
Abstract
Introduction:
Laryngopharyngeal herpes simplex virus infection is rare and presents typically in the supraglottis. Findings on presentation can range from small mucosal lesions to fungating obstructive masses mimicking neoplasm. Laryngopharyngeal herpes is a medically treated disease.
Objectives:
Identify potential treatment in cases that are refractory to antiviral medications.
Methods:
Individual case with treatment adapted from other case report.
Case Presentation:
We report a case of bulky, obstructive supraglottic and glottic herpes virus laryngitis that presented with dysphonia, dysphagia, and airway complaints resistant to acyclovir analogues that was treated effectively with intralesional cidofovir injection.
Conclusions:
Our promising initial response suggests a potential novel treatment for this unusual condition.
Introduction
Herpes simplex virus (HSV) is a double-stranded DNA virus that in the head and neck most commonly affects the cutaneous and mucosal lining of the oral cavity and ocular region. It is speculated that the interaction of viral envelope glycoproteins with host cell receptors convey its propensity for infection of epithelial cells. 1 Laryngopharyngeal manifestations from HSV is exceedingly rare, with fewer than 20 cases presented in the literature. 2 This condition may be underdiagnosed due to its rarity and the difficulty obtaining a diagnosis given its wide range of subjective and physical findings on presentation, ranging from small asymptomatic mucosal lesions to fungating masses concerning for airway obstruction. Several reported cases were in patients with human immunodeficiency virus (HIV) infection, although there is no known relationship between disease burden and quantifiable host factors such as viral load or CD4 count. 3 Steroid use is controversial as some reports identified topical steroid usage as a potential risk factor for onset of herpetic laryngeal lesions. 4 There is no role for surgery except when airway management is the primary concern. Most of the reported cases were treated effectively with systemic antiviral therapy. We present what we believe to be the first case of acyclovir-resistant laryngeal herpes with bulky disease and airway symptoms treated effectively with intralesional cidofovir.
Case report
A 50-year-old male gospel singer with past medical history of well-controlled HIV, hypertension, and asthma presented to clinic with gradual dysphonia, dysphagia, and shortness of breath over several months. The patient’s HIV viral load was undetectable for many years, with CD4 count >600, and he was compliant on his therapy of Darunavir-Cobicistat and Emtricitabine/Tenofovir. He had been on antivirals previously as needed for recurrent anogenital herpes lesions, which included valacyclovir 500 mg oral twice daily from 2001 to 2007 and valcyclovir 1 g daily from 2007 to 2017 with occasional acyclovir as needed. He has a 2-pack year history of intermittent tobacco use and no alcohol, inhaled substances, or intravenous drug abuse. The patient had a penicillin and sulfa drug allergy.
The patient was referred by an otolaryngology colleague for laryngopharyngeal lesions that were biopsied with pathological confirmation of herpes simplex virus. The lesions did not show any response to 2 weeks each of oral famcyclovir and acyclovir or parenteral Foscarnet 40 mg per kg every 12 hours for 7 weeks, initiated by the infectious disease division at the outside institution. The only response noted was to oral steroids. The hope was that further investigation by our group would potentially lead to a different diagnosis and treatment plan.
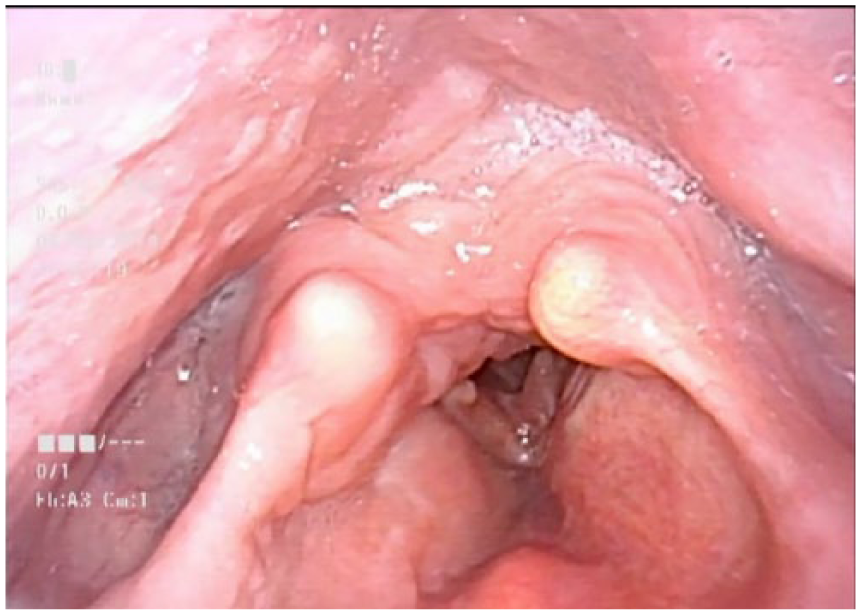
On evaluation in clinic, the patient’s vitals and head and neck exam were normal. Perceptual evaluation of his voice demonstrated severe strain and some audible stridor. The patient did not appear in respiratory distress. On fiberoptic laryngoscopy, he had bulky disease of the supraglottis encompassing his false vocal folds, with little visibility of normal true vocal fold anatomy. The epiglottic petiole was involved with disease, which effaced visualization of the anterior commissure. There was also a lesion of the left pharyngeal wall covered in white exudate (Figure 1). He then underwent operative direct laryngoscopy and debulking for airway concerns as well as repeat biopsies for tissue diagnosis. Surgical pathology showed dense plasma cells and eosinophilic infiltrate with evidence of herpesviral infection (herpes inclusion multinucleated cells). Rule-out tests for HSV-2, HHV-8, as well as aerobic, anaerobic, and fungal acid-fast bacilli were all negative. Flow cytometry of surgical specimens showed no clonal population. At this point, with the help of infectious disease consultation, he was started on parenteral cidofovir infusions. He remained on a course of low-dose oral steroids.

Initial exam with bulky supraglottic and glottic disease.
Due to poor response to antivirals and persistent airway symptoms, the patient required 4 additional trips to surgery, each time for tissue biopsy and debulking using phonosurgical instrumentation and KTP laser ablation of the supraglottis. Surgical pathology remained consistent with mucositis from herpes simplex virus. His tissue was sent to the National Institutes of Health for further resistance testing. Resistance testing showed foscarnet resistance, but there was no commercially available testing for cidofovir resistance. Given the risks to kidney function and no change in disease progress, he was taken off intravenous cidofovir. Steroids were also tapered to see if disease would regress. While there was no regression, the bulky disease of the supraglottis on subsequent in-office stroboscopies and laryngoscopies was not remitting.
Given the refractoriness of the disease to medical and surgical treatment and with the patient stable from an airway standpoint, the next step in treatment remained unknown.
A literature search found a paper documenting the efficacy of intralesional cidofovir in cutaneous herpes simplex virus lesions. 5 We decided to utilize the results of this paper with intralesional injection of cidofovir (375 mg/5 cc in a 1:4 dilution for injection) into the supraglottis and glottis using a percutaneous, trans-thyrohyoid approach. (See supplement for textual description of procedure.)
Our patient was appropriately counseled that this treatment is not standard of care, and risks, benefits, and alternatives of injections were discussed with patient, with the main risk being that there is no change in disease. The efficacy of the dose is unknown and may require multiple injections with no standard protocol of time intervals between injections. The patient agreed to proceed. Given the modeled study that began injections every 2 weeks and extended to every 4 weeks, we elected for serial injections to see improvement approximately every 3 to 4 weeks. The patient then underwent the course of injections described in Table 1.
Timeline of Interventions
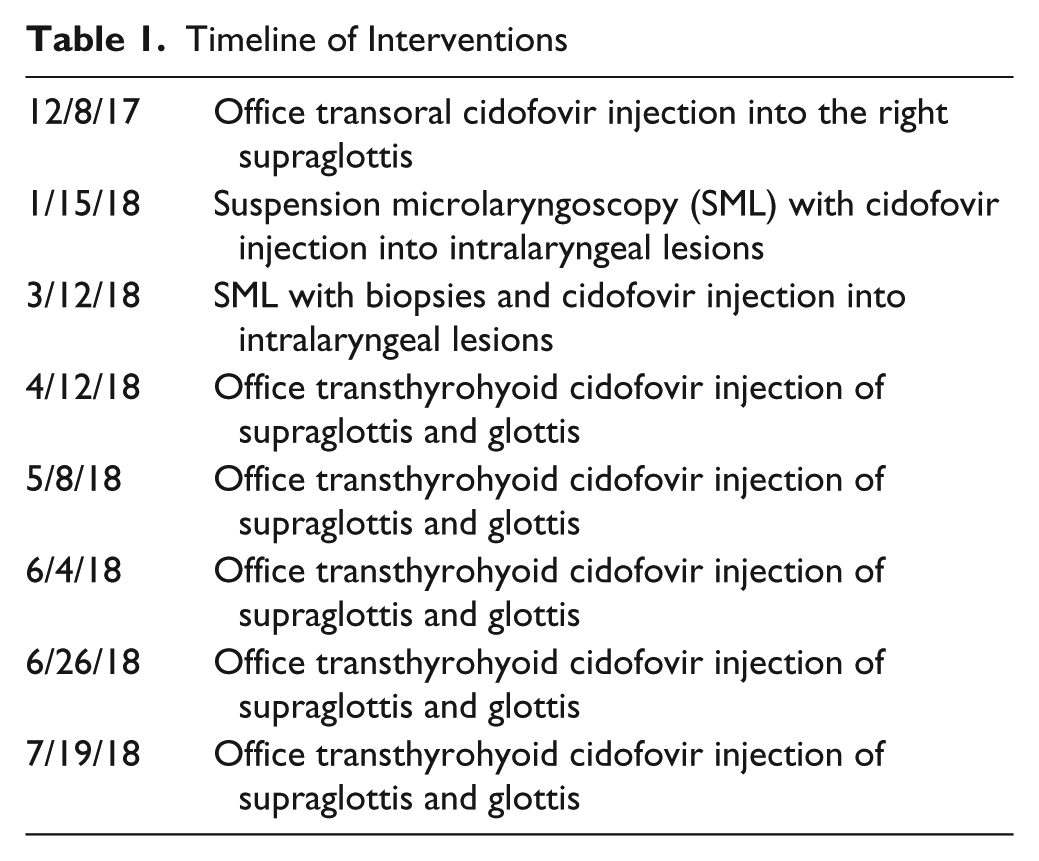
The first cidofovir injection was performed in the office in December 2017, and the next 2 were done in the operating room in conjunction with surgical debulking. Subsequent injections were performed every 4 weeks in the office as his disease remained stable for the next 3 months. Repeat biopsy after the third injection showed persistent ulcerated inflammatory lesion with plasma cellular HSV inclusions. In April 2018, there was the first sign of improvement of his disease burden on office laryngoscopy. His endolaryngeal exam gradually improved as he continued monthly cidofovir injections. In June 2018, there was again notable improvement of his disease burden and the first time both true vocal folds were clearly visible (Figures 2 and 3). Subjectively, his voice felt better, and his VRQOL improved from 33 to 17 from April 2018 to June 2018. At this point, we began extending the time interval to 6 weeks between visits due to stable trend of improvement. On his most recent visit in July 2018, he had newly demonstrable pliability of the true vocal folds. His surveillance and treatment is presently ongoing.

First sign of improving disease burden.
Continued improvement with both vocal folds now visible.
Discussion
Although our patient had a history of HIV infection, his viral load was undetectable for many years, and he had a reconstituted CD4 count to near normal. It remains unknown why he developed clinically apparent HSV laryngitis at this time.
A recent review of adult cases4-8 found only 20 reported cases of HSV laryngitis from 1966 to 2018. All of them were treated successfully with systemic acyclovir/valacyclovir or antibiotics. At this time, there are no known treatment recommendations for antiviral-resistant laryngopharyngeal HSV. The 2015 CDC recommendations for acyclovir-resistant genital and cutaneous HSV include intravenous alternative nucleoside and pyrophosphage analogues such as cidofovir and foscarnet, respectively. 9 Both of these drugs are more toxic than acyclovir. Topical alternatives such as imiquimod and cidofovir gel are used with mixed success in cases of intravenous treatment withdrawal due to systemic adverse reactions, most notably nephrotoxicity. Acyclovir and its analogues are prodrugs that require viral thymidine kinase (TK) for activation to the toxic form. 10 By comparison, cidofovir is a nucleoside analogue that directly inactivates viral DNA polymerase. The molecular basis for acyclovir-resistance is thought due to mutation in viral TK.
Much has been published in the otolaryngology literature about the efficacy of intralesional cidofovir in treating recurrent respiratory papillomatosis of the larynx in adults and children, including reducing the frequency of surgical interventions with no increased risk of dysplasia or systemic adverse effects.11,12 The dermatology literature also reports its intralesional use for plantar warts. 13
A review of the literature showed 1 other case in 2016 describing topical cidofovir for treatment of resistant oral HSV following hematopoietic stem cell transplantation. 14 There are otherwise sparse case reports of other clinical applications of topical and intralesional cidofovir, most notably for the treatment of resistant anogenital herpes in the setting of immunosuppression.12,14
Limitations of our study include a lack of control as the patient may have improved over time regardless of intervention. It is also unknown if his prior exposure to acyclovir and valacyclovir had any effect in the refractoriness of his laryngeal disease to the conventional therapy. The injection interval and concentrations used were also adapted from a reported case of cutaneous herpes as there was a lack of prior research into the optimal treatment strategy. We may need to change the timing and concentration of our injections in the future. The last histologic findings on laryngeal biopsy still demonstrate HSV inclusion cells, which means that the true effect of cidofovir on the laryngeal mucosa is unknown. Future biopsies are required to determine if HSV is eliminated histologically by cidofovir treatments. This is an active next step as part of our continued treatment plan. Nevertheless, our initial success with intralesional injection of cidofovir into supraglottic disease using a standard injection laryngoplasty approach identifies a potential novel therapy for laryngopharyngeal HSV that warrants further investigation, especially in the face of emerging viral resistance. Further clinical studies are needed to establish the safety and efficacy of this treatment.
Supplemental Material
Supplement_1 – Supplemental material for Intralesional Cidofovir for Treatment of Acyclovir-Resistant Laryngeal Herpes Manifesting as Supraglottic Mass
Supplemental material, Supplement_1 for Intralesional Cidofovir for Treatment of Acyclovir-Resistant Laryngeal Herpes Manifesting as Supraglottic Mass by Charles Q. Yang, Anisha Mathur, Princy N. Kumar and Vaninder K. Dhillon in Annals of Otology, Rhinology & Laryngology
Footnotes
Authors’ Note
Written informed consent was obtained from the patient for publication of this case report and any accompanying images.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The contents, views or opinions expressed in this publication are those of the authors and do not reflect official policy or position of Walter Reed National Military Medical Center, the Department of Defense (DoD), or Departments of the Army, Navy, or Air Force. Mention of trade names, commercial products, or organizations does not imply endorsement by the U.S. Government.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.