
Abstract
Objectives:
A three-dimensional (3D) inversion-recovery (IR) sequence with real reconstruction (3D-real IR) sequence 4 hours after intravenous (IV) gadolinium injection has been used to visualize the endolymphatic hydrops (ELH) in Ménière’s disease (MD). This study was designed to investigate the ELH characteristics in clinically diagnosed definite MD and to explore the pathology of MD with magnetic resonance imaging (MRI).
Methods:
One hundred fifty-four patients with definite MD were included in this study. All patients underwent the IV method. The grades of ELH were analyzed on each image, regions of interest of the cochlear perilymph and the cerebellum white matter were determined, and the signal intensity ratio of the former to the latter (CC ratio) on both sides in patients with unilateral MD was subsequently evaluated.
Results:
Endolymphatic hydrops was observed in 148 patients (96.1%) on the clinically affected side; the remaining 6 patients (3.9%) had no apparent ELH. One hundred fifteen patients (74.7%) had unilateral ELH, and 33 patients (21.4%) had bilateral ELH. Eighteen patients (11.7%) had ELH on the clinically silent side. Patients with moderate and significant grades of ELH in the vestibule and cochlea accounted for 88.3% and 90.3%, respectively. The CC ratio of the affected side (1.39 ± 0.37) was higher than that of the unaffected side (1.18 ± 0.29) (P < .01) in 115 patients with unilateral MD.
Conclusions:
Moderate and significant grades of ELH are common in MD; however, the proposed diagnostic criteria are not fully consistent with ELH. The elevated contrast effect in the affected side in patients with unilateral MD may better reflect the pathologic condition of MD.
Introduction
Ménière’s disease (MD) is a poorly understood inner ear disorder characterized by spontaneous vertigo attacks, fluctuating low-frequency hearing loss, tinnitus, and aural fullness. Its pathological hallmark is the underlying endolymphatic hydrops (ELH). 1 Recently, extensive use of gadolinium (Gd) contrast–enhanced MRI has enabled the depiction of ELH.2,3 Magnetic resonance imaging after intratympanic Gd injection (IT method) 4 and intravenous Gd injection (IV method) 5 has been used to visualize ELH in MD. The IV method is less invasive, independent of the condition of the round window membrane, 6 and results in more uniformly distributed Gd 7 compared to the IT method. Moreover, the IV method is able to visualize the bilateral labyrinth simultaneously, 5 enabling MRI to ascertain bilateral blood-labyrinth barrier permeability. Therefore, the IV method was used in our study.
The clinical diagnostic criteria 8 for MD, jointly formulated by the American Academy of Otolaryngology–Head and Neck Surgery (AAO-HNS) and the Bárány Society, proposed 2 categories: “definite” and “probable” MD. The diagnostic criteria of definite MD include episodic vertigo that occurs in a period from 20 minutes to 12 hours and is related to low-to-medium frequency sensorineural hearing loss and fluctuating aural symptoms (tinnitus and/or fullness) in the affected ear. To our knowledge, MD was still a mystery disease with a difficult differential diagnosis, 9 with vestibular migraine and sudden sensorineural hearing loss accompanied by vertigo and tinnitus clinically. Therefore, we supposed that the ELH, as detected by Gd MRI, was essential for the diagnosis of MD as a supplementary tool for clinically based diagnosis. Furthermore, the pathogenesis of MD remained unclear; thus, investigating detailed MRIs may help illustrate the pathology of MD.
Therefore, 154 patients with definite MD confirmed by the proposed diagnostic criteria were included in our study; all patients underwent the IV method. The MRIs were used to analyze the grades of ELH and the characteristics of perilymphatic enhancement in patients with MD. We investigated the characteristics of ELH in clinically diagnosed definite MD and explored the pathology of MD with MRIs.
Materials and Methods
Patients
One hundred fifty-four patients (82 women, 72 men) were included from March 2016 to December 2017, with a mean age of 50.9 ± 14.1 years (range, 7-83 years). Only patients conforming to the diagnostic criteria of definite MD were enrolled. Neurotologic evaluations were performed, including electro-otoscopy, audiometry, and tympanometry. The study obtained permission from the medical ethics committee of the Eye, Ear, Nose, and Throat Hospital of Fudan University, and all patients signed an IV Gd contrast operation consent form.
Intravenous Gd Injection and MRI Acquisition
All patients underwent IV injection of a double dose (0.4 mL/kg body weight) of Gd-HP-DO3A; 4 hours later, MRI was performed. For the IV method, all scans were performed on a 3T MRI scanner (Verio; Siemens Healthcare, Erlangen, Germany) using a 32-channel phased-array receive-only coil. T2-space and 3D real IR sequence MRIs were applied for collecting images. The parameters for the 3D real IR sequence were as follows: voxel size = 0.17 × 0.17 × 0.6 mm; scan time = 15 minutes and 20 seconds; repetition time = 6000 milliseconds; echo time = 181 milliseconds; inversion time = 1850 milliseconds; slice thickness = 0.6 mm; field of view = 160 × 160 mm; and matrix size = 768 × 768.
Image Evaluation
T2-space imaging was used to rule out vestibular schwannoma or other causes of vertigo and hearing loss. The grades of ELH were evaluated according to the expansion of the vestibule and cochlea, which were classified into 3 stage gradings: none or mild, significant, and significant by Nakashima grading standard 10 (Table 1). The ELH were judged by 2 experienced radiologists who were blinded to the diagnosis of all patients. For patients who underwent the IV method, the perilymph was enhanced while the endolymph was not; we randomly determined 3 points on both basal turns of the cochlear perilymph and a coplanar circular 50-mm2 interest region of the cerebellum white matter on 3D real IR images (Figure 1). The intensity ratio of the cochlear perilymph to cerebellum white matter (CC ratio) was calculated. The data were analyzed with blinding of clinical diagnosis status. Moreover, Photoshop CS4 (Adobe Systems, San Jose, California, USA) was used to calculate the area ratio of the endolymphatic space to the vestibular space.
3-Stage Grading of Endolymphatic Hydrops Using Magnetic Resonance Imaging.
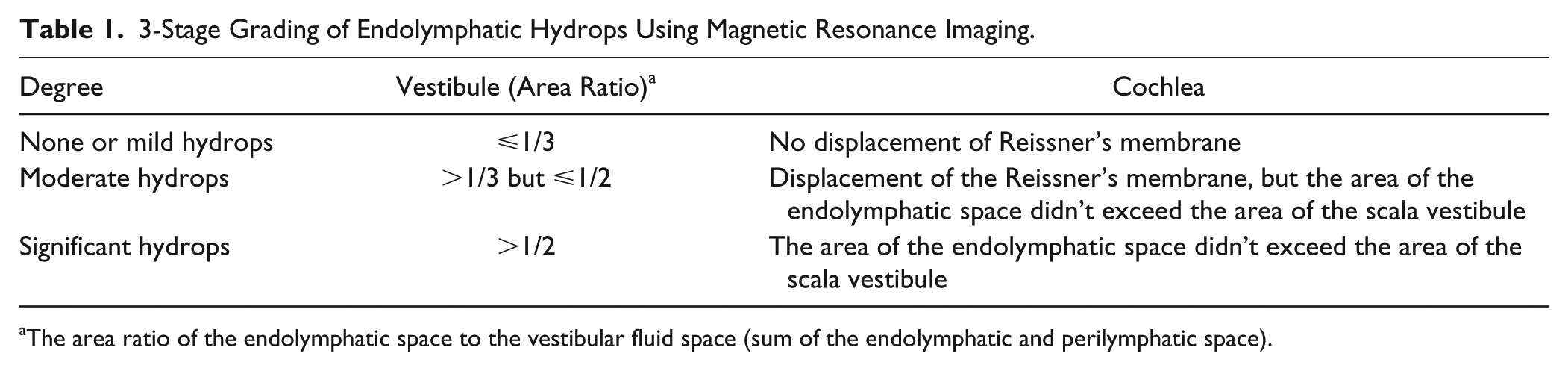
The area ratio of the endolymphatic space to the vestibular fluid space (sum of the endolymphatic and perilymphatic space).
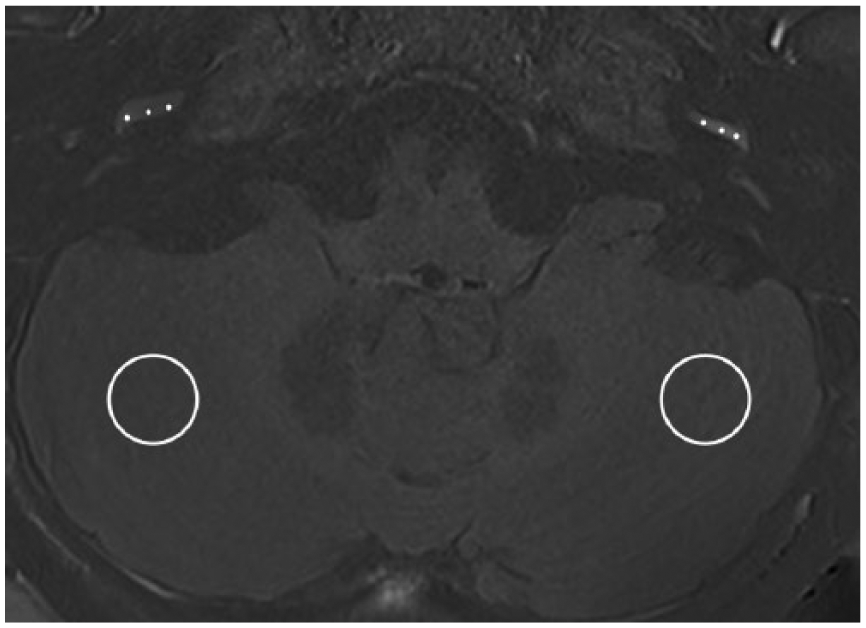
A three-dimensional real inversion-recovery image at the level of the cochlear basal turns after intravenous gadolinium injection with left Ménière’s disease is presented. On this image, 3 points of interest on the scala tympani of both cochlear basal turns and a 50-mm2 circular region of interest on the cerebellar white matter coplanar with the basal turn of both cerebellar hemispheres were set.
Statistical Analysis
Statistical analyses were performed using SPSS Statistics 17 software package (IBM, Chicago, Illinois, USA). Data are shown as mean ± SD. A paired t test was used to compare the differences in CC ratio between the affected and unaffected sides in patients with unilateral MD. Differences were considered statistically significant when P < .05.
Results
Imaging Findings
All patients (N = 154) were diagnosed as definite MD by diagnostic criteria. One hundred forty-eight patients (96.1%) presented ELH in the affected ear, and 6 patients (3.9%) had no significant ELH in the affected ear. One hundred fifteen patients (74.7%) had unilateral ELH, and 33 patients (21.4%) had bilateral ELH. In 33 patients, 15 (9.7%) had ear symptoms in the contralateral side, and 18 (11.7%) were clinically silent in the contralateral side. The ELH grading was based on Nakashima grading standard (Figure 2). The percentages of different ELH grades in the initially affected side of all patients are described in Table 2; 88.3% of vestibules and 90.3% of cochlea presented moderate or significant ELH. The imaging of the vestibule and cochlea was unclear in 2 individuals (1.3%) and 3 individuals (1.9%), respectively. The signal intensity of the basal turn of the cochlea in the affected side was slightly higher than that in the unaffected side in 115 patients with unilateral MD on visual inspection (Figure 3A), and the CC ratio (Figure 3B) of the affected side (1.39 ± 0.37) was higher than that of the unaffected side (1.18 ± 0.29) (P < .01). However, no apparent differences in signal intensity were visible to the naked eye in the apex or medial turn of the cochlea.
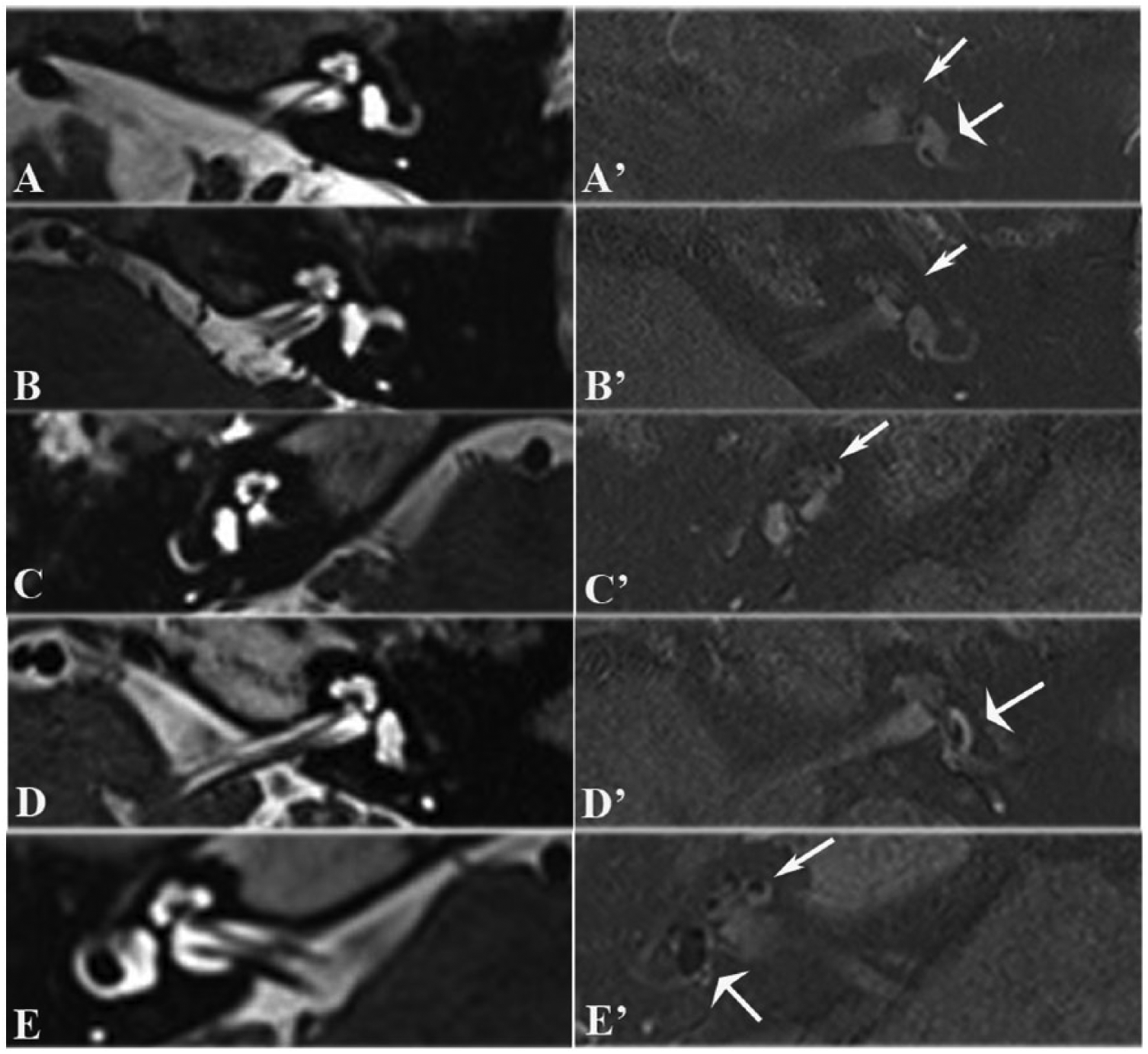
Magnetic resonance imaging scans of patients with different degrees of endolymphatic hydrops (ELH). (A-E) Images of T2-space sequence. (A’-E’) Images of 3-dimensional real inversion-recovery performed 4 hours after intravenous gadolinium injection. (A’) No ELH in vestibule or cochlea. (B’) Mild ELH in cochlea, no ELH in vestibule. (C’) Moderate ELH in cochlea, no ELH in vestibule. (D’) Moderate ELH in vestibule, no ELH in cochlea. (E’) Significant ELH in vestibule and cochlea. Cochlea (thin arrows) and vestibule (broad arrows).
Percentages of Different Degrees of Hydrops in All Patients.


Magnetic resonance imaging scans of patients with unilateral Ménière’s disease (MD). (A) Three-dimensional real inversion-recovery images at the level of the cochlear basal turns after intravenous gadolinium injection in 3 patients with unilateral MD. The signal intensity of the cochlear basal turn in the affected side (thin arrows) was higher than that in the unaffected side (broad arrows). (B) The CC ratio in the affected side was higher than that in the unaffected side (P < .01).
Discussion
All patients enrolled were diagnosed with definite MD by clinical diagnostic criteria. There was no significant gender difference (82 women, 72 men) in the 154 enrolled patients. 11 The IV method was used in our study, as it has recently been applied to the in-depth investigation of ELH clinically, and it rendered the function of the blood-perilymph barrier visible. 12 In accordance with others,13-15 ELH was pronounced in symptomatic ears in 148 (96.1%) patients; the remaining 6 (3.9%) patients had no apparent ELH. However, in the review of Foster and Breeze, 16 165 cases had been reported to fulfill the AAO-HNS 1995 criteria. Two studies found ELH in 100% of MD cases that met the AAO-HNS 1995 criteria.17,18 Only 2 of the 165 cases had been classified as MD without ELH, and these cases were mentioned incidentally in a single study of strial changes in the contralateral ear of MD patients. Moreover, since MD has a difficult differential diagnosis with other diseases clinically 9 and since ELH, as detected by Gd-contrast MRI, was a tool for differential diagnosis of MD, 19 we speculated that clinical symptoms combined with ELH were the most accurate diagnostic criteria for MD. More than half (74.7%) of our patients had unilateral ELH; 21.4% of patients had bilateral ELH, which is higher than the data demonstrated in previous studies (16.7% 20 and 14% 21 ). Using MRI, Barath et al 13 and Yamazaki et al 14 found ELH in 22% and 23.3%, respectively, of clinically “silent” ears in unilateral MD, both of which were higher than an incidence of 11.7% in clinically “silent” ears in our series. The number of patients we recruited outnumbered that in the previous 2 studies. Based on these data, statements about how ELH relates to symptoms of MD cannot be definitive. Moreover, clinical history alone may not provide a comprehensive assessment of bilateral MD. 22
The contrast effect of the affected side (1.39 ± 0.37) was higher than that of the unaffected side (1.18 ± 0.29) (P < .01) in patients with unilateral MD. This was similar to the results of previous studies,12,14 although the references for cochlear signal intensity calculation were different. The alteration of signal intensity can be due to 3 possible causes: (1) impaired blood-perilymph barrier,23,24 (2) blockage of neuroaxonal transport mechanisms, 25 and (3) cellular immune reaction. 26 The alteration in signal intensity may reflect the pathology of MD. However, the elevated signal of MD was less apparent than that in sudden sensorineural hearing loss, 27 so it was easily overlooked.
The limitations of the present study were that the signal intensity measurement was conducted only in the regional basal turn of the cochlea, which cannot represent the entire cochlea or vestibule, and only 1 radiologist performed the measurements of signal intensities. The IV-administered Gd agent distributes into the perilymph space of the scala tympani through the blood-perilymph barrier, and elevation of the cochlear basal turn signal intensity is most easily observed 4 hours after IV Gd injection on 3D real IR in human subjects.5,14 Therefore, we selected the basal turn of the cochlea and the cerebellum white matter for reference to enable the statistical comparison of the cochlear signal intensity of both sides with the IV method. To ensure the reliability of the signal intensity measured in the region of interest of the cochlea and to diminish the measurement error, we determined 3 points in every region of interest and averaged the signal intensities for analysis.
In conclusion, moderate and significant grades of ELH are common in MD; however, the proposed diagnostic criteria are not fully consistent with the ELH. Therefore, we speculate that Gd MRI ELH detection, as a supplementary tool for clinically based diagnosis, may be essential for the diagnosis of MD. The elevated contrast effect in the affected side in patients with unilateral MD may reflect the pathological condition of MD. Overall, our study was conducted prospectively, which may be helpful for the accurate diagnosis of MD.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the National Natural Science Foundation (No. 81670933).