
Abstract
Objectives:
The aim of this study was to assess the feasibility of the submucosal infusion combined with microflap dissection via laser CO2 as both a diagnostic and therapeutic procedure for superficial glottic lesions. To define a safe surgical procedure in terms of local control, a morphometric study of surgical margins was performed.
Methods:
From January 2011 to January 2016, we treated 122 patients with early glottic lesions with phonomicrosurgery. Patients with effective hydrodissection underwent a microflap and type I-II diagnostic cordectomy. In the others, a biopsy was carried out, and in the case of a malignant lesion, a type III to VI cordectomy was performed. Disease-free survival (DFS) for all the lesions was also determined according to comparative assessments of surgical margins. The Voice Handicap Index was used to evaluate functional outcomes.
Results:
In 27 cases (32%), hydrodissection was effective; specifically, 24 (88.8%) were premalignant lesions, and 3 (11.2%) had a carcinoma. In 56 patients (68%), hydrodissection was not adequate, and a biopsy was performed: 9 (16%) were premalignant and 47 (84%) malignant lesions. The DFS analysis suggests that margins >0.7 mm resulted in a cutoff that can guarantee a safe procedure in the case of effective hydrodissection (P < .05).
Conclusion:
Phonomicrosurgery may be both a diagnostic and therapeutic option with oncological efficacy for superficial glottic lesions of undetermined nature when surgical margins exceed 0.7 mm. In case of inadequate hydrodissection, the hypothesis of an infiltrative carcinoma warrants a wider cordectomy.
Keywords
Introduction
The term phonomicrosurgery introduced in 1994 1 represents a procedure of maximally preserving the layered microstructure of the vocal fold. This type of surgery combines the rules of surgical oncology with laryngoscopic microsurgical and less invasive techniques using submucosal infusion, described by Kass et al, 2 to hydrodissect the epithelial basement membrane away from the vocal ligament. The excision of the vocal fold lesion during the phonomicrosurgery treatment includes performing a microflap that could be obtained with cold instruments or laser CO2, which, combined with submucosal infusion, provokes a less instrumental trauma of the superficial lamina propria (SLP) during the excision of the glottic lesions.3,4 The goal for the management of premalignant lesions as well as early glottic cancer should be achieved with the fewest number of procedures, an accurate diagnosis, adequate treatment, and good functional results. Once the histology has characterized the exact nature of the lesion, the treatment of premalignant and malignant glottic lesions is established, and a study of the margins of resection is essential. For malignant lesions, there is not a consensus establishing exact definition for negative, positive, or close margins; the range varies from 0.5 mm to 2 mm.5-8 Furthermore, for precancerous lesions, these values are generally undetermined.
At clinical examination, superficial glottic lesions often show similar characteristics that make a differential diagnosis before obtaining a definitive histopathological report difficult. Therefore, the phonosurgeon frequently performs glottic surgical procedures in a blind fashion and, in an attempt to preserve vocal function, may tend to undertreat an invasive or microinvasive glottic cancer. Frozen section might help in better characterizing the lesion and determining its radical excision, but an accuracy inferior to 90% has been reported. 9
Over the past few years, techniques such as the stripping of the mucosa or random biopsies have been replaced by phonomicrosurgery. In fact, in the case of a lesion contained within the margins and without signs of deep infiltration, the aforementioned procedure can be both diagnostics and potentially curative, 10 allowing us to treat a patient with a 1-time procedure fully respecting the functional structures.
The main aim of our study was to assess the feasibility of the submucosal infusion technique combined with microflap dissection via laser CO2 as both a diagnostic and therapeutic procedure for superficial glottic lesions of an undetermined nature, based on surgical margins assessment and follow-up. As a second aim, we correlate frozen section analysis of surgical margins with outcomes by morphometric measurements, regardless of the nature of the lesions in the attempt to define a cutoff value able to guarantee a safe procedure in both premalignant and malignant glottic lesions. Finally, we analyze the functional outcomes of the different phonomicrosurgical procedures with a self-assessment postoperative test.
Materials and Methods
From January 2011 to January 2016, we treated 122 patients with early glottic lesions with a phonomicrosurgical technique by a single surgeon (O.G.). The study included patients who had been diagnosed with either premalignant or malignant superficial glottic lesions. All patients consented to a minimally invasive endoscopic surgical procedure even when they preferred radiotherapy treatment in the absence of a definitive histopathological report. Patients that presented the following characteristics were excluded: an incomplete medical record, Reinke’s edema, sulcus vocalis, vocal nodules, patients treated with cold instruments, a diagnosis of hyperkeratosis lesions, and patients with cords that had previously been treated. According to clinical preoperative examinations (endoscopy, narrow banding imaging [NBI], stroboscopy, or computed tomography [CT]), we identified 83 suitable patients for hydrodissection and phonomicrosurgery.
The study group was composed of 67 (80.7%) males and 16 (19.3%) females, with a mean age of 66 years (range, 20-90 years; SD ± 12.2). Risk factors such as alcohol consumption and smoking were registered in 72% and 84% of the patients, respectively. The procedure was performed under general endotracheal anesthesia following the technique described by Zeitels, 9 which includes a submucosal saline infusion realized with a 23-gauge needle inserted into the SLP, anterior to the vocal process on the superior surface of the fold. 10 En bloc resection of the glottic lesions were obtained with laser CO2, and the specimens were mounted and oriented on a wooden support to obtain information about the nature of the lesions and the margins with frozen section. Patients with effective hydrodissection, in terms of lifting lesion from the vocal ligament, have undergone a microflap and subsequent type I and II diagnostic cordectomy. When the hydrodissection was not effective and the lesion was difficult or impossible to lift from the vocal ligament, a biopsy was carried out.
Patients with malignant infiltrative lesions underwent a type III to VI cordectomy; those with premalignant or carcinoma in situ, on the other hand, underwent a type I or II cordectomy. Frozen section margins were performed in all patients, and in the event of positive margins, an additional targeted excision was performed. We adopted close follow-up strategy (every 3-4 weeks for the first 6 months, 2 months for the first year, and every 4-6 months for the second year) to determine the disease-free survival rate.
An additional specific morphometric evaluation of surgical margins was carried out retrospectively in 63 out of 83 patients (76%). A comparison between frozen section and definitive diagnosis was done to assess its diagnostic value. Comparative multidimensional assessments of surgical margins according to specific measurements of 5 oriented specimens (anterior, posterior, superior, inferior, and deep) were performed in both groups to evaluate both the diagnostic and therapeutic value of 1-stage excision.
The margins have been classified as positive (when the margin touches the lesion), close (when the distance between margin and lesion was <1 mm), or negative (margin free from disease).
We have categorized close margins in 3 subgroups:
Group 1 for values <0.4 mm (n = 1; 2.5%)
Group 2 for values between 0.4 mm and 0.7 mm (n = 13; 34.5%)
Group 3 for values >0.7 mm and < 1 mm (n = 24; 63%).
The Voice Handicap Index (VHI), a self-administered questionnaire, was given to the patients after surgery; it provides 3 subscale scores (functional, physical, and emotional) in addition to an overall handicap score, to evaluate the functional outcomes. The study was approved by our institutional review board. Patients were given extensive information about the procedures they were about to undergo, and all the participants signed an informed consent agreement.
Statistical analysis was performed using Stata version 13 (StataCorp, College Station, Texas, USA), and a value ofP < .05 was considered statistically significant. Survival curves were generated by the Kaplan-Meier method, and the log-rank test has been used when appropriate.
Results
Preoperative and Operative Setting
Clinical examinations for infiltrative lesions resulted negative or not significant for pathology in 28 cases (33.7%). Positive or uncertain infiltrative lesions results were recorded for 55 patients (66.3%). In all cases, the hydrodissection was performed and was effective in 27 out of 83 cases (32%), allowing the surgeon to carry out a phonomicrosurgical procedure producing a microflap and type I or II diagnostic cordectomy via laser CO2. The intraoperative histopathological report for the 27 patients revealed 24 (88.8%) premalignant and 3 (11.2%) malignant lesions.
The hydrodissection was not adequate in 56 out of 83 (68%) cases, and a biopsy was performed to obtain intraoperative information about the nature of the lesion. Of these patients, 9 (16%) had premalignant lesions, and 47 (84%) had early glottic cancer (Figure 1).
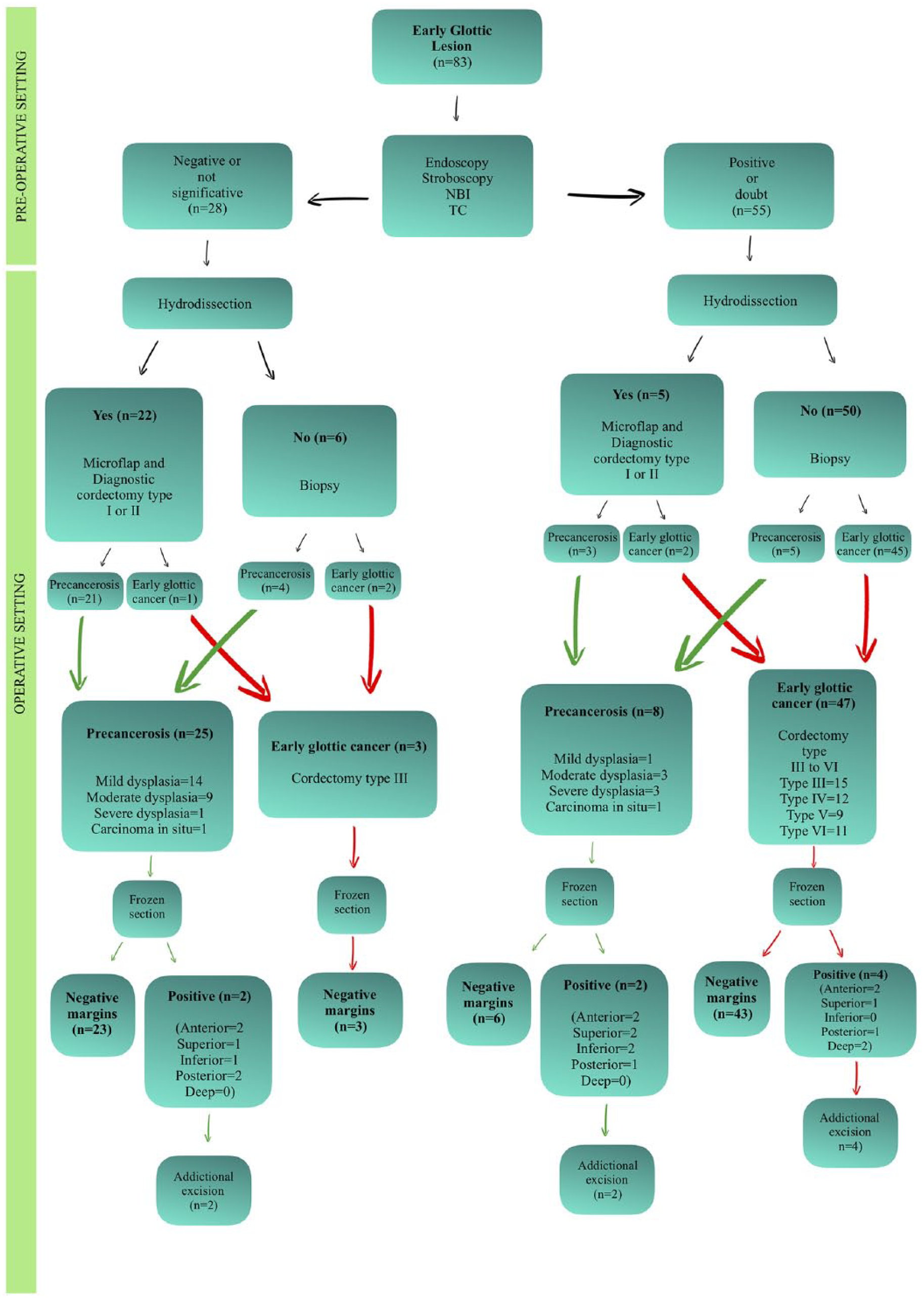
Flow chart of the preoperative and operative setting procedures.
When a diagnosis of early glottic cancer was made (in this sample, in 50 [60.3%] cases), the procedure adopted consisted on type III (n = 18; 36%), IV (n = 12; 24%), V (n = 9; 18%), or VI (n = 11; 22%) cordectomy. The extension of the tumors was classified according to the AJCC staging system as follow: 28 (56%) patients presented T1a, 14 (28%) were T1b, and 8 (16%) had T2 extension.
The intraoperative biopsy or diagnostic cordectomy revealed a premalignant lesion in 33 (39.7%) cases with the following grade of disease: mild dysplasia (n = 15; 45.5%), moderate dysplasia (n = 12; 36.4%), severe dysplasia (n = 4; 12.1%), and carcinoma in situ (n = 2; 6%).
Concerning the feasibility of the phonomicrosurgical procedure with the hydrodissection technique, our results show that in 3 (11%) out of 27 patients, a malignant lesion was documented despite a complete mucoligamentous lifting. On the other hand, 9 (16%) of the 56 patients with an inadequate hydrodissection had lesions that were defined as premalignant in the histopathology report. Therefore, the sensitivity and specificity of the hydrodissection procedure in our series were 72% and 94%, respectively. The positive and negative predictive values were 88% and 84%, respectively. Thus, an overall accuracy of 83% was documented (Table 1).
Hydrodissection Procedure Results.

Abbreviations: NPV, negative predictive value; PPV, positive predictive value.
Surgical Margins
An assessment of the frozen section margins for the malignant lesions showed that 46 (92%) patients had negative margins, and 4 (8%) patients had positive ones, specifically: anterior (n = 2), superior (n = 1), posterior (n = 1), and deep (n = 2). No inferior margin resulted. In the 4 patients with positive margins, an additional excision was performed, obtaining margins free from disease. Frozen section margins of premalignant lesions showed 29 (87.8%) negative results and 4 patients with the following margins involved: anterior (n = 4), superior (n = 3), posterior (n = 3), and inferior (n = 3). No deep margin resulted, and additional excisions were also performed in these 4 cases obtaining negative margins (Figure 1).
In all the patients, the histopathological reports of the specimens confirmed the intraoperative diagnosis. In 63 out of 83 patients (76%), it was possible to perform a measurement of the individual margins of surgical resection. The mean value of the individual margin is reported in Figure 2. In terms of morphometric analysis, the inferior and deep margins are the smallest. In 38 out of 63 (60%) patients, we identified at least 1 margin as “close” (<1 mm).
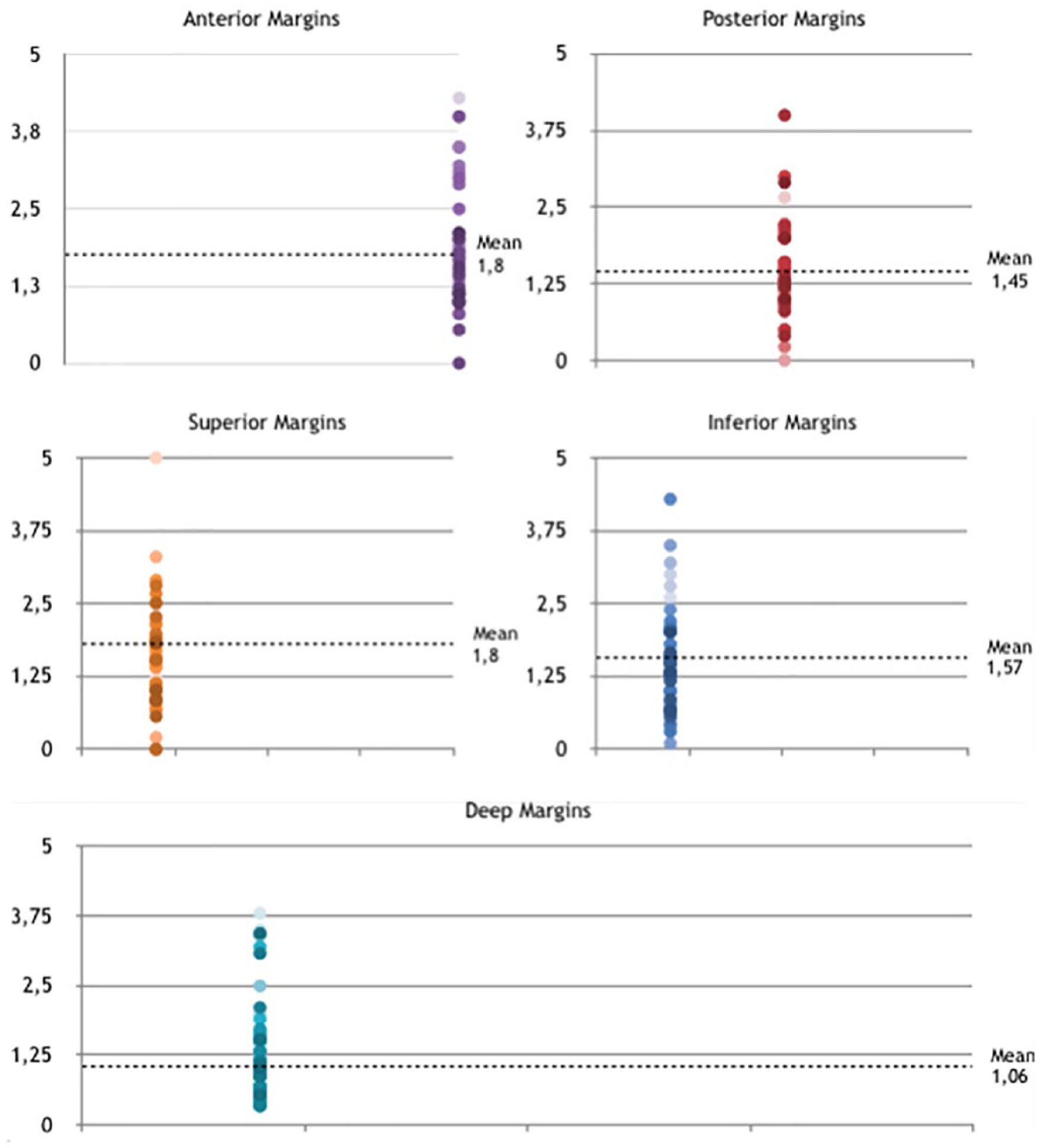
The mean value of the individual margin.
The Kaplan-Meier disease-free survival curves (Figure 3) revealed that lesions with at least 1 margin <0.7 mm (defined by group = 1 and group = 2) had a greater risk of relapse than group 3 patients (P = .03 was obtained with log-rank test).
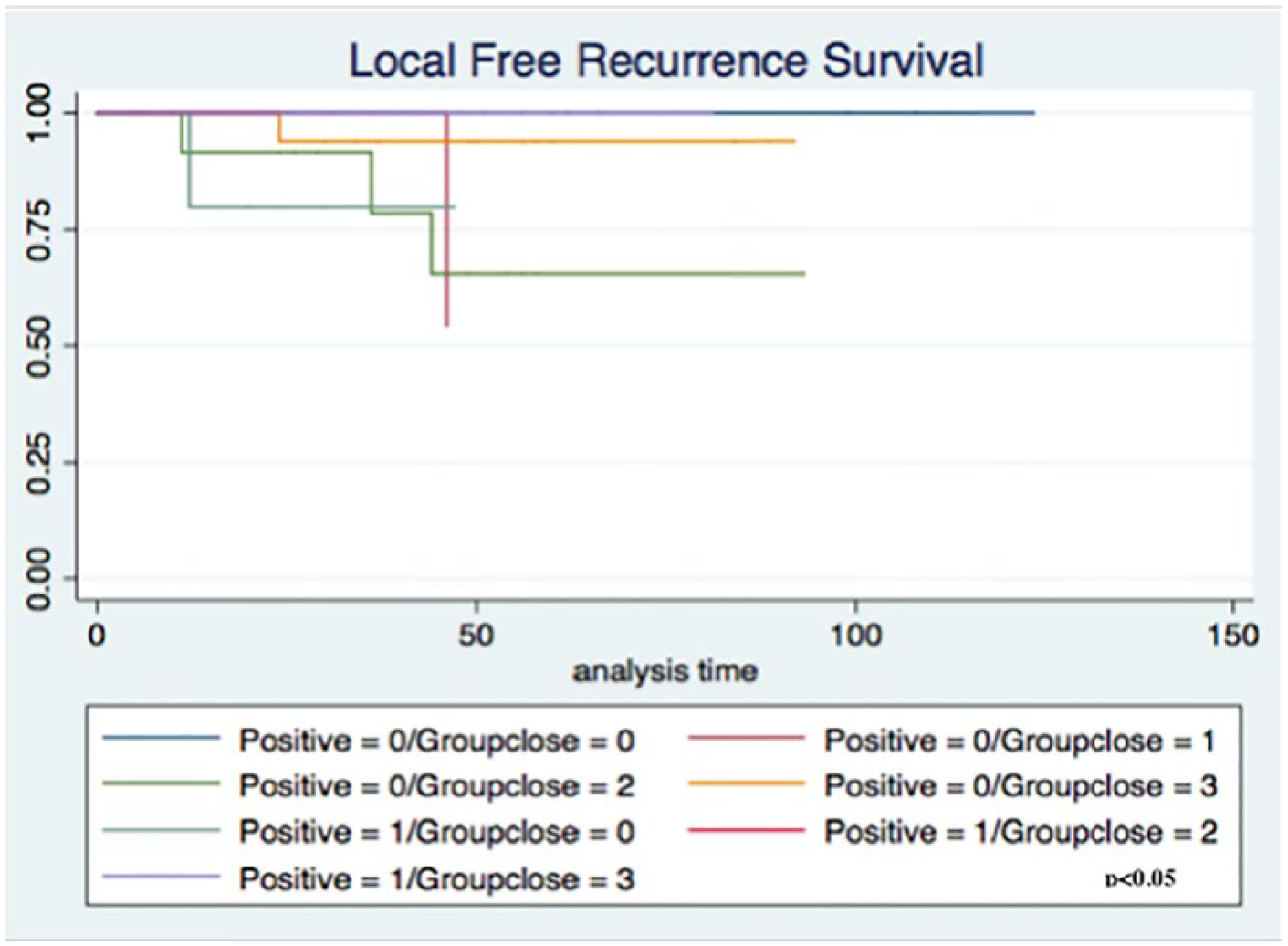
The Kaplan-Meier disease-free survival curves according to positive and close margins.
Recurrence occurred in 8 patients, with the following distribution of lesions: 2 (6%) premalignant lesions, which presented margins that were positive or close <0.7 mm, relapsed in 1 premalignant and 1 malignant lesion, and 6 (12%) were recurrences of malignant lesions, of which 3 had negative or close >0.7 mm margins and 3 had positive or close <0.7 mm margins. The mean time of recurrence was approximately 30 months (range, 11-36 months).
Vocal Functional Results
We also studied the functional outcomes in terms of quality of voice using the VHI questionnaire in 48 (57.8%) patients out of 83. The mean value of the total VHI was 23.8 with a range of 0 to 84 (SD ± 21.37). The values obtained from the specific type of cordectomy were: type I = 11 points with a range of 0 to 52 (SD ± 16); type II = 12.6 points with a range of 3 to 21 (SD ± 6.6); type III = 39.5 points with a range of 19 to 60 (SD ± 22.54); type IV = 38.6 points with a range of 6 to 84 (SD ± 27.23); type V = 37.5 points with a range of 29 to 58 ( SD ± 13.72); and type VI = 36.6 points with a range of 17 to 57 (SD ± 15.6) (P = .02). An evaluation of the VHI score of premalignant and malignant lesions has shown mean values of 10 (SD ± 8.43) and 31 (SD ± 19.32), respectively (P = .746).
Discussion
Despite the introduction of new diagnostic tools, the true nature of an early glottic lesion is still hard to distinguish until the histopathological exam is done. In the past, premalignant glottic lesions were removed with the use of a stripping procedure that lacked oncological radicality and had a higher risk of leaving part of the initial lesion. 11 This would require an additional procedure to achieve the complete excision; this is particularly true in the case of an invasive cancer.
The introduction of phonomicrosurgery, with the use of submucosal injection, might help surgeons better determine the nature of lesions (ie, premalignant lesion or infiltrative cancer) based on the ease with which a tissue can be lifted by mucoligamentous hydrodissection. 12 However, the accuracy of this procedure is still unknown.
In our study, all the patients received a clinical examination that suggested the potentially infiltrative nature of the lesion according to conventional diagnostic tools. In our patients, a hydrodissection with saline injection was attempted; however, when the submucosal lifting was not adequate, a biopsy was performed. According to the literature, 13 the use of the new diagnostic tools (ie, NBI, contact endoscopy, stroboscopy) does not allow an exact preoperative diagnosis of these lesions, and our results confirm this. In 94% (47/50) of cases, lesions that were positive or uncertain in the clinical examination ultimately harbored a malignant lesion, whereas in the 89.3% (25/28) of negative or not significant cases at the clinical examination, premalignant lesions were diagnosed in the definitive histopathological report.
Even if an initial hydrodissection is unable to identify malignant versus premalignant lesions with certainty, random biopsies of superficial glottic lesions are inadequate for several reasons. Herein, we report that hydrodissection with phonomicrosurgery, which was 83% accurate in our series, may represent not only a safe and voice-sparing diagnostic procedure but also a therapeutic tool in a high percentage of superficial hydrodissectable lesions. Therefore, vocal cord stripping or biopsy should be avoided when phonomicrosurgery with saline hydrodissection is feasible. In fact, for macroscopically non-infiltrating glottic lesions, this method is able to sample and accurately remove the pathological area allowing for an intraoperative evaluation of the lesion through study of the resection margins accurately oriented by the surgeon.
The measurement of the margins and the comparison between patients with and without recurrence in our cohort demonstrated that the inferior (1.61 mm) and deep (1.43 mm) margins represent those with the smaller distance between normal tissue and front lesion. According to these data, the phonosurgeon, because he or she knows the geometric limits of the CO2 laser beam, should be particularly careful when resecting the lesion at the inferior and deep plane.
It is accepted worldwide that the status of margins (positive or close) plays an important role in the recurrence-free survival of early glottic cancer. 14 Conversely, the impact of the margins in the premalignant lesions still remains unknown. From the analysis of our data, it is possible to suggest that regardless of the nature of the lesions, patients with margins ≥0.7 mm presented the same rate of recurrence as those with negative ones, thus reducing the safe margin to 0.7 mm.
One of the most critical goals of phonomicrosurgery with hydrodissection procedure is to preserve the SLP to obtain good postoperative vocal outcomes. The results of our VHI questionnaires show worse values proportionate to the increase in the type of cordectomy, according to the literature.15,16 For patients with a histological diagnosis of malignant lesion, the total VHI value is of a moderate severity, whereas for the premalignant, the estimated value is considered mild according to the classification criteria of the VHI. 17 This could be an interesting point of discussion regarding the preservation of greater vocal integrity by comparing the phonosurgical approach with more aggressive laser surgery techniques.
In conclusion, in view of our results, we propose an algorithm for the management of glottic lesions of uncertain nature. As shown in Figure 4, irrespective of the results of the clinical examination, we suggest performing the hydrodissection procedure in all patients. The effectiveness of the hydrodissection allow us to perform a type I or II cordectomy as a diagnostic and therapeutic tool with good functional results.
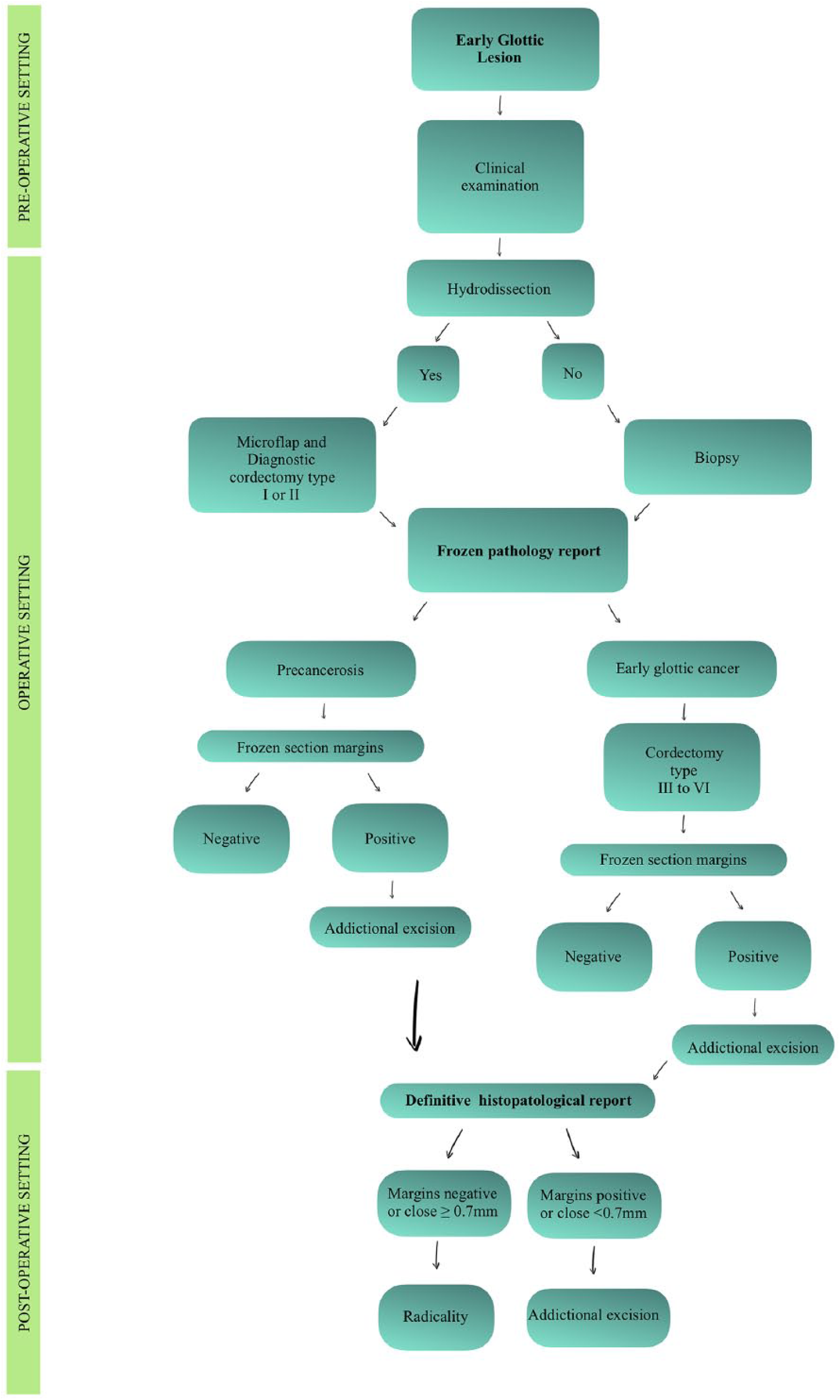
Proposed diagnostic and therapeutic algorithm.
The study presents strengths and weaknesses. The positive aspects are that a standardized procedure was used by a single surgeon in a single institute and the samples were studied by a team of head and neck pathologists, suggesting a high level of reliability. Conversely, the following limitations exist: Preoperative assessment of laryngeal lesions is potentially weakened by individual clinical evaluation, a common problem for pathological examinations. Of course, this case study is not large enough to validate our decisional algorithm definitively.
Conclusions
The phonomicrosurgical resection technique preceded by hydrodissection is a valid surgical approach to treat patients with both premalignant and/or early glottic malignant lesions. Our study suggests that in expert hands, the suggested algorithm is able to allow both diagnosis and therapy in hydrodissected early glottic lesions whose nature is undetermined, minimizing voice side effects. According to our data, we also suggest that lesion excision with margins above 0.7 mm has to be considered negative, reducing the cutoff limit of safe surgical procedure with function advantages. Of course, these results need to be confirmed by larger multicentric studies with an adequate number of patients and follow-up.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.