
Abstract
Objective:
The association between online health resources use in specific otolaryngology patients is poorly understood. To better understand health-related Internet use by otolaryngology patients, we surveyed first-visit patients at academic and private practice clinics in Iowa.
Methods:
Data on socioeconomic status, access, and utilization of online resources were collected. Age distributions were compared by t test, and categorical variables were compared by chi-square analysis. Multivariate logistic regression was used to estimate odds ratios for association between independent variables (age, sex, educational attainment, otolaryngology subspecialty, etc).
Results:
Data showed that 8.7% lacked Internet access; an additional 5.4% reported access only in a public place or at work. Younger, more educated, and more urban patients reported higher rates of Internet access. Among university patients, patients seeing head and neck oncologists were most likely to report no Internet access (10.9%). Just over one-third of patients used the Internet to research their health condition prior to their appointment.
Conclusions:
Internet access was far from universal among this large cohort of otolaryngology outpatients. Head and neck cancer (HNC) patients report the least online access among all otolaryngology subspecialties. Providers should consider nonelectronic patient resources for older, more rural, less educated, and HNC patient populations as online/electronic methods of communication may not be accessible to these groups.
Keywords
Introduction
The Internet and associated electronic forms of communication fundamentally changed the model of patient-caregiver interactions. Prior to the Internet, communication and treatment planning was commonly uneven and hierarchical in nature. 1 The expansion of Internet-based health care information gave patients access to information that had historically been available only to health care providers. The increased information fostered more patient-centric discussion, which in turn encouraged a more level, partnership-based model of health care. 2 Today, significant health care interactions via the Internet and electronic correspondence are common and generally well regarded by both physicians and patients.3,4 Furthermore, physicians and large health care organizations have expended effort and resources on building online educational presences.
Disparities in access to and use of electronic health care information, however, do exist. The National Cancer Institute began evaluating US national trends in health information technology usage via the Health Information National Trends Survey (HINTS) starting in 2003. The HINTS data revealed disparities between patient sex, education level, and socioeconomic status, among others.5,6 Additional research has focused on differences in health information technology (HIT) use among specific patient groups (patients with breast cancer, asthma, and in palliative care, among others) to optimize care.7,8 Their results reflected the HINTS data, with older and more rural patients less likely to utilize HIT for their care.
In the US, head and neck cancer (HNC) is more prevalent in patients with less education and lower socioeconomic status (SES).9,10 Taken together with the HINTS data, this same HNC patient group therefore may lack access to the Internet and so be less likely to use the many health resources offered online. Previous publications evaluated otolaryngology-specific website readability and use of HIT resources by head and neck patient caregivers but have not specifically evaluated HNC patients. Additionally, there may be systematic differences in HIT use between individuals in rural and urban settings. To better understand health-related Internet use by otolaryngology patients, including those with HNC, we surveyed patients attending otolaryngology clinics at the University of Iowa and those at a private otolaryngology clinic in Mason City, Iowa.
Methods and Materials
This study was approved by the University of Iowa Institutional Review Board. An English-language survey was provided on paper to patients attending otolaryngology clinics at University of Iowa and the Mason City Clinic of North Iowa at the beginning of their clinic visit (Figure 1). Respondents were provided the option of having the questions read and answers recorded by clinic staff. The medical record was reviewed to determine county of residence. To determine which factors were associated with access to the Internet and researching medical conditions, age distributions were compared by t test, and categorical variables (sex, level of education, residence, and medical condition) were compared by chi-square analysis. Multivariate logistic regression was used to estimate odds ratios for association between independent variables (age, sex, educational attainment, clinic site, subspecialty need, rurality of residence). All variables were entered into a regression model, and stepwise selection was used to identify the optimal model. Rural-urban status was based on county Rural-Urban Continuum Codes (RUCCs) as defined by the US Department of Agriculture, and we defined rural counties as those with RUCC 6-9 (not in a metropolitan area, with urban population of less than 20 000 or completely rural). All data analysis was performed using SAS 9.3.
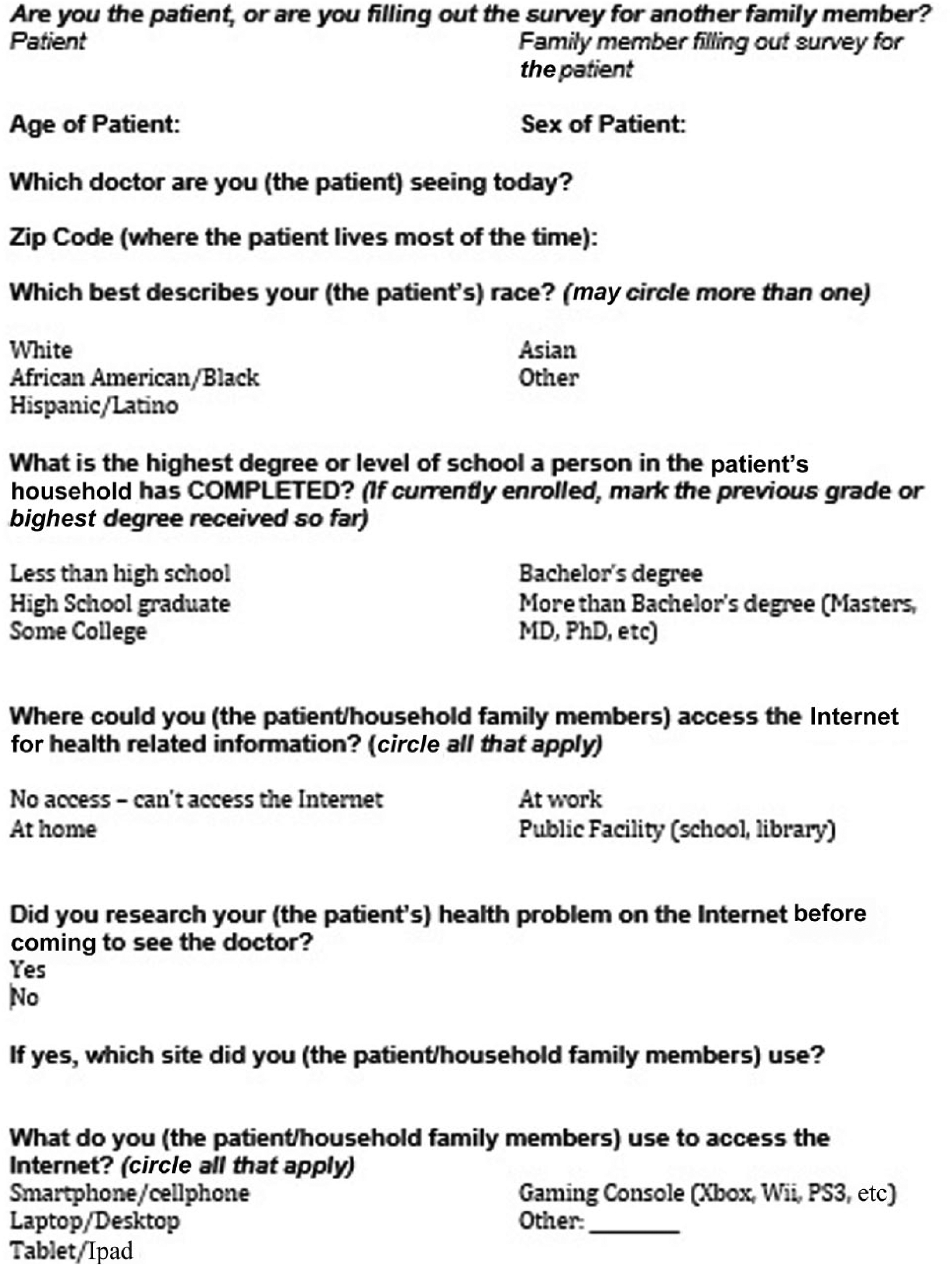
Survey provided to study participants.
Results
Surveys were completed by 1564 patients from 115 counties in Iowa, Minnesota, Illinois, and Missouri—957 patients at University of Iowa Hospitals and Clinics and 607 at the Mason City Clinic of North Iowa (Figure 2). Characteristics of Internet access among the study cohort are shown in Table 1. The proportion of respondents reporting no Internet access at all was 8.7%; an additional 5.4% reported access only in a public place or at work.
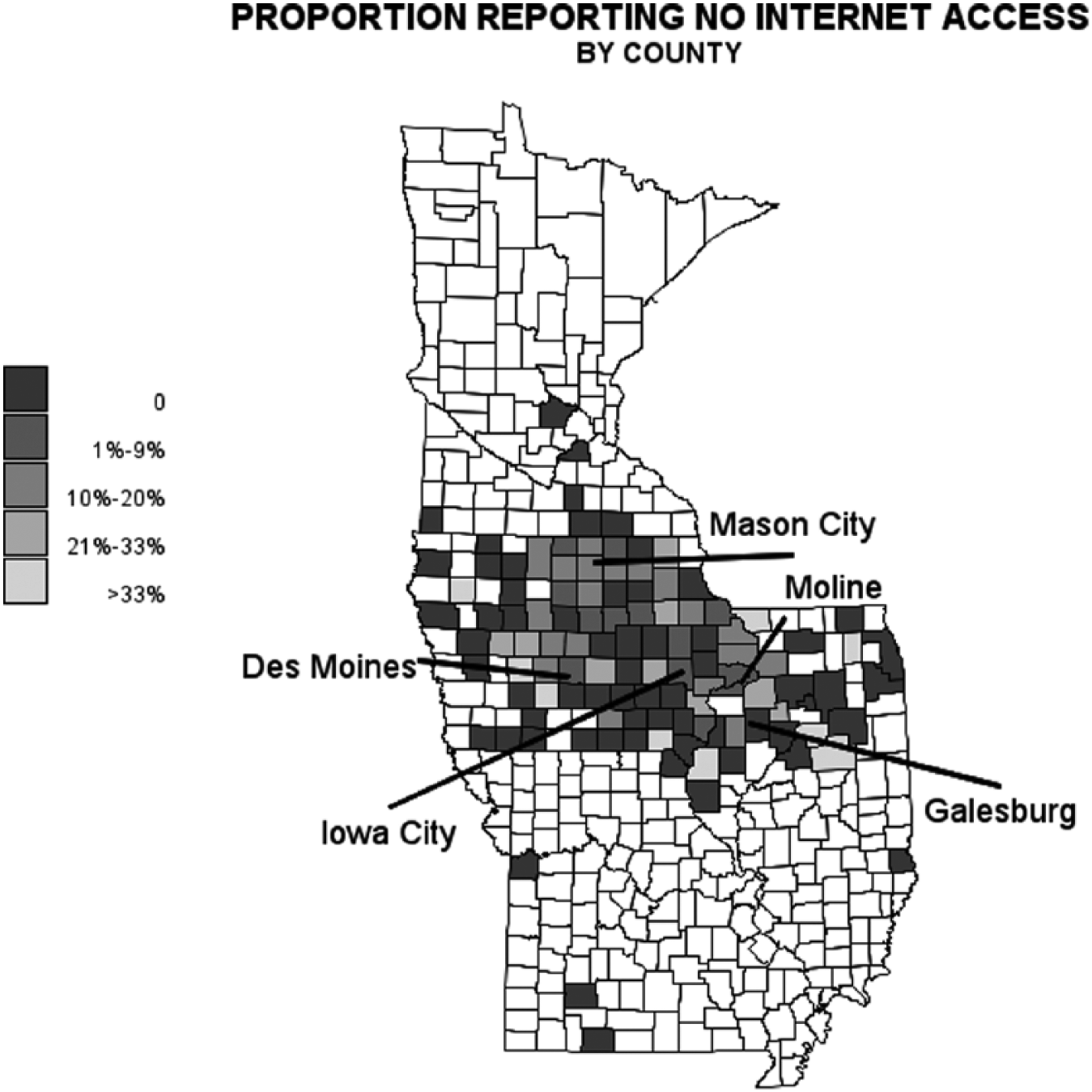
Geographic distribution of self-reported Internet access by home county of patient participant.
Demographics of Internet Access Among Otolaryngology Patients. a
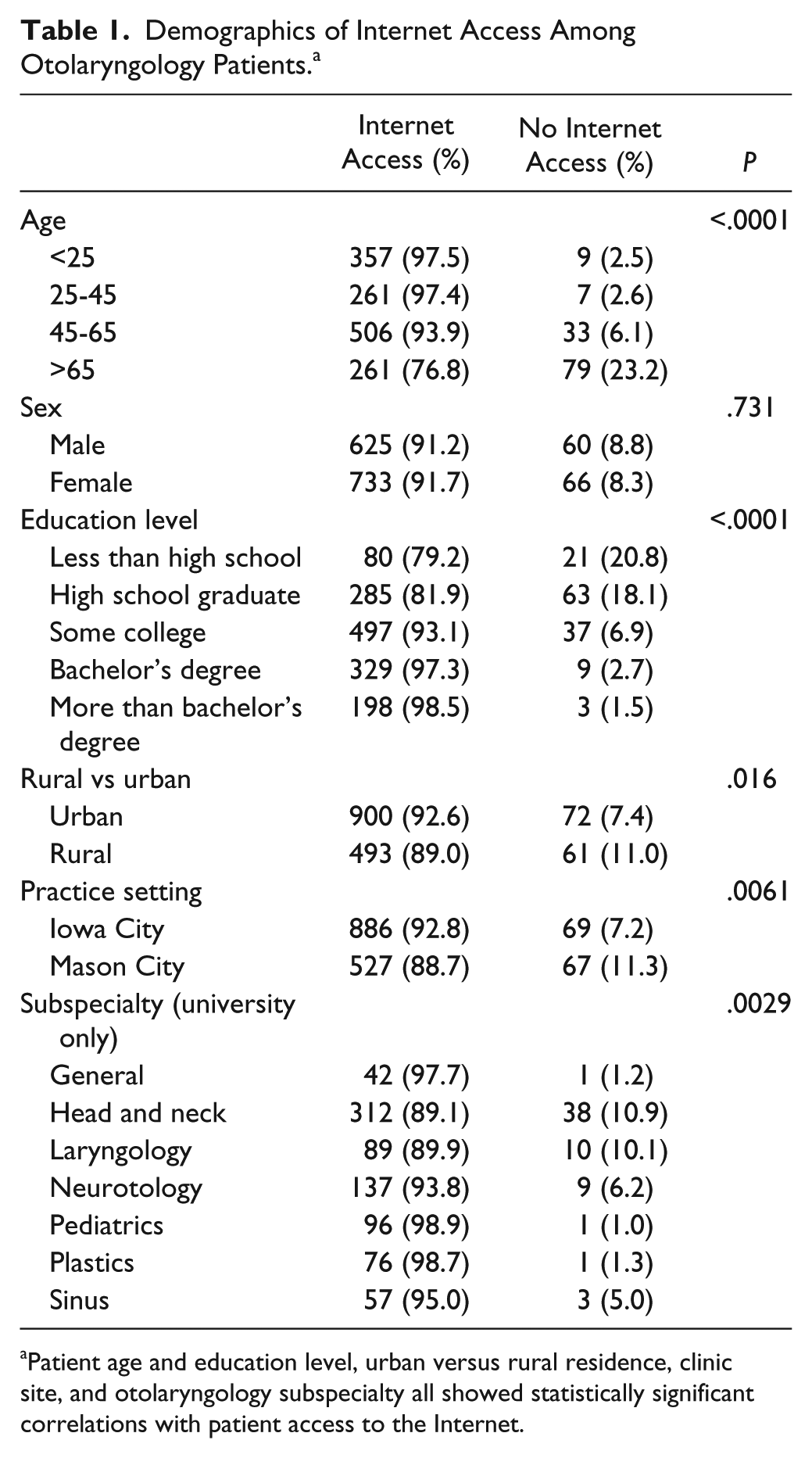
Patient age and education level, urban versus rural residence, clinic site, and otolaryngology subspecialty all showed statistically significant correlations with patient access to the Internet.
Mean age was higher for patients without any Internet access (65 vs 43.9 years, P < .0001). Older patients were progressively less likely to have Internet access, from 97.5% Internet access for patients under age 25 to only 76.8% for patients over age 65. Respondents with higher educational attainment had greater online access, with only 1.5% of respondents with post bachelor level education reporting no Internet access. Conversely, 20.5% of those with less than high school education (P < .0001) reported no Internet access. There was a significant difference between access for individuals attending the Mason City Clinic and those seen at the University of Iowa (88.7% vs 92.7%, P = .006); similarly, patients from urban counties reported 92.6% access compared to 88.9% of patients from more rural counties, P = .016. There were no differences in availability of Internet access between men and women.
When considering only patients at the University of Iowa, whose faculty comprises mostly subspecialists, there was a statistically significant association between Internet access and subspecialty (P = .0029), with proportions varying from 89.2% of head and neck oncology patients to 98.9% of pediatric otolaryngology patients with access.
We also studied whether patients actually performed online research about the health condition that brought them to their clinic visits prior to their clinic visit (Table 2). While a large majority of patients reported having Internet access, 38.8% reported using the Internet to research their health condition prior to their clinic visit. Age was a significant predictor of pre–clinic visit Internet research, with a 53.4% rate among 25- to 44-year-olds and 20.9% among those over 65 years old (P < .0001). Educational attainment was progressively associated with higher rates of Internet research from 11.0% of those with less than high school education to 53.7% of those with more than college education, P < .0001. There was no significant difference between men and women. There was a significant difference between patients seen at Iowa City, at 45.6%, versus Mason City, at 19.8%, and a similar difference between patients living in more urban counties, at 40.7%, versus rural counties, at 27.6% (P ⩽ .0001). More than half of patients who reported specific websites described using more than 1 site, with WebMD the most commonly reported online resource.
Patterns of Internet-Based Health Research by Otolaryngology Patients With Internet Access. a
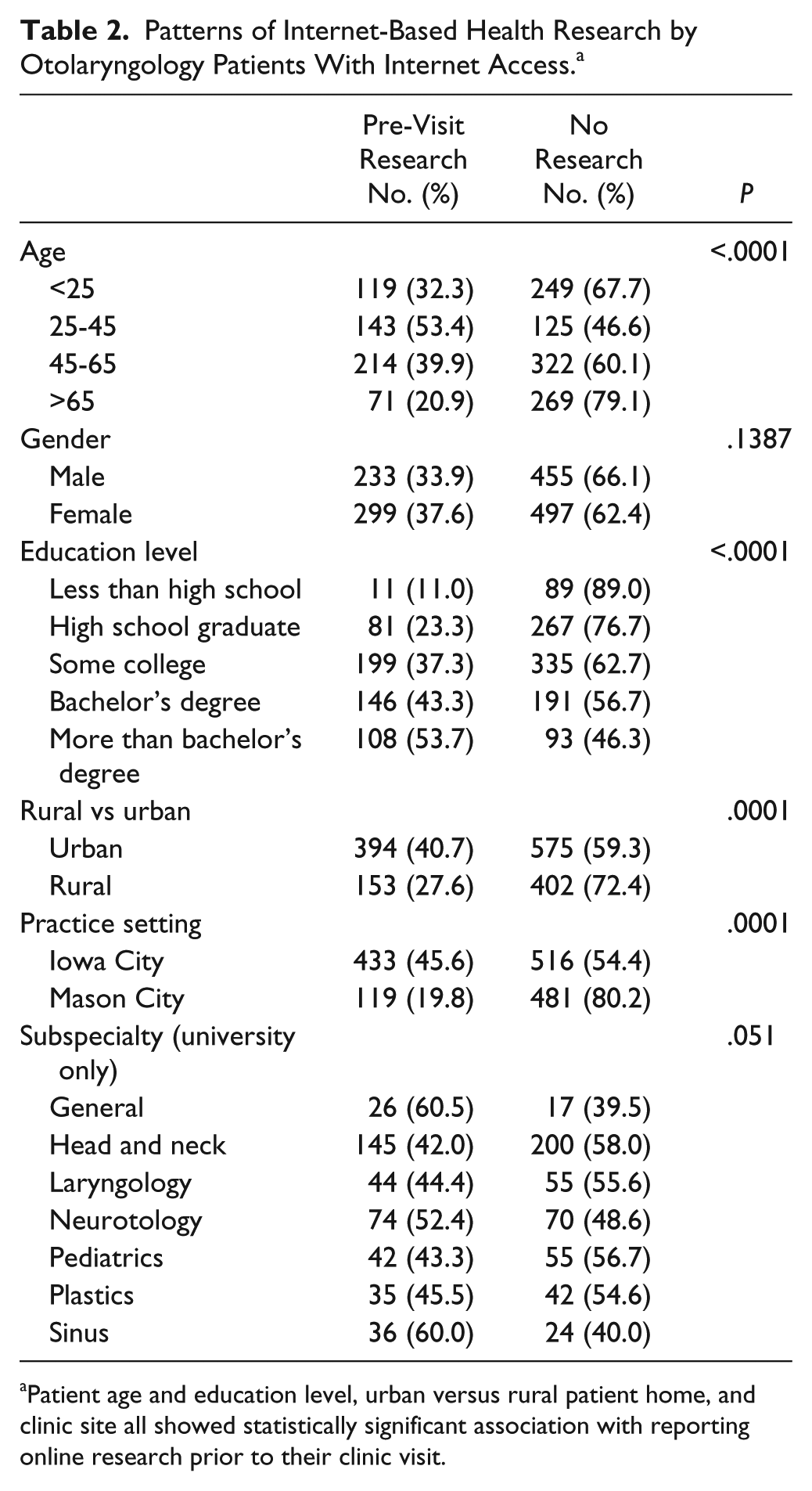
Patient age and education level, urban versus rural patient home, and clinic site all showed statistically significant association with reporting online research prior to their clinic visit.
Discussion
Although most people in the US have access to and report literacy with the Internet, this study highlights specific patient groups for whom online educational resources may be less effective. To our knowledge, this is the first study to quantify online access and evaluate pre-visit patient research trends among otolaryngology patients in the US. Our finding that over 14% of patients lack Internet access in a private setting should inform efforts currently underway by health care providers and systems to better educate and communicate with patients. The findings that older and less educated individuals are less likely to have Internet access should also inform those efforts.
Our results echo previous studies of Internet use by individuals across the US population, with similar inequality of access and use across socioeconomic divisions. The Pew Research Center described Internet access unrelated to the health care setting in broadly sampled surveys of US adults and found similar rates of access and similar effects of socioeconomic conditions. 11 Gurr et al 12 studied a series of 503 patients in a German otolaryngology clinic and described differences based on education status, with degree holders far more likely to use the Internet to obtain health information. Kontos et al 6 in 2014 reported lower SES, male sex, and older age were less likely to participate in eHealth activities, similar to our data and the SES of HNC patients in the US. Privately insured individuals were also more likely to use the Internet than those with public health insurance. Walsh et al 13 found a similar effect of education in an American population of patients with common cancers, as did Kagan et al 14 in a review of HNC patients on the East Coast in 2005. A study of French breast cancer patients found only 24% used the Internet to obtain information. 15 Kim et al 16 found that many cancer patients used the Internet as a primary information source but did not find that these Internet users were particularly well equipped to use the information they obtained.
The data also suggest that Internet access is not synonymous with use of online health resources in the US. Fewer than half of patients in our study used an online resource prior to their office visit. Similar trends were reported in a 2002 study of 330 otolaryngology patients in the UK, where 45% of patients reported having Internet access, but only 13% had used the Internet to obtain information about their own health prior to their clinic visit. 17 Additional reports on the benefits and patient preference of nonelectronic patient communication may explain the disparity between Internet access and health-related Internet use. One US study found patients preferred face-to-face interactions with health care providers—nurse, doctor, or other—over any other way of receiving information. A common reason for this preference was the ability to ask questions immediately for clarification during health care discussions. 1 Patient dissatisfaction with electronic exchanges were further evaluated by Hesse et al, 4 who reported while the number of patients who went first to the Internet with health questions was increasing, those same people also reported a significant decreased trust in information found online. That problem is compounded by the lack of readability of many websites hosting medical information.18,19 Patients may not be clear on how to conduct a useful Internet search given the symptoms or diagnoses they have. Studies show electronic and online resources can be helpful when patients are directly guided to a website,20,21 but our data suggest health care providers should continue to include nonelectronic patient interactions in their practice.
This study faces several limitations. The questions of whether a patient researched an issue online before coming to the appointment could suffer recall bias. 22 Questions on the survey concerning which online website was used likely suffer from recall bias as well. There could also be confusion as to which site a person actually used—in several cases, a patient reported that they first used Google but recorded the name of their choice website within the list of search engine results. There may have been confusion in how to answer the survey when the patient was a child. Additionally, further work utilizing a longitudinal study design would provide a more comprehensive evaluation of research patterns of patients with Internet access, how they used the information they gained, and their satisfaction with their ability to educate themselves.
These findings are specific to the patient population attending clinics at the authors’ institutions. It might be useful to assess patients in other settings with populations and socioeconomic strata not represented in our catchment areas. The proportion of Iowa residents living in a household with Internet access is at the median across states, so data on patients living in areas both above and below the median would be valuable. 23
The survey could also give false confidence in determining a patient’s ease of accessing health-related data as a small subset reported no access at home but did have access at work or public areas. Counting these patients as among “Internet users” could be false—such patients would have to access protected personal health information in a place where their privacy is uncertain.
Conclusion
In a cohort of midwestern otolaryngology patients, overall Internet access and Internet use reflected national trends based on SES. The data also found HNC patients to be at highest risk of lacking Internet access when compared to other otolaryngology subspecialties. Patient access to the Internet was high overall, but Internet access was not synonymous with researching health concerns prior to a clinic visit. Our findings indicate that educational efforts by providers, especially related to head and neck cancer, should not exclusively focus on Internet resources.
Footnotes
Acknowledgements
The authors are deeply indebted to the physicians, clinic staff, physician assistants, and nurse practitioners at both the University of Iowa Hospitals and Clinics, Department of Otolaryngology–Head and Neck Surgery and the ENT and Allergy Department at the Mason City Clinic for their assistance in patient recruitment and data collection, including Ricki Benson, Diane Burke, Krista Buser, Margaret Colwill, Dr Timothy Dettmer, Dr Henry Diggelmann, Jackie English, Karlene Fuller, Pamela Grecian, Himena Harris, Dr Vishram Jalukar, Kara Pasker, Marcy Simpson, Helen Stegall, and Deborah Strike.
Authors’ Note
This work was presented as a poster at Triological Society Combined Sections Meeting, Miami, Florida, USA, January 2016.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding Source: 5T32DC000040-17