
Abstract
Objectives:
Worldwide studies have shown an increasing trend of oropharyngeal squamous cell carcinoma (OPSCC) but a decreasing trend of oral cavity cancers over the past 2 decades, particularly in developed countries with successful tobacco control. This trend has been attributed to the increase in the incidence of human papillomavirus (HPV)–associated OPSCC. The aim of this study was to examine sex differences in incidence trends of oropharyngeal and oral cavity cancers in Hong Kong from 1983 to 2014.
Methods:
Using data from the Hong Kong Cancer Registry from 1983 to 2014, age-standardized incidence rates for potentially HPV-associated sites (oropharyngeal) and non-HPV-associated sites (oral cavity) were calculated, stratified by sex and age groups. Joinpoint regression and an age-period-cohort model were used to assess incidence trends.
Results:
A total of 1,972 cases of oropharyngeal cancer and 7,389 cases of oral cavity cancer were diagnosed from 1983 to 2014. The male/female ratios were 4.16:1 for oropharyngeal cancers and 1.63:1 for oral cavity cancers. A significant increasing trend was observed in oropharyngeal cancers from 1994 to 2014 (average annual percentage change = 2.66, P < .05). In contrast, a significant decreasing trend was observed in oral cavity cancers from 1983 to 1994 (average annual percentage change = −5.36, P < .05). The trends were more significant in men and in patients aged 45 to 69 years. A positive birth cohort effect was observed for oropharyngeal cancer in men.
Conclusions:
The rising trend of oropharyngeal cancer and decreasing trend of oral cavity cancer in Hong Kong from 1983 to 2014 are consistent with worldwide trends. Increase in high-risk sexual behaviors and oral HPV infection may influence the difference in trends.
Introduction
Head and neck cancers include tumors at various anatomic sites with different etiologic factors. They can be divided into those affecting the oral cavity (including the lip and tongue), oropharynx (tonsils and posterior pharynx), and other sites (eg, larynx, nasopharynx, and other unspecific sites). In the United States in 2016, it was estimated that approximately 48,330 Americans would develop head and neck cancers and that 9,570 would die from the disease. 1 Smoking and alcohol consumption are known risk factors for head and neck cancers. 2 Betel quid use is another important etiologic factor in populations in which the habit is common (eg, India, Taiwan). 3 Histologically, more than 95% are squamous cell carcinoma. 2 Among these, oropharyngeal carcinoma is a distinct clinical entity that occurs in posterior pharyngeal wall, soft palate, tonsillar region, or posterior third of the tongue or Waldeyer’s ring (International Classification of Diseases, Tenth Revision [ICD-10], codes C01, C02.4, C05.1-C05.2 C09-C10, and C14.2). Trends in head and neck cancer rates differ among subtypes, countries, and sex. There are increasing trends of oral cavity and oropharyngeal cancers in a number of European countries and some Asian countries. However, in countries with successful tobacco control (eg, Canada, the United States), an increasing trend of oropharyngeal cancers was observed in the past 2 decades, particularly in oropharyngeal squamous cell carcinoma (OPSCC), despite a decrease in oral cavity cancers.4,5
Human papillomavirus (HPV) infection and changing sexual behaviors in Western countries are believed to contribute to the rise of OPSCC incidence. 6 These HPV-positive tumors are different from HPV-negative tumors in terms of clinical presentation, behaviors, treatment response, and prognosis. HPV-positive tumors are observed more in white men, younger than 50 years of age, with no histories of alcohol and tobacco use. They are more responsive to chemotherapy and radiation. HPV-positive tumors are associated with better overall survival and disease-specific survival. 7 The basal layer of the epithelium of the tonsillar crypts provides an easy route of invasion for the virus, with the majority of HPV-positive tumors in the oropharynx and tonsils. 8 In the United States, there is an increasing trend in the incidence rate of HPV-positive OPSCC (from 0.8 per 100,000 in 1988 to 2.6 per 100,000 in 2004). 9 In Hong Kong and the southern Chinese populations, about 20% to 30% of oropharyngeal carcinomas are associated with HPV infection.10,11
Studies of the incidence trend of oropharyngeal carcinoma in the Asian population are limited. A study in Taiwan demonstrated increased incidence of oropharyngeal carcinoma from 1981 to 2000. 12 Studies of the incidence trend of oropharyngeal carcinoma in Hong Kong are lacking. Only 1 study in Hong Kong analyzed the trend of oral cavity cancers over the past 25 years, but some of the anatomic sites for oropharyngeal cancers were grouped together with oral cavity cancers. 13 For the above reasons, the incidence of HPV infection and HPV-related oropharyngeal cancers is expected to rise. The aim of this study was to explore the sex differences in the temporal trend of the incidence rates of oropharyngeal cancers and oral cavity cancers in Hong Kong’s general population. We also used age-period-cohort modeling to assess the independent effects of age, time period, and birth cohort on incidence trends of both types of cancers. Age effects reflect the consequences of growing older; period effects reflect the factors that influence all age groups simultaneously, such as implementation of a screening program; and cohort effects reflect changes in lifestyle or other environmental exposures.
Methods
Source of Data and Case Definition
Using data from the Hong Kong Cancer Registry, all newly diagnosed oropharyngeal cancer cases from 1983 to 2014 were recruited. All cases diagnosed within the period were identified according to sex (male or female) and diagnosed year (in 5-year intervals: 0-4, 5-9, . . . , 80-84, and ⩾85 years). Cases were recruited according to the ICD-10 classification. 14 Cases were classified into potentially HPV-associated subsites (oropharyngeal) and non-HPV-associated subsites (oral cavity). The ICD-10 codes for oropharyngeal cancers were as follows: malignant neoplasms of base of tongue (C01), lingual tonsil (C02.4), soft palate (C05.1), uvula (C05.2), tonsil and oropharynx (C09-C10), and other ill-defined sites in the lip, oral cavity, and pharynx (C14). ICD-10 code C14 includes malignant neoplasms of unspecified sites of the pharynx (C14.0), Waldeyer’s ring (C14.2), and other overlapping lesions of the lip, oral cavity, and pharynx (C14.8). Because oropharyngeal cancers more commonly presented at more advanced clinical stages, precise identification of the site of origin in clinical settings for oropharyngeal cancers was more difficult than for oral cavity cancers. Specific incidence data about ICD-10 code C14.2, a subset of oropharyngeal cancers, were not available from the Hong Kong Cancer Registry. For the above reasons, we decided to include ICD-10 code C14 as part of oropharyngeal cancers. The ICD-10 codes for oral cavity cancers were as follows malignant neoplasms of other and unspecified parts of tongue (C02), gum, floor of the mouth, palate, and other unspecified parts of the mouth (C03-C06). Cancers of the lips, nasopharynx, salivary gland, and hypopharynx were excluded from our analysis.
Statistical Analysis
Crude incidence rates (per 100,000 population at risk) in each calendar year were calculated as count divided by population for each sex in each age group. Age-standardized annual incidence rates were calculated using the direct method for age adjustment, according to the World Health Organization’s 2000 World Standard Population. Joinpoint regression analyses were performed to identify changing points of incidence trends. The average annual percentage changes (AAPCs) of incidence for different age groups and for each gender were calculated. P values < .05 were considered to indicate statistical significance. The joinpoint program used was Joinpoint Regression Program version 4.4.0.0 (National Cancer Institute). 15
Statistical analysis using age-period-cohort regression for each gender was also performed. The effects of age, period, and cohort on the incidence of both cancers were analyzed using an age-period-cohort modeling method developed by Rutherford et al. 16 R version 3.1.1 was used for trend analysis (Epi package version 1.1.67).
Results
A total of 1,972 cases of oropharyngeal cancer were diagnosed from 1983 to 2014, while there were 7,389 cases of oral cavity cancer. Cases in men accounted for 80.6% (1,590 cases) of oropharyngeal cancer and 62.0% (4,581 cases) of oral cavity cancer, respectively. The male/female ratios were 4.16:1 for oropharyngeal cancers and 1.63:1 for oral cavity cancers. The overall age-standardized incidence rates for oropharyngeal cancer increased from 0.93 per 100,000 in 1983 to 1.15 per 100,000 in 2014, while the age-standardized incidence for oral cavity cancer decreased from 2.26 per 100,000 in 1983 to 1.49 per 100,000 in 2014. Supplementary Table 1 shows the age-specific incidences of oropharyngeal and oral cavity cancers.
Figures 1a and 2a show the overall joinpoint analysis results for both oropharyngeal and oral cavity cancers. Both types of cancers showed an initial decreasing trend. The AAPC of oropharyngeal cancers was −5.36% per year from 1983 to 1994 (P < .05; 95% confidence interval, –9.0% to −1.6%) and −2.04% per year from 1983 to 2002 (P < .05; 95% confidence interval, −2.9% to −1.2%) for oral cavity cancers. After 1994, a significant increasing trend was observed in oropharyngeal cancer incidence, with an AAPC of 2.66% per year (P < .05; 95% confidence interval, 1.3% to 4.0%). There was a slightly rising trend for oral cavity cancers of 0.95% per year, but the change was insignificant (P > .05; 95% confidence interval, −0.6% to 2.5%).
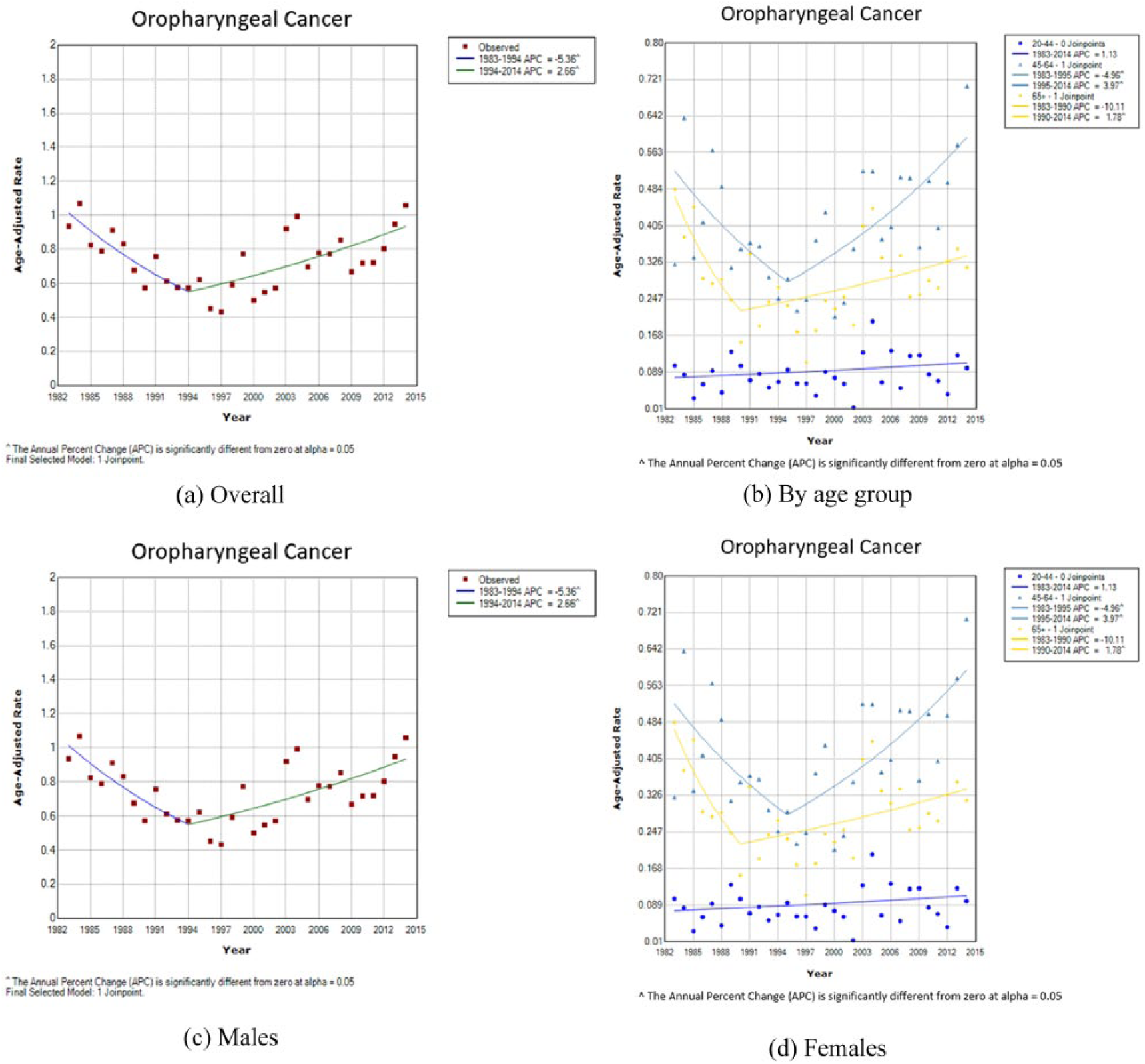
Incidence trend of oropharyngeal cancers among Hong Kong population, 1983 to 2014.
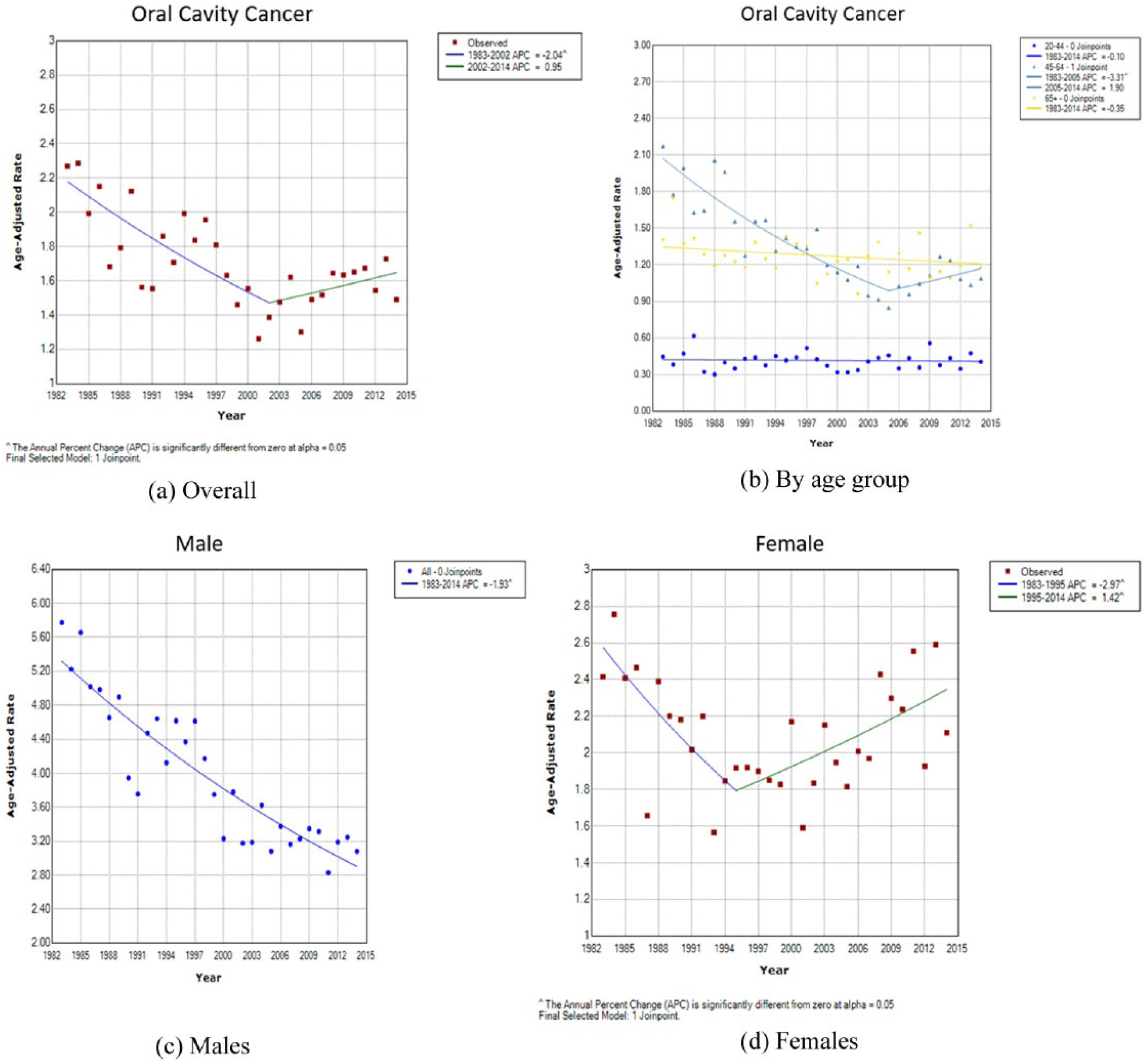
Incidence trend of oral cavity cancers among Hong Kong population, 1983 to 2014.
When the data were stratified by sex, similar biphasic trends were observed in oropharyngeal cancers for both men and women. The AAPCs for men were −6.38% per year from 1983 to 1993 and 3.36% per year from 1993 to 2014 (P < .05); for women, AAPCs were −6.03% per year from 1983 to 1996 and 3.41% from 1996 to 2014 (P < .05) (Figures 1c and 1d). In oral cavity cancers, we observed a different trend for each sex. For men, there was a significant decreasing trend for oral cavity cancers from 1983 to 2014, with an AAPC of −1.93% per year (P < .05; 95% confidence interval, −2.3% to −1.6%). For women, a biphasic trend was observed, with AAPCs of −2.97% per year from 1983 to 1995 (P < .05) and 1.42% per year from 1995 to 2014 (P < .05) (Figures 2c and 2d). Supplementary Table 1 summarizes the joinpoint analysis results for oropharyngeal and oral cavity cancers, stratified by sex.
We also studied the incidence trends of both cancers by different age groups. We observed the most significant change in trends occurred among patients aged 45 to 64 years for both cancers (Figures 1b and 2b). For oropharyngeal cancer, a steeper increase in trend was observed among those aged 45 to 64 years (AAPC = 3.97% from 1995 to 2014) than those aged ⩾65 years (AAPC = 1.78% from 1990 to 2014). For oral cavity cancer, incidence gradually decreased among patients aged ⩾65 years (AAPC = −0.35% from 1983 to 2014), but the decreasing trend was more obvious among those aged 45 to 64 years (AAPC = −3.31% from 1983 to 2005).
Results of the goodness-of-fit analysis for the models of age, period, and cohort are summarized in Supplementary Table 2. The full age-period-cohort model provided the best fit for both oropharyngeal and oral cavity cancers. Figure 3 shows the age-period-cohort analysis for overall oropharyngeal cancers and oral cavity cancers among the Hong Kong population. A strong negative birth cohort effect was observed for oral cavity cancers (rate ratio declined from 1.20 in the 1923 birth cohort to 0.64 in the 1990 birth cohort) (Figure 3, middle), while no obvious birth cohort effect was observed for oropharyngeal cancers. When stratified by sex, a positive cohort effect was observed among men for oropharyngeal cancer (0.80 in the 1896 birth cohort and 1.66 in the 1990 birth cohort), and a negative cohort effect was observed among women for oropharyngeal cancers (rate ratio declined from 1.55 in the 1896 birth cohort to 0.32 in the 1990 birth cohort) (Figure 4, oropharyngeal cancer, middle). For oral cavity cancers, a negative cohort effect was observed among men (rate ratio declined from 1.70 in the 1896 birth cohort to 0.62 in the 1990 birth cohort) but not in women (Figure 4, oral cavity cancer, middle). No significant period effects were observed for both types of cancers in both sexes. The results are illustrated in Figure 4.
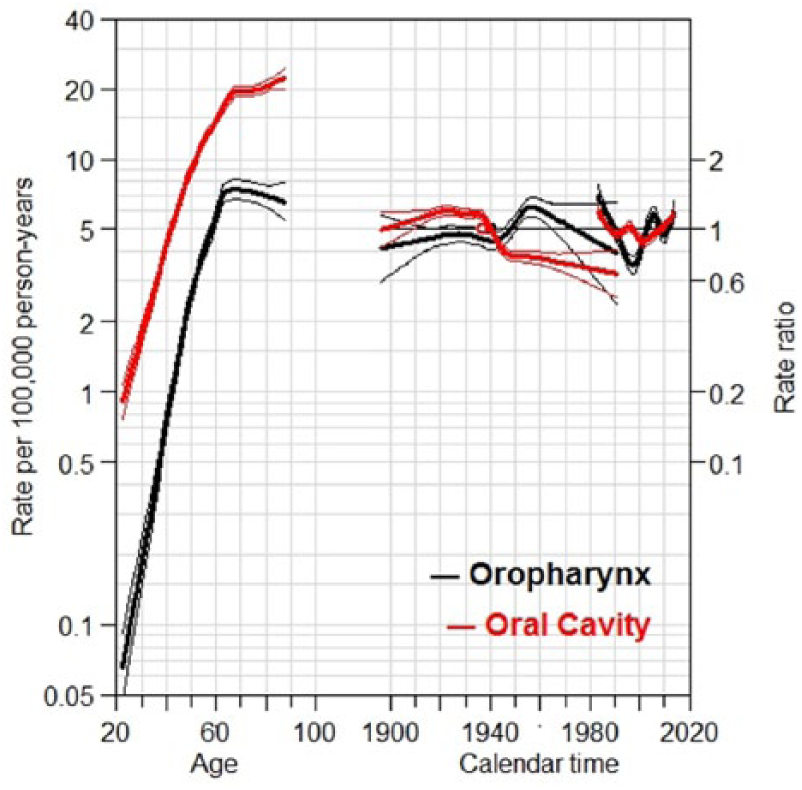
Age-period-cohort effect analysis of overall oropharyngeal and oral cavity cancers in Hong Kong. Curves (red and black) on the left show age-specific incidences (rate per 100,000 person-years), curves in the middle show cohort effects (rate ratio), and curves on the right showed period effects (rate ratio).
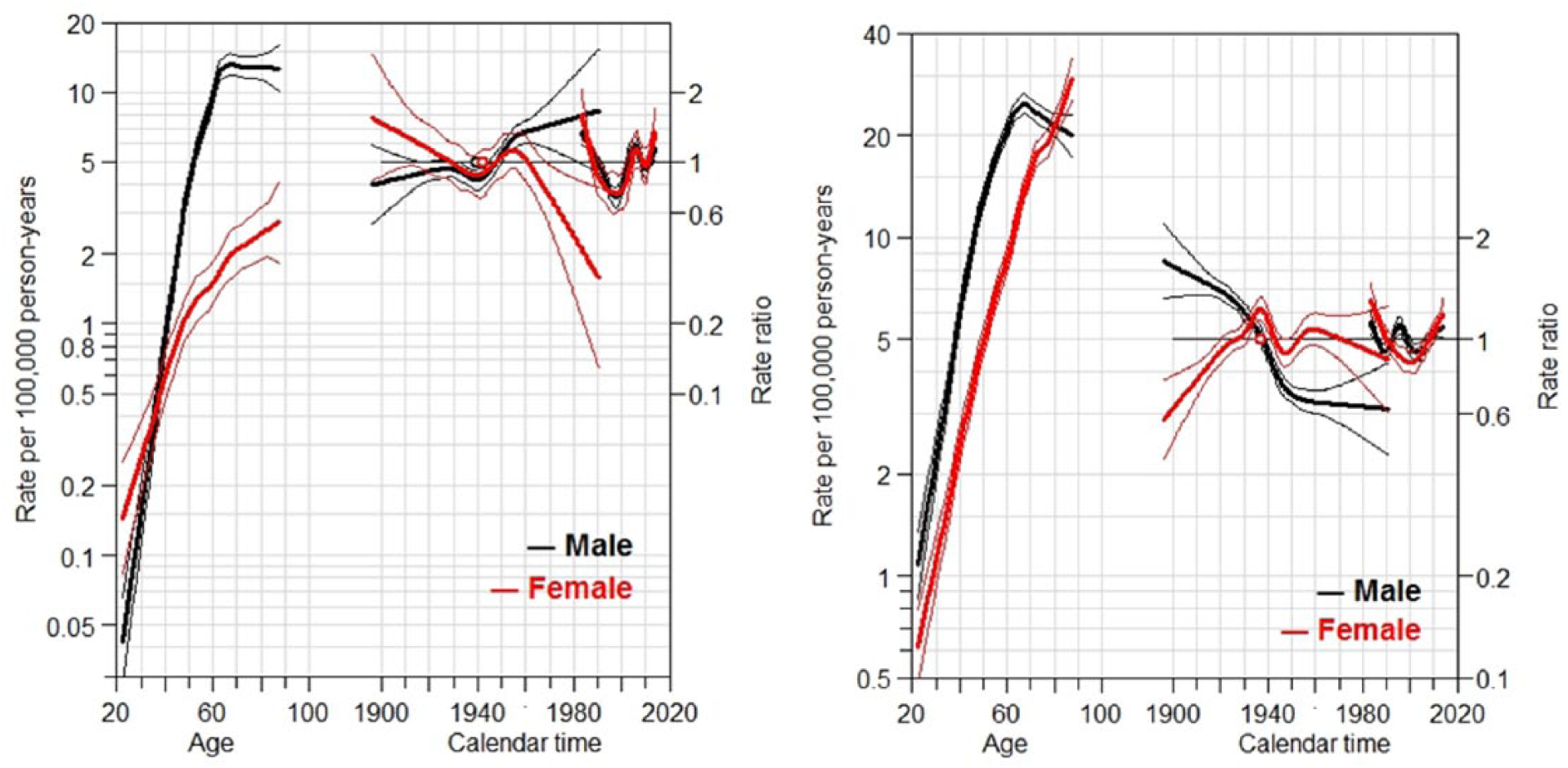
Age-period-cohort effect analysis of oropharyngeal and oral cavity cancers in Hong Kong, stratified by sex. Curves (red and black) on the left side show age-specific incidences (rate per 100,000 person-years), curves in the middle show cohort effects (rate ratio), and curves on the right side show period effects (rate ratio). Left: oropharyngeal cancer; right: oral cavity cancer.
Discussions
This study provides a population-based observation of the temporal trends of potentially HPV-associated and non-HPV-associated cancers in Hong Kong. Incidence rates of HPV-associated cancer (oropharyngeal) showed a significant increasing trend over the past 2 decades, while those of non-HPV-associated cancer (oral cavity) showed a decreasing trend. The incidence rates for both types of cancers were higher among men than women. The incidence of oropharyngeal cancers had a larger increase in younger population (those aged 45-64 years). These results are consistent with epidemiologic trends reported in the United States.5,17-19
For HPV-associated cancers, the incidence has been observed to increase in various developed countries and some Asian countries. In the United States, data from Surveillance, Epidemiology, and End Results program registries revealed an increase in HPV-associated cancer from 1973 to 2004 (AAPC = 0.80%). 20 A similar trend was also observed in Canada (AAPC = 2.7%, 1992-2009), Australia (AAPC = 1.2%, 1982-2008), Korea (AAPC = 2.35%, 1999-2009), and Singapore (AAPC = 1.9% for men and 2.0% for women, 1993-2012).21-24 In our study, we reported an AAPC of 2.66% from 1994 to 2014.
For non-HPV-associated cancers, decreasing trends were reported in various countries in the literature, including Canada, Australia, and Singapore. Our study showed an overall decreasing trend for non-HPV-associated cancer. Interestingly, a similar overall decreasing trend was also observed for HPV-associated cancer sites from 1983 to 1994. This may be contributed by a decline in traditional risk factors that are common to both types of cancers, such as smoking and alcohol consumption. With the enactment of a smoking (public health) ordinance in 1982, the prevalence of daily smokers aged 15 and above decreased from 23.3% in 1982 to 10.5% in 2013. 25 The decrease was more obvious among the male population (from 39.7% to 18.6%) than the female population (from 5.6% to 3.2%). Per capita alcohol consumption remained static between 2.53 and 2.87 L from 2004 to 2015. 26 The change in smoking prevalence may partly explain the decreasing trend of oral cavity cancers, particularly among men. APC analysis results were consistent with the above findings, with a negative birth cohort effect in overall oral cavity cancer incidence and in men with oral cavity cancers.
A significant increase in incidence trend of oral cavity cancers among women since 1995 was observed in our study (Figure 2d). APC analysis showed no significant cohort effect or period effect among women with oral cavity cancers. We were unable to identify potential factors that may account for the observed trend in this study. The relatively static smoking prevalence among the female population compared with the male population may contribute partly to the trend. Other exposure data, such as the proportion of heavy smokers (20 or more cigarettes per day) among female smokers, dental hygiene, and habit of spicy food intake, must be considered to understand the increasing trend of oral cavity cancers among women.
Our data showed no significant period effects for both types of cancers within the study period. Hong Kong is a developed country with a well-developed medical system. The completeness and quality of the data collected by the Hong Kong Cancer Registry after 1983 has been reported to be good. 27 Accessibility of medical assessment, imaging, and treatment did not change significantly over time. Methods of diagnosis, including clinical assessments, biopsy, and radiologic investigations with computed tomography and magnetic resonance imaging, were similar for both types of cancers and may not have had a large influence on the observed trends.
APC analysis showed a difference in birth cohort effect on the incidence trend for oropharyngeal cancers among men and women. A positive birth cohort effect was observed among men, and a negative effect was observed among women. We propose the effect of increased HPV exposure as a possible explanation for the difference in cohort effects we observed. With improved general socioeconomic status in the 1980s and the influence of Western countries, an increase in high-risk sexual behavior was observed among Hong Kong adolescents and students. 28 According to the Youth Sexuality Survey of the Family Planning Association of Hong Kong, unmarried youth held more liberal attitudes toward high-risk sexual behaviors. These include increase acceptance of premarital sex, increase number of sex partners, and premarital pregnancy. The prevalence of premarital sex increased from 35.1% in 1996 to 44% in 2006 among unmarried men and from 27.5% in 1996 to 31.0% among unmarried women. 29 An increased trend of homosexual contact, or men having sex with men, was also observed, as evident by a rising number of reported human immunodeficiency virus infections acquired through men having sex with men in recent years (from 30 cases in 1995 to 96 cases in 2005). 30 All these high-risk sexual behaviors are predictors of oral HPV infection. 31 Our observed increasing trend of oropharyngeal cancers in 1990s, particularly among younger men, is consistent with the change in sexual behavior.
There were limitations to our study. First, the data reported to the Hong Kong Cancer Registry were based on judgments by reporting surgeons of individual institutions. Because these sites were closely related to one another, and advanced diseases usually involve multiple sites, there was potential misclassification of data into different ICD-10 subsets. Because of the retrospective nature of this study, accurate classification of every case according to clinical and radiologil assessments was not possible.
Second, we did not classify the data according to different histologies. However, on the basis of previous studies finding that more than 90% of cancers of the head and neck regions were squamous cell carcinoma, 2 our study provides a reasonable estimate of incidence trends in these cancers.
Third, our classification of oropharyngeal and oral cavity cancer subsides as potentially HPV-associated and non-HPV-associated were based on previous epidemiologic studies worldwide. Studies on true HPV prevalence in head and neck cancers with HPV DNA analysis are lacking in Hong Kong. A study using HPV messenger RNA expression to identify individual tumor HPV status reported an incidence of HPV-related oropharyngeal SCC of 0.12 per 100,000 from 2005 to 2009. 11 A lack of studies on oral HPV prevalence trend in Hong Kong also limits our interpretation of the change in oropharyngeal cancer trend. Further research in these areas is needed to provide more evidence in explaining our observed changes in incidence trends.
Conclusions
We observed an increasing trend of incidence of cancers in potentially HPV-associated subsites and a decreasing trend of potentially non-HPV-associated subsites in Hong Kong from 1983 to 2014. The change was consistent with worldwide epidemiologic studies. Decreasing smoking prevalence may explain the decreasing oral cavity cancer incidence among men. A difference in birth cohort effect was observed for oropharyngeal cancers among men and women, which may be due to the change in sexual behavior and increased risk for HPV infection. Further studies on the prevalence of oral HPV infection among the general population and patients with oropharyngeal cancers are needed to provide more evidence to explain the changing incidence pattern.
Supplemental Material
Supplementary_TablesSupplementary_table_1_Incidence_rates_and_Jointpoint_analysis_results_for_Oropharyngeal_and_Oral_Cavity_cancers_from_1983_to_2014 – Supplemental material for Sex Differences in Time Trends on Incidence Rates of Oropharyngeal and Oral Cavity Cancers in Hong Kong
Supplemental material, Supplementary_TablesSupplementary_table_1_Incidence_rates_and_Jointpoint_analysis_results_for_Oropharyngeal_and_Oral_Cavity_cancers_from_1983_to_2014 for Sex Differences in Time Trends on Incidence Rates of Oropharyngeal and Oral Cavity Cancers in Hong Kong by Man Hin Chan, Feng Wang, Oscar Mang-kong Mang and Lap Ah Tse in Annals of Otology, Rhinology & Laryngology
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental Material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.