
Abstract
Objectives:
The aim of this study was to elucidate the utility of the Kano method with surgical closure of the larynx by cricoid cartilage removal in improving quality of life in patients with severe dysphagia and their caregivers.
Methods:
Nine patients with severe dysphagia who underwent the Kano method were evaluated for oral intake and activities of daily living using the functional oral intake scale and the Barthel index, respectively, as indices of quality of life. Additionally, nutritional status, inflammation, and postoperative complications were assessed. Furthermore, 7 family caregivers were queried regarding frequency of sputum suction, mood of family caregivers, and postoperative satisfaction.
Results:
Functional oral intake scale and Barthel index scores as well as inflammation improved significantly after surgery (P < .05). There were no severe complications or other complications requiring surgical intervention. The frequency of sputum suction was reduced postoperatively (P < .05). The mood of family caregivers was significantly improved and satisfaction level was high postoperatively.
Conclusions:
Surgical closure of the larynx is an appropriate choice for patients with irreversible severe dysphagia and impaired articulation or vocal function because quality of life is improved for both patients and family caregivers and the satisfaction of family caregivers is sufficient.
Keywords
Introduction
Japan currently has a super-aged society. This occurs when 21% (or greater) of a country’s population is aged ⩾65 years. In Japan, 26% of the population is currently ⩾65 years of age; thus, the number of individuals with age-related diseases and disorders resulting in swallowing disorders or dysphagia is also increasing. In 2012, pneumonia became the third leading cause of death in Japan (9.9%), replacing cerebrovascular disease, which reflected the increased prevalence of aspiration pneumonia. The proportion of aspiration pneumonia accounts for 70% in patients in their 70s and 80% in patients in their 80s among those hospitalized with pneumonia, and aspiration pneumonia accounts for the majority with age. 1 Managing dysphagia in elderly patients has become an urgent medical and social issue for otolaryngologists in Japan.
In patients with intractable severe dysphagia due to neurodegenerative or cerebrovascular disease, artificial hydration and nutrition (AHN) including gastrostomy is preferred. However, AHN cannot prevent aspiration pneumonia caused by saliva or gastroesophageal reflux, and patients experience chronic lower respiratory tract infection and frequent tracheal suction. As a result, the quality of life (QOL) of these patients gradually worsens despite AHN. In addition, the presence of severe dysphagia in people receiving home care, who require constant tracheal suction and frequent oral care, is a considerable burden for family caregivers.
A clear approach to prevent aspiration in patients with severe dysphagia is surgical therapy for intractable aspiration to separate the airway and esophagus. Conventional surgical therapies for intractable aspiration, such as laryngotracheal separation 2 or laryngeal closure, 3 are restricted to certain individuals, such as children with severe developmental disabilities, because of resistance to the loss of voice and high risk for postoperative complications, such as severe infection or fistula formation. However, several minimally invasive surgical approaches that prevent aspiration with fewer complications have been introduced to alleviate severe deterioration of the general condition of patients with dysphagia.4-7 The Kano method, surgical closure of the larynx with cricoid cartilage removal, which was developed by Kano et al, 7 has been rapidly adopted as a minimally invasive method that secures tracheal cannula–free status. There are few studies of patient QOL or caregiver burden associated with severe dysphagia in patients who undergo surgical intervention using the Kano method. Therefore, we conducted a retrospective chart review to compare these factors before and after surgery to elucidate the utility of the Kano method.
Methods
The institutional review boards of Tokyo Metropolitan Geriatric Hospital and Tokyo Medical and Dental University approved this study. All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards. Written informed consent was obtained from all patients or their family caregivers.
Subjects
Subjects in this study included 9 patients with diagnoses of intractable dysphagia and repeated episodes of aspiration pneumonia requiring frequent suctioning and underwent surgical closure of the larynx using the Kano method. All subjects were patients observed in the Department of Otolaryngology at Tokyo Metropolitan Geriatric Hospital and in the Department of Head and Neck Surgery at Tokyo Medical and Dental University from November 2011 to October 2013. The study cohort included 6 men and 3 women, with an age range of 63 to 84 years (mean, 73.9 years). Causes of dysphagia were cerebrovascular disease (n = 3), multiple system atrophy (n = 2), multiple inferior cerebral nerve palsy caused by metastatic retropharyngeal lymph nodes of oropharyngeal carcinoma (n = 1), left recurrent nerve palsy after thoracic aortic aneurysm surgery (n = 1), concomitant bilateral recurrent nerve palsy with tracheostomy due to thyroid cancer and Parkinson’s disease (n = 1), and cortical basal degeneration (n = 1). All patients had percutaneous endoscopic gastrostomy (PEG) and were unable to receive oral feeding.
Only 1 patient with multiple inferior cerebral nerve palsy caused by metastatic retropharyngeal lymph nodes of oropharyngeal carcinoma could vocalize, with severe breathy hoarseness. The remaining patients could not communicate through speech, because of severe dysarthria, aphasia, or requirement for mechanical ventilation. Written consent was obtained from 1 patient, whereas alternative or nonverbal means of communication were used to inform the other patients and gain their consent. Families also provided consent in all cases.
Surgical Closure of the Larynx: The Kano Method
Surgical closure of the larynx was performed as described by Kano et al, 7 conducted under either local or general anesthesia. A reverse-T skin incision on the anterior neck was made from the superior thyroid notch to the inferior border of the cricoid cartilage. Strap muscles were gently divided along the midline to the side, and bilateral cricothyroid muscles were dissected from the anterior wall of the cricoid cartilage. Next, bilateral cricopharyngeus muscles were separated from the cricoid cartilage to improve swallowing by releasing the upper esophageal sphincter. Central parts of the thyroid and cricoid cartilage were removed, preserving the perichondrium in the laryngeal side (Figure 1A). After a transverse incision was made on the membrane between the cricoid cartilage and the first tracheal ring, with insertion of a J-shaped tracheostomy tube in patients under general anesthesia, the laryngeal lumen was opened from the first tracheal ring to the superior thyroid notch with a vertical midline mucosal incision (Figure 1B). A horizontal incision was made along the mucosa of bilateral vocal folds, including the interarytenoid fold at the level of the free edge. Next, bilateral thyroarytenoid muscles and arytenoid cartilages were dissected to create superior and inferior flaps (Figure 1C). Both sides of the upper and lower vocal fold flaps were sutured with absorbable sutures (Figure 1D). A better conditioned sternohyoid muscle was isolated, preserving vessels as much as possible, and was cut at the sternum side. The divided muscle pedicle was inserted between the superior and inferior flaps to fill the dead space and anchored to the posterior commissure (Figure 1E). Excess cricothyroid membrane was trimmed, and tracheostomaplasty was performed to shape the stoma into a triangle, the base of which was the upper rim of the first trachea and the top the anterior end of the inferior vocal flap. Finally, the wound above the tracheostomy was closed with a drainage tube.
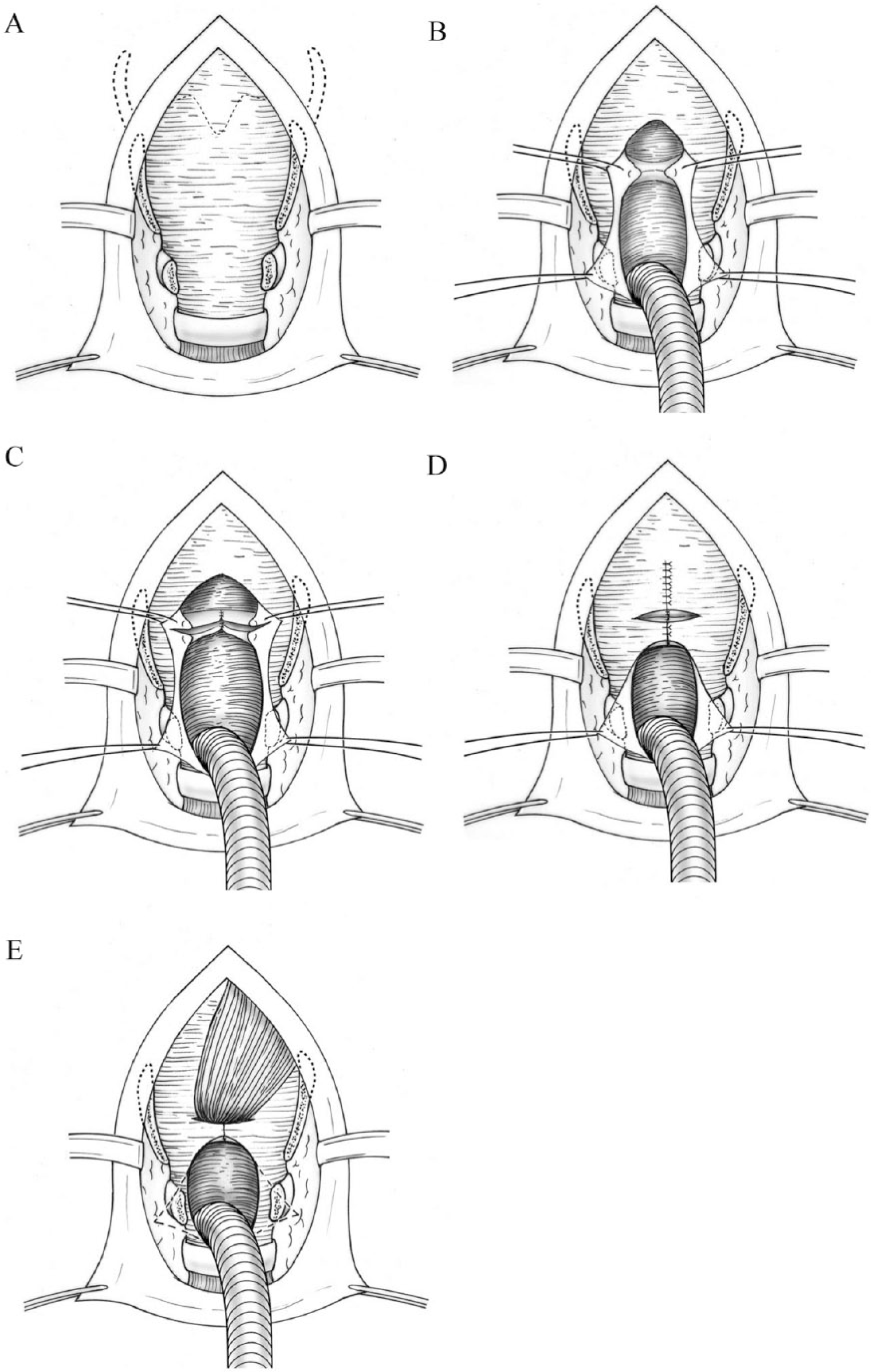
The Kano method for surgical closure of the larynx. (A) Central parts of the thyroid and cricoid cartilages are removed, preserving the perichondrium. (B) The laryngeal lumen is opened from the first tracheal ring to the superior thyroid notch through a vertical midline mucosal incision. (C) Bilateral thyroarytenoid muscles and arytenoid cartilage are dissected to create superior and inferior flaps. (D) Both sides of the upper and lower vocal fold flaps are sutured with absorbable sutures. (E) The divided muscle pedicle is inserted between the superior and inferior flaps to fill the dead space and anchored to the posterior commissure.
Postoperative Management
After the absence of leaks was confirmed by videoendoscopy using colored water or videofluorography 1 week after the operation, oral feeding was initiated, first with clear water and then a liquid diet. To reacquire oral intake after surgery, it is necessary to use the remaining oral functions. Because aspiration disappears and the food transfer pathway becomes like a single pipe, liquid is the most favorable dietary form for swallowing, even in the oral and pharyngeal phase.
Surgical Outcomes
Outcomes of surgical closure of the larynx were assessed via comparisons between pre- and postoperative status regarding eating abilities using the functional oral intake scale (FOIS) 8 and activities of daily living using the Barthel index. 9 The FOIS is a 7-point ordinal scale on which the highest value indicates normal swallowing ability and the lowest indicates the need for a feeding tube without any oral intake. The Barthel index includes 10 scored items using a 5-point scale (full score, 100) and was used to collect information regarding the need for assistance in performing activities of daily living and to establish a degree of independence.Scores for both instruments were derived from the data documented in the patient’s medical chart. We also assessed nutritional status as determined by serum albumin (grams per deciliter), peripheral lymphocyte count (per microliter), and the inflammatory marker C-reactive protein (CRP; milligrams per deciliter), as these factors reflect disruption of the general condition mainly by inflammation of the lower respiratory tract and nutritional disorders in patients with intractable severe dysphagia. Blood tests were performed within 1 month before surgery and repeated 3 to 4 weeks after surgery. Postoperative complications were evaluated as well.
Additionally, questionnaires were sent to 7 family members who could be contacted by telephone at the time of the survey. The remaining 2 families could not be contacted by telephone. The questionnaires compared pre- and postoperative status for parameters such as the residential style of the patient; the daily frequency of sputum suction; the Japanese version of the Zarit Caregiver Burden Interview, which comprehensively targets emotional and physical health, social life, and financial status (full score, 88) 10 ; and mood of family caregivers using a face scale (Figure 2). The questionnaires also ascertained overall level of satisfaction with the surgery on a visual analog scale (VAS) ranging from 0 (dissatisfied) to 100 (satisfied). Suction frequency was assessed as follows: 1 = a few times per day, 2 = once every 2 to 3 hours, 3 = once or twice per hour, and 4 = at least 3 times per hour.

Face scale for assessment of the mood of family caregivers before and after surgery.
Statistical Analysis
All analyses were performed using Statcel 3 (OMS, Tokorozawa, Saitama, Japan). The Barthel index, frequency of suction, Japanese version of the Zarit Caregiver Burden Interview, mood of family caregivers, and overall level of satisfaction with the surgery were analyzed using the Wilcoxon rank sum test. Serum albumin levels, peripheral blood total lymphocyte counts, and CRP levels were statistically examined using the Student paired t test. P values < .05 (2 tailed) were considered to indicate statistical significance.
Results
Postoperative Oral Intake Level
Pre- and postoperative FOIS scores are shown in Figure 3. All 9 patients were incapable of oral intake and had complete dependence on gastrostomy. After surgery, all patients underwent swallowing training by speech therapists and were monitored for proper diet for approximately 1 month. Eight patients exhibited improvement by FOIS score, 5 of whom did not require AHN, because they could ingest orally. The difference between the pre- and postoperative FOIS scores was statistically significant (P = .011).
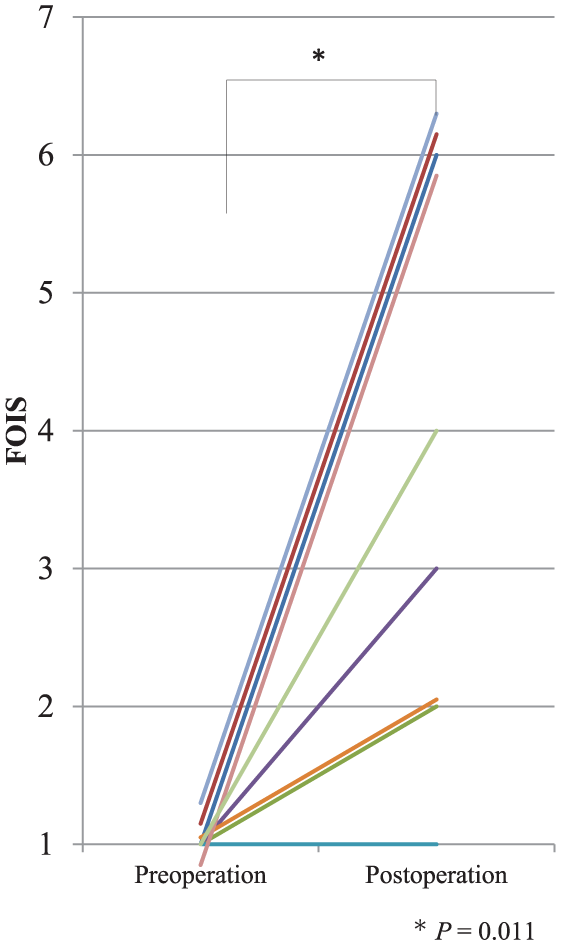
Functional oral intake scale (FOIS) scores before and after surgery. All 9 patients were incapable of oral intake, with percutaneous endoscopic gastrostomy. After surgery, 5 patients could ingest orally, which allowed them to withdraw from artificial hydration and nutrition. The difference between the pre- and postoperative FOIS scores was statistically significant (P = .011).
Activities of Daily Living
Pre- and postoperative Barthel index scores are shown in Figure 4. Eight patients had already lost vocal communication ability, and vocal communication was extremely limited in 1 patient with a metastatic skull base tumor because of vagus nerve palsy. The postoperative index was improved in 6 patients, and the difference between pre- and postoperative Barthel index scores was statistically significant (P = .028).
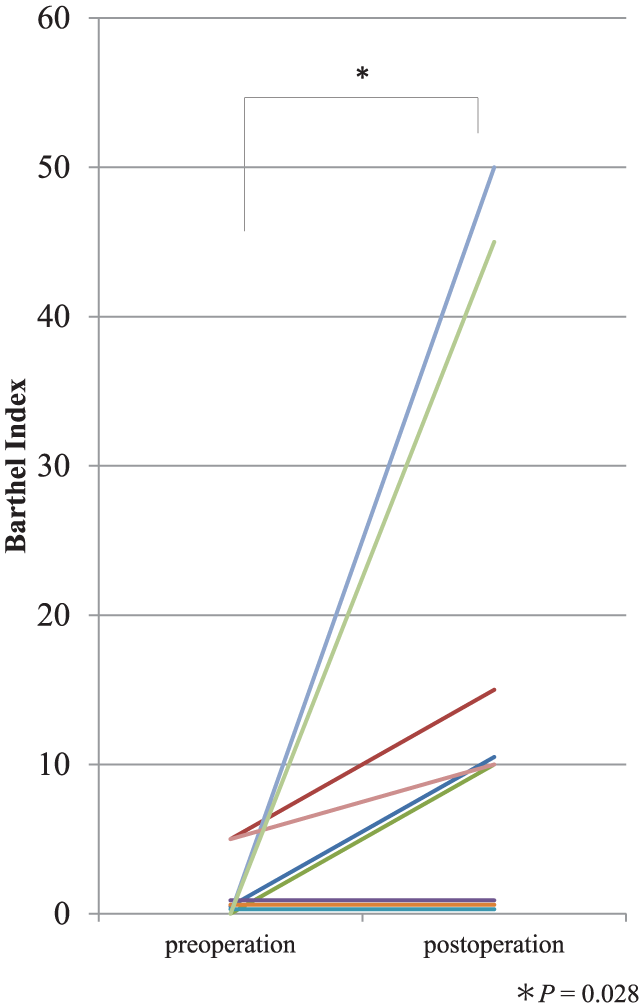
Barthel index scores before and after surgery. Postoperative independence was improved in 6 patients. The difference between pre- and postoperative Barthel index scores was statistically significant (P = .028).
Nutritional Assessment
The average pre- and postoperative serum albumin levels were 2.96 and 3.10 g/dL, respectively (P = .14), whereas the average pre- and postoperative peripheral lymphocyte counts were 1269/µL and 1580/µL, respectively (P = .054) (Table 1).
Clinical Data of the Patients Before and After Surgery. a
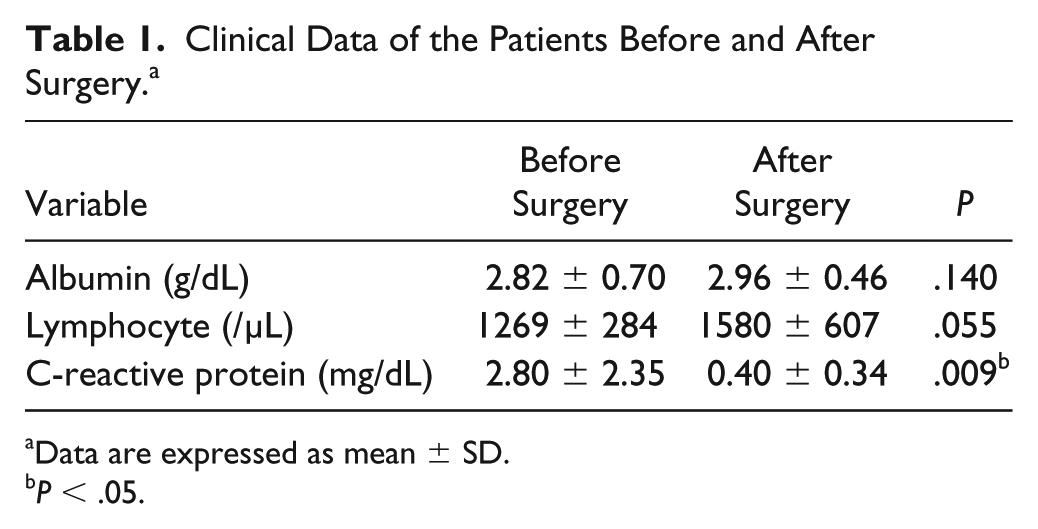
Data are expressed as mean ± SD.
P < .05.
Inflammation
The average CRP level, which was 2.80 g/dL preoperatively, was significantly lower postoperatively at 0.40 g/dL (P = .009; Table 1).
Postoperative Complications
Among the study cohort of 9 patients, only 1 postoperative complication was observed in 1 patient who developed a small subcutaneous abscess that was cured by local treatment. There were no severe complications or other complications requiring surgical intervention. The large tracheostomies enabled all patients to avoid tracheal cannula placement.
Residential Style of the Patients
Among the 7 patients whose family members responded to the questionnaire, 3 patients preoperatively received home care, 3 patients were in special nursing homes, and 1 patient was hospitalized. After surgery, 3 other patients, in addition to the 3 already receiving home health care, were sent for home care, whereas the patient whose wife was his primary caregiver and was too old and frail to administer to him was transferred to a sanatorium-type medical facility for elderly patients requiring long-term care.
Suction Frequency
The average suction score was 2.14 preoperatively, which was significantly reduced to 1.14 postoperatively (P = .001; Figure 5).
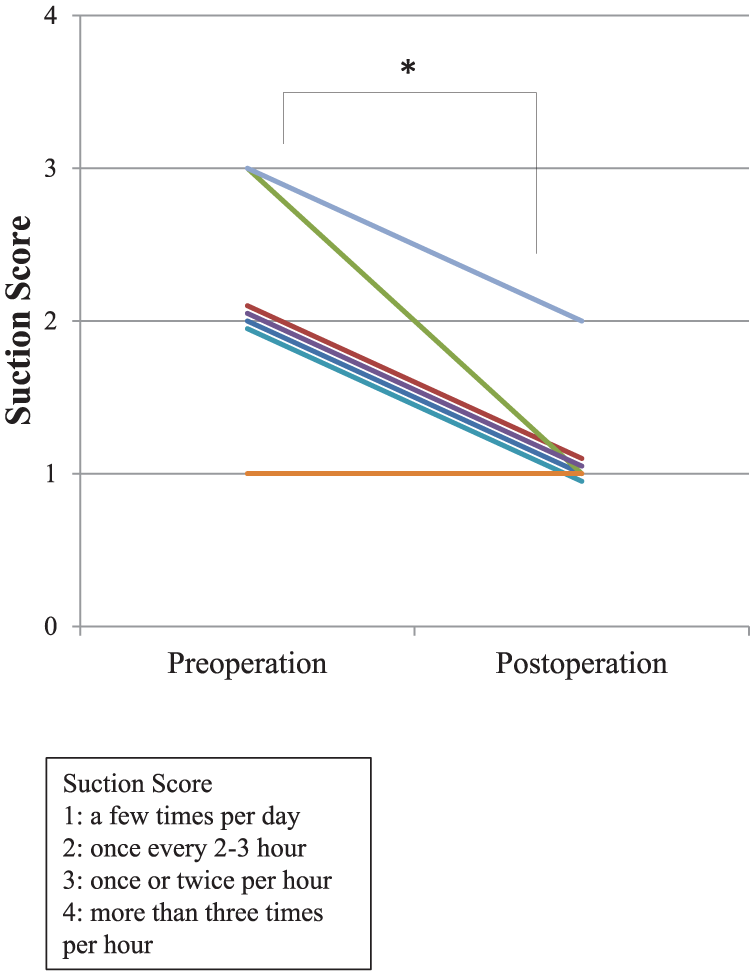
Frequency of suction. The average pre- and postoperative suction scores were 2.14 and 1.14, respectively (P = .001).
Caregiver Burden
The average preoperative Zarit Caregiver Burden Interview score of 30.0 was not significantly different than the postoperative score of 31.3 (P = .634; Table 2).
Quality of Life of the Family Caregivers Before and After Surgery. a
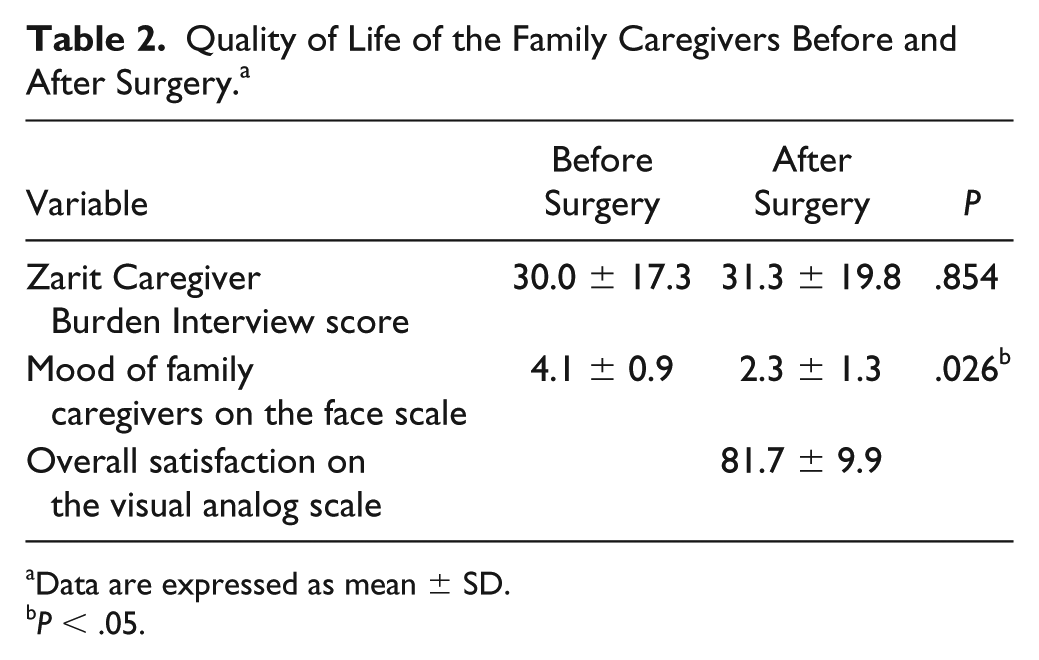
Data are expressed as mean ± SD.
P < .05.
Mood and Satisfaction of Family Caregivers
Among the family caregivers, the average face scale score was 4.14 before surgery and 2.28 after surgery, a significant improvement (P = .004; Table 2). The average satisfaction score, which was evaluated using the VAS, was 81.7 ± 9.9 (Table 2).
Discussion
As Japan transitions into a super-aged society, the number of patients with dysphagia is increasing rapidly. In Japan, the aging rate is expected to reach 30% in 2025, approximately 50% of the medical expenses (approximately ¥5 million per year for PEG and ¥1 million per admission for aspiration pneumonia covered by medical and nursing care insurance plans) are covered by the Medical Care System, which is secured for people aged ⩾75 years of age by the National Treasury. Therefore, the increasing number of patients with severe dysphagia imposes a heavy economic burden on the nation, and new strategies to reduce the incidence of severe dysphagia or repeat aspiration pneumonia are urgently warranted. Compared with other countries, along with a falling birthrate and population aging, Germany and Italy have already become super-aged societies, and other developed countries are expected to shift to this type of society as well. In response to the increasing prevalance of swallowing disorders in Japan, this study is a reference model for other countries for the future (ie, 20-30 years).
Several methods have been developed to prevent aspiration for patients with severe dysphagia, which is characterized by a lack of oral intake and repeat aspiration pneumonia. The Kano method, which was developed by Kano et al 7 and evaluated in this study, has many advantages over other preventive surgical approaches such as classical laryngotracheal separation, 2 laryngeal closure, 3 and total laryngectomy. First, triple-closing the structure using a 2-layer suture of the superior and inferior flaps and moving the sternohyoid muscle flap into the dead space reduces the incidence of postoperative leakage. Second, postoperative leakage, if it occurs, is not severe because it occurs inside the laryngeal compartment; this is distinct from pharyngocutaneous fistula, the major complication of total larnygectomy or laryngotracheal separation, which might result in rupture of cervical major vessels. Third, a stable stoma configuration secures tracheal cannula–free status. Fourth, trachea–innominate artery fistulas induced by the tracheostomy cannula can be avoided because of the tracheal cannula–free status or higher position of the cannula tip in cases of respiratory use. 7 Therefore, the Kano method is increasingly preferred for patients in a poor general condition because of repeat aspiration pneumonia or neurodegenerative disease.
In this study, postoperative QOL as assessed by the FOIS and Barthel index were significantly improved. Five of 9 patients managed to recover oral intake without tube feeding. This was an extremely important and affirmative result considering the indication for the surgery. Regarding the Barthel index, the cause for improved activities of daily living was decreased exhaustion and improved nutritional state due to the amelioration of lower respiratory inflammation, as supported by the significant improvement of CRP levels postoperatively. The amelioration of lower respiratory inflammation led to a marked improvement in the respiratory function; as a result, activities of daily living were thought to have improved. Although not statistically significant, there was a tendency toward improvement in postoperative serum albumin levels and peripheral blood cell counts compared with their preoperative values. Serum albumin has a half-life of 2 to 3 weeks, denotes the long-term nutritional status, and is decreased by surgical stress, so it may not precisely reflect nutritional state during the perioperative period. Moreover, preoperative peripheral lymphocyte count might be highly influenced by chronic lower respiratory inflammation. Therefore, the trend toward improvement in nutritional status as measured by serum albumin level or peripheral lymphocyte count is meaningful even in the absence of significant differences. Proteins with rapid turnover, such as transthyretin, transferrin, and retinol-binding proteins, which denote the short-term nutritional condition and the levels of which are not increased by inflammation, might be helpful for pre- and postoperative nutritional assessment in future prospective studies.
Dysphagia is not a disease but a symptom, and thus most patients with severe dysphagia caused by diseases such as cerebrovascular or neurodegenerative disease require intensive nursing care. In contrast, the core of nursing care for elderly people in the Japanese social insurance system is shifting from institutional or hospitalized care to home nursing care because of the rapid growth of a super-aged society in Japan. However, family caregivers are facing serious difficulties in the home nursing care environment in this country, with the rapidly progressing trends toward nuclear families, declining birthrates, and aging of caregivers.
Concerning the residential style of the patients, 3 of 7 patients received home care, 3 patients were in special nursing homes, and 1 patient was hospitalized before surgery. After surgery, 6 patients were transferred to home care. This finding highlights the value of this surgery in promoting home nursing care due to the stabilization of patients’ general condition, the reduction in suction frequency, and the tracheal cannula–free status after surgery.
There are few reports on care burden and satisfaction among family caregivers of patients after aspiration-preventing surgery. Takano et al 11 measured satisfaction using a depression scale, face scale, and VAS among the families of 7 patients who underwent total laryngectomy or laryngotracheal separation for cerebrovascular disease, neuromuscular disease, or postoperative dysphagia due to laryngeal cancer. Their findings indicated that the depression and face scales after surgery were significantly improved and that the average VAS-based satisfaction score was as high as 96.7 (maximum score, 100). Fuke et al 12 reported QOL among caregivers of patients with neurodegenerative diseases and noted that decreased sputum suction improved QOL and economic burden because of disuse of tracheostomy tubes and reduced use of suction tubes. Iida et al 13 evaluated the QOL of families of pediatric patients after tracheal separation surgery and found that the surgery improved QOL because of decreases in the incidence of aspiration pneumonia and a reduction in nursing care burden. Previous studies thus revealed that the QOL of family caregivers was improved by reduction in the need for suction. However, in the present study, despite the significant reduction in the need for suction, the burden to family caregivers as measured by the Japanese version of the Zarit Caregiver Burden Interview was not significantly different between the preoperative and postoperative periods. There are several factors that should be taken into consideration to reconcile these contradictory results. Although the reduction in the need for suction and the tracheal cannula–free status enabled hospitalized patients to return to home care, the patients required new forms of assistance because of the recovery of oral intake, such as postoperative changes including food preparation or manual feeding with a spoon. Furthermore, previous reports assessed QOL according to suction frequency, whereas the care burden in the present study was assessed using the Zarit Caregiver Burden Interview, which enabled the evaluation of other aspects in addition to the surgical improvement. In contrast, the mood of caregivers as measured by the face scale significantly improved after surgery, and the VAS-based satisfaction score was high, which altogether reflected the satisfaction associated with a reduced need for suction, especially late at night, the level of happiness with returning to home care, and the recovery of oral intake; therefore, the Kano method is expected to improve the emotional QOL of family caregivers.
According to Japanese guidelines for the examination of dysphagia, 14 the indications for surgery to prevent aspiration are as follows: (1) recurrent aspiration pneumonia or high risk for recurrence, (2) irreversible swallowing disorder, (3) severe impairment of articulation or vocal function, and (4) consent to loss of vocal function. The most severe problem associated with this procedure is the loss of voice after surgery. In the 2 patients in whom aspiration was caused by a cranial nerve level disorder with normal cognitive function, the patients could communicate by a combination of writing and electrolarynx after surgery. Of these patients, 1 expressed that with respect to the self-state after surgery, “losing voice is a suffering that fell to hell, but the condition of the body seems to have risen to heaven.” The other patients could not vocally communicate before surgery, and thus, no remarkable change was observed in their communication status after surgery. Therefore, for patients with severe dysphagia who already have difficulty communicating verbally, this method is an appropriate surgical option because it can possibly improve the general condition and reacquisition of oral intake. Conversely, even in cases in which speech is possible and in those in which aspiration pneumonia cannot be controlled and lethal development is anticipated, this method can be applied following careful informed consent procurement.
The indications for PEG have been continually discussed because of the exponential use of PEG even among patients with end-stage dementia. Careful assessment of the decision to perform the Kano method is necessary. Concerning swallowing function, PEG cannot prevent aspiration of saliva or enable oral intake. In contrast, the Kano method can prevent aspiration, which might facilitate the recovery of oral intake. Therefore, we propose that the Kano method is an appropriate choice for patients with irreversible severe dysphagia and impairment of articulation or vocal function, as it can improve QOL of both patients and their family caregivers and increase the satisfaction of family caregivers.
Footnotes
Authors’ Note
This work was presented at the 115th Annual Meeting of Oto-Rhino-Laryngological Society of Japan, May 17, 2014.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This was a specialized study on intractable diseases commissioned by the Specific Disease Control Section, Health Policy Division, Bureau of Social Welfare, and Public Health, Tokyo Metropolitan Government.