
Abstract
Objectives:
This study aimed to compare the characteristics of idiopathic unilateral vocal fold paralysis (IUVFP) in elderly versus younger patients, including the diagnostic yield of computed tomography (CT) scans for identifying the structural causes of IUVFP.
Methods:
We retrospectively analyzed medical records of the patients initially diagnosed with IUVFP in a single referral tertiary hospital. We compared patients’ baseline characteristics, initial symptoms, laryngoscopic findings, and prevalence of structural causes on CT scans with respect to age (younger, <65 years vs older, ⩾65 years).
Results:
One hundred forty-two patients were enrolled (90 younger, 52 older). Evident structural causes were more frequently found on CT in older patients than younger patients (40.4% vs 22.2%, P = .034). Among truly idiopathic cases (70 younger, 31 older), recovered vocal fold mobility was identified in 48.6% younger and 41.9% older patients (P = .666). There was no statistically significant difference in the characteristics between unrecovered and recovered subjects of the older patients with true IUVFP (all P > .05).
Conclusions:
The CT scans provided significantly higher diagnostic yields in older patients than younger patients. The degrees of symptoms and complications and likelihood of natural recovery did not significantly differ between younger and older patients with IUVFP.
Introduction
In older people, dysphonia is a common problem caused not only by the aging of vocal fold structures but also by accompanying respiratory, neurologic, or musculoskeletal diseases. A recent study based on the Korean National Health and Nutrition Examination Survey reported that 8.5% of the general geriatric population complained of vocal problems. 1 And an epidemiologic study of a US population that visited clinics to seek treatment reported a dysphonia prevalence of 29% among older patients. Furthermore, 5% of these dysphonic older patients exhibited impaired vocal fold movement, the incidence of which proportionally increased with advancing age. 2
The most common etiology of unilateral vocal fold paralysis (UVFP) is an iatrogenic cause, such as thyroidectomy (30%-37%).3,4 Approximately 30% of cases of UVFP are idiopathic in nature, and a review of a large case series reported that 36% ± 22% of patients with idiopathic UVFP (IUVFP) achieved complete or partial recovery and 52% ± 17% patients experienced subjective voice recovery; however, spontaneous recovery was rare after the first year from onset. 5 A computed tomography (CT) scan covering the skull base, neck, and mediastinum around the vagus or recurrent laryngeal nerve (RLN) is usually recommended to rule out undetected extra-laryngeal causes, including malignancies, in patients with IUVFP. 6 However, 2 recent studies concerning the diagnostic efficacy of CT in patients with impaired vocal fold movement reported very low diagnostic yields (2.9%-6.0%) and urged caution when deciding whether to use CT scans.7,8
Regardless of the aforementioned findings, it could be hypothesized that the risk of undetected underlying structural causes may be relatively higher among older IUVFP patients than their younger counterparts. Furthermore, older patients with IUVFP may have a high risk of complications such as aspiration pneumonia due to a decreased vocal fold mobility and a low respiratory toileting capacity; additionally, older patients may have a worse recovery rate. Therefore, the diagnosis and management of IUVFP should be approached differently in older patients. As yet, however, no study has addressed this issue.
In this study, we aimed to identify and compare the characteristics of older and younger patients with IUVFP in terms of (1) the diagnostic yields of CT scans for identifying the structural causes of IUVFP and (2) degrees of symptoms/complications and likelihood of recovery. We also aimed to identify at-risk older patients requiring early intervention (ie, those with a high risk of complications, possibly with underlying comorbidities or a poor chance of natural recovery).
Materials and Methods
Patients
We retrospectively reviewed the medical records of patients diagnosed with vocal fold paralysis during the initial visit to the department of otolaryngology at our tertiary referral hospital from 2007 to 2016. We only included patients who were aged 18 years or older at diagnosis and had no concurrent incompletely cured malignancies (particularly lung cancer) within the past 5 years. Patients with plausible causes of vocal fold immobility (eg, iatrogenic causes such as a recent history of endotracheal intubation or surgery or trauma around the larynx, thyroid, lung, mediastinum, aortic arch, or skull base) or bilateral paralysis were excluded. The process of study subject enrollment is depicted in Figure 1. Our Institutional Review Board approved this study and waived the requirement for informed consent.
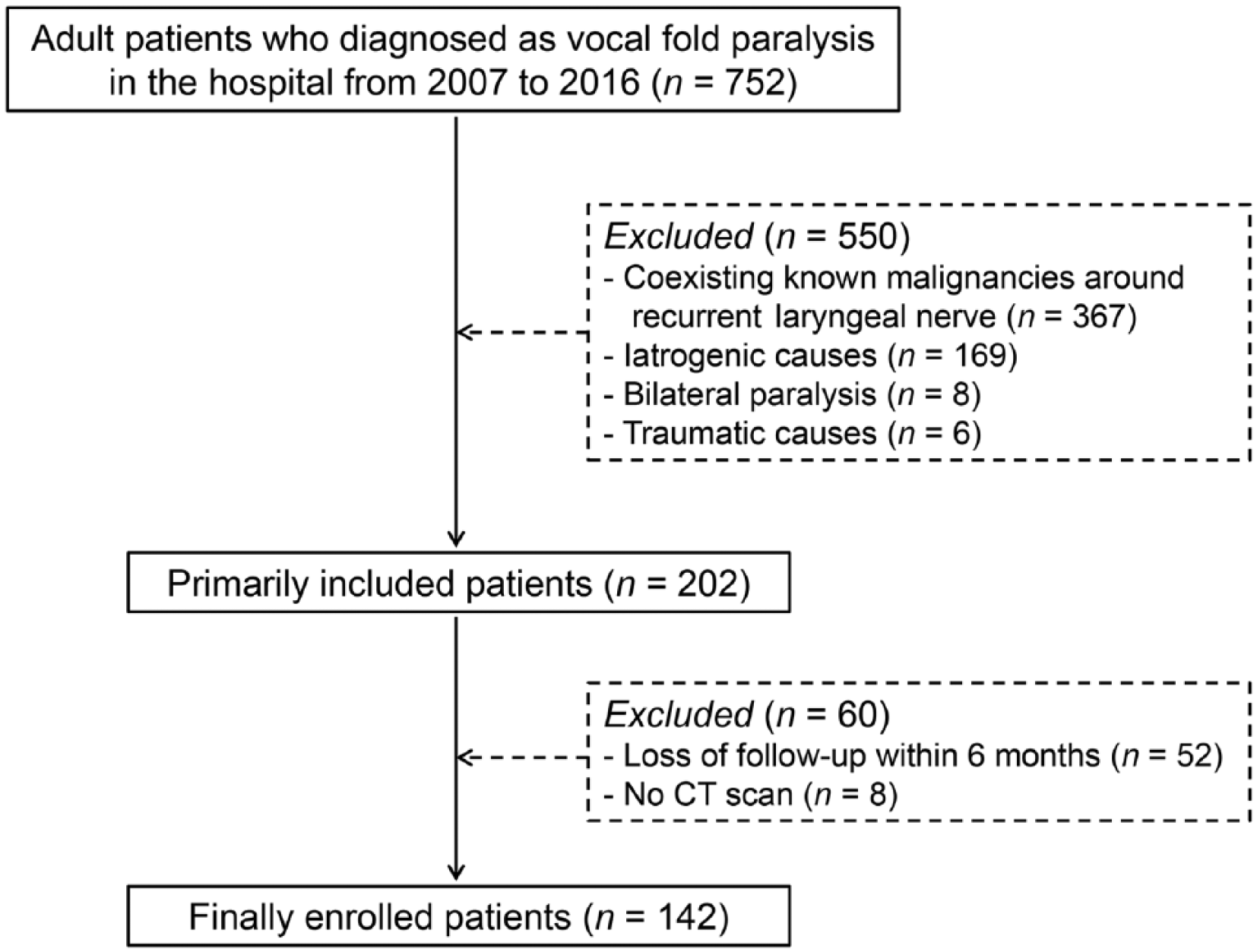
Diagrammatic representation of patient selection.
Variables
We reviewed the patients’ characteristics, including age, sex, and comorbidities, and analyzed their symptoms and laryngoscopic findings at the initial visit. All patients underwent CT scans covering the skull base to the chest, and some underwent esophagography or esophagoscopy; we subsequently determined the incidence of the detection of structural causes of IUVFP from those studies. A positive CT finding was defined as an evident radiological abnormality associated with the compression, encasing, or invasion of the vagus nerve or RLN on the affected side. We followed all patients for more than 6 months; we also investigated their clinical courses, including changes in vocal fold mobility and associated symptoms, development of complications/morbidities, and need for intervention to address the paralyzed vocal fold, every 3 months during the first year of follow-up. We defined complete recovery as the return of paralyzed vocal fold mobility to a level symmetrical to that of the contralateral normal fold. We confined the evaluation of complications/morbidities to patients requiring admission for serious illnesses definitely attributable to IUVFP, such as aspiration pneumonia or severe poor oral intake.
Statistical Analyses
We compared the incidence of detection of the structural causes of IUVFP, degree of symptoms/complications, and likelihood of recovery from IUVFP between older and younger patients. Furthermore, we analyzed risk factors for poor natural recovery or complication development in older patients with IUVFP. We used Fisher’s exact test and the Mann-Whitney U test to compare categorical and continuous variables, respectively. We performed all analyses using IBM SPSS Software (version 22.0; IBM Corp, Armonk, New York, USA), and we considered a 2-sided P value of <.05 to be statistically significant.
Results
Characteristics of Older and Younger Patients
We enrolled a total of 142 patients and divided them into 2 groups based on their age at diagnosis: younger group (n = 90, <65 years) and older group (n = 52, ⩾65 years). An intergroup comparison of characteristics is shown in Table 1. The older group had a predominance of male subjects (63.5% vs 43.3% [younger group], P = .024). Comorbidities such as diabetes and cardiovascular disease were more frequent in the older group, whereas the groups did not differ in terms of pulmonary or neuromuscular diseases. Vocal change was the most common initial symptom in both groups, and although moderately serious problems such as aspiration, dysphagia, or dyspnea were relatively more frequent in the older group, this intergroup difference was not statistically significant. Regarding laryngoscopic findings, left-side involvement, complete paralysis, and a paramedian fixed location were more commonly identified in both groups.
Patient Characteristics According to Age at the Time of IUVFP Diagnosis (N = 142). a
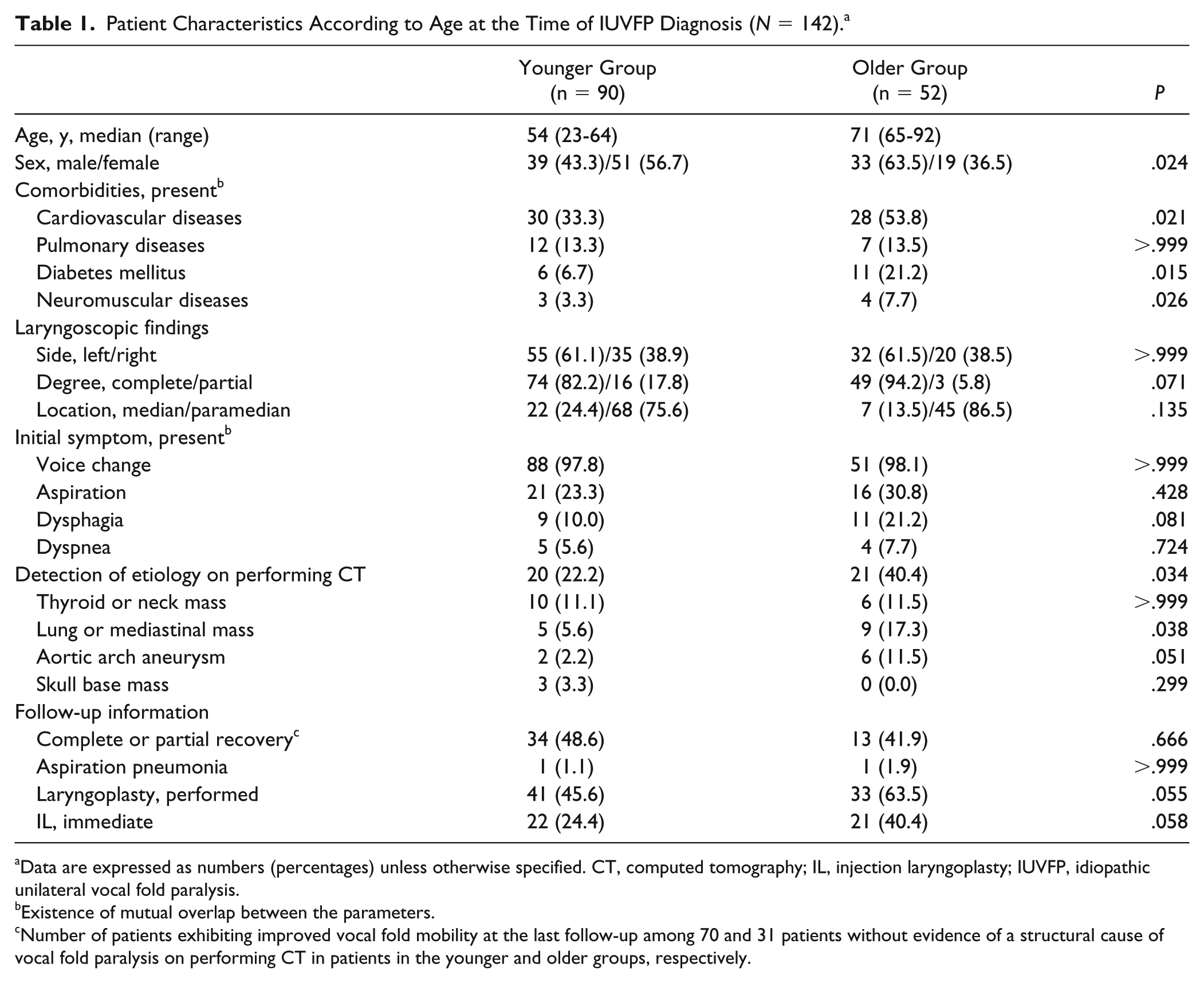
Data are expressed as numbers (percentages) unless otherwise specified. CT, computed tomography; IL, injection laryngoplasty; IUVFP, idiopathic unilateral vocal fold paralysis.
Existence of mutual overlap between the parameters.
Number of patients exhibiting improved vocal fold mobility at the last follow-up among 70 and 31 patients without evidence of a structural cause of vocal fold paralysis on performing CT in patients in the younger and older groups, respectively.
All patients underwent CT scans to identify the structural causes of paralysis, and evident causes were more frequently found in the older group than the younger group (40.4% vs 22.2%, P = .034). In the younger group, thyroid cancer involving the RLN and a neurogenic tumor or metastatic cancer involving the vagus nerve were the most common structural causes of IUVFP (11.1%). By contrast, lung cancer or a mediastinal mass were the major causes of IUVFP in the older group (17.3%), followed by aortic arch aneurysm (11.5%).
For all patients, the median follow-up duration was 13.3 months (range, 6.3-36.5 months). Among truly idiopathic cases (ie, no evidence of a structural cause of paralysis on CT scans), complete recovery of vocal fold mobility was identified at the last visit in 11 of 70 (15.7%) patients in the younger group and 4 of 31 (12.9%) patients in the older group. Furthermore, 23 (32.9%) and 9 (29.0%) patients in the corresponding groups exhibited partial recovery of vocal fold movement and improved voice quality. Generally, age did not significantly correlate with the natural paralysis recovery rate of paralysis in the younger and older groups (48.6% vs 41.9%, P = .666).
During the observation period, we performed laryngoplasty (injection laryngoplasty and framework surgery) in 41 (45.6%) patients in the younger group and 33 (63.5%) patients in the older group. Overall, 43 (30.3%) patients underwent early laryngeal intervention within the first 3 months, and the rate of patients undergoing early intervention was higher in the older group than the younger group (40.4% vs 24.4%, P = .058). Among the total 101 patients with IUVFP, injection laryngoplasty was performed in 30 (29.7%) subjects without any framework surgery. The frequency of early interventions in IUVFP patients also appeared to be higher in the older group (13/31 patients, 41.9%) than the younger group (17/71 patients, 17.3%). We identified aspiration pneumonia in only 1 patient in both groups; we did not observe other significant complications of vocal fold paralysis.
Comparison of the Characteristics of Older Patients With IUVFP Based on Recovery From Paralysis
Next, we explored predictors of a higher risk of poor natural recovery or complicating morbidity requiring early intervention among older patients with IUVFP. Among the 31 truly idiopathic older patients, 13 (41.9%) demonstrated natural recovery of vocal fold mobility. Despite a comparison of demographic factors, including age, sex, comorbidities, initial laryngoscopic findings, and symptoms, between unrecovered and recovered patients, we did not identify any statistically significant difference. Similarly, we indicated 8 and 5 unrecovered and recovered patients, respectively, for immediate laryngeal intervention (injection laryngoplasty), but this intergroup difference was not significant (Table 2).
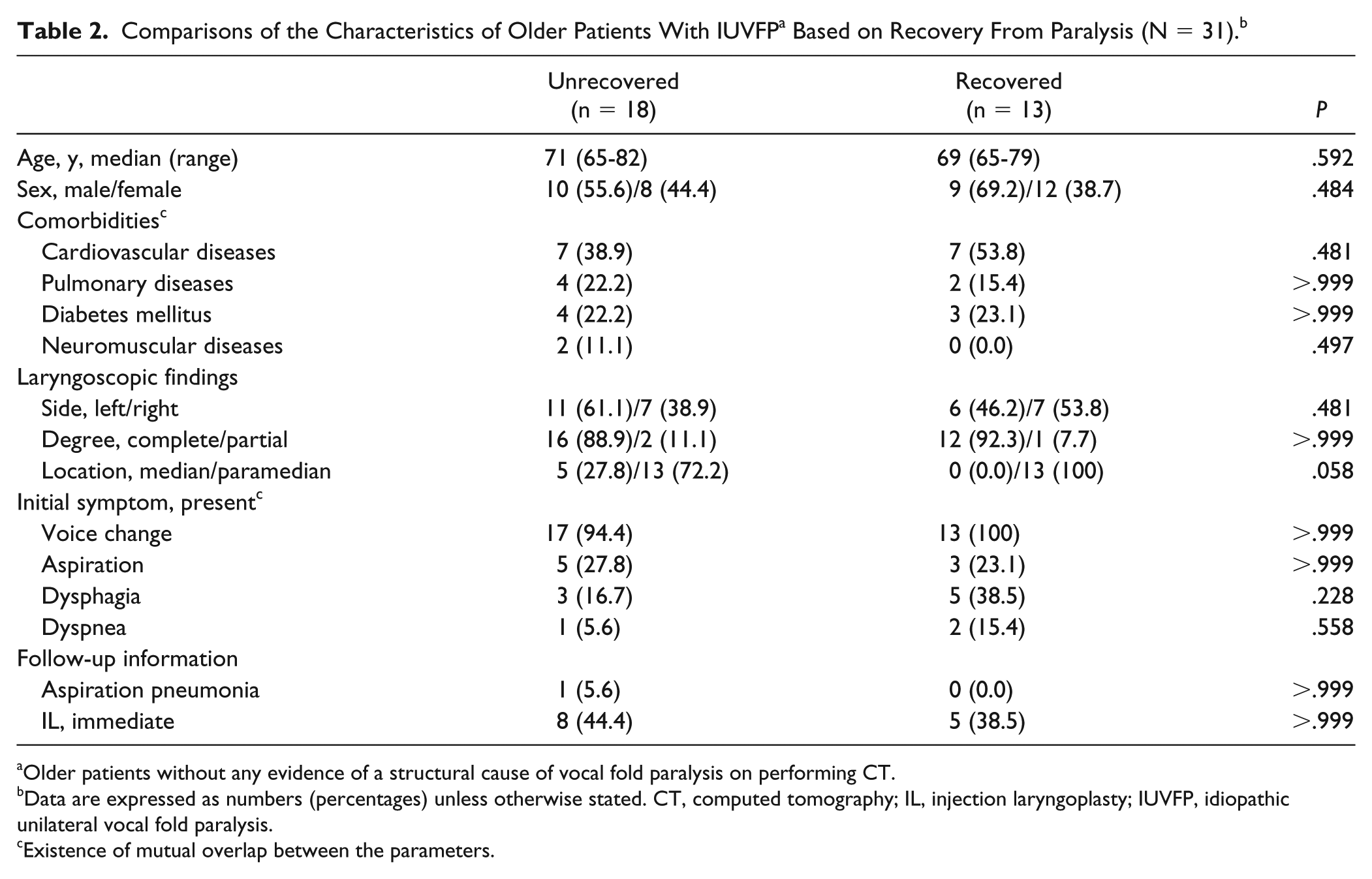
Older patients without any evidence of a structural cause of vocal fold paralysis on performing CT.
Data are expressed as numbers (percentages) unless otherwise stated. CT, computed tomography; IL, injection laryngoplasty; IUVFP, idiopathic unilateral vocal fold paralysis.
Existence of mutual overlap between the parameters.
Discussion
In this study, we compared the clinical characteristics of patients with IUVFP according to age. We observed a predominance of male subjects in the older group and a predominance of a paramedian-fixed vocal fold location and left-side involvement in both groups. These results were in line with those of a previous epidemiologic study on UVFP in Korean patients not stratified by age. 9 We found that older patients did not have a significantly higher incidence of serious initial symptoms, including aspiration, dyspnea, or dysphagia, in contrast to our expectations. Older patients may have a greater risk of vocal dysfunction related to a greater number of co-existing deconditioning diseases and reduced fundamental laryngeal function (eg, sensation and clearance of secretions and poorer pulmonary reserves). 10 We hypothesized that older patients would have more underlying comorbidities that could serve as risk factors for nonstructural causes (ie, nonvisible but plausible causes such as neuropathy) related to vocal fold immobility. Although we more frequently observed cardiovascular disease and diabetes in patients in the older group than patients in the younger group, we did not observe age-related differences in the incidence of pulmonary or neuromuscular diseases. Unfortunately, this finding is somewhat meaningless in terms of risk factor analysis for IUVFP as these comorbidities tend to naturally increase with advancing age. A further age-adjusted study is needed to confirm the significance of underlying nonstructural diseases.
Our study demonstrated a significantly higher likelihood that CT can be used to identify the unknown structural causes of IUVFP among older patients compared with younger patients. Thyroid mass was the most common etiology in patients in the younger and older groups and affected these groups at similar rates. In contrast, we more frequently detected a lung or mediastinal mass and aortic arch aneurysm in patients in the older group, and this finding is in line with the natural age-dependent prevalence of such diseases. Behkam et al 11 reported that aortic arch compliance and diameter change measured by thoracic imaging were significantly higher in patients with left-sided IUVFP than age- and sex-matched normal controls; accordingly, the authors suggested that parameters related to changes in aortic compliance should be evaluated as potential contributors to the onset of left-sided IUVFP, particularly in older patients. Williams et al 12 also tried to identify the relative influence of the properties of aorta in controlling the biomechanical milieu of the RLN and found an important role of aorta in controlling the RLN potentially in the onset of left-sided IUVFP. Overall, the most remarkable finding of our analysis was the significantly higher likelihood that CT can be used to detect structural causes compared to what was reported in previous studies.7,8,13 We attribute this result to the characteristics of our institution, wherein referrals from other hospitals are relatively frequently accompanied by existing CT scans that highlight noticeable structural problems. However, our findings may also introduce a counterargument to skeptical views regarding the necessity of CT scans for evaluating patients with IUVFP.
We further inspected the clinical courses of truly idiopathic patients with UVFP, including the rates of natural recovery and complications. However, we found no significant differences in those parameters between the 2 groups of patients. Laryngeal interventions, including immediate treatment, were relatively more frequent in the older group, although this difference was not statistically significant. However, this retrospective analysis is limited by the difficulty of making an accurate comparison of the degrees of natural recovery and complications given the uncontrolled and irregularly performed interventions, which were completed using diverse methods and administered at variable times during follow-up. We additionally searched for factors predictive of natural recovery and the need for early intervention in the 31 older patients with IUVFP. Although we used various analytical tools to identify these parameters from the patients’ clinical characteristics, we did not find any significant results. We attribute this to a limitation related to the retrospective study design. However, to date, no study has conducted factor analysis related to the aforementioned concerns or stated the importance of early intervention for the prevention of complications in patients with truly IUVFP. Hence, a well-designed, prospective, large population study of patients with IUVFP is warranted.
Conclusions
The diagnostic yield of CT scans performed to identify the structural causes of UVFP was significantly higher in older patients than their younger counterparts. Despite the higher incidence of structural abnormalities among older patients with IUVFP, the symptom degree, complication rate, and natural recovery rate did not significantly differ with respect to age. Furthermore, we did not identify clinical predictors of at-risk older patients with a poor likelihood of natural recovery and a high risk of complications. Further studies are needed to identify these patients as they would benefit from early laryngeal intervention.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Research Foundation of Korea (NRF) grant funded by the Korean government (MSIP) (2016R1C1B1014827).