postoperatively, 158 of 197 ears showed postoperative air bone gaps better than 30 dB (80%), and 89 of 197 showed postoperative air bone gaps better than 20 dB (45%). On average, the postoperative ears showed a 21-dB improvement of air bone gaps without any sensorineural increases or extrusion of ossicles. Columellar struts from a mobile footplate to a reconstructed TM appeared to have the best postoperative hearing improvements, but these cases represented only 11 of 197 ears. Figure 4 depicts the improvement in the means, standard deviations, and ranges of PTA air bone gaps.
In this series of 188 patients (197 ears), we found on microscopic examination a 95% closure of the TM perforations on the first try. Since postoperative tympanometry was not employed, perhaps some small residual perforations were undetected. We cannot explain why our closure rates appear to be so good—whether it is an error in our postoperative evaluations or something advantageous about our technique.
Similarly, we cannot explain the distribution of ages for our patients—ages 12 to 56 years. There was no intentional restriction of ages. In the same vein, there seem to be more female than male patients. This, too, we cannot account for and warrants further evaluation in the future.
Finally, we are well aware of the limitations of a retrospective study compared with a prospective one. However, most of these patients were hundreds of miles from the capital city. The postal communication is rudimentary. Transportation is difficult. Because of these limitations, a progressive clinical study, in which the cohort study design applies, is very difficult. Therefore, we opted for the retrospective clinical study, in which only those patients who returned for re-examination after the ossiculoplasty surgery were included in the study.
We present this report to encourage repair of the ossicular chain in developing countries and to offer a realistic strategy—use of the patient’s own ossicles. Tympanic membrane closure rates and improvements in air bone gaps are acceptable. This article serves to demonstrate that acceptable outcomes are attainable in a resource-poor setting.
Footnotes
Author Note
Es-Hak Bedri is also affiliated to OtoRinoENT-Specialty Clinic, Addis Ababa, Ethiopia.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.